
Abstract
We analyzed the FRAXAC2 and DXS548 microsatellites in normal and fragile X chromosomes from Sweden and the Czech Republic in order to investigate a possible founder effect for chromosomes carrying a fragile X mutation. We report a much stronger linkage disequilibrium between the marker haplotypes and the disease in Swedish fragile X chromosomes than in Czech and most other previously studied Caucasian populations. Two haplotypes accounted for 64% of Swedish fragile X chromosomes and for only 14% of normal chromosomes. Neither of these two haplotypes was found in Czech chromosomes, but the most common Swedish fragile X haplotype is the same as that reported to be predominant in Finnish fragile X patients. Linkage disequilibrium was observed in the Czech fragile X chromosomes but the haplotypes were more diverse and similar to those observed in other Caucasian populations. The most prevalent Swedish fragile X haplotype was traced back from affected males to common ancestors in the early 18th century. This indicates an apparently silent segregation of fragile X alleles through up to nine generations. The geographical distribution of the two major at-risk haplotypes in Sweden suggests that they were present among early settlers in different parts of the country.
Similar content being viewed by others
Introduction
The fragile X syndrome, the most common type of inherited mental retardation, is caused by the expansion of an unstable CGG repeat sequence located in a 5′ exon of the FMR1 gene [1–3]. The CGG repeat varies in length in the normal population with allele sizes ranging from 6 to 54 [4]. Two types of allele can be distinguished in fragile X families: a premutation (60–200 repeats) present in intellectually normal carriers and a full mutation (>200 repeats) present in fragile X patients [5]. The transition from premutation to full mutation occurs only when transmitted by a carrier female to her offspring, and the probability of the event depends on the size of the premutation [4, 6, 7]. Because observations of direct passage from a normal allele to a premutation are lacking, no mutation rate has been determined for the first premutation event. It has been speculated that premutated fragile X chromosomes may be passed through several generations before a full mutation occurs [8, 9]. Recent investigations using microsatellite markers FRAXAC1 and FRAXAC2 flanking the CGG repeat have shown haplotypes in linkage disequilibrium with fragile X mutations [10, 11]. Three haplotypes were found to be significantly overrepresented in Australian and US populations, accounting for 58% of fragile X chromosomes. Similar findings were reported from a French study where the markers FRAXAC2 and DXS548 showed two haplotypes overrepresented on fragile X chromosomes [12]. This suggests that certain chromosomes may be susceptible to develop the full mutation present in fragile X patients. The initial event(s) leading to a premutation has presumably occurred on a limited number of chromosomes and has remained silent over many generations. This is an unexpected finding in a relatively common X-lmked disease that decreases reproductive fitness [13].
We have used the microsatellite markers FRAXAC2 and DXS548 flanking the CGG repeat in Swedish and Czech populations to search for linkage disequilibrium. The FRAXAC2 marker is located only 10 kb distal, and DXS548 150 kb proximal to the CGG repeat [2, 10, 14]. We show that the putative founder effect in Sweden is much stronger than that observed in the Czech Republic and in other previously studied populations of central European origin [11,12]. Genealogical information and results of haplotype analysis were combined for a few affected individuals, allowing us to follow the mutation back through several generations of silent carriers. Our combined results indicate that the initial mutation events that create susceptibility to further expansion are rare, in agreement with the hypothesis of a founder effect.
Patients and Methods
Typing of CA repeats FRAXAC2 and DXS548, both highly informative microsatellites [2,10,14], was performed on a population of 28 Swedish and 15 Czech fragile X patients. The healthy chromosomes of their mothers or in some cases fathers or unrelated males were used as reference haplotypes. Close relationship between affected individuals was excluded, i.e. up to third or fourth cousin. The diagnosis of fragile X syndrome was made on the basis of clinical criteria, standard cytogenetic procedures and results of DNA analysis with the probe StB12.3 [15]. The polymerase chain reaction (PCR) was performed using oligonucleotide primers for the FRAXAC2 and DXS548 loci after end-labeling of one primer with 32P. Amplification by PCR was carried out simultaneously for the two loci as described by Oudet et al. [16]. The PCR products were diluted 1:25, denatured and separated on a 6% denaturing Polyacrylamide gel, with an M13mp18 sequence marker for sizing. Consistency of allele denomination was ensured by typing control DNAs used in previous studies [12, 16]. For calculations of statistical significance we used χ2 tests with correction for continuity.
Results
We haplotyped 28 Swedish normal and fragile X chromosomes as well as 20 normal and 15 fragile X chromosomes in the Czech Republic.
The apparent sizes of the FRAXAC2 alleles in our control sample extended from 146 to 153 bp and the alleles were separated by one nucleotide as reported recently by Zhong et al. [17]. The most frequent allele in the control populations was 150 bp (E allele). The polymorphism displayed a bimodal distribution (table 1). The apparent sizes of the DXS548 polymorphism extended from 192 to 204 bp in our controls. The alleles were separated by two base pairs with a bimodal distribution.
The distribution of normal alleles for the two markers was similar when comparing the Swedish and Czech populations. There were slight deviations, but the populations were too small to test whether such differences are significant between these two populations, and also in comparison to previously studied Australian, US and French populations [11, 12, 17]. In contrast, significant differences were observed when comparing the normal alleles and the alleles on fragile X chromosomes within both populations (table 1).
In both cohorts the major haplotypes on fragile X chromosomes were distinct from those on normal chromosomes. In the Swedish population 10 different haplotypes were observed on normal chromosomes and 7 on fragile X chromosomes (table 2). Similarly, the figures in the Czech population were 8 and 6, respectively. The two major haplotypes on control chromosomes, 149–194 (Dc) and 150–194 (Ec) were together observed at a frequency of 57% in Sweden and 70% in the Czech Republic.
In the Swedish cohort, the two most common fragile X haplotypes 147–194 (Bc) and 150–196 (Ed) were significantly more frequent than in controls. None of these were observed in the Czech material where three fragile X haplotypes, 147–196 (Bd), 149–204 (Dh) and 151–204 (Fh) were overrepresented and together significantly more frequent than in corresponding controls. Similarly, the 150–194 (Ec) haplotype is significantly underrepresented in both fragile X populations. In the Swedish population, the major fragile X haplotype 150–196 (Ed) accounted for 36%, and was found on only 11 % of normal chromosomes. The haplotype 147–194 (Be) was found on 29% of fragile X chromosomes but was observed only once (4%) in normal chromosomes. Taken together, the distribution of haplotypes on fragile X chromosomes in Sweden was significantly different from those observed in the Czech Republic (table 2). The two major haplotypes which constituted 64% of fragile X chromosomes in Sweden were not found in Czech chromosomes and represent only 1% of French chromosomes [12].
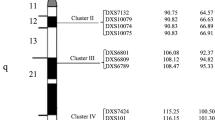
A founder effect was further supported by combining genealogical [8] and molecular analysis of fragile X patients from northern Sweden. Common ancestors of affected individuals with the 150–196 (Ed) haplotype were traced back to the early 18th century (fig. 1). This shows that the mutation has been carried over 8–9 generations of silent carriers.

Two pedigrees with alleles for loci FRAXAC2-DXS548 in individuals segregating for the fragile X syndrome. In each pedigree two affected individuals could be traced back through 7–9 generations to common ancestors living in the early 18th century. The identical haplotype in distantly related affected individuals suggests a silent premutation or a mutant carrier state through the generations.
The geographical distribution of the fragile X haplotype showed variations in Sweden. The predominant haplotype 150–196 (Ed) was seen on 86% of fragile X chromosomes originating from the northern half of Sweden (6 out of 7). The frequency differed significantly from that observed in the southern part where only 19% of fragile X chromosomes (4 out of 21) carried the 150–196 haplotype (p < 10−3). The second major haplotype in Sweden, 147–194 (Bc), was found predominantly in the southern half of the country where it is present on 38% of fragile X chromosomes (8 of 21). Southern Sweden also showed a more diverse mixture of haplotypes.
Discussion
The heritable unstable element responsible for the fragile X syndrome was recently demonstrated to be in linkage disequilibrium with flanking microsatellite alleles [11, 12, 16–18]. The existence of a founder effect for the fragile X syndrome was unexpected. Indeed, the fragile X syndrome reduces reproductive fitness of affected males and is found at a high frequency in many populations throughout the world [19]. A high mutation rate would thus be expected, as observed in other X-linked traits. The difference in frequency of the haplotypes on normal and fragile X chromosomes indicates a limited number of primary mutational events. This putative founder effect was tested in Swedish and Czech populations that share no recent demographic interaction. We have shown that the fragile X mutation in Sweden is associated with a stronger founder effect than that observed in the Czech Republic and previously reported for France [12]. Two major haplotypes account for 64% of Swedish fragile X chromosomes but only 14% of normal chromosomes. The two haplotypes were not found in any Czech patients and have previously been reported on only 1% of a French fragile X population [12]. By contrast, the distribution of haplotypes on fragile X chromosomes in the Czech population is more similar to that observed in France which might reflect a recent demographic interaction of the populations of central Europe, whereas the Scandinavian peninsula has remained more isolated.
Furthermore, we have demonstrated that the most prevalent fragile X haplotype in the Swedish population can be traced to common ancestors 8–9 generations back. This supports the assumption that the premutation can be carried through many generations by silent carriers. However, the initial event that produced the premutated founder chromosome must have occurred much earlier in history [13].
It has been suggested that part of the complexity observed for the haplotypes flanking the fragile X mutation may result from a higher mutation rate of the microsatellite markers compared to biallelic restriction fragment Length polymorphisms. Polymerase slippage has been proposed to account for the heterogeneity of fragile X haplotypes [12]. New mutations at the FRAXAC2 locus have indeed been reported [17] but have not been observed in our material. Furthermore, with a distance between the two markers of about 160 kb, recombination can occur, although at a very low frequency.
Mutations that alter the length of the CGG repeat at the FMR1 gene are likely to be rare but not unique events. A mutation rate of 2.5 × 10−4 has been suggested [13]. This would generate different risk haplotypes in different populations. Our results comparing fragile X and normal chromosomes between Sweden and the Czech Republic supports this hypothesis. One or a few founders in Sweden for the most prevalent fragile X haplotype 150–196 (Ed) is the most probable explanation, as the haplotype is apparently very rare on fragile X chromosomes in other populations. This haplotype could originally have arisen by single slippage from the 150–194 (Ec) allele which seems to be predominant in other Caucasian fragile X populations. The second most prevalent fragile X haplotype in Sweden, 147–194 (Bc), which has not been seen in other Caucasian populations studied, may have been derived through an ancient recombination event or may represent an independent mutational event at the CGG repeat. Interestingly, the most common haplotype, 150–196 (Ed), in the Swedish fragile X population is even more predominant in Finnish fragile X patients [17; J. Leisti, pers. commun.] indicating a common origin for part of the Swedish and Finnish fragile X patients.
The predominant population of the Scandinavian peninsula is thought to derive from two prehistorical immigrations, about 10,000 and 6,000 years ago. Since then, immigrations have taken place but of less numerical importance. A possible explanation for the haplotype differences within Sweden, with a more homogeneous pattern in the north, is that this region has had a small and stable gene pool with little demographic movement. The second predominant haplotype in the Swedish fragile X population, 147–194 (Bc), was probably present among early settlers in the southern part of the country. The more diverse haplotype pattern found in the south is probably due to additional founders of more recent arrival in Sweden, and these haplotypes are also found in a higher proportion in other Caucasian fragile X populations.
References
Kremer EJ, Pritchard M, Lynch M, et al: Mapping of DNA instability at the fragile X to a trinucleotide repeat sequence (CCG)n. Science 1991;252:1711–1714
Verkerk AJM, Pierreti M, Sutcliffe JS, et al: Identification of a gene (FMR-1) containing a CGG repeat coincident with a breakpoint cluster region exhibiting length variation in fragile X syndrome. Cell 1991;65:905–914
Yu S, Pritchard M, Kremer E, Lynch M, Nancarrow J, Baker E, Holman K, Mulley JC, Warren ST, Schlessinger D, Sutherland GR, Richards RI: Fragile X genotype characterized by an unstable region of DNA. Science 1991;252:1179–1181
Fu YH, Kuhl DPA, Pizzuti A, et al: Variation in the CGG repeat at the fragile X site results in genetic instability: Resolution of the Sherman paradox. Cell 1991;67:1047–1058
Oberlé I, Rousseau F, Heitz D, et al: Instability of a 550 base-pair DNA segment and abnormal methylation in fragile X syndrome. Science 1991;252:1097–1102
Yu S, Mulley J., Loesch D, et al: Fragile X syndrome: Unique genetics of the heritable unstable element. Am J Hum Genet 1992;50:968–980
Heitz D, Devys D, Imbert G, Kretz C, Mandel JL: Inheritance of the fragile X syndrome: Size of the fragile X premutation is a major determinant of the transition to full mutation. J Med Genet 1992;29:794–801
Drugge U, Blomquist HK, Gustavson KH, Holmgren G: Fragile X families in a northern Swedish county: A genealogical study demonstrating possibly affected individuals in the 19th century. Am J Med Genet 1991;38:363–366
Smits A, Smeets D, Hamel B, Dreesen J, van Oost B: High prevalence of the Fra(X) syndrome cannot be explained by a high mutation rate. Am J Med Genet 1992;43:345–352
Richards RI, Holman K, Kremer E, et al: Fragile X syndrome: Genetic localisation by linkage mapping of two microsatellite repeats FRAXAC1 and FRAXAC2 which immediately flank the fragile site. J Med Genet 1991;28:818–823
Richards RI, Holman K, Friend K, et al: Evidence of founder chromosomes in fragile X syndrome. Nature Genet 1992;1:257–260
Oudet C, Mornet E, Serre JL, et al: Linkage disequilibrium between the fragile X mutation and two closely linked CA repeats suggests that fragile X chromosomes are derived from a small number of founder chromosomes. Am J Hum Genet 1993;52:297–304
Morton NE, Macpherson JN: Population genetics of the fragile X syndrome: Multiallelic model for the FMR1 locus. Proc Natl Acad Sci USA 1992;89:4215–4217
Riggins G, Sherman S, Oostra BA, Sutcliffe J, Feitell D, Nelson D, van Oost B, Smits A, Ramos F, Pfendner E, Kuhl D, Caskey T, Warren S: Characterization of a highly polymorphic dinucleotide repeat 150 kb proximal of the fragile site. Am J Med Genet 1992;43:237–243
Rousseau F, Heitz D, Biancalana V, Blumenfeld S, Kretz C, Boué J, Tommerup N, Van der Hagen C, DeLozier-Blanchet C, Croquette MF, Gilgenkrantz S, Jalbert P, Voelckel MA, Oberlé I, Mandel JL: Direct diagnosis by DNA analysis of the fragile X syndrome of mental retardation. N Engl J Med 1991;325:1673–1681
Oudet C, von Koskull H, Nordstrom AM, Peippo M, Mandel JL: Striking founder effect for the fragile X syndrome in Finland. Eur J Med Genet 1993;1:181–189
Zhong N, Dobkin C, Brown T: A complex mutable polymorphism located within the fragile X gene. Nature Genet 1993;5:248–253
Hirst MC, Knight S, Christoudoulu Z, Grewal P, Fryns J, Davies K: Origins of the fragile X syndrome mutation. J Med Genet 1993;30:647–650
Sherman SL, Morton NE, Jacobs PA, Turner G: The marker (X) syndrome: A cytogenetic and genetic analysis. Ann Hum Genet 1984;48:21–37
Acknowledgements
We thank Dr. Eva Seémanova for clinical expertise. This study was supported by grants from the Swedish Medical Research Council, the Beijer Foundation, the Swedish Medical Society, the Swedish Institute, the Nilsson-Ehle Foundation and the Savstaholms Society.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Malmgren, H., Gustavson, KH., Oudet, C. et al. Strong Founder Effect for the Fragile X Syndrome in Sweden. Eur J Hum Genet 2, 103–109 (1994). https://doi.org/10.1159/000472350
Received:
Revised:
Issue Date:
DOI: https://doi.org/10.1159/000472350
