
Abstract
Huntington’s disease (HD) is associated with an expanded unstable (CAG)n repeat in the IT 15 gene. This repeat was investigated in 44 HD patients and 59 of their relatives at risk who were members of 29 unrelated families from various parts of Greece. Abnormal elongation of the (CAG)n repeat ranging from 39 to 95 trinucleotide units was found in all but one of the 44 HD patients tested with 70% of these patients showing 42–47 repeats. The size of the expanded sequence correlated inversely with the age at disease onset (r = 0.77, p < 0.00001, n = 43). In a single sporadic case, de novo expansion of the (CAG)n repeat was detected. Twenty-four of 59 asymptomatic family members at risk showed expansion of the (CAG)n repeat in the HD range (39–56 trinucleotide units) while three had intermediate alleles (36–37 repeats). Evaluation of the adjacent polymorphic (CCG)n repeat showed a strong linkage disequilibrium between the 7-unit (CCG)n repeat allele and the HD mutation, with 51% of normal and 93% of HD chromosomes showing this allele (χ2 = 15.55, p < 0.0001, n = 260). These data on HD patients of Greek origin are consistent with the thesis that the (CAG)n expansion is the primary gene defect of the disease and that this mutation occurred primarily on chromosomes with the (CCG)7 repeat haplotype.
Similar content being viewed by others

Introduction
Huntington’s disease (HD) is a dominantly inherited neurodegenerative disorder characterized by progressive choreic movements, oculomotor abnormalities, cognitive decline and emotional disturbances [1]. Recently, IT15, a gene located on the short arm of chromosome 4, has been identified and shown to contain a polymorphic CAG trinucleotide repeat in the 5′ end of its putative open reading frame that is abnormally elongated in HD chromosomes [2]. Studies on HD families from around the world [2–15], have shown that the size of elongated (CAG)n repeats correlates inversely with age at disease onset and that this correlation is stronger for patients whose disease started prior to 40 years of age.
We studied 29 families from various regions of Greece encompassing 472 family members, of whom 109 are known to be affected by HD. The CAG repeat was examined in DNA samples of 44 of these HD patients and 59 of their asymptomatic relatives at risk for developing the disease. In addition, a polymorphic (CCG)n repeat [13, 14], which is located on the IT15 gene in close proximity to the (CAG)n repeat, was also investigated. Our results are reported below.
Materials and Methods
Family histories were collected for patients from various parts of Greece with dominantly inherited choreic disease, and genealogical trees were constructed. The diagnosis of HD disease was based on conventional clinical criteria [1], positive family history and brain CT or MRI scans. Many of the families studied had been evaluated previously using RFLP analysis [16].
Genomic DNA was extracted from mixed leukocytes or lymphocytes isolated from peripheral blood using standard techniques [17]. For determining the (CAG)n repeat, the method described by the Huntington’s Disease Collaborative Research Group [2] was used. This involves PCR amplification in a 25-µl reaction volume in the presence of 50 µg genomic DNA, 5 ug of each primer, 200 µM of each dNTP, 2.5 µCi [32P]dCTP (New England Nuclear), 10% DMSO, 0.1 U Perfectmatch (Stratagene) and 1.25 U Amplitaq (Perkin Elmer). Forty cycles were carried out at 94°C for 1 min, 60°C for 1 min and at 72°C for 2 min. The last extension step was done at 72°C for 10 min. The PCR products were diluted with an equal volume of 95% formamide loading buffer. After heat denaturation at 95°C for 2–3 min, the radiolabeled PCR products were loaded on 6% Polyacrylamide gels and run for 4 h at a constant power of 100 W. An M13 DNA sequencing ladder was added for determining the size of the amplified repeats. Following electrophoresis, the gels were fixed for 30 min in a solution of 12% methanol/10% acetic acid, dried and revealed by autoradiography.
Because this PCR method [2] amplifies a part of the IT 15 gene which contains the (CAG)n repeat and an adjacent polymorphic (CCG)n repeat, the actual length of the (CAG)n repeat was estimated by taking into consideration the (CCG)n repeat length. Determination of the (CCG)n repeat only was carried out using the PCR primers and conditions described by Andrew et al. [13]. In addition to this indirect method, we also measured the (CAG)n repeat size directly by amplifying a segment of the IT15 gene that contains the (CAG)n repeat only as described by Warner et al. [18]. Results obtained with the two methods were comparable. The PCR products obtained by these methods were radiolabelled by incorporation of [32P]dCTP and resolved on a 6% denaturing Polyacrylamide gel as described above.
Results
The size of the HD (CAG)n and the (CCG)n repeat was obtained in 44 HD patients, 59 of their relatives at risk for developing this disease and 103 controls of Greek origin. Forty-three of these patients were members of 28 multigenerational HD families, while 1 had a negative family history (sporadic occurrence) and is considered to represent a de novo HD case. Both parents of this patient were alive and free of neurologic disease; DNA fingerprinting confirmed true paternity. Moreover, extensive evaluation of this patient’s pedigree, which included 55 family relatives, failed to reveal evidence for choreic disease in any of these individuals.
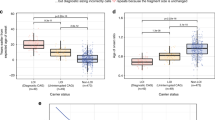
In control individuals, two alleles of the (CAG)n repeat ranging from 7 to 29 trinucleotide units (median = 19 repeats) were detected, in accordance with previously reported data on normal controls [2–12]. In contrast, all but one of the patients with dominantly inherited choreic disease had one elongated (CAG)n allele with 39–95 repeats (median = 45 repeats) and one normal allele with 13–26 repeats (median = 20 repeats) (fig. 1). In 70% (30/43) of HD patients, the size of the expanded allele ranged from 42 to 47 trinucleotide units, 25% (11/43) had more than 47 repeats and only 5% (2/43) had 39–41 repeats.

Histogram of the IT15 gene (C AG)n repeat of HD patients and asymptomatic family members at risk for developing this disease. Normal alleles contain 14–19 repeats and elongated (HD) alleles 39–95 repeats. Intermediate alleles, as defined by Myers et al. [9] and Goldberg et al. [10], containing 36–37 repeats, were observed in 3 at-risk individuals.
The patient with sporadic choreic disease had one elongated (50 trinucleotide units) and one normal (19 units) (CAG)n repeat. His asymptomatic elderly father had an intermediate allele of 37 units [9, 10] and a normal allele of 17 units, while his mother, who was also healthy, had two normal alleles of 19 and 20 CAG repeats (fig. 2). In addition, the patient’s clinically unaffected sibling had an intermediate allele (37 repeats) of paternal origin and a normal allele of maternal origin (20 repeats) (fig. 2). These data suggest that the elongated (CAG)n repeat of the sporadic HD case originated from the paternal intermediate allele probably representing a de novo mutation [9, 10].

PCR amplification of DNA from 3 HD families. The PCR products were resolved on 6% Polyacrylamide 8 M urea gels. An M13 sequencing ladder was used for determining the size of these alleles. Affected individuals are shown by closed symbols in each pedigree. Numbers below the amplification products indicate the number of CAG repeat units. Families A and B are affected by dominantly inherited HD, whereas in family C, the disorder was expressed de novo in one individual. An elongation of the CAG repeat (50 trinucleotide units) of paternal origin was found in this patient. The asymptomatic father and sibling of this patient had an intermediate allele (37 CAG repeats).
In the HD patients studied, age at disease onset varied from 3 to 64 years (median = 47 years) and showed a significant inverse correlation with the size of the expanded (CAG)n repeat (r = 0.77, p < 0.00001, n = 43; fig. 3). This correlation was very strong for patients who experienced the onset of their disease before age 42 years (r = 0.86, p = 0.0001, n = 18) and absent for the subgroup of patients whose disease started after 42 years of age (r = 0.25, p = 0.084, n = 25). The two curves were significantly different (p = 0.002).

Number of (CAG)n repeats (VAR2) and age of onset (VAR1) of 43 HD patients. VAR2 = 69.02817 − (0.5119808 VAR1); Pearson’s correlation = −0.772468.
Of 59 family members at risk who were tested, 24 had one elongated and one normal allele ranging from 39 to 55 and from 7 to 29 (CAG)n repeats, respectively. Three individuals had an intermediate allele (36–37 repeats) [9, 10] along with a normal allele (<29 repeats) (fig. 1). Of these, two were the asymptomatic father and sibling of the de novo HD case described above. The third intermediate allele (36 CAG repeats) belonged to a sibling of two HD patients who inherited the disease from their father and had expanded (CAG)n repeats of 46 and 52 units. Although DNA from the father (deceased) was not available for study, determination of the (CAG)n repeat in the unaffected mother of the three siblings showed that the intermediate allele was of paternal origin. The remaining 32 family members at risk had two (CAG)n repeats of normal size (<29).
Evaluation of the (CAG)n repeat in parent-child pairs showed that maternal transmissions were more stable than paternal transmissions. In 7 of 8 maternal transmissions, the repeat was either the same or had changed only by one trinucleotide unit. In contrast, in 7 of 9 paternal transmissions studied, the repeat had increased by 5 (three cases), 7, 11, 13 and 52 repeat units. Of 22 pairs of siblings studied with one expanded (CAG)n repeat (15 of maternal origin and 7 of paternal origin), 13 (59%) showed either no difference or a difference of one trinucleotide repeat; eight sib pairs (36%) differed by 2–6 repeats and 1 by 9 repeats.
Study of the polymorphic (CCG)n repeat that is adjacent to the (CAG)n repeat, showed that 51 and 29% of normal chromosomes (n = 233) had 7 and 10 CCG repeats, respectively (table 1). In contrast 93 and 7% of the HD chromosomes from unrelated patients (n = 27) had 7 and 10 CCG repeats, respectively (table 1). These data show that a strong linkage disequilibrium exists between the 7-unit CCG repeat allele and the HD mutation (elongated CAG repeat; χ2 = 15.55, p < 0.0001, n = 260) in the Greek population studied.
Discussion
This study evaluated the IT15 (CAG)n repeat in 29 HD families from different regions of Greece. Of 44 HD patients tested all but one had an elongated (CAG)n repeat allele within the size range considered to be diagnostic for Huntington’s disease (39–95 trinucleotide units) [2–15]. Moreover, 24 of 59 asymptomatic family members at risk for developing HD had a (CAG)n repeat within this range (>39 units), while 3 had intermediate alleles (36–37 repeats) [10, 11]. Two of these were the asymptomatic father and sibling of a de novo HD case, in whom the paternal intermediate allele might have undergone expansion during transmission, resulting in a new HD mutation as previously suggested [9, 10]. The third intermediate allele (36 CAG repeats) occurred in a sibling of two HD patients (with 46 and 52 CAG repeats) and probably represents a back mutation from a larger paternal HD (CAG)n allele.
The length of the expanded (CAG)n repeat ranged from 42 to 47 trinucleotide units in 70% of the Greek HD patients studied. These data are unlike those reported for other populations [2–5, 8] in which only 40% of HD patients showed a (CAG)n repeat in the range of 42–47 trinucleotide units, but are similar to those derived from HD patients of Danish, Dutch, German and Italian origin [6, 7, 11, 15], 60% of whom showed a (CAG)n repeat elongation in this range.
This study also evaluated a polymorphic (CCG)n repeat adjacent to the HD (CAG)n repeat and revealed that a strong linkage disequilibrium exists between the expanded (CAG)n repeat and the 7-unit (CCG)n repeat. These data, which accord with those previously reported for Canadian [13], Scottish [14] and Italian [15] populations, suggest that the (CAG)n repeat expansion (HD mutation) has occurred primarily on chromosomes with the (CCG)7 repeat haplotype.
In conclusion, the observed distribution of the expanded and the normal (CAG)n alleles, the instability of the HD allele during meiotic transmission and the linkage disequilibrium between the expanded (CAG)n repeat and the adjacent (CCG)n repeat in HD patients of Greek origin is similar to that reported for other European populations, suggesting the common origin of the disorder in these populations.
References
Harper PS: Huntington’s Disease. London, Saunders, 1991.
The Huntington’s Disease Collaborative Research Group: A novel gene containing a trinucleotide repeat that is expanded and unstable on Huntington’s disease chromosomes. Cell 1993;72:971–983.
Duyao M, Ambrose C, Myers R, Novelletto A, Perischetti F, Frontali M, Folstein S, Ross C, Franz M, Abbott M, Gray J, Coneally P, Young A, Penney J, Hollingsworth Z, Shoulson I, Lazzarini A, Falek A, Koroshetz W, Sax D, Brid E, Vonsattel J, Bonilla E, Alvir J, Bickham Conde J, Cha JH, Dure L, Gomez F, Ramos M, Sanchez-Ramos J, Snodgrass S, de Young M, Wexler N, Moscowitz C, Penchaszadeh G, MacFarlane H, Anderson M, Jenkins B, Srinidhi J, Barnes G, Gusella J, MacDonald M: Trinucleotide repeat length instability and age at onset of Huntington’s disease. Nat Genet 1993;4:387–392.
Snell RG, MacMillan JC, Cheadle JP, Fenton I, Lararou LP, Davies P, MacDonald M, Gusella J, Harper PS, Shaw DJ: Relationship between trinucleotide repeat expansion and phenotypic variation in Huntington’s disease. Nat Genet 1993;4: 393–397.
Andrew SE, Goldberg YP, Kremer B, Telenius H, Theilman J, Adam S, Starr E, Squitieri F, Lin B, Kalchman MA, Graham RK, Hayden MR: The relationship between trinucleotide (CAG) repeat length and clinical features of Huntington’s disease. Nat Genet 1993;4:398–403.
Norremolle A, Riess O, Epplen J, Fenger K, Hasholt L, Sorensen SA: Trinucleotide repeat elongation in the Huntington gene in Huntington diesease patients from 71 Danish families. Hum Mol Genet 1993;2: 1475–1476.
Zuhlke C, Riess O, Schroder K, Siedlaczck I, Epplen J, Engle W, Thies V: Expansion of the (CAG)n repeat causing Huntington’s disease in 352 patients of German origin. Hum Mol Genet 1993;2:1467–1469.
MacMillan JC, Snell RG, Tyler A, Houlihan GD, Fenton I, Cheadle JP, Lazarou LP, Shaw DJ, Harper PS: Molecular analysis and clinical correlations of the Huntington’s disease mutation. Lancet 1993;342: 954–958.
Myers RH, MacDonald ME, Koroshetz WJ, Duyao MP, Ambrose CM, Taylor SAM, Barnes G, Srinidhi J, Lin CS, Whaley WL, Lazzarini CM, Schwartz M, Wolff G, Bird ED, Vonsattel JPG, Gusella JF: De novo expansion of a (CAG)n repeat in sporadic Huntington’s disease. Nat Genet 1993;5:168–173.
Goldberg YP, Kremer B, Andrew SE, Theilmann J, Graham RK, Squitieri F, Telenius H, Adam S, Sajoo A, Starr E, Heiberg A, Wolf G, Hayden MR: Molecular analysis of new mutations for Huntington’s disease: Intermediate alleles and sex of origin effects. Nat Genet 1993;5: 174–180.
De Rooiji KE, De Koning Gans PAM, Skraastad MI, Belfroid RDM, Vegter-Van Der Vlis M, Roos RAC, Bakker E, Van Ommen GB, Den Dunnen JT, Losekoot M: Dynamic mutation in Dutch Huntington’s disease patients: Increased paternal repeat instability extending to within the normal size range. J Med Genet 1993;30:996–1002.
Kremer B, Goldberg P, Andrew SE, Theilmann J, Telenius H, Zeisler J, Squitieri F, Lin B, Basset A, Almquist E, Brid T, Hayden MR: A worldwide study of the Huntington’s disease mutation. New Engl J Med 1994;330–20:1401–1406.
Andrew S, Goldberg YP, Theilmann J, Zeisier J, Hayden MR: A CCG repeat polymorphism adjacent to the CAG repeat in the Huntington disease gene: Implications for diagnostic accuracy and predictive testing. Hum Mol Genet 1994;3:65–67.
Barron L, Rae A, Holloway S, Brock DHD, Warner JP: A single allele from the polymorphic CCG rich sequence immediately 3′ to the unstable CAG trinucleotide in the IT15 cDNA shows almost complete disequilibrium with Huntington’s disease chromosomes in the Scottish population. Hum Mol Genet 1994; 3:173–175.
Novelletto A, Persichetti F, Sabbadini G, Mandich P, Bellone E, Ajmar F, Pergola M, Del Senno L, MacDonald ME, Gusella JF, Frontali M: Analysis of the trinucleotide repeat expansion in Italian families affected with Huntington disease. Hum Mol Genet 1994;3:93–98.
The World Federation of Neurology Research Group on Huntington’s Disease: Presymptomatic testing for Huntington’s disease: A world wide survey. J Med Genet 1993;30:1020–1022.
Miller SA, Dykes D, Prensky H: A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acid Res 1988; 16:1215.
Warner JP, Barron LH, Brock DJH: A new polymerase chain reaction (PCR) assay for the trinucleotide repeat that is unstable and expanded on Huntington’s disease chromosomes. Mol Gen Probes 1993;7: 235–239.
Acknowledgements
This work was supported by a Stride Hellas grant and, in part, by NIH grant NS-16871. We thank Mrs. S. Pomoni and Drs. P. Shashidharan and A. Papadimitriou for their assistance in these studies. We are indebted to Ariadne Plaitakis for editorial assistance.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Yapijakis, C., Vassilopoulos, D., Tzagournisakis, M. et al. Linkage Disequilibrium between the Expanded (CAG)n Repeat and an Allele of the Adjacent (CCG)n Repeat in Huntington’s Disease Patients of Greek Origin. Eur J Hum Genet 3, 228–234 (1995). https://doi.org/10.1159/000472303
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1159/000472303
Key Words
This article is cited by
-
Huntington’s Chorea—a Rare Neurodegenerative Autosomal Dominant Disease: Insight into Molecular Genetics, Prognosis and Diagnosis
Applied Biochemistry and Biotechnology (2021)
-
A common SNP haplotype provides molecular proof of a founder effect of Huntington disease linking two South African populations
European Journal of Human Genetics (2007)
