
Abstract
Whole-genome sequencing (WGS) has the potential to accelerate drug-susceptibility testing (DST) to design appropriate regimens for drug-resistant tuberculosis (TB). Several recently developed automated software tools promise to standardize the analysis and interpretation of WGS data. We assessed five tools (CASTB, KvarQ, Mykrobe Predictor TB, PhyResSE, and TBProfiler) with regards to DST and phylogenetic lineage classification, which we compared with phenotypic DST, Sanger sequencing, and traditional typing results for a collection of 91 strains. The lineage classifications by the tools generally only differed in the resolution of the results. However, some strains could not be classified at all and one strain was misclassified. The sensitivities and specificities for isoniazid and rifampicin resistance of the tools were high, whereas the results for ethambutol, pyrazinamide, and streptomycin resistance were more variable. False-susceptible DST results were mainly due to missing mutations in the resistance catalogues that the respective tools employed for data interpretation. Notably, we also found cases of false-resistance because of the misclassification of polymorphisms as resistance mutations. In conclusion, the performance of current WGS analysis tools for DST is highly variable. Sustainable business models and a shared, high-quality catalogue of resistance mutations are needed to ensure the clinical utility of these tools.
Similar content being viewed by others

Introduction
Tuberculosis (TB) control is threatened by the emergence and spread of resistant Mycobacterium tuberculosis complex (MTBC) strains. In 2015, an estimated 480,000 new cases of multidrug-resistant (MDR, defined as resistant to the most effective first-line drugs isoniazid [INH] and rifampicin [RMP]) TB occurred globally. Of those, approximately 9.5% are extensively drug-resistant (XDR) with additional resistances to at least one fluoroquinolone and one injectable drug1. MDR and XDR TB requires prolonged treatment with more expensive and less effective drugs that can result in severe side effects2.
This situation is exacerbated by the fact that conventional, phenotypic drug-susceptibility testing (DST) can take weeks or months because of the slow growth rate of MTBC3. Targeted genotypic assays, such as line probe assays or the Cepheid Xpert MTB/RIF, have been developed to provide DST results within hours or days4. However, these assays only target the most frequent resistance mutations for a limited number of drugs.
By contrast, whole-genome sequencing (WGS) can theoretically be used to rule-in resistance to all drugs simultaneously, provided that the genetic basis of resistance is elucidated further (WGS directly from the primary sample would be ideal, but is not feasible reliably and cheaply at the moment)5,6,7. Yet, given the amount and complexity of WGS data, its interpretation represents a significant challenge. Specifically, three main steps have to be performed accurately. First, variants (i.e. SNPs, insertions or deletions) have to be identified accurately. Second, these variants have to be interpreted correctly (e.g. mutations that do not confer resistance have to be distinguished from mutations that do)8. Finally, a plain language report that contains clear and appropriate results has to be generated.
To date, three web-servers (CASTB, PhyResSE, and TBProfiler) and two software solutions (KvarQ and Mykrobe Predictor TB) have been developed to enable non-specialists to infer drug resistance from WGS data9,10,11,12,13. Moreover, all tools provide epidemiological typing results, which might be used for contact tracing or surveillance, and can affect patient treatment directly if a member of MTBC is identified that is intrinsically resistant to one or more TB drug14. The respective strengths and weaknesses of all of these tools have not been compared so far15. Using a collection of 91 clinical strains with resistance mutations that were confirmed by classical Sanger sequencing, we therefore set out to assess the performance and functionalities of these tools.
Methods
Evaluation dataset
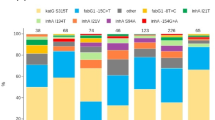
Our collection consisted of 91 strains from Sierra Leone for which phenotypic DST results, WGS data (ENA accession number: PRJEB7727), Sanger sequencing data for key resistance genes (katG, rpoB, embB, rrs, rpsL, gidB, pncA, and, in some cases, inhA, ahpC, embA, and embC), as well as conventional typing data were available (Supplementary Tables S1 and S2). This set of strains has been described before16,17. Half of them were pan-susceptible, whereas the remaining strains were resistant to at least one antibiotic. The strains were highly diverse phylogenetically and comprised both M. africanum genotypes (West African I, n = 6; West African II, n = 14) and ten M. tuberculosis lineages (Beijing, n = 4; Cameroon, n = 4; EAI, n = 4; Ghana, n = 1; Haarlem, n = 11; LAM, n = 15; S-type, n = 3; Sierra Leone I, n = 7; Sierra Leone II, n = 9; X-type, n = 2). Using conventional methods (MIRU-VNTR, IS6110-RFLP, and spoligotyping), the lineage could not be identified for 11 strains. DNA was extracted from cultures as previously described and prepared for sequencing on an Illumina MiSeq benchtop sequencer (251 bp or 301 bp with paired-ends) using the Nextera XT kit according to the manufacturer’s instruction.
Moreover, we analysed three M. bovis genomes to investigate the ability of CASTB to identify intrinsic pyrazinamide (PZA) resistance (4258-00 (ENA accession: ERS457842), 751-01 (ERS458720), and 7540-01 (ERS458073))8.
Software tools
CASTB version 1.1
CASTB is an automated analysis web-server for WGS data from MTBC strains (http:\\castb.ri.ncgm.go.jp\CASTB\). The server provides typing results (using in silico spoligotyping, large sequence polymorphisms, or specific variants) and predicts drug resistance to ciprofloxacin (CFX), ethambutol (EMB), INH, PZA, RMP, and streptomycin (SM) based on SNPs (Table 1)13. The results are stored online for seven days. The resistance prediction (R = resistant; <blank> = not resistant) includes no information about the evidence used in the analysis. We opened three browser tabs to analyse the fastq files of three samples in parallel, as suggested by the authors of the tool.
KvarQ version 0.12.1
KvarQ is a software tool to scan fastq files for known variants9. The source code can be downloaded from GitHub (http://github.com/kvarq/kvarq/releases). Python and a C compiler are required to run the program. In the default setting, the user can choose between two so-called ‘testsuites’ for M. tuberculosis, which are collections of short sequences in a reference genome. The output is given in the ‘JavaScript Object Notation’ (json) format. The resistance catalogue includes variants located within 63 bp of gyrA, 81 bp of rpoB, 3 bp of katG and 561 bp of pncA (Supplementary Table S3). To analyse our WGS data, we had to merge our paired-end data for each strain into a single file. We used the default settings and standard MTBC testsuites to scan the fastq files. Finally, we produced a table that included all results using the summary-command, which is only available in the command-line version.
Mykrobe Predictor TB version 0.1.3
Mykrobe Predictor TB is designed for rapid antibiotic resistance prediction and species identification from WGS data of M. tuberculosis10. The tool and source-code can be downloaded via GitHub (https:\\github.com\iqbal-lab\Mykrobe-predictor\releases). The resistance panel consists of mutations in 62 codons; 27 in rpoB, one in katG, four in inhA, ten in gyrA, 14 in rrs, three in embB, two in rpsL and one in eis (Supplementary Table S3) to detect resistance against the drugs shown in Table 1. PZA is not included. Mykrobe Predictor TB is specifically designed to detect low-frequency resistance mutations. Therefore, Mykrobe Predictor TB reports even minor alleles at the positions included in the aforementioned list of resistance loci, but does not interpret them. We used the program with merged fastq files.
PhyResSE version 1.0
PhyResSE is a web-server for lineage identification and resistance prediction based on raw WGS data (www.phyresse.org)12. Its mutation catalogue is based on both a literature review and experimental data. The catalogue (Version 27) comprises 301 variants to predict resistance to 12 antibiotics (Table 1; Supplementary Table S3) and 239 SNPs in 135 genes for phylogenetic typing. We analysed our paired-end data using the batch mode and relied on the summary function to produce a table with the results for all strains.
TBProfiler
TBProfiler is a web-server that reports drug resistance and strain-type profiles (http:\\tbdr.lshtm.ac.uk\)11. Its output comprises resistance predictions for 11 antibiotics (Table 1) as well as information on the resistance mutation in question and further mutations in 22 candidate genes. Resistance predictions are based on a catalogue (including SNPs and indels) with 902 nucleotide positions at 26 loci that comprise six promotors and 20 coding regions (Supplementary Table S3). We ran the program offline after installing it locally (downloaded and installed 01\2016).
Statistical analyses
Sensitivities and specificities, including the corresponding 95% confidence intervals, were calculated using the statistical software R (Version 3.1.0).
Results
Functionality
We compared CASTB, KvarQ, Mykrobe Predictor TB, PhyResSE and TBProfiler with regards to their handling, outputs, adjustability and ability to perform contamination checks. The full results of this comparison can be found in Table 2, but the following differences were notable.
Only KvarQ and PhyResSE offer batch uploads, which meant that all 91 strains from our collection could be uploaded in parallel and processed automatically. The other tools either have no batch mode at all (CASTB, TBProfiler) or can only analyse files in batches in the command-line version (Mykrobe Predictor TB). Moreover, paired-end fastq files have to be merged for KvarQ and Mykrobe Predictor TB, which may represent a challenge for some users.
The ability to export and store the outputs differed significantly between the tools. In the case of PhyResSE, the complete reports for all strains analysed in the same session can be exported easily as a ‘comma separated values’ (csv) file. Similar ‘batch mode’ reports were not available for CASTB or limited to the command-line version of KvarQ. Customised perl scripts were required to obtain comparable reports for Mykrobe Predictor TB and TBProfiler. The results of single strains can be stored in the json format for Mykrobe Predictor TB and KvarQ, whereas PhyResSE and CASTB used the csv format. By contrast, no dedicated export and storage function exists for TBProfiler.
A further important difference between the tools was the ease in which they could be updated. Specifically, it is important to refine the list of resistance variants whenever the understanding of the genetic basis of antibiotic resistance improves. Currently, only PhyResSE allows users to extend the existing list of resistance mutations by simply updating a downloadable list of variants. For CASTB no adjustments are possible, whereas for the remaining tools more advanced skills are needed. In the case of TBProfiler, adjustments are possible by editing the source code. The testsuites, which are Python source files, can be changed for KvarQ. A code generator in Python is provided to modify the variant list of Mykrobe Predictor TB.
Phylogenetic lineage classification
Each tool differs in its approach for epidemiological typing. CASTB is the only tool that interrogates large sequence polymorphisms, whereas all other tools rely exclusively on SNPs, but use different SNP catalogues. KvarQ combines SNPs from Comas et al. and Stucki et al.17, whereas Mykrobe Predictor TB only uses the latter study18,19. The SNP catalogues from Homolka et al. and Coll et al. form the basis of the classification in PhyResSE16,20. TBProfiler only employs the scheme from Coll et al.20 Despite these varied approaches, the results for 73 strains only differed in their resolution (i.e. tools that rely on Coll et al., which represents the most advanced typing scheme to date, provided the best resolution at the sub-lineage level)20. All tools classified the 11 strains, for which our classical experimental techniques had failed to provide a result (Table 3).
Of the remaining seven discrepancies, six might have affected contact tracing only (i.e. all six M. africanum West African 1 strains were reported as ‘unknown species’ by Mykrobe Predictor TB). By contrast, the misclassification of the M. tuberculosis Latin-American Mediterranean (LAM) strain 10205-03 (ERS457959) as M. bovis by CASTB might have resulted in a major diagnostic error if PZA resistance had been inferred, given that M. bovis is intrinsically resistant to this antibiotic14,21. The strain was in fact phenotypically susceptible and did not harbor any pncA mutations (Supplementary Table S3). Notably, it was not reported as PZA resistant by CASTB. However, in light of the fact that CASTB does not provide a list of mutations used to infer resistance, it would be reasonable for a user of the tool to assume that the mutation responsible for intrinsic resistance in M. bovis (pncA H57D) was missing from the catalogue, which would explain the apparent susceptible result based on pncA (the mutation does, indeed, appear not to feature in the catalogue given that our three M. bovis strains were not reported as PZA resistant by the tool)14.
As a consequence, KvarQ, PhyResSE and TBProfiler showed an accuracy of 100% for lineage identification, whereas the accuracy of CASTB and Mykrobe Predictor TB were 98.9% and 93.4%, respectively.
Resistance prediction
The sensitivities and specificities for predicting resistance compared with phenotypic DST varied significantly between the different tools and antibiotics (Table 4). Whereas sensitivities and specificities for INH and RMP were high for all tools evaluated, this was much more variable for the other first-line drugs. In fact, the sensitivities for four tool-drug combinations ranged between just 22–44% (Table 4). The equivalent values with Sanger sequencing as the reference standard can be found in Supplementary Table S4.
Incorrect resistance predictions can either arise because of four factors (see discussion for more details):
- a
The inadequate limit of detection of the genotypic method,
- b
Errors in variant calling,
- c
Incorrect interpretation of variants (using the mutation catalogues in Supplementary Table S3), or
- d
Errors in phenotypic DST.
CASTB
In the case of CASTB, we were unable to dissect these sources of error since this tool does not provide an output of the variants identified in a particular sample. Moreover, the authors of this tool have not included a list of mutations that are used to predict resistance (the genes shown in Table 1 were inferred based on the analyses for this study). As a result, we were only able to conclude that 61 out of 66 resistance calls by this tool were valid compared with phenotypic DST, but could not assess whether these predictions were based on the correct mutations, as opposed to another mutation that happened to occur in the strains in question. However, 41 cases of resistance were missed compared with phenotypic DST.
Differences in variant calling
Differences in variant calling in regions, for which Sanger data were available, were observed in 11 cases (Supplementary Table S2). In eight of those cases, involving one katG and seven rpoB mutations, Mykrobe Predictor TB reported minor mutations that did not meet the threshold to be reported as causing resistance. These occurred in strains that were INH and RMP susceptible, respectively. The corresponding Sanger results did not support the presence of minor resistance mutations. We investigated this further by examining the Stampy-mapped WGS data with the Integrative Genome Viewer. This showed that the majority of mutated bases had low quality scores (below 15, i.e. the probability of being called incorrectly is above 3%), which suggested that these were likely sequencing errors (Supplementary Table S2 and Figure S1). Because these mutations were detected, but not reported to cause resistance, we did not regard these as errors when calculating the sensitivities and specificities of the WGS analysis tools (Table 4 and Supplementary Table S4).
Heteroresistance was the cause for differences in variant calling in three cases. The rpoB L452P and embB M306I mutations, which were reported by at least one WGS tool, were originally missed by Sanger sequencing in strains 8082-03 and 8867-03, respectively. A re-examination of the electropherograms for both strains confirmed the presence of these mutations (data not shown). Based on an inspection of the mapped WGS data, strain 10517-03 contained at least two rpoB populations. The T400A and S450L mutations occurred in the same population at approximately 65% of the total. The H445Y occurred at about 21% and was initially missed by Sanger sequencing. PhyResSE and TBProfiler reported both populations. A third potential population with an S441L mutation, which was not detectable using Sanger sequencing as it had a frequency of just 14%, was reported by Mykrobe Predictor TB as a low-quality call and was consequently not interpreted (Z. Iqbal, personal communication). Mykrobe Predictor TB did not report the S450L mutation despite the fact that, unlike the T400A mutation, S450L is listed of its resistance catalogue (Supplementary Table S3). This was due to a bug in the software, which is due to be corrected (Z. Iqbal, personal communication).
Differences in interpretation
Differences in interpretation of mutations, for which Sanger data were available, accounted for most differences in resistance predictions. Specifically, 52 mutations were not reported by at least one WGS analysis tool because they do not feature in the respective lists that each tool relies on for the interpretation of variants (10 for PhyResSE, 35 for KvarQ, 40 for Mykrobe Predictor TB, and 24 for TBProfiler, as shown in Table 5). It was unclear why the embB G406D mutation in strain 1599-04 was not reported by Mykrobe Predictor TB despite featuring in the resistance catalogue of this tool. This issue has been corrected in a recently released version of the tool.
Other cases
There were 18 cases in which resistance mutations were reported by at least one tool, for which no Sanger data were available (Supplementary Table S5). All of these mutations were called correctly based on an inspection of the WGS data. In six of these cases (strains 3156-04, 4139-04, 8864-03, 10011-03, 2509-04, and 7520-04) this did not make a difference for predicting INH resistance given that they coincided with INH resistance mutations elsewhere in the genome that were interpreted. In two strains the detection of these additional mutations increases the sensitivity compared with phenotypic DST (4518-03 and 8868-03)22,23.
For seven strains, TBProfiler inferred INH resistance based on the kasA G269S mutation, resulting in false-resistant results. However, allelic exchange experiments have demonstrated that this mutation does not confer INH resistance23. In accordance with this observation, the authors of TBProfiler had recognised that this was merely a phylogenetic marker for a subgroup of the LAM family11,20. Yet, contrary to Supplementary Table 2 in Coll et al., in which they claim to have excluded this mutation, kasA G269S features in their resistance catalogue (Supplementary Table S3), which accounted for the incorrect interpretation of this mutation11.
Finally, TBProfiler reported 12657-03 and 11096-03 to be resistant to INH and EMB because of ahpC C-81T and embB Q497P mutations, respectively. The role of both mutations is poorly understood and both strains tested susceptible to the respective drugs (Supplementary Table S5).
False-resistance compared with phenotypic DST
In total 23 strains were reported as resistant by at least one genotypic method. In addition to the strains discussed above, two cases of false-resistance to EMB, two to INH, four to PZA, five to RMP, and one to SM were observed (Supplementary Table S6).
False-susceptibility compared with phenotypic DST
There were three resistances that were missed by Sanger as well as all WGS analysis tools (Supplementary Table S6).
Discussion
In this study, we performed the most comprehensive comparison of five software pipelines for the automated analysis and interpretation of WGS data of MTBC strains to date. Unlike more general WGS analysis pipelines, the ultimate goal for these tools is to be used clinically, as opposed to research. Consequently, their DST results based on either the species identification or the detection and interpretation of resistance variants need to be highly accurate and standardized.
We had expected that false-susceptible results would occur because of differences in variant calling of heteroresistant strains (i.e. phenotypic DST can detect resistance at 1% (or 10% in the case of PZA), whereas the limit of detection of WGS depends on the sequence coverage24) and because of resistance mutations that did not feature in the catalogues used for the interpretation of variants, as shown by Phelan et al., who recently compared TBProfiler and Mykrobe Predictor TB using 10 clinical strains15. Specifically, we found that differences in interpretation mainly affected EMB, PZA, and SM, for which the genetic basis of resistance is more complex than for RMP and INH.
Yet, we had not expected false-resistance calls because of the inappropriate interpretation of known polymorphisms that do not cause resistance, as was the case with TBProfiler and the kasA G269S mutation with regards to INH, a key drug for the treatment of TB (Supplementary Table S6)14. Notably, this flaw appeared to be specific to the command-line version of TBProfiler, whereas the online version interpreted this mutation correctly (data not shown). In a separate study, we found an additional example in which KvarQ, Mykrobe Predictor TB, and TBProfiler generated false-resistance results to fluoroquinolones with the gyrA T80A+A90G double mutations25. This underlines the importance of developing a clinical-grade database to interpret resistance mutations, as is currently underway with the ReSeqTB initiative14,26. However, it has to be appreciated that new resistance mutations will continue to be discovered over time, particularly in non-essential genes where the spectrum of resistance mutations is large6. Therefore, genotypic assays, including WGS, should generally only be used as tools to rule-in resistance and phenotypic DST will still be needed to confirm susceptibility4.
By contrast, the remaining 15 cases of false-susceptibility were likely mostly due to problems with phenotype rather than the genotypic results (Supplementary Table S6). For example, mutations in embB are known to result in only slight MIC increases to EMB, which means that the MIC distributions of wild-type and mutated strains overlap, unless secondary mutations increase the MICs even further27,28,29,30. Similarly, several rpoB mutations are known to test susceptible in MGIT, but resistant on Löwenstein-Jensen medium31,32,33. These false-susceptible results with MGIT are likely due to a breakpoint artefact (i.e. because the critical concentration is set above the epidemiological cut-off)4,34,35. A thorough re-evaluation of the critical concentrations using modern principles is the only option to resolve these systematic differences4,24,36.
We also had not anticipated to find a case in which the misidentification of an M. tuberculosis strain as M. bovis by CASTB would result in a false-resistance result to PZA, if this species identification was used as a surrogate for intrinsic resistance to this drug14. Importantly, we were not able to investigate what the reason for this error was, since CASTB takes automation to an extreme by providing very little information on how it works and no evidence at all about variants detected in a particular strain that were used to infer resistance or the lineage. In our view, tools that function as complete ‘black boxes’ should not be used clinically since their independent assessment is only possible by trial and error (e.g. we actually had to analyse three M. bovis strains to ascertain that the pncA H57D does not feature in its resistance catalogue).
From the point of view of addressing the discrepancies identified in this study, the errors fall into two groups. Both false-positives and false-negative results due to incorrect variant interpretation can be solved by simply updating the resistance catalogues, although, in practice, this is easier for some tools than others, as outlined in the ‘functionality’ section above. By contrast, differences in variant calling and the ease of use of the tools would require more extensive modifications. This includes improved algorithms for the detection of resistance caused by insertions and deletions, particularly in heteroresistant strains4,24,37. In this context, we would recommend for Mykrobe Predictor TB not to report low-quality, low-frequency mutations even if these are not interpreted. In our view, software tools should only report high-quality mutations in order not to risk that inexperienced users reach wrong conclusions (e.g. it was not clear from the output for 10517-03 which rpoB mutation the tool had used to infer RMP resistance).
This raises a more fundamental question. We believe that the central issue is not which tool is currently ‘best’, but how these tools will be maintained and improved. The recent interest by academics in translating WGS, which has resulted in the development of the tools investigated in this study, is a welcome development. However, none of the tools currently combines all features needed to meet regulatory requirements, such as record-keeping capabilities and version control38. Even if they did, academics would be unlikely to maintain and refine these tools (e.g. to adjust them to solve yet unknown reasons for incorrect variant calling or to accommodate novel sequencing technologies). Instead, viable models are called for that ensure the longevity of analysis tools, whilst preventing private monopolies, as has been the case with genetic testing in other areas39.
Additional Information
How to cite this article: Schleusener, V. et al. Mycobacterium tuberculosis resistance prediction and lineage classification from genome sequencing: comparison of automated analysis tools. Sci. Rep. 7, 46327; doi: 10.1038/srep46327 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
World Health Organization. Global tuberculosis report 2016.http://apps.who.int/iris/bitstream/10665/250441/1/9789241565394-eng.pdf. OCLC: 961271202 (2016).
Horsburgh, C. R. J., Barry, C. E. I. & Lange, C. Treatment of Tuberculosis. New England Journal of Medicine 373, 2149–2160. http://dx.doi.org/10.1056/NEJMra1413919, doi: 10.1056/NEJMra1413919 (2015).
Köser, C. U. et al. Routine Use of Microbial Whole Genome Sequencing in Diagnostic and Public Health Microbiology. PLoS Pathogens 8, e1002824. http://dx.doi.org/10.1371/journal.ppat.1002824, doi: 10.1371/journal.ppat.1002824 (2012).
Schön, T. et al. Mycobacterium tuberculosis drug-resistance testing: challenges, recent developments and perspectives. Clinical Microbiology and Infection: The Official Publication of the European Society of Clinical Microbiology and Infectious Diseases, doi: 10.1016/j.cmi.2016.10.022 (2016).
Köser, C. U. et al. Whole-Genome Sequencing for Rapid Susceptibility Testing of M. tuberculosis. The New England journal of medicine 369. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3836233/, doi: 10.1056/NEJMc1215305 (2013).
Walker, T. M. et al. Whole-genome sequencing for prediction of Mycobacterium tuberculosis drug susceptibility and resistance: a retrospective cohort study. The Lancet. Infectious Diseases, 15, 1193–1202. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4579482/, doi: 10.1016/S1473-3099(15)00062-6 (2015).
McNerney, R. et al. Removing the bottleneck in whole genome sequencing of Mycobacterium tuberculosis for rapid drug resistance analysis: a call to action. International journal of infectious diseases: IJID: official publication of the International Society for Infectious Diseases, doi: 10.1016/j.ijid.2016.11.422 (2016).
Feuerriegel, S., Köser, C. U. & Niemann, S. Phylogenetic polymorphisms in antibiotic resistance genes of the Mycobacterium tuberculosis complex. The Journal of Antimicrobial Chemotherapy 69, 1205–1210, doi: 10.1093/jac/dkt535 (2014).
Steiner, A., Stucki, D., Coscolla, M., Borrell, S. & Gagneux, S. KvarQ: targeted and direct variant calling from fastq reads of bacterial genomes. BMC Genomics 15, 881. http://www.biomedcentral.com/1471-2164/15/881/abstract, doi: 10.1186/1471-2164-15-881 (2014).
Bradley, P. et al. Rapid antibiotic-resistance predictions from genome sequence data for Staphylococcus aureus and Mycobacterium tuberculosis. Nature Communications 6, 10063. http://www.nature.com/ncomms/2015/151221/ncomms10063/full/ncomms10063.html, doi: 10.1038/ncomms10063 (2015).
Coll, F. et al. Rapid determination of anti-tuberculosis drug resistance from whole-genome sequences. Genome Medicine 7, 51. http://genomemedicine.com/content/7/1/51/abstract, doi: 10.1186/s13073-015-0164-0 (2015).
Feuerriegel, S. et al. PhyResSE: a Web Tool Delineating Mycobacterium tuberculosis Antibiotic Resistance and Lineage from Whole-Genome Sequencing Data. Journal of Clinical Microbiology 53, 1908–1914, doi: 10.1128/JCM.00025-15 (2015).
Iwai, H., Kato-Miyazawa, M., Kirikae, T. & Miyoshi-Akiyama, T. CASTB (the comprehensive analysis server for the Mycobacterium tuberculosis complex): A publicly accessible web server for epidemiological analyses, drug-resistance prediction and phylogenetic comparison of clinical isolates. Tuberculosis (Edinburgh, Scotland) 95, 843–844, doi: 10.1016/j.tube.2015.09.002 (2015).
Köser, C. U., Feuerriegel, S., Summers, D. K., Archer, J. A. C. & Niemann, S. Importance of the Genetic Diversity within the Mycobacterium tuberculosis Complex for the Development of Novel Antibiotics and Diagnostic Tests of Drug Resistance. Antimicrobial Agents and Chemotherapy 56, 6080–6087. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3497208/, doi: 10.1128/AAC.01641-12 (2012).
Phelan, J. et al. The variability and reproducibility of whole genome sequencing technology for detecting resistance to anti-tuberculous drugs. Genome Medicine 8, 132, doi: 10.1186/s13073-016-0385-x (2016).
Homolka, S. et al. High genetic diversity among Mycobacterium tuberculosis complex strains from Sierra Leone. BMC Microbiology 8, 103. http://www.biomedcentral.com/1471-2180/8/103/abstract, doi: 10.1186/1471-2180-8-103 (2008).
Feuerriegel, S. et al. Sequence analysis for detection of first-line drug resistance in Mycobacterium tuberculosis strains from a high-incidence setting. BMC Microbiology 12, 90. http://www.biomedcentral.com/1471-2180/12/90/abstract, doi: 10.1186/1471-2180-12-90 (2012).
Stucki, D. et al. Two New Rapid SNP-Typing Methods for Classifying Mycobacterium tuberculosis Complex into the Main Phylogenetic Lineages. PLoS ONE 7, e41253. http://dx.doi.org/10.1371/journal.pone.0041253, doi: 10.1371/journal.pone.0041253 (2012).
Comas, I., Homolka, S., Niemann, S. & Gagneux, S. Genotyping of Genetically Monomorphic Bacteria: DNA Sequencing in Mycobacterium tuberculosis Highlights the Limitations of Current Methodologies. PLoS ONE 4, e7815. http://dx.doi.org/10.1371/journal.pone.0007815, doi: 10.1371/journal.pone.0007815 (2009).
Coll, F. et al. A robust SNP barcode for typing Mycobacterium tuberculosis complex strains. Nature Communications 5. http://www.nature.com/ncomms/2014/140901/ncomms5812/full/ncomms5812.html, doi: 10.1038/ncomms5812 (2014).
US Food and Drug Administration. Class II Special Controls Guidance Document: Antimicrobial Susceptibility Test (AST) Systems. http://www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/ucm388961.pdf (2009).
Miotto, P. et al. Mycobacterium tuberculosis pyrazinamide resistance determinants: a multicenter study. mBio 5, e01819–01814, doi: 10.1128/mBio.01819-14 (2014).
Vilchèze, C. et al. Transfer of a point mutation in Mycobacterium tuberculosis inhA resolves the target of isoniazid. Nature Medicine 12, 1027–1029, doi: 10.1038/nm1466 (2006).
Ellington, M. J. et al. The role of whole genome sequencing in antimicrobial susceptibility testing of bacteria: report from the EUCAST Subcommittee. Clinical Microbiology and Infection: The Official Publication of the European Society of Clinical Microbiology and Infectious Diseases 23, 2–22, doi: 10.1016/j.cmi.2016.11.012 (2017).
Ajileye, A. et al. Some synonymous and nonsynonymous gyrA mutations in Mycobacterium tuberculosis lead to systematic false-positive fluoroquinolone resistance results with the Hain GenoType MTBDRsl assays. Antimicrobial Agents and Chemotherapy, 61, e02169-16, doi: 10.1128/AAC.02169-16 (2017).
Starks, A. M. et al. Collaborative Effort for a Centralized Worldwide Tuberculosis Relational Sequencing Data Platform. Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America 61 Suppl 3, S141–146, doi: 10.1093/cid/civ610 (2015).
Böttger, E. C. The ins and outs of Mycobacterium tuberculosis drug susceptibility testing. Clinical Microbiology and Infection: The Official Publication of the European Society of Clinical Microbiology and Infectious Diseases 17, 1128–1134, doi: 10.1111/j.1469-0691.2011.03551.x (2011).
Safi, H. et al. Evolution of high-level ethambutol-resistant tuberculosis through interacting mutations in decaprenylphosphoryl-β-D-arabinose biosynthetic and utilization pathway genes. Nature Genetics 45, 1190–1197, doi: 10.1038/ng.2743 (2013).
Yakrus, M. A. et al. Molecular and Growth-Based Drug Susceptibility Testing of Mycobacterium tuberculosis Complex for Ethambutol Resistance in the United States. Tuberculosis Research and Treatment 2016, 3404860, doi: 10.1155/2016/3404860 (2016).
World Health Organization. Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-Resistant Tuberculosis. WHO Guidelines Approved by the Guidelines Review Committee. http://www.ncbi.nlm.nih.gov/books/NBK247420/ (World Health Organization, Geneva, 2014).
Rigouts, L. et al. Rifampin resistance missed in automated liquid culture system for Mycobacterium tuberculosis isolates with specific rpoB mutations. Journal of Clinical Microbiology 51, 2641–2645, doi: 10.1128/JCM.02741-12 (2013).
Van Deun, A. et al. Disputed rpoB mutations can frequently cause important rifampicin resistance among new tuberculosis patients. The International Journal of Tuberculosis and Lung Disease: The Official Journal of the International Union Against Tuberculosis and Lung Disease 19, 185–190, doi: 10.5588/ijtld.14.0651 (2015).
Gonzalo, X. et al. True rifampicin resistance missed by the MGIT: prevalence of this pheno/genotype in the UK and Ireland after 18 month surveillance. Clinical Microbiology and Infection: The Official Publication of the European Society of Clinical Microbiology and Infectious Diseases, doi: 10.1016/j.cmi.2016.11.015 (2016).
ängeby, K., Juréen, P., Kahlmeter, G., Hoffner, S. E. & Schön, T. Challenging a dogma: antimicrobial susceptibility testing breakpoints for Mycobacterium tuberculosis. Bulletin of the World Health Organization 90, 693–698, doi: 10.2471/BLT.11.096644 (2012).
Heyckendorf, J. et al. What is resistance? Impact of genotypic drug-resistance testing on the therapy of multidrug resistant tuberculosis. American Journal of Respiratory and Critical Care Medicine (submitted).
Kahlmeter, G. The 2014 Garrod Lecture: EUCAST - are we heading towards international agreement? The Journal of Antimicrobial Chemotherapy 70, 2427–2439, doi: 10.1093/jac/dkv145 (2015).
Moradigaravand, D. et al. dfrA thyA Double Deletion in para-Aminosalicylic Acid-Resistant Mycobacterium tuberculosis Beijing Strains. Antimicrobial Agents and Chemotherapy 60, 3864–3867 doi: 10.1128/AAC.00253-16 (2016).
Wyres, K. et al. WGS Analysis and Interpretation in Clinical and Public Health Microbiology Laboratories: What Are the Requirements and How Do Existing Tools Compare? Pathogens 3, 437–458. http://www.mdpi.com/2076-0817/3/2/437/, doi: 10.3390/pathogens3020437 (2014).
Köser, C. U. et al. Drug-resistance mechanisms and tuberculosis drugs. Lancet (London, England) 385, 305–307, doi: 10.1016/S0140-6736(14)62450-8 (2015).
Acknowledgements
We would like to thank Zamin Iqbal for his help regarding Mykrobe Predictor TB.
Author information
Authors and Affiliations
Contributions
V.S. and C.U.K. wrote the main manuscript text and V.S. prepared all tables. P.B. and S.F. analyzed and interpreted the Sanger data. S.N. made substantial contributions to conception and design of the study. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
C.U.K. has collaborated with Illumina Inc. on a number of scientific projects and is a consultant for the Foundation for Innovative New Diagnostics. The Bill & Melinda Gates Foundation, PerkinElmer, and Janssen Pharmaceutica covered C.U.K.’s travel and accommodation to present at meetings. The European Society of Mycobacteriology awarded C.U.K. the Gertrud Meissner Award, which is sponsored by Hain Lifescience. S.N. is a consultant for the Foundation for Innovative New Diagnostics.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Schleusener, V., Köser, C., Beckert, P. et al. Mycobacterium tuberculosis resistance prediction and lineage classification from genome sequencing: comparison of automated analysis tools. Sci Rep 7, 46327 (2017). https://doi.org/10.1038/srep46327
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep46327
This article is cited by
-
TB-DROP: deep learning-based drug resistance prediction of Mycobacterium tuberculosis utilizing whole genome mutations
BMC Genomics (2024)
-
A Profile of Drug-Resistant Mutations in Mycobacterium tuberculosis Isolates from Guangdong Province, China
Indian Journal of Microbiology (2024)
-
Whole genome sequencing analysis to evaluate the influence of T2DM on polymorphisms associated with drug resistance in M. tuberculosis
BMC Genomics (2022)
-
INGOT-DR: an interpretable classifier for predicting drug resistance in M. tuberculosis
Algorithms for Molecular Biology (2021)
-
Prediction of rifampicin resistance beyond the RRDR using structure-based machine learning approaches
Scientific Reports (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
