
Abstract
Alzheimer’s disease (AD) is a severe neurodegenerative disorder still in search of effective methods of diagnosis. Altered levels of the NMDA receptor co-agonist, d-serine, have been associated with neurological disorders, including schizophrenia and epilepsy. However, whether d-serine levels are deregulated in AD remains elusive. Here, we first measured D-serine levels in post-mortem hippocampal and cortical samples from nondemented subjects (n=8) and AD patients (n=14). We next determined d-serine levels in experimental models of AD, including wild-type rats and mice that received intracerebroventricular injections of amyloid-β oligomers, and APP/PS1 transgenic mice. Finally, we assessed d-serine levels in the cerebrospinal fluid (CSF) of 21 patients with a diagnosis of probable AD, as compared with patients with normal pressure hydrocephalus (n=9), major depression (n=9) and healthy controls (n=10), and results were contrasted with CSF amyloid-β/tau AD biomarkers. d-serine levels were higher in the hippocampus and parietal cortex of AD patients than in control subjects. Levels of both d-serine and serine racemase, the enzyme responsible for d-serine production, were elevated in experimental models of AD. Significantly, d-serine levels were higher in the CSF of probable AD patients than in non-cognitively impaired subject groups. Combining d-serine levels to the amyloid/tau index remarkably increased the sensitivity and specificity of diagnosis of probable AD in our cohort. Our results show that increased brain and CSF d-serine levels are associated with AD. CSF d-serine levels discriminated between nondemented and AD patients in our cohort and might constitute a novel candidate biomarker for early AD diagnosis.
Similar content being viewed by others


Introduction
Alzheimer’s disease (AD) is a complex neurological disorder characterized by progressive memory loss and cognitive impairment. AD neuropathology includes brain deposition of amyloid plaques, neurofibrillary tangles and significant synapse loss.1, 2 AD remains as a largely idiopathic disorder, although mounting evidence suggests that levels of amyloid-β oligomers (AβOs) build up in patient brains to cause synapse failure and memory loss.3, 4
Currently, diagnosis of probable AD is based on neuropsychological testing, fluid biomarker assessment and brain imaging,5, 6, 7, 8, 9 but diagnosis of the earliest stages of AD, before major brain damage takes place, is still challenging. In order to improve diagnostics and to allow treatment to be initiated at the earliest possible stage, there is an urgent need to incorporate biomarkers capable of detecting disease onset or at early stages. In this context, cerebrospinal fluid (CSF) levels of amyloid-β1–42 (Aβ42), total tau protein and hyperphosphorylated tau (p-tau) have now been included in diagnostic guidelines.6, 10 Such CSF biomarkers have been advocated for research purposes, but sensitivity and specificity issues have generally raised concerns about their widespread clinical application.5, 6, 11
Aberrant activation of glutamate receptors of the N-methyl-d-aspartate subtype (NMDARs) has been associated with synapse dysfunction and neurotoxicity in AD.12, 13, 14, 15, 16, 17 Accordingly, memantine (an open-channel blocker of NMDARs) has been approved for clinical use in patients with moderate-to-severe AD.18 d-serine is the main co-agonist at NMDARs in frontal brain areas19, 20, 21 and has been implicated in NMDAR-mediated neurotoxicity.22 Consistent with a possible role in pathological states, in vitro studies have shown increased release of d-serine from both glial and neuronal cells and NMDAR activation under injury, in particular in AD model systems.23, 24 On the other hand, exogenous d-serine administration may improve behavioral deficits in experimental models25, 26 and may act as a NMDAR antagonist under some circumstances.27
Literature reports on changes in d-serine levels in AD brains have been controversial. Early studies reported unaltered d-serine levels in the frontal and parietal cortices of AD patients,28, 29, 30 whereas another study found increased d-serine levels in the CSF of AD patients compared with healthy controls.31
The goal of the current study was to investigate whether d-serine levels are deregulated in AD, and to assess its potential as a novel biomarker in AD. We initially investigated d-serine levels in post-mortem AD brains in comparison with brains from cognitively intact control subjects. To determine whether there was a causal relationship between AβO toxicity and d-serine levels, we next studied d-serine levels in cellular and animal models of AD. Finally, we collected CSF and measured d-serine levels in patients with probable AD, major depression or hydrocephalus and healthy controls. Results showed elevated d-serine levels in brain tissue from AD patients in comparison with controls. In experimental models, we found that Aβ oligomers caused elevations in d-serine levels, likely via upregulation of serine racemase (SR). Further, we found increased d-serine levels in the CSF of patients with probable AD. Incorporation of d-serine measurements into the amyloid-tau biomarker index significantly increased diagnostic sensitivity and specificity in our cohort, suggesting that CSF d-serine determination may constitute a simple and effective manner to improve in vivo diagnosis of AD.
Materials and methods
Study approval
Experiments using human samples were approved by local ethics committees from each participating institution. All study subjects or their next-of-kin (in the case of post-mortem samples) provided written informed consent for study participation. Experiments in animals were approved by the Institutional Animal Care and Use Committee of the Federal University of Rio de Janeiro (protocols # IBqM 022, 041 and 055).
Post-mortem samples
Post-mortem tissue samples were obtained from the Brain Bank of the Brazilian Aging Brain Study Group,32 School of Medicine of the University of Sao Paulo. Brains were obtained from the Sao Paulo Autopsy Service, after written informed consent. We studied 17 cases with a neuropathological diagnosis of AD confirmed for the presence of pathological hallmarks by an experienced neuropathologist, and 12 cases without neuropathological changes. The clinical dementia rating (CDR) was determined by a validated interview conducted with the informant caregiver.33, 34 The control group consisted of cases with CDR=0, whereas the AD group included cases with CDR ranging from 1 to 3. Demographic characteristics of those groups are presented in Table 1. More detailed information on individual subjects is provided in Supplementary Table 1.
CSF samples
Twenty-one patients with probable AD were recruited from the AD Center at the Institute of Psychiatry of the Federal University of Rio de Janeiro (IPUB/UFRJ). Patients with probable AD were diagnosed according to the National Institute of Neurological and Communicative Disorders and Stroke (NINCDS-ADRDA) and the Diagnostic and Statistical Manual of Mental Disorders, 4th edition criteria, using a combination of clinical evaluation, neuropsychological testing and biomarker (Aβ and total tau protein) assessment, as described.35 Nine nondemented patients diagnosed with major depression according to Diagnostic and Statistical Manual of Mental Disorders, 4th edition criteria were also recruited at IPUB/UFRJ. Ten healthy control subjects and nine patients with normal pressure hydrocephalus, diagnosed according to the International Classification of Diseases, 10th edition, were recruited at the Neurolife Laboratory, a private clinic specialized in CSF analysis in the city of Rio de Janeiro. Patients were subjected to the mini-mental state exam to assess cognitive performance. All patients included in the study were older than 60 years of age. Exclusion criteria for all groups included psychiatric and neurological diagnoses other than AD and major depression, any unstable clinical diagnoses, cigarette smoking (more than 10 packs per year) and alcohol abuse. CSF samples were collected through lumbar puncture in the L3–4 or L4–5 interspace and were immediately stored at −80 °C. All lumbar punctures were performed around 1100 hours in order to minimize possible circadian fluctuations in the concentrations of analytes.
Demographic characteristics for the four subject groups are presented in Table 1. More detailed information on individual subjects is provided in Supplementary Table 2. Studied groups were significantly different in terms of gender distribution. However, d-serine levels were similar between males and females across diagnostic groups (c2=0.23; P=0.63) (Supplementary Figure 1).
Psychotropic medication used by probable AD patients included rivastigmine (47.6%; n=10), risperidone (38.1%; n=8), memantine (28.6%; n=6), donepezil (23.8%; n=5), clonazepam (19.0%; n=4), citalopram (4.8%; n=1), trazodone (4.8%; n=1), biperiden (4.8%; n=1), escitalopram (4.8%; n=1) and mirtazapine (4.8%; n=1). Two (9.5%) patients with probable AD were not taking any medication at the time of the study. None of the medications used showed any significant effect on CSF d-serine levels (Supplementary Table 3).
Biochemical analyses of human samples
Post-mortem tissue was homogenized in buffer containing 20 mM Tris-HCl (pH 7.4), 2 mM EDTA and a cocktail of protease inhibitors (Roche complete mini, Basel, Switzerland). d-serine, l-serine and glycine levels in tissue homogenates, CSF and culture media were measured by high-performance liquid chromatography as previously described.36, 37 Amino-acid concentrations were expressed per gram of total proteins in tissue homogenates or as actual concentration in CSF and culture media.
CSF levels of p-tau, total tau protein and Aβ42 were measured using commercially available enzyme-linked immunosorbent assays (ELISA INNOTEST p-tau181, INNOTEST htau, INNOTEST β-amyloid(1-42) kits, respectively; Innogenetics, Gent, Belgium) according to manufacturer’s instructions. The INNOTEST amyloid/tau index (IATI) was calculated as:

Soluble AβOs
AβOs were prepared weekly from synthetic Aβ1–42 (American Peptide, Sunnyvale, CA, USA), and were routinely characterized by size-exclusion chromatography and, occasionally, by western immunoblots and transmission electron microscopy, as previously described.38, 39 Oligomers were stored at 4 oC and were used within 48 h of preparation.
Mature hippocampal cultures
Primary rat embryo hippocampal neuronal cultures, prepared and developed in Neurobasal medium supplemented with B27 (Invitrogen, Carlsbad, CA, USA) and antibiotics according to established procedures,16 were used after 18–21 days in vitro. Cultures were exposed for 24 h to 500 nM AβOs or an equivalent volume of vehicle (2% dimethyl sulfoxide in phosphate-buffered saline) at 37 °C.
Animals
C57Bl/6 wild-type (WT) mice were obtained from the animal facility at CECAL/FIOCRUZ (Rio de Janeiro, Brazil). Three-month-old mice received a single intracerebroventricular injection of either vehicle (2% dimethyl sulfoxide in phosphate-buffered saline) or Aβ oligomers (10 pmol total Aβ, corresponding to 45 ng) as described.40, 41 After 8 days, animals were killed and had their hippocampi collected for d-serine analysis.
APPSwe/PS1ΔE9 transgenic mice on a C57Bl/6 background42 were obtained from the Jackson Laboratories (Bar Harbor, ME, USA). WT littermates were used as controls. For d-serine assessment in APP/PS1 brains, nine animals aged 14–16 months were used per experimental group.
Surgical procedures in adult male Wistar rats were performed as described,43 with slight modifications. A sagittal incision was made on the scalp and a small craniotomy was performed unilaterally to implant a cannula in the hippocampus (A/P: −3.0 mm; L: 1.5 mm; D/V: 3.5 mm). After 7–10 days of recovery from surgery, animals were chronically injected with 1 μg of AβOs or vehicle (2% dimethyl sulfoxide in saline; 3–5 μl per injection) once a week for 5 weeks. Rats were euthanized and samples collected 3 days after the last AβO injection.
In all experiments, animals were caged in groups of five with controlled room temperature and humidity. Animals had free access to food/water and were under a 12-h light/dark cycle.
Biochemical analyses in experimental models
Homogenates from hippocampi or primary neuronal cultures were prepared in RIPA buffer (25 mM Tris-HCl, pH 7.5, 150 mM NaCl, 1% NP-40, 1% sodium deoxycholate, 0.1% SDS, 5 mM EDTA and 1% Triton X-100) containing protease and phosphatase inhibitor cocktails (Thermo-Pierce, Rockford, IL, USA). Protein concentration was determined by the BCA assay (Thermo-Pierce). Homogenates or conditioned media were treated with trichloroacetic acid (5% final concentration) to precipitate proteins and extract free amino acids. Samples were centrifuged (20 000 g for 5 min), the supernatants were extracted three times with water-saturated diethyl ether to remove trichloroacetic acid and amino acids were measured by high-performance liquid chromatography, as described.36, 37, 44
For western blot analysis, soluble lysates (30 μg protein applied per lane) were resolved on 10% SDS-polyacrylamide gel electrophoresis, electrotransferred onto nitrocellulose membranes and probed using anti-serine racemase antibody (BD Biosciences, San Jose, CA, USA; 1:500). β-actin (Abcam, Cambridge, UK; 1:50 000) was used as a loading control. Immunoblots were developed with SuperSignal West Femto Maximum Sensitivity substrate (Thermo Scientific, Waltham, MA, USA) and imaged on photographic film.
For determination of SR messenger RNA levels in primary neuronal cultures exposed to vehicle or AβOs, total RNA was extracted with Trizol (Life Technologies, Carlsbad, CA, USA). RNA characterization and complementary DNA synthesis were performed as described.38, 41 Quantitative reverse transcription-PCR protocols were performed using specific primers for SR (forward 5′-TAGCGGGACAAGGGACAATT-3′; reverse 5′-TGCATACTTGATTTCATCTTCCGTG-3′) and β-actin (forward 5′-GTCTTCCCCTCCATCGTG-3′; reverse 5′-AGGATGCCTCTCTTGCTCTG-3′), as described.41 Results were analyzed according to the 2-(ΔΔCt) method45 and are shown normalized by levels in vehicle-treated cultures.
Statistical analyses
Results from human samples are presented as means±s.d., except for analysis of covariance results, which are presented as means±s.e. The distributions of d-serine and l-serine levels were evaluated for normalcy, and winsorized means were calculated if outliers were present. For d-serine, we adjusted one outlier in the data set for the hippocampus and two outliers in the data set for the occipital cortex in the AD group. For l-serine, we adjusted one outlier in the CSF study data set in the AD group and two outliers in the hydrocephalus group; one outlier in the hippocampus data set, one in the parietal cortex data set and one in the occipital cortex in the AD group. For glycine, we adjusted one outlier in the CSF study data set in the AD group. Statistical significances of differences between groups were determined by analysis of covariance followed by Bonferroni’s multiple comparison tests. Associations between measures were analyzed by Pearson’s bivariate correlation. Effect size was measured by Cohen’s test, and post hoc statistical power analysis was performed using G Power (University of Dusseldorf; available at http://www.gpower.hhu.de46) to determine the minimal sample size that would be required for a duplication effect under our conditions.
In experimental studies, analyses were performed with GraphPad Prism (La Jolla, CA, USA) and data sets were assessed for normality prior to significance determination. Values are expressed as means±s.e.m., unless otherwise stated. Significance was set at 5% in two-sided tests.
Results
Brain d-serine levels in neuropathologically confirmed AD
We initially investigated d-serine levels in post-mortem samples from three brain regions: hippocampus, parietal and occipital cortices. Cases were divided in two groups: controls (cases without clinical dementia or neuropathology) and AD (cases with clinical signs of dementia and neuropathology typical of full-blown AD). Demographic characteristics of cases are presented in Table 1. Because the AD group was significantly older (80.9±4.7 years) than the control group (74.7±11.5 years), age was entered as a covariate in the analyses.
After adjustment for age, d-serine levels were significantly higher in AD brains compared with controls in both the hippocampus (Figure 1a) and parietal cortex (Figure 1b), two regions severely affected by AD. In contrast, d-serine levels were not significantly different between groups in the occipital cortex, an area more resistant to AD pathology (Figure 1c). Glycine levels were unchanged in the hippocampus and occipital cortex, but were fairly elevated in the parietal cortex of AD patients in comparison with controls (Table 2). No significant differences between groups were observed in brain levels of l-serine and total serine (Table 2). Results demonstrate that d-serine levels are elevated in post-mortem brain regions affected by AD.

d-serine levels are increased in Alzheimer’s disease (AD) post-mortem brain tissue. d-serine levels in the hippocampus (a), parietal cortex (b) and occipital cortex (c) of post-mortem samples from control (Ctrl) and AD subjects. Values are presented as nmol of d-serine per g of wet tissue (WT). Horizontal lines represent mean values for each diagnostic group. Data points correspond to individual values. Statistical significance is given by the Student’s t-test (*P<0.05; NS, not significant).
Soluble AβOs increase d-serine levels in hippocampal cultures
To gain insight into the mechanism underlying elevated d-serine levels in AD brains, we examined the impact of soluble AβOs, which accumulate in AD brains and are thought to trigger synapse failure, on d-serine levels in cultured hippocampal neurons. Exposure of cultures to AβOs (500 nM) for 24 h significantly increased d-serine levels in conditioned medium compared with vehicle-treated cultures (Figure 2a). We next looked at messenger RNA and protein levels of SR, the enzyme responsible for synthesis of d-serine.47, 48 AβOs increased SR at both messenger RNA (Figure 2b) and protein levels (Figure 2c) in hippocampal cultures, likely explaining the increase in d-serine release to the medium in such cultures.

Amyloid-β oligomers (AβOs) increase d-serine and serine racemase (SR) levels in hippocampal cultures. Primary rat hippocampal neuronal cultures were exposed to 500 nM AβOs or vehicle (2% dimethyl sulfoxide in phosphate-buffered saline) for 24 h. (a) AβOs increased extracellular levels of d-serine. (b and c) AβOs increased total levels of SR messenger RNA (mRNA) (b) and protein (c). d-serine was measured by high-performance liquid chromatography and its values were corrected by total protein content in the analyzed samples. SR protein levels were detected by western blotting, using β-actin as a loading control. *P<0.05 (Student’s t-test), statistical significance was assessed in comparison with control. Results are expressed as means±s.e.m. of three independent experiments (each carried out in triplicate wells) with different neuronal cultures.
d-serine is elevated in the brains of AβO-injected rodents and of APP/PS1 transgenic mice
To determine whether AβO−induced upregulation of d-serine levels occurs in vivo, we chronically injected AβOs into rat hippocampi for 5 weeks (see Materials and methods). AβOs increased hippocampal d-serine levels compared with levels measured in hippocampi of vehicle-injected rats (Figure 3a). We next examined WT C57Bl/6 mice that received a single intracerebroventricular injection of either vehicle or 10 pmol AβOs, recently shown to cause memory/behavioral impairments.40, 41 We found significantly increased d-serine levels in the hippocampi of AβO-injected mice compared with vehicle-injected animals (Figure 3b). Importantly, levels of l-serine (Supplementary Figure 2a) and glycine (Supplementary Figure 2b), another NMDAR co-agonist, were unaltered by AβO injection, likely not reflecting a global deregulation of amino-acid levels triggered by AβOs.

Amyloid-β oligomers (AβOs) increase hippocampal d-serine and serine racemase (SR) levels in vivo. (a) AβOs increased d-serine levels in hippocampal homogenates of rats that received intrahippocampal injections of AβOs (1 μg) or vehicle (2% dimethyl sulfoxide in phosphate-buffered saline) once a week for 5 weeks (n=8 veh; n=7 AβOs), as analyzed 3 days after the last injection. (b) d-serine content is increased in the hippocampi of mice that received a single intracerebroventricular injection of AβOs (10 pmol, or 45 ng). d-serine levels were measured 8 days post injection (n=10 per group). (c and d) Thirteen- to fourteen-month-old APPSwe/PS1ΔE9 (APP/PS1) transgenic mice showed increased hippocampal levels of d-serine (c) and SR (d) compared with wild-type (WT) mice (n=8 per group). d-serine was measured by high-performance liquid chromatography and its values were corrected by total protein (ptn) content in the analyzed samples. SR protein levels were detected by western blotting using β-actin as the loading control. *P<0.05; **P<0.01 (Student’s t-test), statistical significances were assessed in comparison with controls. Results are presented as means±s.e.m. of individuals.
Further, we measured d-serine levels in the brains of APPSwe,PS1ΔE9 (APP/PS1) mice, which harbor transgenes for human amyloid precursor protein (APP) bearing the Swedish mutation and a mutant form of presenilin 1 (PS1). These animals display elevated Aβ levels and develop age-related cognitive deficits.42, 49, 50 In harmony with our hypothesis, we found markedly increased hippocampal d-serine levels in APP/PS1 mice compared with WT littermates (Figure 3c). This was accompanied by increased SR levels in the hippocampus (Figure 3d). Levels of l-serine (Supplementary Figure 2c) and glycine (Supplementary Figure 2d) were similar in WT and APP/PS1 mice. Results thus establish that AβOs instigate increases in hippocampal d-serine and SR levels in vivo.
CSF levels of d-serine in patients with probable AD
Given our findings in post-mortem brains and in experimental models of AD, we next investigated whether CSF levels of d-serine were altered in a group of patients with probable AD, as compared with healthy controls, patients with major depression or patients with hydrocephalus. Remarkably, mean d-serine levels in probable AD patients were approximately fivefold higher than in healthy controls, and about twofold higher than in the depression and hydrocephalus patient groups (Figure 4a and Table 3), yielding an effect size (d, Cohen’s test) of 7.1 between controls and probable AD subjects. Mean d-serine levels in the major depression and hydrocephalus groups were also significantly higher than in healthy controls (Figure 4a and Table 3). Further, when biomarker combination (IATI) was used to separate AD from non-AD cases (using either 0.83, 0.96 or 1.246 as cutoffs, in accordance with previous studies that used cutoffs of <0.8, <1.0 or <1.2 for AD diagnosis51, 52, 53, 54), CSF d-serine levels were again significantly different from non-AD patients (Figure 4b). Remarkably, cases clinically diagnosed as probable AD by neuropsychological assessment had higher CSF d-serine levels (Figure 4b) than nondemented patients. In addition, total serine levels (that is, d-serine+l-serine) were higher in AD and major depression compared with healthy controls (Table 3), whereas l-serine levels did not differ significantly between groups (Table 3). CSF glycine levels were not significantly different between AD and control groups (Table 3).

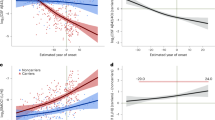
Increased cerebrospinal fluid (CSF) levels of d-serine in patients with probable Alzheimer’s disease (AD). (a) CSF levels of d-serine in healthy controls (Ctrl) and in patients with probable AD, major depressive disorder (MDD) or hydrocephalus (Hydro). Statistical significance was assessed by one-way analysis of variance (ANOVA) followed by Bonferroni adjustment for multiple comparisons. (b) CSF d-serine levels (μmol l−1) in non-AD (white circles for INNOTEST amyloid/tau index (IATI)-based classification; blue circles for neuropsychological assessment) and AD cases (black circles for IATI-based classification; red circles for neuropsychological assessment) using different IATI cutoffs (0.83; 0.96; 1.24). Horizontal bars represent mean values for each group. ***P<0.001; Student’s t-test. (c) CSF levels of d-serine as a function of the mini-mental state exam (MMSE). (d) CSF levels of d-serine as a function of CDR scores. Horizontal lines represent mean values for each CDR group. Data points correspond to individual values. Statistical significance is given by one-way ANOVA followed by Bonferroni adjustment for selected groups: CDR 0.5, 1, 2 and 3 versus CDR 0. (e) CSF levels of d-serine as a function of IATI across subject groups. (f) Receiver-operating characteristic curves for diagnostic based on IATI alone (blue line) or IATI/D-ser levels (red line), showing increased sensitivity and specificity when d-serine is added to the calculation. *P<0.05; ***P<0.001. CDR, clinical dementia rating score; NPA, neuropsychological assessment.
As expected, mean mini-mental state exam scores were significantly lower in the AD group compared with the other patient groups (Table 4). Interestingly, individual d-serine levels across all subjects, regardless of diagnosis, were negatively correlated to the mini-mental state exam score (Figure 4c). We further investigated how d-serine levels correlated to dementia by separating subjects into groups stratified by CDR scores. The CDR 0 (cognitively normal) group showed significantly lower levels of d-serine than the groups with CDR 0.5, 1, 2 and 3 (Figure 4d). It is interesting to note that d-serine levels were already elevated in patients with a CDR score of 0.5, typically associated with pre-dementia mild cognitive impairment.
CSF d-serine versus amyloid/tau biomarkers of AD
IATI is a score that combines CSF Aβ42 and total tau protein levels, and has been proposed as a biomarker to assist in the diagnosis of AD.51 As expected, the mean IATI score was significantly lower in the AD group than in the other three groups (Table 4). Interestingly, individual d-serine levels were negatively associated with IATI scores (Figure 4e).
To explore the potential of d-serine as a biomarker, we compared CSF d-serine levels and IATI scores on their specificity and sensitivity for the diagnosis of probable AD in our cohort. Using the cutoff of 1.246, IATI showed 81.4% sensitivity and 94.4% specificity (in good agreement with published values55), whereas determination of CSF d-serine levels (using a cutoff of 9.82 μmol l−1) afforded 92.9% sensitivity and 85.7% specificity for AD. Remarkably, combined use of both IATI and CSF d-serine levels (that is, calculating an IATI/ d-serine ratio, and using a cutoff of 0.14) resulted in significantly increased sensitivity (96.3%) and specificity (100%) for the diagnosis of probable AD. Increased sensitivities and specificities were also obtained by inclusion of d-serine determination using lower IATI cutoff values (Supplementary Table 4). Receiver-operating characteristic curves for IATI alone and IATI/ d-serine are shown in Figure 4f.
Discussion
We identified elevated levels of d-serine in post-mortem samples from brain regions involved in disease progression in neuropathologically confirmed AD cases. Pathological changes in AD usually spread from limbic structures, comprising the hippocampal formation, to associative areas such as the posterior parietal cortex, and only later reach primary neocortical areas, such as the striate cortex in the occipital lobe.56, 57 Consistent with this pattern, we found increased d-serine levels in the hippocampus and parietal cortex of AD brains compared with nondemented controls, but no differences in the occipital cortex. Noteworthy, three early studies using post-mortem frontal or temporal cortical tissue failed to detect altered d-serine levels between AD and controls.28, 29, 30 Those findings, when contrasted to our results stratified by regions and CDR, raise the possibility that d-serine elevation is not a widespread event in AD brains, but rather occurs in a region-specific manner according to disease progression. These observations are consistent with a scenario in which regional elevations in d-serine levels trigger localized deregulation of NMDAR-dependent synaptic plasticity and, ultimately, NMDAR-related excitotoxicity and neuronal injury, culminating in cognitive decline in AD.
To gain insight into the underlying mechanisms leading to increased d-serine levels in the AD brain, we next investigated d-serine levels in AD model systems. AβOs build up in AD brains58, 59, 60 and are thought to trigger toxic mechanisms leading to synapse failure in AD,3 including aberrant NMDAR function,15, 16, 17 increased glutamate release17, 24 and impaired synaptic plasticity.13, 61 We now report that d-serine is elevated in the extracellular medium of hippocampal cultures exposed to AβOs and in the hippocampi of rodents that received brain injections of AβOs. Furthermore, APP/PS1 mice, which display age-dependent AD pathology and memory impairment, showed markedly increased brain d-serine levels. Consistently, increased SR levels were also verified in both AβO-exposed cultures and transgenic rodent brains likely explaining elevated d-serine content in vitro and in vivo. Importantly, elevations in d-serine content do not appear to reflect a general deregulation of neuroactive amino-acid levels, as levels of neither l-serine nor of the NMDAR co-agonist, glycine, were altered in the hippocampus and CSF of AD cases and in AβO-injected mice or APP/PS1 mice. These observations suggest a causal relationship between AβO accumulation and d-serine increases in AD brains.
Abnormal NMDAR function is thought to underlie, at least in part, AD pathogenesis,4, 12, 17, 62, 63 and AβOs impair NMDAR-dependent synaptic plasticity and instigate NMDAR-mediated synapse loss and oxidative stress.13, 15, 16, 61, 64 Thus, our finding of elevated levels of d-serine, the main co-agonist at NMDARs in frontal brain regions, points to a novel mechanism by which AβOs may trigger synapse dysfunction and memory impairment.
Importantly, AD brains present reduced levels of NMDAR65, 66, 67 in areas that are relevant for disease progression. Therefore, it is tempting to speculate that increased d-serine levels could comprise an initial adaptive response to maintain proper neurotransmission. However, given that NMDAR function appears to be overactivated in AD,12 elevated d-serine could contribute to an excitotoxic scenario, worsening AD neuropathological outcomes.
Whether and how increased levels of d-serine participate in cognitive and behavioral outcomes in AD is still unknown. d-serine administration has been shown to promote synaptogenesis and to have memory-enhancing effects.25, 68, 69 Conversely, excessive d-serine levels were shown to mediate NMDAR-dependent late-phase apoptosis70 and to contribute to neurological insults, such as excitotoxicity and brain ischemia.22 Further, a recent report suggested that d-serine might act as a NMDAR antagonist under some circumstances.27 Therefore, a fine regulation of d-serine levels is required for maintaining proper synaptic homeostasis and function. Future experimental studies may unravel the role of d-serine in synapse dysfunction and neurotoxicity in AD.
The main finding of the current study is that CSF levels of d-serine are significantly higher in patients diagnosed with probable AD than in nondemented subjects, suggesting that d-serine could be a novel AD biomarker. Importantly, the significant correlation between increased d-serine content in the CSF and poorer cognitive performance in the mini-mental state exam suggests that d-serine determination could comprise a powerful diagnostic tool in conjunction with assessment of cognitive decline. As CSF d-serine is already significantly elevated in patients with CDR 0.5, this might facilitate diagnosis of AD-related cognitive decline at an early stage of cognitive impairment, and permit interventional approaches at a phase in which disease could still be modifiable.
The fact that CSF levels of d-serine are also elevated in depression and hydrocephalus, compared with control subjects, might suggest that d-serine would not be a specific AD biomarker. We note, however, that d-serine levels in AD are clearly and significantly higher than in depression or hydrocephalus, allowing definition of a cutoff value that discriminates between those disorders. Further, combination of CSF d-serine measurements with the validated IATI biomarker yielded 100% specificity in our cohort. Our results suggest that CSF d-serine levels adequately discriminate AD from non-AD cases when used in combination with different IATI cutoff values, and correlate well with neuropsychological diagnosis. Results thus indicate that determination of CSF d-serine levels could improve diagnostic accuracy in AD. Nonetheless, as a pilot study, replication of these findings in other cohorts would make a strong case for the incorporation of d-serine levels in a panel of CSF biomarkers for AD.
It is interesting to note that elevated d-serine levels in depression might be related to late development of AD. Depression is often clinically associated with AD.71, 72 It has recently been shown that AD and depression share common mechanisms, and that both memory loss and depressive-like symptoms are instigated by AβOs in mice.40 Because AβOs increase brain d-serine levels, it is plausible that elevated levels of d-serine in AD and depression are both consequences of the neurotoxic impact of Aβ. This interesting hypothesis deserves further investigation and might open new avenues for studying the pathogenesis of AD-linked disorders.
In conclusion, our results show that AD patients have increased levels of d-serine in the CSF and in specific brain regions, and that this appears to be triggered by the action of soluble AβOs in the brain. CSF d-serine levels are strongly correlated with memory impairment and could constitute an effective diagnostic tool for probable AD. A limitation of this study is the cohort size and heterogeneity, although these factors did not compromise robustness of our findings, as indicated by statistical power analyses with adequate sample sizes. Our present study constitutes a novel and encouraging effort toward improved AD diagnostics. Nevertheless, despite the current statistically robust results, we acknowledge that this is a pilot investigation and, thus, a larger prospective clinical study is warranted to extend the validity of our results.
The field of AD diagnostics still suffers from the lack of accurate and efficient biomarkers. This may be attributed, in part, to the complex nature of this disease. Nonetheless, very recent approaches have provided advances in establishing clearer and more efficient strategies for biomarker-based diagnosis. For example, a recent paper by Lehmann et al.55 proposed a new diagnostic scale that might be translated into clinical applications in the near future. Furthermore, other recent efforts have unveiled a number of promising CSF biomarkers, including AβOs, double-stranded RNA-dependent protein kinase and other neuronal injury markers.73, 74, 75, 76, 77 Combined use of those biomarkers and others currently in development with determination of CSF d-serine concentrations could constitute a valuable strategy to increase sensitivity and specificity in the diagnosis of AD.
References
Tarawneh R, Holtzman DM . The clinical problem of symptomatic Alzheimer disease and mild cognitive impairment. Cold Spring Harb Perspect Med 2012; 2: 1–17.
Mattson MP . Pathways towards and away from Alzheimer’s disease. Nature 2004; 430: 631–639.
Ferreira ST, Klein WL . The Aβ oligomer hypothesis for synapse failure and memory loss in Alzheimer’s disease. Neurobiol Learn Mem 2011; 96: 529–543.
Mucke L, Selkoe DJ . Neurotoxicity of amyloid-beta protein: synaptic and network dysfunction. Cold Spring Harb Perspect Med 2012; 2: 1–17.
Jack CR, Albert MS, Knopman DS, McKhann GM, Sperling RA, Carrillo MC et al. Introduction to the recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 2011; 7: 257–262.
McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR, Kawas CH et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 2011; 7: 263–269.
McKhann GM . Changing concepts of Alzheimer's disease. JAMA 2011; 305: 2458–2459.
Selkoe DJ . Preventing Alzheimer's disease. Science 2012; 337: 1488–1492.
DeKosky ST, Carrillo MC, Phelps C, Knopman D, Petersen RC, Frank R et al. Revision of the criteria for Alzheimer's disease: a symposium. Alzheimers Dement 2011; 7: e1–e12.
Blennow K, Hampel H, Weiner M, Zetterberg H . Cerebrospinal fluid and plasma biomarkers in Alzheimer disease. Nat Rev Neurol 2010; 6: 131–144.
Hampel H, Bürger K, Teipel SJ, Bokde ALW, Zetterberg H, Blennow K . Core candidate neurochemical and imaging biomarkers of Alzheimer’s disease. Alzheimers Dement 2008; 4: 38–48.
Paula-Lima AC, Brito-Moreira J, Ferreira ST . Deregulation of excitatory neurotransmission underlying synapse failure in Alzheimer's disease. J Neurochem 2013; 126: 191–202.
Li S, Jin M, Koeglsperger T, Shepardson NE, Shankar GM, Selkoe DJ . Soluble Aβ oligomers inhibit long-term potentiation through a mechanism involving excessive activation of extrasynaptic NR2B-containing NMDA receptors. J Neurosci 2011; 31: 6627–6638.
Li S, Hong S, Shepardson NE, Walsh DM, Shankar GM, Selkoe D . Soluble oligomers of amyloid-β protein facilitate hippocampal long-term depression by disrupting neuronal glutamate uptake. Neuron 2009; 62: 788–801.
Shankar GM, Bloodgood BL, Townsend M, Walsh DM, Selkoe DJ, Sabatini BL . Natural oligomers of the Alzheimer amyloid-β protein induce reversible synapse loss by modulating an NMDA-type glutamate receptor-dependent signaling pathway. J Neurosci 2007; 27: 2866–2875.
De Felice FG, Velasco PT, Lambert MP, Viola K, Fernandez SJ, Ferreira ST et al. Aβ oligomers induce neuronal oxidative stress through an N-methyl-D-aspartate receptor-dependent mechanism that is blocked by the Alzheimer drug memantine. J Biol Chem 2007; 282: 11590–11601.
Talantova M, Sanz-Blasco S, Zhang X, Xia P, Akhtar MW, Okamoto S et al. Aβ induces astrocytic glutamate release, extrasynaptic NMDA receptor activation, and synaptic loss. Proc Natl Acad Sci USA 2013; 110: E2518–E2527.
Parsons CG, Danysz W, Dekundy A, Pulte I . Memantine and cholinesterase inhibitors: complementary mechanisms in the treatment of Alzheimer’s Disease. Neurotox Res 2013; 24: 358–369.
Wolosker H, Radzishevsky I . The serine shuttle between glia and neurons: implications for neurotransmission and neurodegeneration. Biochem Soc Trans 2013; 41: 1546–1550.
Radzishevsky I, Sason H, Wolosker H . D-Serine: physiology and pathology. Curr Opin Clin Nutr Metab Care 2013; 16: 72–75.
Wolosker H, Dumin E, Balan L, Foltyn VN . d-Amino acids in the brain: d-serine in neurotransmission and neurodegeneration. FEBS J 2008; 275: 3514–3526.
Mustafa AK, Ahmad AS, Zeynalov E, Gazi SK, Sikka G, Ehmsen JT et al. Serine racemase deletion protects against cerebral ischemia and excitotoxicity. J Neurosci 2010; 30: 1413–1416.
Wu S-Z, Bodles AM, Porter MM, Griffin WS, Basile AS, Barger SW . Induction of serine racemase expression and D-serine release from microglia by amyloid-β peptide. J Neuroinflammation 2004; 1: 1–11.
Brito-Moreira J, Paula-Lima AC, Bomfim TR, Oliveira FF, Sepúlveda FJ, Mello FG et al. Aβ oligomers induce glutamate release from hippocampal neurons. Curr Alzheimer Res 2011; 8: 552–562.
Bado P, Madeira C, Vargas-Lopes C, Moulin TC, Wasilewska-Sampaio AP, Maretti L et al. Effects of low-dose d-serine on recognition and working memory in mice. Psychopharmacology 2011; 218: 461–470.
Guercio GD, Bevictori L, Vargas-Lopes C, Madeira C, Oliveira A, Carvalho VF et al. D-serine prevents cognitive deficits induced by acute stress. Neuropharmacology 2014; 86: 1–8.
Di Prisco GV, Huang W, Buffington SA, Hsu CC, Bonnen PE, Placzek AN et al. Translational control of mGluR-dependent long-term depression and object-place learning by eIF2alpha. Nat Neurosci 2014; 17: 1073–1082.
Kumashiro S, Hashimoto A, Nishikawa T . Free D-serine in post-mortem brains and spinal cords of individuals with or without neuropsychiatric diseases. Brain Res 1995; 681: 117–125.
Nagata Y, Borghi M, Fisher GH, D'Aniello A . Free D-serine concentration in normal and Alzheimer human brain. Brain Res Bull 1995; 38: 181–183.
Chouinard ML, Gaitan D, Wood PL . Presence of the N-methyl-D-aspartate-associated glycine receptor agonist, d-serine, in human temporal cortex: comparison of normal, Parkinson, and Alzheimer tissues. J Neurochem 1993; 61: 1561–1564.
Fisher GH, Lorenzo N, Abe H, Fujita E, Frey WH, Emory C et al. Free D- and L-amino acids in ventricular cerebrospinal fluid from Alzheimer and normal subjects. Amino Acids 1998; 15: 263–269.
Grinberg LT, Lucena Ferretti RE, Farfel JM, Leite R, Pasqualucci CA, Rosemberg S et al. Brain bank of the Brazilian aging brain study group—a milestone reached and more than 1,600 collected brains. Cell Tissue Bank 2007; 8: 151–162.
Ferreti R, Damin AE, Brucki SM, Morillo LS, Perroco TR, Campora F et al. Post-mortem diagnosis of dementia by informant interview. Dement Neuropsychol 2010; 4: 138–1441.
Morris JC . The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology 1993; 43: 2412–2412a.
Reis T, Brandão CO, Freire Coutinho ES, Engelhardt E, Laks J . Cerebrospinal fluid biomarkers in Alzheimer's disease and geriatric depression: preliminary findings from Brazil. CNS Neurosci Ther 2012; 18: 524–529.
Calcia MA, Madeira C, Alheira FV, TCS Silva, Tannos FM, Vargas-Lopes C et al. Plasma levels of D-serine in Brazilian individuals with schizophrenia. Schizophr Res 2012; 142: 83–87.
Hashimoto A, Nishikawa T, Hayashi T, Fujii N, Harada K, Oka T et al. The presence of free D-serine in rat brain. FEBS Lett 1992; 296: 33–36.
Sebollela A, Freitas-Correa L, Oliveira FF, Paula-Lima AC, Saraiva LM, Martins SM et al. Amyloid-β oligomers induce differential gene expression in adult human brain slices. J Biol Chem 2012; 287: 7436–7445.
Jurgensen S, Antonio LL, Mussi GE, Brito-Moreira J, Bomfim TR, De Felice FG et al. Activation of D1/D5 dopamine receptors protects neurons from synapse dysfunction induced by amyloid-β oligomers. J Biol Chem 2011; 286: 3270–3276.
Ledo JH, Azevedo EP, Clarke JR, Ribeiro FC, Figueiredo CP, Foguel D et al. Amyloid-β oligomers link depressive-like behavior and cognitive deficits in mice. Mol Psychiatry 2013; 18: 1053–1054.
Lourenco Mychael V, Clarke Julia R, Frozza Rudimar L, Bomfim Theresa R, Forny-Germano L, Batista André F et al. TNF-α mediates PKR-dependent memory impairment and brain IRS-1 inhibition induced by Alzheimer’s β-amyloid oligomers in mice and monkeys. Cell Metab 2013; 18: 831–843.
Jankowsky JL, Slunt HH, Ratovitski T, Jenkins NA, Copeland NG, Borchelt DR . Co-expression of multiple transgenes in mouse CNS: a comparison of strategies. Biomol Eng 2001; 17: 157–165.
Vargas-Lopes C, Madeira C, Kahn SA, Albino do Couto I, Bado P, Houzel JC et al. Protein kinase C activity regulates d-serine availability in the brain. J Neurochem 2011; 116: 281–290.
Panizzutti R, De Miranda J, Ribeiro CS, Engelender S, Wolosker H . A new strategy to decrease N-methyl-D-aspartate (NMDA) receptor coactivation: inhibition of D-serine synthesis by converting serine racemase into an eliminase. Proc Natl Acad Sci USA 2001; 98: 5294–5299.
Livak KJ, Schmittgen TD . Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001; 25: 402–408.
Faul F, Erdfelder E, Buchner A, Lang AG . Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods 2009; 41: 1149–1160.
Wolosker H, Mori H . Serine racemase: an unconventional enzyme for an unconventional transmitter. Amino Acids 2012; 43: 1895–1904.
Wolosker H, Sheth KN, Takahashi M, Mothet J-P, Brady RO, Ferris CD et al. Purification of serine racemase: biosynthesis of the neuromodulator D-serine. Proc Natl Acad Sci USA 1999; 96: 721–725.
Smith DL, Pozueta J, Gong B, Arancio O, Shelanski M . Reversal of long-term dendritic spine alterations in Alzheimer disease models. Proc Natl Acad Sci USA 2009; 106: 16877–16882.
Puzzo D, Staniszewski A, Deng SX, Privitera L, Leznik E, Liu S et al. Phosphodiesterase 5 inhibition improves synaptic function, memory, and amyloid- load in an Alzheimer's disease mouse model. J Neurosci 2009; 29: 8075–8086.
Hulstaert F, Blennow K, Ivanolu A, Schoonderwaldt HC, Riemenschneider M, De Deyn P et al. Improved discrimination of AD patients using β-amyloid(1-42) and tau levels in CSF. Neurology 1999; 52: 1555–1562.
Dauvilliers YA, Lehmann S, Jaussent I, Gabelle A . Hypocretin and brain beta-amyloid peptide interactions in cognitive disorders and narcolepsy. Front Aging Neurosci 2014; 6: 119.
Lehmann S, Schraen S, Quadrio I, Paquet C, Bombois S, Delaby C et al. Impact of harmonization of collection tubes on Alzheimer's disease diagnosis. Alzheimers Dement 2014; 10: e392.
Tabaraud F, Leman JP, Milor AM, Roussie JM, Barriere G, Tartary M et al. Alzheimer CSF biomarkers in routine clinical setting. Acta Neurol Scand 2012; 125: 416–423.
Lehmann S, Dumurgier J, Schraen S, Wallon D, Blanc F, Magnin E et al. A diagnostic scale for Alzheimer’s disease based on cerebrospinal fluid biomarker profiles. Alzheimers Res Ther 2014; 6: 1–9.
Braak H, Braak E . Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol 1991; 82: 239–259.
Armstrong RA, Nochlin D, Bird TD . Neuropathological heterogeneity in Alzheimer’s disease: a study of 80 cases using principal components analysis. Neuropathology 2000; 1: 31–37.
Xia W, Yang T, Shankar GM, Smith IM, Shen Y, Walsh D et al. A specific enzyme-linked immunosorbent assay for measuring β-amyloid protein oligomers in human plasma and brain tissue of patients with Alzheimer disease. Arch Neurol 2009; 66: 190–199.
Gong Y, Chang L, Viola KL, Lacor PN, Lambert MP, Finch CE et al. Alzheimer's disease-affected brain: presence of oligomeric Aβ ligands (ADDLs) suggests a molecular basis for reversible memory loss. Proc Natl Acad Sci USA 2003; 100: 10417–10422.
Kayed R, Head E, Thompson JL, McIntire TM, Milton SX, Cotman CW et al. Common structure of soluble amyloid oligomers implies common mechanism of pathogenesis. Science 2003; 300: 486–489.
Lambert MP, Barlow AK, Chromy BA, Edwards C, Freed R, Liosatos M et al. Diffusible, nonfibrillar ligands derived from Abeta1-42 are potent central nervous system neurotoxins. Proc Natl Acad Sci USA 1998; 95: 6448–6453.
Decker H, Jürgensen S, Adrover MF, Brito-Moreira J, Bomfim TR, Klein WL et al. N-methyl-D-aspartate receptors are required for synaptic targeting of Alzheimer’s toxic Aβ oligomers. J Neurochem 2010; 115: 1520–1529.
Hardingham GE, Bading H . Synaptic versus extrasynaptic NMDA receptor signalling: implications for neurodegenerative disorders. Nat Rev Neurosci 2010; 11: 682–696.
Roselli F, Tirard M, Lu J, Hutzler P, Lamberti P, Livrea P et al. Soluble β-amyloid 1-40 induces NMDA-dependent degradation of postsynaptic density-95 at glutamatergic synapses. J Neurosci 2005; 25: 11061–11070.
Hynd MR, Scott HL, Dodd PR . Selective loss of NMDA receptor NR1 subunit isoforms in Alzheimer's disease. J Neurochem 2004; 89: 240–247.
Mishizen-Eberz AJ, Rissman RA, Carter TL, Ikonomovic MD, Wolfe BB, Armstrong DM . Biochemical and molecular studies of NMDA receptor subunits NR1/2 A/2B in hippocampal subregions throughout progression of Alzheimer's disease pathology. Neurobiol Dis 2004; 15: 80–92.
Ikonomovic MD, Mizukami K, Warde D, Sheffield R, Hamilton R, Wenthold RJ et al. Distribution of glutamate receptor subunit NMDAR1 in the hippocampus of normal elderly and patients with Alzheimer's disease. Exp Neurol 1999; 160: 194–204.
Filali M, Lalonde R . The effects of subchronic d-serine on left–right discrimination learning, social interaction, and exploratory activity in APPswe/PS1 mice. Eur J Pharmacol 2013; 701: 152–158.
Diniz LP, Almeida JC, Tortelli V, Vargas Lopes C, Setti-Perdigao P, Stipursky J et al. Astrocyte-induced synaptogenesis is mediated by transforming growth factor β signaling through modulation of D-serine levels in cerebral cortex neurons. J Biol Chem 2012; 287: 41432–41445.
Esposito S, Pristerà A, Maresca G, Cavallaro S, Felsani A, Florenzano F et al. Contribution of Serine racemase/D-serine pathway to neuronal apoptosis. Aging Cell 2012; 11: 588–98.
Wilson RS, Barnes LL, Mendes de Leon CF, Aggarwal NT, Schneider JS, Bach J et al. Depressive symptoms, cognitive decline, and risk of AD in older persons. Neurology 2002; 59: 364–370.
Ownby RL, Crocco E, Acevedo A, John V, Loewenstein D . Depression and risk for Alzheimer disease: systematic review, meta-analysis and metaregression analysis. Arch Gen Psychiatry 2006; 63: 530–538.
Savage MJ, Kalinina J, Wolfe A, Tugusheva K, Korn R, Cash-Mason T et al. A sensitive a oligomer assay discriminates alzheimer's and aged control cerebrospinal fluid. J Neurosci 2014; 34: 2884–2897.
Mouton-Liger F, Paquet C, Dumurgier J, Lapalus P, Gray F, Laplanche J-L et al. Increased cerebrospinal fluid levels of double-stranded RNA-dependant protein kinase in Alzheimer's disease. Biol Psychiatry 2012; 71: 829–835.
Dumurgier J, Mouton-Liger F, Lapalus P, Prevot V, Laplanche J-L, Hugon J et al. Cerebrospinal fluid PKR level predicts cognitive decline in Alzheimer's disease. PLoS One 2013; 8: e53587.
Harari O, Cruchaga C, Kauwe JSK, Ainscough BJ, Bales K, Pickering EH et al. Phosphorylated Tau-Aβ42 ratio as a continuous trait for biomarker discovery for early-stage Alzheimer’s disease in multiplex immunoassay panels of cerebrospinal fluid. Biol Psychiatry 2014; 75: 723–731.
Fagan AM, Xiong C, Jasielec MS, Bateman RJ, Goate AM, Benzinger TLS et al. Longitudinal change in CSF biomarkers in autosomal-dominant Alzheimer's disease. Sci Transl Med 2014; 6: 226ra230–226ra230.
Acknowledgements
Research was supported by grants from DECIT/SCTIE/MS, SESDC and Fundação de Amparo a Pesquisa do Estado do Rio de Janeiro (FAPERJ) to RP and STF; Conselho Nacional de Desenvolvimento Cientifico e Tecnológico (CNPq) to RP, STF and JL; Instituto Nacional de Ciência e Tecnologia de Biologia Estrutural e Bioimagem to RP; and Instituto Nacional de Neurociência Translacional to STF. RP is a recipient of a Long-Term Fellowship from the Human Frontier Science Program. CM, MVL and CVL were supported by fellowships from FAPERJ and CNPq. The Brain Bank of the Brazilian Aging Brain Study Group is funded by LIM05-FMUSP, Hospital Albert Einstein—Sao Paulo, FAPESP, CNPq and CAPES. We thank all sample donors and their families/caregivers for contributing to this study. We thank AC Rangel for secretarial support and A Fantinatti for technical support.
Disclaimer
Funding agencies had no role in study design, collection, analysis, interpretation of data, writing of the report or the decision by the authors to submit the paper for publication. The Federal University of Rio de Janeiro has intellectual property rights in the use of d-serine as a biomarker in Alzheimer’s disease.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Competing interests
CM, STF and RP are inventors. The remaining authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Translational Psychiatry website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/4.0/
About this article

Cite this article
Madeira, C., Lourenco, M., Vargas-Lopes, C. et al. d-serine levels in Alzheimer’s disease: implications for novel biomarker development. Transl Psychiatry 5, e561 (2015). https://doi.org/10.1038/tp.2015.52
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/tp.2015.52
This article is cited by
-
Fabrication of a polymer brush-functionalized porphyrin-based covalent organic framework for enrichment of N-glycopeptides
Microchimica Acta (2024)
-
Proteomic alterations in the brain and blood–brain barrier during brain Aβ accumulation in an APP knock-in mouse model of Alzheimer’s disease
Fluids and Barriers of the CNS (2023)
-
Detection and analysis of chiral molecules as disease biomarkers
Nature Reviews Chemistry (2023)
-
Synaptic proteasome is inhibited in Alzheimer’s disease models and associates with memory impairment in mice
Communications Biology (2023)
-
Promising applications of D-amino acids in periprosthetic joint infection
Bone Research (2023)
