
Abstract
We have extended our previous work investigating the neural correlates of cue-induced cocaine craving through the use of positron emission tomography with greater spatial resolution (<4.6 mm), an evocative script, and a pixel-by-pixel analysis. Craving and cerebral glucose metabolism were measured after presentation of cocaine-related or neutral cues to 11 cocaine abusers. Cocaine cues elicited a higher degree of craving than has been previously reported and resulted in left hemispheric activation of lateral amygdala, lateral orbitofrontal cortex, and rhinal cortex and right hemispheric activation of dorsolateral prefrontal cortex and cerebellum. The intensity of activation in these areas (except cerebellum), as well as left insula, was also correlated with craving. Deactivation occurred in left ventral pole and left medial prefrontal cortex. The results suggest that induction of drug craving involves a neural network that assigns incentive motivational value to environmental stimuli through the coactivation of brain regions that process information about memories and emotions.
Similar content being viewed by others

Main
Cocaine craving is a complex phenomenon that contributes to relapse after abstinence from drug use. Self-reports of drug craving can be evoked reliably in a laboratory setting by presenting cocaine-related stimuli to cocaine abusers (Childress et al. 1993; Ehrman et al. 1992). Our research group has previously demonstrated that exposing cocaine abusers to a videotape depicting persons engaged in cocaine use and paraphernalia related to cocaine use induced craving and increases in regional cerebral metabolic rates for glucose in many cortical areas, including the dorsolateral prefrontal cortex, the medial orbitofrontal cortex (OFC), and the temporal lobe (Grant et al. 1996). Cue-induced craving was also correlated with an increase in rCMRglc (regional cerebral metabolic rate for glucose) in the medial temporal lobe (amygdala), dorsolateral prefrontal cortex, and cerebellum. These regions have been implicated in several forms of memory (Molchan et al. 1994; Tulving et al. 1999), suggesting that a distributed neural network that integrates emotion with memory may link environmental cues with cocaine craving. Subsequent brain imaging studies that investigated cocaine craving using positron emission tomography (PET) (Childress et al. 1999; Kilts et al. 2001; Volkow et al. 1999; Wang et al. 1999) and functional magnetic resonance imaging (fMRI) (Breiter et al. 1997; Garavan et al. 2000; Maas et al. 1998; Wexler et al. 2001) have supported our original evidence that a number of cortical and subcortical brain regions involved in emotional memory are activated during craving.
In this study, we sought to extend our previous observations using a positron emission tomograph with greater spatial resolution (<4.5 vs. 8.6 mm, within-plane full width at half maximum [FWHM]), a script that described in detail the physiological and psychological sensations associated with being high on cocaine, and a pixel-by-pixel analysis (rather than a region-of-interest analysis). The accumulation of published studies permitted the generation of a priori hypotheses regarding activation of specific brain regions in response to cocaine-related cues. Seven brain areas were selected for these a priori hypotheses: anterior cingulate, amygdala, dorsolateral prefrontal cortex (DLPFC), OFC, ventral striatum, cerebellum, and parahippocampal gyrus. Three additional regions (paracentral cortex, posterior thalamus, and caudate nucleus) were predicted a priori to not show changes in response to cocaine cues and thus served as a check for false positives or generalized brain activation.
METHODS
Research Participants
Structured psychiatric interviews were conducted with each participant before admission using the Diagnostic Inventory Survey (DIS), an instrument based on psychiatric criteria in the Diagnostic and Statistical Manual (DSM-IV-TR; American Psychiatric Association 2000). The diagnosis of cocaine dependence was not an inclusionary criterion; however, those included in the study had to be current cocaine users who identified cocaine as their drug of choice. Exclusionary criteria included lifetime history of any DSM-IV axis I diagnosis other than a substance abuse disorder, evidence of physical disease, history of head trauma, claustrophobia, or pregnancy. Dependence (as defined by DSM-IV-TR) on any drug other than nicotine or cocaine was also exclusionary. All participants had urine toxicology on admission to the inpatient unit to document recent illicit substance use.
Experimental Procedures
All procedures were reviewed and approved by the National Institute on Drug Abuse (NIDA) Institutional Review Board, and every subject signed a statement of informed consent before participation in this study. Subjects participated in two study sessions; one involved exposure to arts cues (neutral condition) and the other involved exposure to cocaine cues (experimental condition). As in our prior study, the neutral session always came before the cocaine session in order to prevent an association effect between the experimental environment and drug-related stimuli. Sessions were separated by at least 1 week for male subjects, whereas female subjects typically returned for their second session 4 weeks later to approximate the same phase of their menstrual cycle. Cocaine abusers resided on a closed ward at the NIDA Intramural Research Program for two nights before each test session to ensure abstinence from drugs. Before the first PET session, subjects were familiarized with the experimental environment and procedures. During this time, they were fitted with a custom-molded thermoplastic mask that served to minimize head motion and facilitate alignment within the scanner.
All volunteers abstained from nicotine and caffeine and had not eaten any food for at least 6 h before consuming a nonketogenic breakfast on the morning of each test session. Upon arrival at the PET center, a venous catheter was placed in the antecubital vein of each subject for injection of the radiotracer. After placement of the catheter, subjects were placed in the scanner for a transmission scan that utilized three internal rotating 68Ge/68Ga rod sources. The transmission scan served as the basis for measured attenuation correction. Subjects were then seated in a comfortable chair facing a video monitor in a separate room, and baseline psychometric measures were obtained. Ambient sounds were masked with “pink” noise (70 dB).
During each experimental session (arts cues or cocaine cues), subjects listened to an evocative script, watched a videotape, and viewed items placed in front of the video monitor that were related to the experimental session. The videotapes and paraphernalia were identical to those used in our previous study (Grant et al. 1996). Briefly, the arts-related video showed art supplies and natural objects being handled in a manner that was meant to parallel the handling of drug-related objects in the cocaine-related video. Items related either to art (paint brush, paper, art pencils, leather punch, items used by participants in the activity room,) or to cocaine (glass crack pipe, mirror, razor blade, straw, rolled $20 bill, lactose powder and simulated “crack rocks” that subjects were told to think of as “pharmaceutical cocaine”) were displayed on a table in front of the video monitor.
Immediately before injection of the radiotracer, an investigator read a script detailing the stimuli that the subject would view (arts cues or cocaine cues). Depending on the session, the investigator encouraged subjects to imagine themselves in a setting where they would have been making art or would have been using cocaine. The script was constructed to vividly describe the emotions and sensations associated with either making art or using cocaine, and it was read in an effusive manner. Concurrent with the start of exposure to the session video, 4–5 mCi of [18F]fluorodeoxyglucose (FDG) was infused intravenously over 1 min. Exposure to the neutral or cocaine cues continued throughout the 30-min period after the FDG injection.
An experimenter was in the room during the entire 30-min period to ensure that the subject sat quietly and kept his or her attention focused on the video and cue objects. Before the cue exposure and at 10, 20, and 30 min during cue exposure, the experimenter administered six self-report questions to the subject: “How good do you feel?”; “Do you have a craving or urge for cocaine?”; “Do you want cocaine?”; “Do you need cocaine?”; “Are you turned off?”; “How awake are you?”. Participants were instructed to respond verbally on a scale of 0 to 10, with “0” indicating “not at all” and “10” indicating “extremely.” The responses at 10, 20, and 30 min were averaged within each session, and changes across sessions were evaluated using paired t-tests.
Subjects were then encouraged to void, and they were positioned on the scanner bed. PET images were acquired on a Siemens (Knoxville, TN) ECAT EXACT HR+ whole-body scanner in 3D mode. The scanner simultaneously acquires 63 slices, with an axial field of view of 15.5 cm and a resolution of 4.6 mm (within-plane FWHM) at the center of the field of view. Scanning began ∼45 min after FDG injection and continued for 20 min. Subjects then returned to the ward and were released on the day after the PET study.
Analysis of PET Data
PET images were reconstructed using filtered back-projection with a ramp filter (0.5 Hz cutoff). Scatter and attenuation correction were applied by using the ECAT-7 software provided by the scanner manufacturer (CTI PET Systems, Knoxville, TN). The reconstruction resulted in images with a 128 matrix size and transaxial pixel size of 1.9 mm. Changes between sessions across the entire brain volume were assessed via a pixel-by-pixel analysis with SPM99 (Wellcome Dept of Cognitive Neurology; http://www.fil.ion.ucl.ac.uk/spm). Briefly, pairs of PET images (decay-corrected raw counts) from the two sessions for each subject were coregistered and then spatially transformed to a space using the PET template image supplied with the SPM99 package (Ashburner and Friston 1997). This template image is based on the space defined by the International Consortium for Brain Mapping Project (ICBMP). The spatially transformed images consisted of isotropic 2-mm voxels, but smoothing with an 8 mm × 8 mm × 8 mm Gaussian filter yielded an effective resolution to 9 mm. Before statistical analysis, the smoothed images were proportionally scaled to the global brain value to yield normalized (relative) rates of regional cerebral glucose metabolism (nrCMRglc). Statistical analysis was performed using the general linear model method implemented in SPM99, using the method of Friston to estimate residual variance (Holmes et al. 1997; Poline et al. 1997). The factors of interest were session and craving scores.
Based on previous studies, a set of seven brain areas, identified a priori, were expected to show either changes across sessions or correlations with craving: anterior cingulate, amygdala, DLPFC, OFC, ventral striatum, cerebellum, and parahippocampal gyrus. Three additional regions—paracentral cortex, posterior thalamus, and caudate nucleus —were predicted a priori to not show changes in response to cocaine cues and thus served as a check for false positives or generalized brain activation. A statistical significance threshold of 10 contiguous pixels with Z-scores of at least 2.58 (p < .005 uncorrected for multiple comparisons) was used to assess changes in nrCMRglc across sessions within these regions. This statistical threshold represents an α level criterion of p < .05 adjusted for 10 a priori regions. To limit spurious regressions driven by outlier data points, a more stringent threshold was used when analyzing the correlations between the change in nrCMRglc and change in self-reported craving for cocaine (10 contiguous pixels with a t-score of at least 3.09, p < .001 uncorrected for multiple comparisons). This threshold required correlations to account for at least 66% of the variance (i.e., |r| > 0.82). Regions not specified a priori that exceeded this threshold were noted on an exploratory basis. Anatomical identification of the regions was based on the set of structural MRI scans provided by the ICBMP and published atlases of the human brain (Damasio 1995; Duvernoy 1999; Mai et al. 1998), except for the OFC, for which we followed the nomenclature of Ongur and Price (2000).
RESULTS
Research Participants
Eleven cocaine abusers completed this study (age range 32–39 years; nine men, two women; nine black, two white). Eleven additional subjects were enrolled but did not complete the study due to failure to appear (three), medical reasons (six), or technical problems (two). All participants reported regular current use of cocaine (mean use 2.3 gm/wk, range 0.4–5.1 gm/wk) with a mean history of use of 6.4 years (range 14 months to 10 years). Seven participants met criteria for current dependence on cocaine, and one additional participant who did not meet criteria for current dependence did meet criteria for a history of cocaine dependence within the past 6 months. Participants also reported current use of opioids (1/11 subjects), marijuana (4/11 subjects), alcohol (8/11 subjects), and nicotine (10/11 subjects). One participant met criteria for nicotine dependence.
Subjective Reports
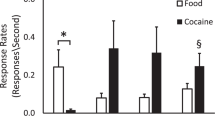
Self-reports of cocaine craving increased significantly from an average of 1.4 ± 0.6 (SEM) during presentation of neutral stimuli to 5.1 ± 1.1 after presentation of drug-related stimuli (t = 4.23, 10 d.f., p < .001) in response to the question “Do you have a craving or urge for cocaine?” The time course of the craving response during the two sessions is shown in Figure 1. There were also corresponding increases for the self-reports of wanting cocaine (neutral cues −1.3 ± 0.6, cocaine cues 2.4 ± 0.6, t = 3.35, p < .005) and needing cocaine (neutral cues 0.6 ± 3.4, cocaine cues 3.4 ± 1.0, p < .01). Substantial individual differences in response to the cocaine cues were indicated by the wide range of changes in craving (0–8.7). For more than half of the participants (6/11), the change in self-reported craving for cocaine exceeded 4.0 (range 4.3–to 8.7), but three participants reported no change in craving. There was no correlation between degree of cocaine craving and years of cocaine use (r = 0.012, n.s.) or amount of weekly cocaine use (r = 0.051, n.s.). There were no significant differences between sessions in self-reports of mood (3.8 ± 1.0 vs. 4.1 ± 1.0, t = 0.43, n.s.) or wakefulness (5.8 ± 0.5 vs. 5.9 ± 0.7, t = 0.47, n.s.).

Cocaine craving self-reports. Average time course of self-report of craving for cocaine during presentation of neutral (open squares) and cocaine (solid circles) cues. Note that self-reports of craving were approximately equal before presentation of the cues across both sessions and that craving tended to remain elevated throughout the 30-min cocaine cues presentation period.
PET Data
Table 1 lists the coordinates and Z-scores of the peak voxel in each region exhibiting significant changes in nrCMRglc across the two sessions. Data from four of the expected a priori regions, but none of the a priori comparison regions, reached the threshold criterion. As predicted, significant increases in nrCMRglc during the cocaine cues session relative to the neutral session were observed in the DLFPC (right superior frontal gyrus, BA 9), left lateral OFC (BA 12/47), and right cerebellum. Activation was also present in an area of the left anterior temporal cortex that encompassed both the ventrolateral aspect of the amygdala and surrounding rhinal (entorhinal and perirhinal) cortex. Because the borders between the rhinal cortex and amygdala or individual nuclei within the amygdala cannot be distinguished given the limits of resolution of the scanner used, this region of activation is hereafter collectively labeled as amygdala/rhinal cortex. Significant decreases in nrCMRglc during the cocaine cues session were observed in a region of DLPFC (a priori region, left medial prefrontal cortex, BA10m) and in the ventromedial frontal pole (BA10r), for which we did not have an a priori hypothesis.
Table 2 shows the coordinates and Z-scores of the peak voxel in regions that exhibited significant correlations between brain activations and self-reports of cocaine craving. Positive correlations with craving were observed in four brain regions that also exhibited activations during the cocaine cues session: right DLPFC (superior frontal gyrus; BA 9), left lateral OFC (BA 12/47), left insula (BA13), left amygdala/rhinal cortex. In addition, a correlation between craving and activation of the anterior cingulate was present at a lower threshold (Z = 2.32, r = 0.74, p < .01). None of the a priori regions exhibited negative correlations with craving, including the comparison regions. Three other regions, however, that had not been selected a priori also exceeded the threshold criteria: negative correlations were present in the right retrocalcarine gyrus and right pons and a positive correlation was present in the superior temporal gyrus. These correlations did not remain significant after correction for multiple comparisons. Figures 2 and 3 show brain images of regional activations, deactivations, and correlations between activations and craving.

Statistical parametric maps of changes in nrCMRglc across sessions and correlations with craving. Regions of activation during the cocaine cues session are shown in red, and areas of deactivation are shown in blue (threshold, 10 contiguous voxels at p < .005, uncorrected). Regions where changes in self-report of craving for cocaine were positively correlated with changes in nrCMRglc are shown in green (threshold, 10 contiguous voxels at r > 0.82, p < .001, uncorrected). Note overlap of activation and correlations in the DLPFC, orbitofrontal cortex, and anterior ventromedial temporal lobe (rhinal cortex).

Statistical parametric maps of positive correlation of self-report of craving for cocaine with changes in nrCMRglc (threshold, 10 contiguous voxels at r > 0.82, p < .001, uncorrected). Crosshairs (blue) are centered on the peak voxel. The activation in the anterior medial temporal lobe can be most clearly seen in saggital plane (top image) as extending down from the ventral portion of the left amygdala into the surrounding rhinal cortex. Regions of correlation are also visible in the left OFC in the saggital section (top) and the left insula in the coronal section (bottom).
DISCUSSION
Cocaine-related stimuli, consisting of visual cues and an evocative script, elicited an increase in self-reports of craving for cocaine and increased brain activations in left amygdala/rhinal cortex, left lateral OFC, right superior frontal cortex, and right cerebellum. Deactivations during the cocaine session occurred in the left frontal pole and left medial prefrontal cortex. The regional pattern of brain activation closely paralleled the correlations between cue-induced changes in brain metabolism and craving. Consistent with our a priori predictions, self-reports of craving correlated positively with activity in right superior frontal cortex, left lateral OFC, and left amygdala/rhinal cortex as well as the left posterior insula. Because none of the a priori defined comparison regions exhibited significant metabolic changes, it is unlikely that the observed effects are due to false positives or reflect generalized brain activation in response to the cocaine cues. The deactivations in the frontal pole are more difficult to interpret. One likely possibility is that the deactivations may have been an artifact of the fixed order design and represent habituation to the experimental environment (Stapleton et al. 1997). On the other hand, a number of studies have shown deactivations of the frontal pole during the transition from a “resting” condition to a “task condition” (Binder et al. 1999; Christoff and Gabrieli 2000), which may be similar to the transition in the present study from the neutral cues session to the cocaine cues session.
The results presented here show substantial overlap with the regional changes reported in previous studies of brain activation during cocaine craving (Breiter et al. 1997; Childress et al. 1999; Garavan et al. 2000; Grant et al. 1996; Kilts et al. 2001; Maas et al. 1998; Volkow et al. 1999; Wang et al. 1999; Wexler et al. 2001). Inconsistencies between studies likely reflect methodological differences in image acquisition (PET with either 18F-FDG or 15O-H2O; fMRI-BOLD), data analysis (regions of interest vs. pixel-by-pixel, absolute quantification vs. global normalization, correlations with self-reports of craving), craving induction (exposure to a narrative video, brief video imagery, script-driven imagery, and/or stimulant administration), and subject selection (open enrollment or prescreening for subjects with high craving responses). For example, anterior cingulate activation during cue-elicited drug craving has been reported in most other studies, including our prior study (Childress et al. 1999; Garavan et al. 2000; Grant et al. 1996; Kilts et al. 2001; Maas et al. 1998; Wexler et al. 2001). In the current study, a correlation between craving and activation of the anterior cingulate was present, but only at a threshold (p < .01) that does not reach statistical significance after our correction for multiple comparisons. Thus, the failure to detect changes in regions reported in previous studies may have reflected constraints on the statistical power of the analysis due to the limited sample size and number of scans in the present study.
Nonetheless, a remarkably consistent pattern of regional brain activation during the subjective state of cocaine craving emerges despite the many methodological differences among these studies. Those brain regions most consistently identified across studies are the following: DLPFC, OFC, anterior cingulate cortex, insular cortex, and amygdala. The challenge at this point is to explain the functional contribution of these different regions. We previously stressed that regions activated during exposure to cocaine cues are also activated in studies of memory. The regional activation that occurs during exposure to drug-related stimuli most likely is not unique to drug craving but instead constitutes a general circuit that integrates emotion and cognition in the representation and ongoing evaluation of incentive value (LeDoux 2000, Maddock 1999). The regions in this proposed network might share an interrelated set of functions that translate drug-related stimuli into a representation of the expected outcomes of drug use, including direct drug effects and psychosocial sequelae. This representation consists not only of the identity of the goal object but also its current value to the organism and how close the organism is to obtaining it. Thus, each node in this network might make a specific contribution to this multidimensional construct.
Of all the regions implicated in drug craving, the amygdala has attracted the most attention because of its prominent role in emotional responses and memories (Canli et al. 2000; LeDoux 2000). In the present study, activation of the amygdala occurred during exposure to cocaine cues and was correlated to cocaine craving, similar to results from other studies of cocaine craving (Childress et al. 1999; Grant et al. 1996; Kilts et al. 2001). Although the scatter inherent in PET and spatial smoothing during data analysis makes identification of specific nuclei activated by cocaine cues problematic, animal studies indicate that only specific parts of the amygdala play a critical role in drug-associated responses. Lesions of the basolateral nucleus of the amygdala prevents establishment of cocaine-conditioned place preference (Brown and Fibiger 1993) and abolishes the ability of cocaine cues to reinstate cocaine self-administration (Meil and See 1997; Whitelaw et al. 1996), even though the amygdala is not involved in the direct reinforcing effects of cocaine (Lyons et al. 1996; Whitelaw et al. 1996). The limited amygdala activation in the present study supports the contention that only particular regions of the amygdala mediate memories of stimuli associated with prior drug reinforcement (Kruzich and See 2001).
In the present investigation, the activations and correlations with craving in the anterior medial temporal lobe extended ventrally beyond the amygdala into the surrounding rhinal (perirhinal and entorhinal) cortex. In fact, the peak activations were in the rhinal cortex, not amygdala per se. Substantial data indicate that both the rhinal cortex and the amygdala contribute to the evaluation of drug-related cues. There are prominent reciprocal connections between the amygdala and the rhinal cortex (McDonald and Mascagni 1997). In human and nonhuman primates, rhinal cortical areas are critical to visual object recognition (Buckley and Gaffan 1998; Erickson and Desimone 1999; Mishkin et al. 1997; Murray 1996) and the integration of object memory with incentive motivation. Although the rhinal cortex does not set the reward value of the goal object (Thornton et al. 1998), it identifies environmental stimuli in terms of their established value. Recent data show that the activity of neurons in the rhinal cortex track the progress that an individual makes toward a reward by identifying how much work remains to be done to obtain the reward (Liu et al. 2000). Conversely, lesions of the rhinal cortex impair an animal's ability to modulate its efforts to obtain a reward, based on stimuli that provide information about the proximity of reward delivery (Liu et al. 2000). Overall, these investigations suggest that the rhinal cortex may participate in the maintenance of cocaine abuse by using environmental cues to set appropriate motivational levels for action.
Similar to the amygdala, the anterior cingulate is activated during most studies on cocaine craving and may be involved in the formation of emotional memories. In this study, activity in the anterior cingulate was correlated with the self-reports of craving, but only at a threshold (p < .01) that does not reach statistical significance after correction for multiple comparisons. Even so, the correlation in the anterior cingulate accounted for 50% of the variance (r = 0.74). The correlation of the anterior cingulate in this study may have been attenuated by wide subject inclusion criteria and subsequent variability in the level of craving elicited. In other studies in which strong activation of the anterior cingulate was reported, subjects were included only if they had exhibited robust craving responses during a screening session or had met criteria for current cocaine dependence (Childress et al. 1999; Garavan et al. 2000, Kilts et al. 2001, Maas et al. 1998; Wang et al. 1999, Wexler et al. 2001). It is possible that the inclusion of subjects in the current study who did not meet these criteria contributed to a lower level of activation in the anterior cingulate. The anterior cingulate has long been known to be important for emotional processing and executive control of cognition (Carter et al. 1999), especially with regard to motivated attention and allocation of attention. In human studies, activation of the anterior cingulate has been shown to correlate with recall of specific feelings presented in emotional films (Lane et al. 1998). Overall, these investigations suggest that the anterior cingulate plays a critical role in the maintenance of cocaine abuse through its ability to integrate the association between environmental cues and emotional states in which expectancy of a positive outcome has been repeatedly fulfilled.
Activation of regions that process the affective valence or reinforcement value of stimuli may not be sufficient to produce the experience or expression of cocaine craving, however. Damasio (1999) has suggested that the conscious recognition of an emotional sensation in the body involves a representation of the relationship between body and emotions in the insula, the major cortical target of visceral afferents. In other words, one does not “feel” an emotion until it has been processed in the insula. In the present study, activation of the insula was correlated with cocaine craving, and others have also reported activation of the insula during presentation of drug cues (Garavan et al. 2000; Sell et al. 2000; Wang et al. 1999). The insula also shares substantial reciprocal connections with the rhinal cortex (Burwell and Amaral 1998), and the “gut feelings” abusers have during craving may only be experienced as emotionally significant after information signaling occurs between these two brain regions. Although it has been posited that the physical sensations reported during craving are akin to being high on a drug (Childress et al. 1999), it is notable that the pattern of neural activity during cue-induced craving is not identical to the response after drug administration (Breiter et al. 1997; Grant et al. 1996; London et al. 1990). For example, striatal activity only seems to be related to craving after drug administration (e.g., cocaine or methylphenidate) (Breiter et al. 1997; Volkow et al. 1999). Damasio (1999) has suggested that perception of the body and one's internal milieu provide and represent one's first level of self-identity. As discussed in more detail below, the bodily sensations experienced during craving may reflect a variety of higher order cognitive and psychological processes rather than a simple replication of the pharmacological effects of drugs.
In contrast to the role of the aforementioned limbic regions in evaluating associations with past events, the OFC may participate in the creation and maintenance of expectations about possible outcomes by integrating experiential history with changing current events. Lateral OFC neurons are activated by both the expectation and delivery of reward (Elliott et al. 2000; Rolls 2000; Schultz et al. 2000). Neurons in the OFC are also active during presentation of stimuli associated with a reinforcer in a manner that directs behavior (Tremblay and Schultz 1999). Information flow between the lateral OFC and amygdala/rhinal cortex may be particularly critical during periods when the predictive reliability of stimuli associated with reward or the value of the reward itself is uncertain or undergoing change. The OFC and connected regions are active when an organism must decide between conflicting choices (Bechara et al. 2000; Elliott and Dolan 1998), such that activity of OFC increases with the degree of conflict in a decision (Rogers et al. 1999). Furthermore, interactions between the amygdala/rhinal cortex and OFC play a critical role in setting the incentive value of such stimuli and thereby the overall motivation state of the organism (Baxter et al. 2000; Gallagher et al. 1999; Schoenbaum et al. 2000). These results suggest that as long as outcomes do not satisfy the expectations of an organism, the OFC will be activated. The insula may play a contributing role because it is activated when violations of expectancy occur (Casey et al. 2000), suggesting that increased conflict involves an increase in somatic sensations.
Although it has been suggested that two behavioral syndromes often associated with OFC activation—craving for drugs (Grant et al. 1996; Maas et al. 1998; Wang et al. 1999; Volkow et al. 1999) and obsessive-compulsive disorder (OCD) (Breiter and Rauch 1996; McGuire et al. 1994; Perani et al. 1995; Rauch et al. 1997; Swedo et al. 1989)—represent parallel disorders (Volkow and Fowler 2000), these syndromes might better be characterized as the opposite consequences of emotional memories for which expectations do not accurately reflect reality. Drug craving, then, could represent the expectation of a positive outcome despite minimal reward and/or a large aversive outcome, whereas the obsessions of OCD could represent the expectation of a negative outcome despite minimal aversive results and/or a large positive outcome.
Once cocaine cues have been evaluated and positive expectations have been generated, a cocaine abuser may continue to focus on and plan to obtain reward-related goals (i.e., cocaine). The DLPFC may function to maintain and coordinate representations received from the other regions during cocaine craving. In this study as well as in our prior investigation, DLPFC activation was correlated with cocaine craving (Grant et al. 1996). It is notable that the portion of the DLPFC associated with craving (BA9) has strong anatomical links to the OFC (Ongur and Price 2000). It is well known that the prefrontal cortex is critical in planning for the future and in working memory. During tasks that require extensive monitoring of complex information within working memory, it is the DLPFC (rather than the ventromedial prefrontal cortex) that is activated (Barch et al. 1997; Curtis et al. 2000; Dagher et al. 1999; Hartley and Speer 2000; MacDonald et al. 2000; Stern et al. 2000). Involvement of DLPFC may be the mechanism by which multifactored cocaine cues are processed to hold the attention of abusers and produce a consistent craving response across a 30-min session.
In this study, our stimulus complex included a script designed to evoke emotions and memories associated with the cocaine experience. Emotionally intense memory has been characterized as “hot” memory (Metcalfe and Mischel 1999), whereas “cool” memory represents emotionally neutral contemplation. In this theory, hot and cool memory work in opposition to each other, so that under hot memory control, behavior becomes more reflexive than reflective. The addition of the script to the videotape and paraphernalia we used in our previous study (Grant et al. 1996) increased response scores to the questions of how much abusers craved, wanted, or needed cocaine, suggesting high functioning of hot memory systems. In the present sample, 6 of 11 abusers had changes in craving scores that ranged from 4.3 to 8.7 (mean = 5.1), much greater than the moderate (2.0–3.0) change scores typically seen in studies of induced craving. The induction of a high craving response in most of our subjects is notable because generally only one-third or fewer research participants have reported high levels of experimentally evoked craving (Avants et al. 1995).
Because abusers have personal experiences with the cocaine-related events described in the script, it is interesting that the patterns of activation similar to those that occur during craving are also seen during recall of autobiographical memories (Andreasen et al. 1995; Fink et al. 1996; Maguire and Mummery 1999). A key to understanding the phenomenon of craving may be derived from Andreasen and coworkers’ (1995) observation that recall of personal history “permits human beings to experience personal identity.” Although craving may appear to be driven only by the desire for cocaine or the feeling that the drug produces, an abuser ultimately may be seeking the positive personal identity that was experienced while high on cocaine. This view is consistent with the contention that cravings are metacognitive statements about desires to modify ongoing cognitive experience rather than statements about the desire for the physiological responses to drug use (Toneatto 1999). Behavioral therapy might therefore be useful in curbing cocaine craving, given the success in modifying behavioral outcomes of hot memory under a variety of cognitive experimental conditions (Metcalfe and Mischel 1999).
References
American Psychiatric Association. (2000): Diagnostic and Statistical Manual of Mental Disorders, Text Revision 4th Edition. Washington, DC, American Psychiatric Press, Inc.
Andreasen NC, O'Leary DS, Cizadlo T, Arndt S, Rezai K, Watkins GL, Ponto LL, Hichwa RD . (1995): Remembering the past: Two facets of episodic memory explored with positron emission tomography. Am J Psychiatry 152: 1576–1585
Ashburner J, Friston KJ . (1997): Spatial Transformation of Images. In Frackowiak RSJ, Friston KJ, Frith CD, Dolan RJ, Mazziotta JC (eds), Human Brain Function. New York, Academic Press, pp 43–58
Avants SK, Margolin A, Kosten TR, Cooney NL . (1995): Differences between responders and nonresponders to cocaine cues in the laboratory. Addict Behav 20: 215–224
Barch DM, Braver TS, Nystrom LE, Forman SD, Noll DC, Cohen JD . (1997): Dissociating working memory from task difficulty in human prefrontal cortex. Neuropsychologia 35: 1373–1380
Baxter MG, Parker A, Lindner CC, Izquierdo AD, Murray EA . (2000): Control of response selection by reinforcer value requires interaction of amygdala and orbital prefrontal cortex. J Neurosci 20: 4311–4319
Bechara A, Tranel D, Damasio H . (2000): Characterization of the decision-making deficit of patients with ventromedial prefrontal cortex lesions. Brain 123: 2189–2202
Binder JR, Frost JA, Hammeke TA, Bellgowan PSF, Rao SM, Cox RW . (1999): Conceptual processing during the conscious resting state: A functional MRI study. J Cog Neurosci 11: 80–93
Breiter HC, Rauch SL . (1996): Functional MRI and the study of OCD: From symptom provocation to cognitive-behavioral probes of cortico-striatal systems and the amygdala. Neuroimage 4: S127–S138
Breiter HC, Gollub RL, Weisskoff RM, Kennedy DN, Makris N, Berke JD, Goodman JM, Kantor HL, Gastfriend DR, Riorden JP, Mathew RT, Rosen BR, Hyman SE . (1997): Acute effects of cocaine on human brain activity and emotion. Neuron 19: 591–611
Brown EE, Fibiger HC . (1993): Differential effects of excitotoxic lesions of the amygdala on cocaine-induced conditioned locomotion and conditioned place preference. Psychopharmacology 113: 123–130
Buckley MJ, Gaffan D . (1998): Perirhinal cortex ablation impairs visual object identification. J Neurosci 18: 2268–2275
Burwell RD, Amaral DG . (1998): Cortical afferents of the perirhinal, postrhinal, and entorhinal cortices of the rat. J Comp Neurol 398: 179–205
Canli T, Zhao Z, Brewer J, Gabrieli JD, Cahill L . (2000): Event-related activation in the human amygdala associates with later memory for individual emotional experience. J Neurosci 20: RC99:1–5
Carter CS, Botvinick MM, Cohen JD . (1999): The contribution of the anterior cingulate cortex to executive processes in cognition. Rev Neurosci 10: 49–57
Casey BJ, Thomas KM, Welsh TF, Badgaiyan RD, Eccard CH, Jennings JR, Crone EA . (2000): Dissociation of response conflict, attentional selection, and expectancy with functional magnetic resonance imaging. Proc Natl Acad Sci USA 97: 8728–8733
Childress AR, Hole AV, Ehrman RN, Robbins SJ, McLellan AT, O'Brien CP . (1993): Cue reactivity and cue reactivity interventions in drug dependence. NIDA Res Monogr 137: 73–95
Childress AR, Mozley PD, McElgin W, Fitzgerald J, Reivich M, O'Brien CP . (1999): Limbic activation during cue-induced cocaine craving. Am J Psychiatry 156: 11–18
Christoff K, Gabrieli JDE . (2000): The frontopolar cortex and human cognition: Evidence for a rostralcaudal hierarchical organization with the human prefrontal cortex. Psychobiology 28: 168–186
Curtis CE, Zald DH, Pardo JV . (2000): Organization of working memory within the human prefrontal cortex: A PET study of self-ordered object working memory. Neuropsychologia 38: 1503–1510
Dagher A, Owen AM, Boecker H, Brooks DJ . (1999): Mapping the network for planning: A correlational PET activation study with the Tower of London task. Brain 122: 1973–1987
Damasio H . (1995): Human Brain Anatomy in Computerized Images. New York, Oxford University Press
Damasio A . (1999): The Feeling of What Happens: Body and Emotion in the Making of Consciousness. New York, Harcourt Brace & Company
Duvernoy HM . (1999): The Human Brain, 2nd Edition. New York, Springer-Verlag
Ehrman RN, Robbins SJ, Childress AR, O'Brien CP . (1992): Conditioned responses to cocaine-related stimuli in cocaine abuse patients. Psychopharmacology 107: 523–529
Elliott R, Dolan RJ . (1998): Activation of different anterior cingulate foci in association with hypothesis testing and response selection. Neuroimage 8: 17–29
Elliott R, Dolan RJ, Frith CD . (2000): Dissociable functions in the medial and lateral orbitofrontal cortex: Evidence from human neuroimaging studies. Cereb Cortex 10: 308–317
Erickson CA, Desimone R . (1999): Responses of macaque perirhinal neurons during and after visual stimulus association learning. J Neurosci 19: 10404–10416
Fink GR, Markowitsch HJ, Reinkemeier M, Bruckbauer T, Kessler J, Heiss WD . (1996): Cerebral representation of one's own past: Neural networks involved in autobiographical memory. J Neurosci 16: 4275–4282
Gallagher M, McMahan RW, Schoenbaum G . (1999): Orbitofrontal cortex and representation of incentive value in associative learning. J Neurosci 19: 6610–6614
Garavan H, Pankiewicz J, Bloom A, Cho JK, Sperry L, Ross TJ, Salmeron BJ, Risinger R, Kelley D, Stein EA . (2000): Cue-induced cocaine craving: Neuroanatomical specificity for drug users and drug stimuli. Am J Psychiatry 157: 1789–1798
Grant S, London ED, Newlin DB, Villemagne VL, Liu X, Contoreggi C, Phillips RL, Kimes AS, Margolin A . (1996): Activation of memory circuits during cue-elicited cocaine craving. Proc Natl Acad Sci USA 93: 12040–12045
Hartley AA, Speer NK . (2000): Locating and fractionating working memory using functional neuroimaging: Storage, maintenance, and executive functions. Microsc Res Tech 51: 45–53
Holmes A, Poline JB, Friston KJ . (1997): Characterizing brain images with the general linear model. In Frackowiak RSJ, Friston KJ, Frith CD, Dolan RJ, Mazziotta JC (eds), Human Brain Function. New York, Academic Press, pp 59–84
Kilts CD, Schweitzer JB, Quinn CK, Gross RE, Faber TL, Muhammad F, Ely TD, Hoffman JM, Drexler KP . (2001): Neural activity related to drug craving in cocaine addiction. Arch Gen Psychiat 58: 334–341
Kruzich PJ, See RE . (2001): Differential contributions of the basolateral and central amygdala in the acquisition and expression of conditioned relapse to cocaine-seeking behavior. J Neurosci 21: RC155:1–5
Lane RD, Reiman EM, Axelrod B, Yun LS, Holmes A, Schwartz GE . (1998): Neural correlates of levels of emotional awareness. Evidence of an interaction between emotion and attention in the anterior cingulate cortex. J Cogn Neurosci 10: 525–535
LeDoux JE . (2000): Emotion circuits in the brain. Annu Rev Neurosci 23: 155–184
Liu Z, Murray EA, Richmond BJ . (2000): Learning motivational significance of visual cues for reward schedules requires rhinal cortex. Nat Neurosci 3: 1307–1315
London ED, Cascella NG, Wong DF, Phillips RL, Dannals RF, Links JM, Herning R, Grayson R, Jaffe JH, Wagner HN Jr . (1990): Cocaine-induced reduction of glucose utilization in human brain. A study using positron emission tomography and [fluorine 18]-fluorodeoxyglucose. Arch Gen Psychiatry 47: 567–574
Lyons D, Friedman DP, Nader MA, Porrino LJ . (1996): Cocaine alters cerebral metabolism within the ventral striatum and limbic cortex of monkeys. J Neurosci 16: 1230–1238
Maas LC, Lukas SE, Kaufman MJ, Weiss RD, Daniels SL, Rogers VW, Kukes TJ, Renshaw PF . (1998): Functional magnetic resonance imaging of human brain activation during cue-induced cocaine craving. Am J Psychiatry 155: 124–126
MacDonald AW III, Cohen JD, Stenger VA, Carter CS . (2000): Dissociating the role of the dorsolateral prefrontal and anterior cingulate cortex in cognitive control. Science 288: 1835–1838
Maddock RJ . (1999): The retrosplenial cortex and emotion: New insights from functional neuroimaging of the human brain. TINS 22: 310–316
Maguire EA, Mummery CJ . (1999): Differential modulation of a common memory retrieval network revealed by positron emission tomography. Hippocampus 9: 54–61
Mai JK, Assheuer JK, Paxinos G . (1998): Atlas of the Human Brain. New York, Academic Press
McDonald AJ, Mascagni F . (1997): Projections of the lateral entorhinal cortex to the amygdala: A Phaseolus vulgaris leucoagglutinin study in the rat. Neuroscience 77: 445–459
McGuire PK, Bench CJ, Frith CD, Marks IM, Frackowiak RS, Dolan RJ . (1994): Functional anatomy of obsessive-compulsive phenomena. Br J Psychiatry 164: 459–468
Meil WM, See RE . (1997): Lesions of the basolateral amygdala abolish the abilityof drug associated cues to reinstate responding during withdrawal from self-administered cocaine. Behav Brain Res 87: 139–148
Metcalfe J, Mischel W . (1999): A hot/cool-system analysis of delay of gratification: Dynamics of willpower. Psychol Rev 106: 3–19
Mishkin M, Suzuki WA, Gadian DG, Vargha-Khadem F . (1997): Hierarchical organization of cognitive memory. Philos Trans R Soc Lond B Biol Sci 352: 1461–1467
Molchan SE, Sunderland T, McIntosh AR, Herscovitch P, Schreurs BG . (1994): A functional anatomical study of associative learning in humans. Proc Natl Acad Sci 91: 8122–8126
Murray EA . (1996): What have ablation studies told us about the neural substrates of stimulus memory. Semin Neurosci 8: 13–22
Ongur D, Price JL . (2000): The organization of networks within the orbital and medial prefrontal cortex of rats, monkeys and humans. Cereb Cortex 10: 206–219
Perani D, Colombo C, Bressi S, Bonfanti A, Grassi F, Scarone S, Bellodi L, Smeraldi E, Fazio F . (1995): [18F]FDG PET study in obsessive-compulsive disorder. A clinical/metabolic correlation study after treatment. Br J Psychiatry 166: 244–250
Poline JB, Holmes A, Worsley K, Friston KJ . (1997): Making statistical inferences. In Frackowiak RSJ, Friston KJ, Frith CD, Dolan RJ, Mazziotta JC (eds), Human Brain Function. Academic Press, New York, pp 85–106
Rauch SL, Savage CR, Alpert NM, Fischman AJ, Jenike MA . (1997): The functional neuroanatomy of anxiety: A study of three disorders using positron emission tomography and symptom provocation. Biol Psychiatry 42: 446–452
Rogers RD, Owen AM, Middleton HC, Williams EJ, Pickard JD, Sahakian BJ, Robbins TW . (1999): Choosing between small, likely rewards and large, unlikely rewards activates inferior and orbital prefrontal cortex. J Neurosci 19: 9029–9038
Rolls ET . (2000): The orbitofrontal cortex and reward. Cereb Cortex 10: 284–294
Schoenbaum G, Chiba AA, Gallagher M . (2000): Changes in functional connectivity in orbitofrontal cortex and basloateral amygdala during learning and reversal training. J Neurosci 20: 5179–5189
Schultz W, Tremblay L, Hollerman JR . (2000): Reward processing in primate orbitofrontal cortex and basal ganglia. Cereb Cortex 10: 272–283
Sell LA, Morris JS, Bearn J, Frackowiak RS, Friston KJ, Dolan RJ . (2000): Neural responses associated with cue evoked emotional states and heroin in opiate addicts. Drug Alcohol Depend 60: 207–216
Stapleton JM, Morgan MJ, Liu X, Yung BC, Phillips RL, Wong DF, Shaya EK, Dannals RF, London ED . (1997): Cerebral glucose utilization is reduced in second test session. J Cereb Blood Flow Metab 17: 704–712
Stern CE, Owen AM, Tracey I, Look RB, Rosen BR, Petrides M . (2000): Activity in ventrolateral and mid-dorsolateral prefrontal cortex during nonspatial visual working memory processing: Evidence from functional magnetic resonance imaging. Neuroimage 11: 392–399
Swedo SE, Schapiro MB, Grady CL, Cheslow DL, Leonard HL, Kumar A, Friedland R, Rapoport SI, Rapoport JL . (1989): Cerebral glucose metabolism in childhood-onset obsessive-compulsive disorder. Arch Gen Psychiatry 46: 518–523
Thornton JA, Malkova L, Murray EA . (1998): Rhinal cortex ablations fail to disrupt reinforcer devaluation effects in rhesus monkeys (Macaca mulatta). Behav Neurosci 112: 1020–1025
Toneatto T . (1999): A metacognitive analysis of craving: Implications for treatment. J Clin Psychol 55: 527–537
Tremblay L, Schultz W . (1999): Relative reward preference in primate orbitofrontal cortex. Nature 398: 704–708
Tulving E, Habib R, Nyberg L, Lepage M, McIntosh AR . (1999): Positron emission tomography correlations in and beyond medial temporal lobes. Hippocampus 9: 71–82
Volkow ND, Fowler JS . (2000): Addiction, a disease of compulsion and drive: Involvement of the orbitofrontal cortex. Cereb Cortex 2000 10: 318–325
Volkow ND, Wang GJ, Fowler JS, Hitzemann R, Angrist B, Gatley SJ, Logan J, Ding YS, Pappas N . (1999): Association of methylphenidate-induced craving with changes in right striato-orbitofrontal metabolism in cocaine abusers: Implications in addiction. Am J Psychiatry 156: 19–26
Wang GJ, Volkow ND, Fowler JS, Cervany P, Hitzemann RJ, Pappas NR, Wong CT, Felder C . (1999): Regional brain metabolic activation during craving elicited by recall of previous drug experiences. Life Sci 64: 775–784
Wexler BE, Gottschalk GH, Fulbright RK, Prohovnik I, Lacadie CM, Rounsaville BJ, Gore JC . (2001): Functional magnetic resonance imaging of cocaine craving. Am J Psychiat 158: 86–95
Whitelaw RB, Markou A, Robbins TW, Everitt BJ . (1996): Excitotoxic lesions of the basolateral amygdala impair the acquisition of cocaine-seeking behaviour under a second-order schedule of reinforcement. Psychopharmacology 127: 213–224
Acknowledgements
The authors wish to thank Drs. Alane Kimes, Herb Weingartner, Brian Knutson, and B. Potrezebie for their useful comments on this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bonson, K., Grant, S., Contoreggi, C. et al. Neural Systems and Cue-Induced Cocaine Craving. Neuropsychopharmacol 26, 376–386 (2002). https://doi.org/10.1016/S0893-133X(01)00371-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1016/S0893-133X(01)00371-2
Keywords
This article is cited by
-
The anterior insula and its projection to amygdala nuclei modulate the abstinence-exacerbated expression of conditioned place preference
Psychopharmacology (2024)
-
Modulation of methamphetamine memory reconsolidation by neural projection from basolateral amygdala to nucleus accumbens
Neuropsychopharmacology (2023)
-
A sex-dependent role for the prelimbic cortex in impulsive action both before and following early cocaine abstinence
Neuropsychopharmacology (2021)
-
Noradrenergic correlates of chronic cocaine craving: neuromelanin and functional brain imaging
Neuropsychopharmacology (2021)
-
The changing opioid crisis: development, challenges and opportunities
Molecular Psychiatry (2021)
