
Figures, tables and video
From the following article
Laryngeal and pharyngeal complications of gastroesophageal reflux disease
Gregory N. Postma and Stacey L. Halum
GI Motility online (2006)
doi:10.1038/gimo46

Figure 1
Laryngeal granulomas in a patient with numerous episodes of pharyngeal acid exposure and no history of intubation.
Full size figure and legend (50K)
Figure 2
Infraglottic edema: a finding highly sensitive but not specific for laryngopharyngeal reflux (LPR).
Full size figure and legend (47K)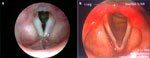
Figure 3
a: Ventricular obliteration is secondary to edema of the true vocal folds and false vocal cords.
Full size figure and legend (19K)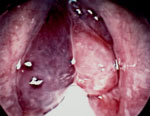
Figure 4
Intraoperative photo of polypoid degenerations of the true vocal folds (Reinke's edema).
Full size figure and legend (79K)
Figure 5
An extraordinary degree of diffuse laryngeal edema is seen in an individual with more than 80 episodes of LPR on pH testing.
Full size figure and legend (47K)
Figure 6
Chronic laryngitis in a patient following radiation therapy for glottic carcinoma.
Full size figure and legend (67K)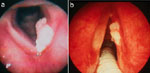

Figure 8
Crusting granulation tissue seen in the larynx and subglottis of a patient with Wegener's granulomatosis.
Full size figure and legend (52K)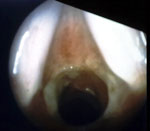
Figure 9
A patient with subglottic stenosis with no history of intubation of trauma.
Full size figure and legend (39K)
Figure 10
A nonsmoker with severe pH probe documented LPR and squamous cell carcinoma on both true vocal folds.
Full size figure and legend (48K)

Table 2
The reflux symptom index (RSI): a score greater than 5 in the proper clinical situation is strongly suggestive of laryngopharyngeal reflux (LPR)
Full size table and legendTable 3
The reflux finding score (RFS): a score greater than 11 in the proper clinical situation is strongly suggestive of laryngopharyngeal reflux (LPR)
Full size table and legend
Video 1
Left vocal process granuloma, which responded well to antireflux therapy and speech therapy.
Full size video and legend (0K)