
Abstract
We have shown previously that the most common point mutation in the RBI gene in retinoblastoma tumours is a C→T transition and that the majority of these occur in CGAarg codons. As a result of this mutation, a TGAstop codon is generated directly. We have analysed the 14 CGAarg codons in the RB1 gene for mutations in 113 patients with bilateral retinoblastoma. At 6 of these sites, C→T mutations in CGA codons alter a restriction enzyme site which makes their identification relatively straightforward. It was necessary, however, to analyse the other 8 CGA codons using single-strand conformation polymorphism (SSCP) analysis. A total of 18 C→T mutations were found, which represents 16% of all patients. Of these 13 (73%) were at two particular CGA codons in exon 8 (codon 251) and exon 17 (codon 552). During the course of the SSCP analysis, mutations were identified in 7 other individuals. Thus, 20–25% of all mutations can be identified by a relatively quick survey of the CGA codons in the RB1 gene, which has important implications for genetic screening programmes. All of the mutations in the RB1 gene in these bilaterally affected patients would be predicted to result in the absence of a functional protein.
Similar content being viewed by others

Introduction
As a result of the cloning of the retinoblastoma (Rb) gene, it is now possible to predict which individuals in the population are at risk for tumour development. Approximately 12–15% of patients with Rb already have a family history, where the tumour phenotype segregates as an autosomal dominant trait with high (90%) penetrance [1]. For these individuals, predicting who is at risk can be achieved using linked RFLP markers [2, 3], a procedure which can also be performed prenatally [4, 5]. Given the large numbers of polymorphic markers within the RB 1 gene, the majority of families can be offered genetic counselling. It is now well established that both copies of the RBI gene must be inactivated for tumour initiation [6–10] and that predisposed individuals carry heterozygous mutations in their constitutional cells [9, 11–13]. These individuals will usually develop bilateral, multifocal tumours at an earlier age than sporadic cases [14]. Approximately 50% of all Rb patients have multifocal tumours and, therefore, presumably, carry predisposing mutations. By identifying these constitutional mutations it would be possible to offer prenatal screening to these patients for their first-born child.
With the characterisation of the genomic structure of RB1 [15], it was shown to have 27 individual exons which were all relatively small and, following sequencing of the intron regions flanking each of the 27 exons [16], it became possible to analyse the coding region of the gene, exon by exon, using PCR and DNA sequencing to identify the mutations predisposing to tumourigenesis. This was first demonstrated by Yandell et al. [10] although others analysed the mRNA in tumours using RNAase-protection techniques [7, 8]. We chose to prescreen individual exons using single-strand conformation polymorphism (SSCP) analysis [9, 12, 13]. In our recent study of Rb tumours [9], we showed that approximately 80% of mutations result in the generation of premature stop codons. Many of these are a result of small deletions or insertions which produce frameshifts, but 30% resulted from single base pair changes. At present, however, there does not seem to be any single exon more frequently involved in mutation than the others, which has made screening bilaterally affected individuals to identify the causative mutation a tedious and time-consuming task. The majority of point mutations in our study of tumours [9] were C→T transitions occurring in CGA codons specifiying the arginine amino acid. As a result of these changes, a TGA stop codon is generated. Within the 928 amino acids of the RBI gene there are 46 arginine codons but only 14 of these are encoded by CGA which are distributed in only 10 different exons. In order to speed up the screening process, we have investigated whether the high frequency of CGA→TGA changes seen in tumours is also found in germline mutations in individuals predisposed to Rb. To this end we analysed the 14 CGA sites from 113 bilaterally affected individuals, with and without a family history, using a combination of PCR and SSCP analysis.
Materials and Methods
Blood samples were collected in lithium heparin tubes and DNA prepared from isolated white cells using standard phenol/chloroform procedures [17]. PCR primers for the amplification of all 27 exons of RB1 were as described by Hogg et al. [9] and prepared by the ICRF central oligonucleotide facility. PCR amplification for SSCP analysis was as described by Hogg et al. [12] where a32dCTP was used to incorporate radioactivity directly into the PCR product. SSCP was carried out on 6% Polyacrylamide, non-denaturing gels containing glycerol [12], Sequencing of PCR products was achieved using biotinylated primers and streptavidin-coated magnetic beads to recover single-stranded DNA which was then sequenced with Sequenase [12]. When the PCR products were subjected to restriction enzyme digestion, 20 of the PCR reaction was removed and 10 U of the appropriate enzyme added directly. The digestion proceeded at 37 or 65 °C (TaqI) for 2 h before the results were analysed on a 2% agarose gel.
Results
There are 14 CGA codons in the RB1 gene (fig. 1). To investigate these codons the relevant coding regions were amplified from genomic DNA using PCR. Six of these codons occur within the DNA sequence which would be recognised by restriction enzymes. Mutations within these codons would alter the recognition site which proved to be a convenient and easy way of identifying them. In all, 113 bilaterally affected patients were analysed. The patients were chosen because of the expectation that they would all be carriers of germline mutations [18] and Southern blot analysis using HindIII digestion had failed to show any structural aberrations in the RB1 gene (data not shown). In some cases there was a family history of retinoblastoma. Where a restriction enzyme site would not be affected by a mutation the exon was analysed using SSCP.

Location of the 14 CGAarg codons, by exon, in the RBI gene. The CGA codons are identified by their number (below) and where a restriction enzyme site contains the CGA sequence it is indicated by the solid bar above the sequence. In exon 14 the arginine codon is the first in the exon and the intron sequences in this case are indicated by the lower case letters. In exon 18, the CGAarg codon affects an AvaII site and the location of the other AvaII site not interrupting a CGA codon is shown to demonstrate its proximity (see text).
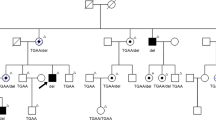
No mutations were found in the CGA sites in exons 1, 11, 14, 15 or 27. There are 2 CGA sites in exon 8, the first of which (codon 251) disrupts a TaqI site which makes this a relatively easy mutation to identify. Using the primers described previously [12] a 315-bp fragment is amplified and, if the mutation is not present, enzyme digestion yields two fragments, 204 and 111 bp long (fig. 2). Mutations were identified in 7/113 patients all of which were confirmed by sequencing. Four of these mutations occurred in individuals with a family history of Rb (fig. 2) and so this enzyme analysis was used to demonstrate that only affected members of the families carried the mutation. The second CGA (codon 255) in exon 8 is 13 bp downstream of the TaqI site (fig. 1) but does not form part of a restriction enzyme site. A search for mutations in this CGA codon, therefore, required SSCP analysis and only one example was found.

Identification of mutations in codon 251 using TaqI digestion in two Rb families. The marker lanes contain a 1-kb ladder. In lanes 1–3 PCR products have been digested with TaqI which produces two bands 204 and 111 bp long. Two families carrying C→T mutations in codon 251 are indicated in lanes 4–6 (family H) and 7–10 (family G). All of the affected individuals in these families carry the undigested 315-bp fragment because of the C → T mutation.
The CGA codon at position 320 in exon 10 can only be identified on SSCP gels and, in our epxerience, produces only a very subtle band shift even if the gel is run for 6 h. Only one mutation was found at this location in this series (table 1).
A mutation in the CGA site in exon 11 (codon 358) creates an NlaIII site. For a normal sequence the 265-bp PCR fragment can be digested to fragments 210 and 55 bp long. However, if the C→T mutation is present then three fragments are produced 110, 100 and 55 bp long and an extra band is seen corresponding to the 110/100 doublet. No mutations were found in this exon in this series.
Exon 17 also contains two CGA sites, one of which (codon 557) is incorporated into a TaqI site. The other CGA is 12 bp upstream (fig. 1). Since there are two TaqI sites in the normal PCR product, on digestion, fragments 212, 80 and 71 bp long are generated. If the TaqI site involving the CGAarg is destroyed, an extra band 151 bp (71 + 80) long is seen which can also be seen easily using SSCP.
The CGA site in exon 18 (codon 579) is located within an AvaII site but another AvaII site is located 10 bp upstream which does not involve a CGA codon. Digesting the PCR product with AvaII produces 2 bands which run closely together on a 2% agarose gel and so it is not easy to identify mutations in this way. On an SSCP gel, the band shifts are subtle and their detection is further complicated by the presence of a polymorphic site in this exon. It is possible, however, to detect the C→T mutation on a denaturing gel where direct incorporation of 32P-CTP during the PCR reaction means that, following autoradiography of the urea gel, the position of the mutant band can be clearly seen (fig. 3). Normally, digestion of the 220-bp product with AvaII produces bands 115, 95 and 10 bp long, although the 10-bp fragment is not seen on the gel. When the C→T mutation is present, a band 105 bp long is seen in heterozygotes lying between the two other bands (fig. 3). Three mutations were found in this exon at this site in our series as well as three mutations at other sites (table 1).

DNA sequencing gel carrying the PCR products from exon 18 digested with AvaII. DNA fragments not carrying the CGAarg mutation show two bands at 115 and 95 bp. Patient 45, carrying a C→T mutation, produces an extra band 105 bp long (see text).
The only CGA site in exon 23 is in codon 787 which is easy to analyse, since a TaqI site is disrupted by a C→T mutation in this codon. The 416-bp fragment is normally digested by TaqI to fragments 336 and 90 bp long. The 416-bp fragment is retained if the C→T change is present. Only one mutation was found at this site.
During the course of this survey, we also identified several bandshifts on the SSCP gels which did not affect the CGA sites. A summary of all the mutations found in this series of experiments is shown in table 1. Consistent with our previous findings [9] direct repeats were present at the junction of the deletions seen in patients TS28 and TS64. In patient TS72, the insertion was a direct repeat of 7 nucleotides whereas in patient TS76 the 2-bp insertion followed a run of AT repeats (fig. 4).

Summary of mutations not involving CGAarg codons in the series of 113 Rb patients. In all cases the normal sequence is shown above and the mutant sequence below. In the two deletions (TS28 and TS64) the perfect repeats at the breakpoints are shown in boxes. The 7-bp insertion in TS72 is also a direct repeat (boxes). In TS76 and TS94 the lower case letters represent the intron sequences and the exon sequences are in capitals.
Discussion
A number of different experimental approaches have been used to identify mutations in the RB1 gene with varying success. RNase protection proved useful in the analysis of some tumour cell lines [7, 8] but, using this technique, mutations in constitutional cells were not found. It was suggested that mutant mRNAs are not as stable as the normal transcript and so could not be identified. We also found this to be the case when using PCR analysis of mRNA from constitutional cells from patients carrying known mutations [19]. Direct sequencing of the 27 individual exons of the RB1 gene [10] successfully identified germline mutations but this is a laborious procedure. More recently, methods of pre-screening the individual exons have been used which have allowed more extensive searches for mutations. The SSCP analysis has proved very successful in our hands [9, 12, 13] although chemical mismatch procedures were favoured by others including the denaturant gradient gel electrophoresis (DGGE) [11] and HOT [20] techniques. If conclusions are to be drawn about the efficiency of these techniques, however, then all of the exons in all of the patients must be analysed. Whilst our analysis of tumours [9] followed this requirement, only selected exons were screened in other studies [11, 20].
The majority of RBI mutations in Rb patients published so far, with a few exceptions, result in the generation of nonsense mutations which is consistent with the observation that tumour cells rarely contain the Rb protein. Until now, however, there has been no evidence of a mutational hotspot within the gene. We have shown here that the CGAarg codons in exons 8 and 17 account for 10–15% of all mutations in hereditary cases. Clearly this has important implications for screening programmes since these sites should now become the first ones to be analysed. Where the mutation affects a restriction enzyme site, the analysis becomes unequivocal and easy. Clearly, where the single CGA codon affects a restriction enzyme site, as in exon 23, other mutations in these exons will not be detected. In fact, we have since identified other mutations in exon 23 using SSCP from individuals in this series of 113 patients. Although disruption of an enzyme site is easy to detect, there was no evidence in our study that these mutations were preferentially identified over those identified as band shifts on SSCP gels. Thus, although in exon 8 seven of the eight mutations involved the CGA in the TaqI site, the reverse was true for exon 17 where only 1/5 of the mutations destroyed the TaqI site. Although some of the CGA sites in RB1 can be studied using restriction enzymes alone, it is preferable to perform SSCP analysis for all the exons since, for relatively little extra effort, other mutations not affecting these codons could also be identified. This is particularly true for exons 8, 17 and 27 where only one of the CGA sites affects a restriction enzyme site so SSCP must be used anyway. In exons 8 and 17, mutations at only one CGA can be identified by TaqI digestion. SSCP is still required to identify mutations in the other one. Thus only 4 of the CGA coding exons can be identified.
Some mutations, however, are difficult to identify on SSCP gels because the resultant band shifts are very subtle and experience in reading these gels is essential. This is particularly true of the CGA sites in exon 10 and 11. Although no mutations were found at the CGA sites in exons 11, 14 and 15 in this series, we have previously reported mutations which were indentified in these positions using SSCP [9, 12] and Yandell et al. [10] also reported mutations in CGA codons in exons 11 and 14. This further demonstrates that mutations at these sites are not being missed using this technique. There is, however, variation in the quality of SSCP gels depending on local conditions in the experimental procedure and in many cases where we felt that the banding profile obtained could not be interpreted the samples were rerun. Thus, whilst we feel confident that most mutations will be detected by SSCP, we cannot, as yet, exclude the possibility that some were missed. Curiously, in the survey of 80 bilaterally affected individuals reported by Blanquet et al. [11], even though exons 11, 14 and 18 were analysed, no mutations in any of the CGA codons in these exons were observed. Although this was only a limited survey of the exons, it is surprising in the light of our findings and may point to the limited usefulness of DGGE in the analysis of RB1.
An important consideration in this type of study is, whether, having found what appears to be a gene-inactivating mutation, it is worthwhile screening the remaining exons in the gene or more efficient to move on to other patients. In our previous survey of late-onset, unilateral unifocal tumours where homozygous mutations were identified early in the study, we nonetheless analysed all of the remaining exons and in no case were any additional mutations found. We feel sure, therefore, that it is unnecessary to continue screening the RB gene once a logical mutation has been found. The majority of single-base-pair polymorphisms have now been recorded and so these should not be confused with gene-inactivating mutations although they can complicate the analysis of the SSCP gels, for example [13]. Since a nonsense mutation anywhere in the gene would be predicted to result in the absence of a functional protein, it is not clear why exons 8 and 17 are most frequently involved or why mutations in these CGA codons are more frequent than in others.
Our analysis of deletions and insertions in this study shows that direct repeats occur at the breakpoints as we had noticed previously [9], which supports the idea that these mutations arise as a result of errors during replication. In one patient, however, a missense mutation was found in exon 17. We have previously suggested that missense mutations are associated with familial Rb where the affected individuals only have a ‘mild’ form of the disease such as regressed tumours or carry the mutation but are unaffected [21]. Patients in these families, however, do sometimes develop bilateral multifocal tumours. It is possible in these cases that, instead of the (‘weak’) mutation being duplicated through mitotic recombination or non-dysjunction as often happens in 70% of Rb tumours [6], the second mutation in the homologous normal gene is a nonsense mutation and in combination with the missense mutation produces a more severe phenotype. Evidence for this mechanism has been provided by Dryja et al. [22] who were able to show that the ‘weak’ germline mutation in a low-penetrance family was not duplicated in the tumour analysed but rather a nonsense mutation was found in the homologous gene. This may be the case for patient TS23 who had bilateral, multifocal tumours. Alternatively, it may be that it is the position of the missense mutations in the RB1 gene that is important for its effect. Thus, the mild (arginine to tryptophan substitution) mutation reported by Onadim et al. [21] occurred in exon 20 and has since been shown to have some, albeit weaker, properties of the wild-type gene [19]. In patient TS23, the missense mutation is in exon 17 which is part of the protein-binding domain of RB1 [23]. Another missense mutation in exon 21 (a cysteine to phenylalanine substitution) was identifed in a small cell lung cancer cell line [24] which is also in the protein-binding domain but which, unlike the exon 20 mutation, abolishes the function of the Rb protein. Yandell et al. [10] also reported a serine to leucine missense mutation in exon 18 from an Rb tumour from a patient who was affected bilaterally. All of these mutations fall within the region of the protein responsible for binding other endogenous and viral proteins. Blanquet et al. [11], however, reported a germline missense mutation in exon 4 which was the same exon as that described in a low-penetrance family by Dryja et al. [22]. Clearly it is the nature of the mutation rather than its location which appears to be important in generating this phenotype. It remains to be seen what effect the TS23 mutation has on gene function, but the identification of this and other missense mutations will possibly improve our understanding of RB1 gene action.
References
Vogel F: Genetics of retinoblastoma. Hum Genet 1979;52:1–54
Wiggs J, Nordenskjeld M, Yandell D, Rapaport J, Grondin V, Janson M, Werelius B, Petersen R, Craft A, Riedel K, Lieberfarb R, Walton D, Wilson W, Dryja TP: Prediction of the risk of hereditary retinoblastoma using DNA polymorphisms within the retinoblastoma gene. New Engl J Med 1988;318:151–157
Onadim ZO, Mitchell CD, Rutland PC, Buckle BG, Jay M, Hungerford JL, Harper K, Cowell JK: Application of intragenic DNA probes in prenatal screening for retinoblastoma gene carriers in the United Kingdom. Arch Dis Child 1990;65:651–656
Mitchell CD, Nicolaides K, Kingston J, Hungerford J, Jay M, Cowell JK: Prental exclusion of hereditary retinoblastoma. Lancet 1988;i:826.
Onadim Z, Hungerford J, Cowell JK: Follow-up of retinoblastoma patients having prenatal and perinatal predictions for mutant gene carrier status using intragenic polymorphic probes from the RB1 gene. Br J Cancer 1992;65:711–716
Cavenee WK, Dryja TP, Phillips RA, Benedict WF, Godbout R, Gallie BL, Murphree AL, Strong LC, White RL: Expression of recessive alleles by chromosomal mechanisms in retinoblastoma. Nature 1983;305:779–784
Dunn JM, Phillips RA, Becker AJ, Gallie BL: Identification of germline and somatic mutations affecting the retinoblastoma gene. Science 1988;241:1797–1800
Dunn JM, Phillips RA, Zhu X, Becker A, Gallie BL: Mutations in the RB1 gene and their effects on transcription. Mol Cell Biol 1989,9:4596–4604.
Hogg A, Bia B, Onadim Z, Cowell JK: Molecular mechanisms of oncogenic mutations in tumours from patients with bilateral and unilateral retinoblastoma. Proc Natl Acad Sci USA 1993;90:7351–7355
Yandell DW, Campbell TA, Dayton SH, Petersen R, Walton D, Little JB, McConkie-Rosell A, Buckley EG, Dryja TP: Oncogenic point mutations in the human retinoblastoma gene: Their application to genetic counselling. New Engl J Med 1989;321:1689–1695
Blanquet V, Turleau C, Gross MS, Goossens M, Besmond C: Identification of germline mutations in the RB1 gene by denaturant gradient gel electrophoresis and polymerase chain reaction direct sequencing. Hum Mol Genet 1993;2:975–979
Hogg A, Onadim Z, Baird PN, Cowell JK: Detection of heterozygous mutations in the RB1 gene in retinoblastoma patients using single-strand conformation polymorphism, analysis and polymerase chain reaction sequencing. Oncogene 1992;7:1445–1451
Onadim Z, Hogg A, Cowell JK: Mechanisms of oncogenesis in patients with familial retinoblastoma. Br J Cancer 1993;68:958–964
Draper GJ, Sanders BM, Brownbill PA, Hawkins MM: Patterns of risk of hereditary retinoblastoma and applications to genetic counselling. Br J Cancer 1992;66:211–219
Friend SH, Horowitz JM, Gerber MR, Wang XF, Bogenmann E, Li FP, Weinberg RA: Deletions of a DNA sequence in retinoblastomas and mesenchymal tumours: Organization of the sequence and its encoded protein. Proc Natl Acad Sci USA 1987;84:9059–9063
McGee TL, Yandell DW, Dryja TP: Structure and partial genomic sequence of the human retinoblastoma susceptibility gene. Gene 1989;80:119–128
Sambrook J, Fritsch EF, Maniatis T: Molecular Cloning: A Laboratory Manual, ed 2. Cold Spring Harbor, Cold Spring Harbor Laboratory Press, 1989.
Knudson AG: Mutation and cancer: Statistical study of retinoblastoma. Proc Natl Acad Sci USA 1971;68:820–823
Kratzke RA, Hogg A, Otterson GA, Coxon AB, Geradts A, Cowell JK, Kaye FJ: Incomplete penetrance of familial retinoblastoma and benign retinal tumors associated with partial inactivation of the RB product. Oncogene 1994;9:1321–1326
Weir-Thompson E, Condie A, Leonard RCF, Presser J: A familial RB1 mutation detected by the HOT technique is homozygous in a second primary neoplasm. Oncogene 1991;6:2353–2356
Onadim Z, Hogg A, Baird PN, Cowell JK: Oncogenic point mutations in exon 20 of the RB1 gene in families showing incomplete penetrance and mild expression of the retinoblastoma phenotype. Proc Natl Acad Sci USA 1992;89:6177–6181
Dryja TP, Rapaport J, McGee TL, Nork TM, Schwartz TL: Molecular etiology of low-penetrance retinoblastoma in two pedigrees. Am J Hum Genet 1993;52:1122–1128
Hu Q, Dyson N, Harlow E: The regions of the retinoblastoma protein needed for binding to adenovirus E1A or SV40 large T antigen are common sites for mutation. EMBO J 1990;9:1147–1155
Kaye FJ, Kratzke RA, Gerster JL, Horowitz JM: A single amino acid substitution results in a retinoblastoma protein defective in phosphorylation and oncoprotein binding. Proc Natl Acad Sci USA 1990;87:6922–6926
Acknowledgements
BB is supported by a grant from the David Allen Retinoblastoma Fund.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Cowell, J.K., Smith, T. & Bia, B. Frequent Constitutional C to T Mutations in CGA-Arginine Codons in the RB1 Gene Produce Premature Stop Codons in Patients with Bilateral (Hereditary) Retinoblastoma. Eur J Hum Genet 2, 281–290 (1994). https://doi.org/10.1159/000472372
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1159/000472372
Key Words
This article is cited by
-
The management of retinoblastoma
Oncogene (2018)
-
Rapid detection of RB1 recurrent mutations in retinoblastoma by ARMS-PCR
Journal of Genetics (2016)
-
Advantages of a next generation sequencing targeted approach for the molecular diagnosis of retinoblastoma
BMC Cancer (2015)
-
Genetic screening in patients with Retinoblastoma in Israel
Familial Cancer (2015)
-
Novel mutations in the RB1 gene from Chinese families with a history of retinoblastoma
Tumor Biology (2015)
