
Abstract
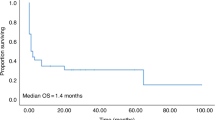
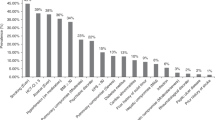
The role of ICU support in BMT patients is controversial. In an era of constrained resources, the use of prognostic factors predicting outcome may be helpful in identifying patients who are most likely (or unlikely) to benefit from this intervention. We attempted to define the survival of patients admitted to ICU following autologous or allogeneic BMT and to identify those factors important in determining patient outcome. A retrospective study of all adult BMT recipients admitted to intensive care over a 6 year study period was performed to determine overall and prognostic indicators of poor outcome. Pre-treatment, pre-ICU admission and ICU admission data were analyzed to identify factors predicting long-term survival. 116 patients were admitted to ICU on 135 separate occasions with the primary reasons for admission being respiratory failure (66%), sepsis associated with hypotension (10%), and cardiorespiratory failure (8%). No pre-ICU characteristics were predictive of survival. Univariate analysis identified the number of support measures required, the need for ventilation or hemodynamic support, the APACHE II score, the year of ICU admission and the serum bilirubin as significant predictors of post-discharge survival. On multivariate analysis the year of ICU admission, the need for hemodynamic support and the serum bilirubin remained significant. The APACHE II score significantly underestimated survival in the 46% of patients with scores less than 35, and could only be used to predict 100% mortality when it exceeded 45. Twenty-three percent of all BMT patients admitted to the ICU and 17% of ventilated patients survived to hospital discharge. Of the 27 patients surviving to leave hospital, 16 remain alive with a median follow-up of 4.2 years and a mean Karnofsky performance status of 90. Although mortality in BMT recipients admitted to ICU is high our results indicate that intensive care support can be lifesaving and that the outcome in patients requiring ventilation and ICU support may not be as poor as has been previously reported. No single variable was identified which could be used to predict futility but patients requiring both hemodynamic support and mechanical ventilation, and those with an APACHE II score greater than 45 have a very poor prognosis and are unlikely to benefit from lengthy ICU support.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Jackson, S., Tweeddale, M., Barnett, M. et al. Admission of bone marrow transplant recipients to the intensive care unit: outcome, survival and prognostic factors. Bone Marrow Transplant 21, 697–704 (1998). https://doi.org/10.1038/sj.bmt.1701158
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1701158
Keywords
This article is cited by
-
Prognostic Factors and Intensive Care Outcome in Post-Transplant Phase of Hematopoietic Stem Cell Transplantation
Indian Journal of Hematology and Blood Transfusion (2023)
-
Der knochenmarktransplantierte Patient auf der Intensivstation
Medizinische Klinik - Intensivmedizin und Notfallmedizin (2021)
-
Improved short- and long-term outcome of allogeneic stem cell recipients admitted to the intensive care unit: a retrospective longitudinal analysis of 942 patients
Intensive Care Medicine (2018)
-
Prognostic factors and outcome of patients undergoing hematopoietic stem cell transplantation who are admitted to pediatric intensive care unit
BMC Pediatrics (2016)
-
Adaptive Immune Response Impairs the Efficacy of Autologous Transplantation of Engineered Stem Cells in Dystrophic Dogs
Molecular Therapy (2016)
