
Abstract
Stepped care is an increasingly popular treatment model for common mental health disorders, given the large discrepancy between the demand and supply of healthcare service available. In this review, we aim to compare the efficacy and cost-effectiveness of stepped care prevention and treatment with care-as-usual (CAU) or waiting-list control for depressive and/or anxiety disorders. 5 databases were utilized from its earliest available records up until April 2015. 10 randomized controlled trials were included in this review, of which 6 examined stepped care prevention and 4 examined stepped care treatment, specifically including ones regarding depressive and/or anxiety disorders. Only trials with self-help as a treatment component were included. Results showed stepped care treatment revealed a significantly better performance than CAU in reducing anxiety symptoms and the treatment response rate of anxiety disorders was significantly higher in stepped care treatment than in CAU. No significant difference was found between stepped care prevention/treatment and CAU in preventing anxiety and/or depressive disorders and improving depressive symptoms. In conclusion, stepped care model appeared to be better than CAU in treating anxiety disorders. The model has the potential to reduce the burden on existing resources in mental health and increase the reach and availability of service.
Similar content being viewed by others

Introduction
Depressive and anxiety disorders bring severe health and financial burdens to the sufferers and the public1,2. Although extensive evidence has shown that psychological treatment is effective in treating depressive and anxiety disorders3,4,5, resource constraints limit its reach, especially in countries with developing economies. Per 100,000 people in low-income countries, there are merely 5% and 4% of them that are psychiatrists and psychologists respectively6. Given the significant discrepancies between the demand for evidence-based psychotherapy and the availability of healthcare professionals7, it is crucial to make efficient use of the limited healthcare resources to maximize the number of beneficiaries.
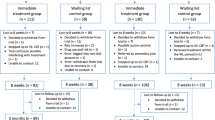
Recently, stepped care model is considered as one of the possible solutions to reduce the existing healthcare burden8. Within the stepped care model (Supplementary Fig. S1), evidence-based psychological treatments are distributed to different steps9. This starts with less intensive treatments, for example, through self-help treatments delivered through the internet10, bibliotherapy11, and/or group therapy12, to more intensive treatments involving individual therapy provided by specialists13 and possibly subsequent pharmacological treatment14. Stepped care model as a healthcare delivery method has two core features, “least restrictive” and “self-correcting”15. “Least restrictive” refers to a low-intensity, cost effective and least time consuming feature of this method and is used as the first-line treatment. “Self-correcting” refers to the “stepping-up” criteria that are utilized in possible preparation of more intensive and expensive treatment and this is necessary based on treatment outcome. Patients are monitored systematically and referred to the next step if they do not respond significantly to the prior steps in the model. A care manager or psychiatric nurse is sometimes assigned to coordinate the treatment program, monitor the progress and assist patients to decide the level of treatment, all of which take into account of the severity of their symptoms16. The advantage of the stepped care model is that it maximizes the effectiveness and efficiency of treatments by optimizing resource allocation.
Currently, stepped care model is recommended in the clinical guidelines by the National Institute for Health and Clinical Excellence in the United Kingdom for common mental health problems8. The model has been implemented and evaluated for various mental health problems such as eating disorders17, depression and anxiety18, obsessive-compulsive disorder19, posttraumatic stress disorder20, chronic fatigue syndrome21, nicotine dependence22 and alcohol use disorders23. The findings of some of these randomized controlled trials (RCTs) support the clinical benefits of stepped care approach. For example, stepped care treatment was found superior than CAU in treating eating disorders in a 1-year follow-up17 and alcohol use disorders in a 6-month follow-up23. On the other hand, other clinical trials failed to show significant outcome differences between the stepped care and CAU groups18. Nonetheless, the stepped care model appears to be more cost effective than traditional approaches. For example, stepped care was more cost effective in comparison to traditional cognitive-behavioral therapy (CBT) in treating bulimia nervosa24. The cost per abstinent subject of stepped care and traditional CBT were USD $12,146 and USD $20,317 respectively.
Given the potential benefits of the stepped care model on the one hand and the structural constraints of traditional modes of treatment delivery on the other, it would be of interest to systematically examine its clinical efficacy and cost effectiveness. To our knowledge, there are only two systematic reviews that summarized the efficacy of the stepped care model; one for alcohol use disorders and nicotine dependence25 and the other for depression26. The former found little evidence to conclude that the stepped care model is superior to CAU in terms of treatment outcome but they recognized that this might be partially due to insufficient statistical power. The latter, on the other hand, found moderate effect size in treating depression, but had limited evidence to conclude that stepped care should be the dominant treatment model. The review by van Straten26 has summarized the studies on stepped care model as a treatment intervention for depression, but the review did not include studies on stepped care model as a preventive intervention, which has important clinical and public health implication.
There is great heterogeneity in the architecture of stepped care model, in terms of the number of steps and treatment components incorporated, which may limit the generalizability of the results in previous meta-analysis26. We argue that self-help is a crucial first treatment step in the model because of its cost effectiveness and least restrictive nature. The inclusion of self-help treatment has the advantage of allowing a larger proportion of patients to reach the service, especially for individuals who are not able to afford pharmacotherapy or psychotherapy and/or those who have geographical or transportation constraints27,28. However, to date, there is no systematic review and meta-analysis of stepped care prevention and treatment for depressive and anxiety disorders that specifically investigated studies using self-help treatment as the first step in stepped care model. Given these knowledge gaps, we conducted a meta-analysis of RCTs that examined the efficacy of stepped care vis-à-vis CAU or waiting-list (WL) as a treatment or prevention intervention for depression or/and anxiety. We included both prevention and intervention studies. Furthermore, cost-effectiveness of stepped care approach was also evaluated.
Methods
Selection of Studies
Two authors (FYH and THN) independently searched electronic databases, including Cochrane Central Register of Controlled Trials, PubMed, PsycINFO, CINAHL Plus and ProQuest Dissertations & Theses from the earliest available records to April 2015. The search terms were indicative of stepped care treatment and prevention and RCTs: (psychotherapy OR psychological treatment OR cognitive-behavioral OR CBT OR mental OR counsel*) AND (random* OR controlled trial OR randomized controlled trial OR RCT) AND (stepped care OR adjunctive treatment OR treatment tiering OR adaptive treatment). The combination of terms was searched by title, abstract or keyword. We also searched for additional relevant articles from the reference lists of retrieved papers. We did not set any restrictions for duration of treatment, outcome measure or study quality.
Studies that employed stepped care model as a treatment or prevention intervention for depressive and/or anxiety disorders were included in this review. Prevention referred to intervention provided to people with high risk or subthreshold symptoms of depressive and anxiety disorders; whereas treatment referred to intervention given to those with a diagnosis of a depressive and/or anxiety disorder. Our inclusion criteria were the following: (1) studies examining stepped care treatment or prevention in comparison with CAU or WL; (2) participants with depressive and/or anxiety disorders diagnosed by standard diagnostic criteria such as Diagnostic and Statistical Manual of Mental Disorders (DSM-IV or DSM-5) or chief complaint of depressive and/or anxiety symptoms assessed by standardized measures; and (3) studies with self-help as the first treatment step in stepped care model (i.e., “least restrictive”) without a combination of non-self-help treatments, because self-help was considered appropriate to be the first line treatment due to its low cost and wide availability27,29. We excluded studies with no “stepping-up” criteria (i.e., “self-correcting”). Collaborative care RCTs were considered as eligible if both the inclusion and exclusion criteria were met.
Data Extraction
Data extraction was performed by two authors (FYH and THN) independently. Disagreements on inclusion and exclusion were resolved through discussion. Consensus was achieved for all included publications. The methodological qualities in the included studies were evaluated by the Cochrane’s risks of bias assessment29. The risks-of-bias assessment covers six domains in evaluating RCTs, including selection bias, performance bias, detection bias, attrition bias, reporting bias and other possible biases. Assessors assigned a judgment for each domain, which can be “yes” (low risk of bias), “no” (high risk of bias) or “unclear” (uncertain risk). An inter-rater reliability analysis using the Kappa statistic was performed on the quality assessment and the agreement was substantial (Cohen’s Kappa = 0.76, p < 0.001). Discrepancies were resolved by discussion with the third author (WFY).
Statistical Analyses
The program Review Manager (RevMan 5.2.4) was used for statistical analysis. Continuous outcome data were combined using either mean difference or standardized mean difference with 95% confidence intervals (CI); dichotomous outcome data were combined using risk ratio and odds ratio with 95% CI. Random effects model was used in view of the anticipated between-study variance29. Publication bias was evaluated by funnel plot if 10 or more studies were included29.
Results
Selection of Studies
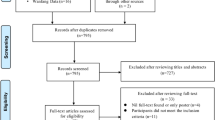
There were 3093 citations identified from the search, of which 907 were identical citations and 2123 were irrelevant papers. A total of 63 full texts were retrieved for further review, of which 53 articles were excluded due to the violation of inclusion criteria (Fig. 1). Of the remaining 10 RCTs included in this review, 6 examined stepped care prevention and 4 examined stepped care treatment. Since 2 included prevention studies were extensions of the other 2 already included prevention studies, the total number of included studies were greater than the actual number of trials described in the tables and figures. Details of the excluded studies are available from the authors.

Selection Flow of Trials for Inclusion in the Review.
Description of Included Studies
Stepped care prevention
The four stepped care prevention trials30,31,32,33,34,35 included a total of 731 participants (sample size ranged from 136 to 240) (Table 1). Participants were elderly from the Netherlands with depressive or anxiety symptoms and adults from Hong Kong with subthreshold depression and/or anxiety. Participants’ mean age was 78.2 years and 68.6% of the sample was female. Standardized self-rating scales, the Center for Epidemiologic Studies Depression Scale (CES-D) and the Hospital Anxiety and Depression Scale–Anxiety (HADS-A) were used in three and one of the included trials for screening respectively; however, a different cutoff score was adopted. The remaining trial was a relapse prevention, which only included participants who had undergone previous psychological or pharmacological treatment for depression (Study 1)30,31. The major inclusion and exclusion criteria are presented in Supplementary Table S1. All studies compared stepped care prevention with CAU. Participants had unrestricted access to any form of health care (e.g., psychological interventions and prescription medications) in CAU group. Treatment outcome was evaluated with self-report measures in all four studies and with structured diagnostic interviews in three studies.
Stepped care treatment
The four stepped care treatment trials included a total of 488 participants; the sample size ranged from 30 to 180 (Table 1)16,18,19,36. The average age of the participants was 43.9 years and 63.5% of the sample was female. Participants were adults aged ≥18 years from the Netherlands or United States with depressive and/or anxiety disorders. The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) was used in all trials for screening. All studies compared stepped care treatment with CAU. Participants had unrestricted access to any form of health care (e.g., no treatment, psychological interventions, prescription medications, referrals to psychiatric nurse, primary care psychologist, specialized mental health center or other professional) or standard exposure and response prevention (ERP)19 in CAU group. Treatment outcome was evaluated with self-rated or clinician-administered questionnaires.
Description of Stepped Care Content
Stepped care prevention
In the identified stepped care prevention studies, all of the prevention programs consisted of 4 steps, with watchful waiting as the first step, self-help psychotherapy as the second step, face-to-face psychotherapy as the third step and referral to specialists as the last step. Self-help psychological treatments were based on CBT from the book Coping with Depression37 in all except one trial (Study 4)35. Various treatment contents were adopted in face-to-face psychotherapy step, including CBT, life review therapy and problem-solving treatment (PST) (Table 2).
Stepped care treatment
In the identified stepped care treatment studies, the treatment program consisted of 2 to 4 steps. One study used 4 steps with the same treatment sequence as stated in stepped care prevention; one study used 3 steps with self-help psychotherapy as the first step, followed by face-to-face psychotherapy and pharmacotherapy; two studies used 2 steps with self-help and face-to-face psychotherapy. Self-help psychological treatments included PST, exposure therapy, ERP and CBT. Face-to-face psychological treatments were based on PST, CBT and ERP. Details of the stepped care treatment content are described in Table 2.
“Stepping Up” Criteria
Stepped care prevention
“Stepping up” refers to the progression from less restrictive treatments to more intensive treatments if no significant health benefits were achieved. All of the four prevention trials invited participants to progress to the next step if the symptom severity, as measured by CES-D and HADS-A, remained greater than a cutoff score (Table 2). Different cutoff scores were used across four studies: They were CES-D score ≥15, ≥16, less than a 5-point improvement or HADS-A ≥6, respectively. Direct referral to the last step was given to participants who had a diagnosis of depressive and/or anxiety disorders in three studies.
Stepped care treatment
The stepping-up criteria were diverse across the four included treatment studies (Table 2). One of the studies18 adopted stringent criteria, with a combination of three self-report assessments, including Inventory of Depressive Symptomatology (IDS) ≥14, Hospital Anxiety and Depression Scale (HADS) ≥8 and Work and Social Adjustment Scale (WSAS) ≥6. The other 3 studies used Beck Anxiety Inventory (BAI) >11 or less than 50% score reduction16, Clinical Global Impression-Severity Scale (CGI-S) ≥336, or the Yale–Brown Obsessive–Compulsive Scale (Y-BOCS) >1319. Serious cases were referred to the last step if the following criteria were fulfilled: WSAS ≥8 on 3 of the 4 daily functioning domains, depression with psychotic features or suicidal ideation, or Y-BOCS >13. One of the included studies did not report the direct referral requirement (Study 4)16.
Attrition Rate and Reasons for Attrition
Stepped care prevention
Attrition rate was reported in all included prevention studies; however, the assessment time points were different across studies (Table 2). Three of the four studies reported the attrition rates in both groups. The average cumulative attrition rates of stepped care prevention were 15.0% at posttreatment and the corresponding rate of CAU was only reported in 3 included studies, which was 8.9% at posttreatment. There was significant difference between stepped care prevention group and CAU group in attrition rate (risk ratio: 1.7, 95% CI: 1.2 to 2.4, p < 0.01 I2 = 40%, N = 3). Reasons for attrition were reported in all four studies. The most commonly cited reasons were physical illness and death, which might be due to the advanced age of the target population.
Stepped care treatment
Attrition rate was reported in three of the four included treatment studies (Table 2). Of the three treatment studies, two reported the attrition rates of both stepped care and CAU groups. The average cumulative attrition rates of stepped care treatment were 19.4% at posttreatment and the corresponding rates of CAU were 5.0%. No significant difference was found between stepped care treatment group and CAU group in attrition rate (risk ratio: 1.9, 95% CI: 0.9 to 4.3, p = 0.11, I2 = 0%, N = 2). The dropouts provided various attrition reasons including unwillingness to complete assessment, contact failure and physical illness.
Quality Assessment
Cochrane’s risks of bias assessment
There were some methodological flaws in all of the included studies (Supplementary Table S2). Due to the nature of the study, it made blinding of participants improbable and thus the risk of bias was assessed as “high” in all included studies. On the other hand, because the independent assessor was usually masked from the conditions, the risk of bias for blinding of assessor was generally assessed as “low.” The majority of studies did not report the allocation concealment method and thus the risk of bias were rated as “uncertain.” In addition, all included studies were free of bias in selective reporting and other possible biases.
Meta-analyses
Stepped care prevention vs. CAU
The incidence rate of anxiety and/or depressive disorders in stepped care prevention did not differ significantly from CAU (Fig. 2; OR = 0.75, 95% CI: 0.41, 1.38, p = 0.36, I2 = 45%, N = 3), indicating that the chances of developing anxiety and/or depressive disorders in stepped care group and CAU group were similar.

Stepped Care Treatment vs. CAU control on the Incidence of Anxiety and/or Depressive Disorders at Immediate Posttreatment.
Stepped care treatment vs. CAU
At immediate posttreatment, the pooled analysis of three RCTs found that stepped care treatment was significantly better than CAU in reducing anxiety symptoms (Fig. 3; standardized mean difference = −0.29, 95% CI: −0.48, −0.10, p < 0.01, I2 = 0%). The pooled treatment response rate of anxiety disorders in two RCTs was significantly higher in stepped care treatment than in CAU (Supplementary Fig. S2; OR = 2.38, 95% CI: 1.25, 4.52, p < 0.01, I2 = 0%). No significant difference was found between stepped care treatment and CAU in improving depressive symptoms.

Stepped Care Treatment vs. CAU control on Anxiety Symptoms at Immediate Posttreatment.
Cost-effectiveness
Among the included stepped care prevention studies, two reported data on cost-effectiveness (Study 2 and 3)38,39. Both studies evaluated stepped care prevention in the older population. In Study 2, the cost estimate was derived from Trimbos and Institute of Medical Technology Assessment Questionnaire (TIC-P) at each prevention step38. It demonstrated that there was no significant difference in total mean cost between stepped care prevention (€4,284) and CAU (€3,446) and the prevention was not considered cost-effective when comparing with CAU in elderly. Study 3 found that stepped care prevention halved the incidence rate of depression and anxiety at an incremental cost of €563 per recipient and an average of €4,367 for a depression/anxiety-free year39. The cost was estimated based on the healthcare uptake measured by the TIC-P and out-of-pocket expenses from patients at each prevention step. The study concluded that the stepped care prevention allowed depression/anxiety-free survival years in elderly at an affordable cost. Data on productivity cost was considered irrelevant in the older population. Hence, it was not included in the cost-effectiveness analysis in both studies. Cost-effectiveness was not examined in any of the treatment studies that were included.
Publication Bias
Funnel plots for the comparison of stepped care prevention or treatment and CAU were not possible due to the small number of included studies; hence, publication bias could not be determined.
Discussion
Stepped care model is an emerging delivery method in preventing and treating depression and anxiety disorders. The aim of this review study was to compare the efficacy and cost-effectiveness between stepped care and CAU groups. The comparison of stepped care treatment and CAU revealed significant difference in favor of the former in terms of anxiety symptoms and treatment response rate of anxiety disorders. Significant difference was not found between stepped care prevention/treatment and CAU in preventing anxiety and/or depressive disorders and reducing depressive symptoms. Cost-effectiveness analysis demonstrated inconsistent findings between stepped care prevention and CAU in two studies, with one considered effective at an affordable cost but not the other. Overall, there was evidence showing that stepped care treatment is effective in alleviating anxiety symptoms.
In our meta-analysis, sample sizes merged from multiple studies increased the chance of detecting the difference of treatment effect between the two groups, if any. On the other hand, stepped care prevention had significantly higher attrition rate than CAU, perhaps patients in the stepped care group lost their interest and patience to step up. The included studies had various treatment components at each step and a wide range of stepping-up criteria, which may have affected the treatment effect of the whole treatment model. Nonetheless, the heterogeneity test in the meta-analysis of stepped care treatment indicated no observed statistical heterogeneity (i.e., I2 = 0%); therefore, the detected treatment effect was likely to be genuine, given the high level of consistency across the studies40.
To date, there is no consensus on the structure of the stepped care model. Indeed, other than the fact that they all included self-help as a treatment component, the RCTs included in the current review have different combinations, sequences and number of steps in their rendition of the model. Although there might be merit to standardize the architecture of the model, we argue that flexibility is also needed to adequately respond to the differences in resource availability and logistical constraints across diverse settings. As such, stepped care model, we argue, should be evaluated as a whole and not independently at each step. Researchers are encouraged to focus their attention on constructing the most feasible model in response to the needs and available resources of the particular setting. Nevertheless, there remains a need to select evidence-based treatments as the basis of the model, such as, but not limited to, CBT41,42, PST43, behavioral activation44 and mindfulness and acceptance-based treatments45. Generally, the delivery modality of these evidence-based treatments comprises self-help therapy, guided group therapy, brief and long-term individual therapy. In terms of number of steps in the model, the prevention studies we included generally had four steps, whereas treatment studies adopted two to four steps. The optimal number of steps can vary under different circumstances. Two major factors—the intensity of treatment and the upper limit of therapist input in a routine healthcare setting—can help to determine how many steps should be included15.
Self-correcting is one of the key features on the health gain and patients’ progress15. It is underscored that whether or not a model is cost-effective may partly depend on the stepping-up criteria8. A well-defined stepping-up criterion should be sensitive enough to detect those who fail to respond to the first-line treatments, so that the model is able to maximize the proportion of patients who may benefit from the low-intensity first-line interventions. On the one hand, it should be able to rapidly identify and provide appropriate treatment to patients in need of more intensive care.
The heterogeneity of the stepping-up criteria among the included studies did not allow us to draw a conclusion on a best-fit assessment tool or cut-off score. Conventional questionnaires for screening depression and/or anxiety, such as CES-D46, BDI47, BAI48 and HADS49, can be considered as screening tools. The cut-off score can be decided based on previous validation studies with good sensitivity and specificity analyses. Nonetheless, there is room for cut-off score adjustment depending on the nature of trial. For example, relative to treatment studies, prevention studies tend to recruit high-risk populations who do not meet full criteria for a diagnosis. For this reason, prevention studies might have relatively more conservative cut-off scores whereas treatment studies might adopt more stringent cut-off scores. Alternatively, the option for clinician administrated structured diagnostic assessments is more desirable. Nonetheless, the additional therapist time and cost may undermine the core feature (i.e. least restrictive) of the stepped care model.
There were several limitations in our study. First, the number of studies included in the meta-analysis was small. Since stepped care for depression and anxiety is a relatively new area of research, only few trial studies have been completed. The exclusion of non-self-help treatment at the entry step also reduced the amount of studies. Nevertheless, since the step care model varied greatly across studies, the inclusion of stepped care studies regardless of their model design may hinder the comparison between studies. We encourage researchers to interpret the current findings with caution and extend and replicate the current findings in the future to provide further evaluations for stepped care.
Second, the variation of treatment effect among studies might be related to different model structures. The content, duration, sequence and delivery method of treatment might have an impact on the treatment outcome. In addition, the diversity of diagnostic criteria and age groups in the included studies may also contribute to the variation in the treatment outcome. Finally, most of the included studies were from healthcare systems in European or American contexts, with the majority of trials conducted in the Netherlands. It is unknown whether the stepped care model is applicable or generalizable to healthcare systems in emerging countries where resources for mental health might be scarce. To date, no studies examining the efficacy of stepped care for depressive and anxiety disorders have been conducted in emerging countries with very limited mental healthcare resources.
In response to the high demand yet simultaneously limited resources for mental health services, the stepped care model for common mental health disorders is of increasing relevance around the globe. The result in this review study sheds light on the efficacy and cost-effectiveness of stepped care model in preventing and treating depressive and/or anxiety disorders. The model has the potential to reduce the burden on existing resources in mental health and at the same time increase the reach and availability of service. The model might also be of particular interest in regions where stigma is preventing those in need of mental health services to seek help. The lower steps in the stepped care model may be less stigmatizing than full-blown psychotherapy or psychiatric care. We suggest further fine-tuning of the stepped care model with the utilization of technology to further enhance its efficacy and efficiency. A smartphone application, for example, might be a favourable platform to support patients in clinical settings50. It can even serve as a tool used in the first step (e.g., self-help). Emerging countries have become more aware of the importance of mental health service. Unfortunately, investment on resources continues to be lacking51. Stepped care model serves as an economically viable and effective treatment option.
Additional Information
How to cite this article: Ho, F. Y.-Y. et al. The Efficacy and Cost-Effectiveness of Stepped Care Prevention and Treatment for Depressive and/or Anxiety Disorders: A Systematic Review and Meta-Analysis. Sci. Rep. 6, 29281; doi: 10.1038/srep29281 (2016).
References
Greenberg, P. E. et al. The economic burden of anxiety disorders in the 1990s. J. Clin Psychiatry. 60, 427–435 (1999).
Simon, G. E. Social and economic burden of mood disorders. Biol. Psychiatry. 54, 208–215 (2003).
Ayers, C. R., Sorrell, J. T., Thorp, S. R. & Wetherell, J. L. Evidence-based psychological treatments for late-life anxiety. Psychol. Aging. 22, 8–17 (2007).
Hollon, S. D. & Ponniah, K. A review of empirically supported psychological therapies for mood disorders in adults. Depress Anxiety. 27, 891–932 (2010).
Kazdin, A. E. Evidence-based treatment and practice: new opportunities to bridge clinical research and practice, enhance the knowledge base and improve patient care. Am. Psychol. 63, 146–159 (2008).
Horton, R., Saxena, S., Thornicroft, G., Knapp, M. & Whiteford, H. Global mental health 2 Resources for mental health: scarcity, inequity and inefficiency. Commentary. Lancet. 370, 878–889 (2007).
Grant, A., Townend, M., Mulhern, R. & Short, N. in Cognitive behavioural therapy in mental health care. (Sage, 2010).
Richards, D. A. et al. Delivering stepped care: an analysis of implementation in routine practice. Implement Sci. 7 (2012).
Espie, C. A. Stepped care”: A health technology solution for delivering cognitive behavioral therapy as a first line insomnia treatment. Sleep. 32, 1549–1558 (2009).
Spek, V. et al. Internet-based cognitive behaviour therapy for symptoms of depression and anxiety: A meta-analysis. Psychol. Med. 37, 319–328 (2007).
Anderson, L. et al. Self-help books for depression: How can practitioners and patients make the right choice. Br. J. Gen. Pract. 55, 387–392 (2012).
Kunik, M. E. et al. COPD education and cognitive behavioral therapy group treatment for clinically significant symptoms of depression and anxiety in COPD patients: A randomized controlled trial. Psychol. Med. 38, 385–396 (2008).
Stikkelbroek, Y., Bodden, D. H., Dekovi, M. & van Baar, A. L. Effectiveness and cost effectiveness of cognitive behavioral therapy (CBT) in clinically depressed adolescents: individual CBT versus treatment as usual (TAU). BMC Psychiatry. 13, 314 (2013).
Baldessarini, R. J. Drug therapy of depression and anxiety disorders in Goodman and Gilman’s the Pharmacological Basis of Therapeutics (eds Brunton, L. L. et al.) 429–460 (McGraw-Hill, 2006).
Bower, P. & Gilbody, S. Stepped care in psychological therapies: Access, effectiveness and efficiency. Br. J. Psychiatry. 186, 11–17 (2005).
Muntingh, A. et al. Effectiveness of collaborative stepped care for anxiety disorders in primary care: A pragmatic cluster randomised controlled trial. Psychother Psychosom. 83, 37–44 (2014).
Mitchell, J. E. et al. Stepped care and cognitive–behavioural therapy for bulimia nervosa: Randomised trial. Br. J. Psychiatry. 198, 391–397 (2011).
Seekles, W., van Straten, A., Beekman, A., van Marwijk, H. & Cuijpers, P. Stepped care treatment for depression and anxiety in primary care. A randomized controlled trial. Trials. 12, 171 (2011).
Tolin, D. F., Diefenbach, G. J. & Gilliam, C. M. Stepped care versus standard cognitive–behavioral therapy for obsessive–compulsive disorder: A preliminary study of efficacy and costs. Depress Anxiety. 28, 314–323 (2011).
Zatzick, D. et al. A randomized stepped care intervention trial targeting posttraumatic stress disorder for surgically hospitalized injury survivors. Ann. Surg. 257, 390–399 (2013).
Tummers, M., Knoop, H. & Bleijenberg, G. Effectiveness of stepped care for chronic fatigue syndrome: A randomized noninferiority trial. J. Consult. Clin. Psychol. 78, 724–731 (2010).
Cabezas, C., Advani, M., Puente, D., Rodriguez-Blanco, T. & Martin, C. Effectiveness of a stepped primary care smoking cessation intervention: Cluster randomized clinical trial (ISTAPS study). Addiction. 106, 1696–1706 (2011).
Drummond, C. et al. Effectiveness and cost-effectiveness of a stepped care intervention for alcohol use disorders in primary care: Pilot study. Br. J. Psychiatry. 195, 448–456 (2009).
Crow, S. J., Agras, W. S., Fairburn, C. G., Mitchell, J. E. & Nyman, J. A. A cost effectiveness analysis of stepped care treatment for bulimia nervosa. Int J Eat Disord. 46, 302–307 (2013).
Jaehne, A. et al. The efficacy of stepped care models involving psychosocial treatment of alcohol use disorders and nicotine dependence: A systematic review of the literature. Curr Drug Abuse Rev. 5, 41–51 (2012).
van Straten, A., Hill, J., Richards, D. A. & Cuijpers, P. Stepped care treatment delivery for depression: A systematic review and meta-analysis. Psychol. Med. 45, 231–246 (2015).
van Boeijen, C. A. et al. Efficacy of self-help manuals for anxiety disorders in primary care: A systematic review. Fam. Pract. 22, 192–196 (2005).
Scogin, F. R., Hanson, A. & Welsh, D. Self-administered treatment in stepped-care models of depression treatment. J. Clin. Psychol. 59, 341–349 (2003).
Higgins, J. P. T. & Green, S. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. (The Cochrane Collaboration, 2011).
Apil, S. R., Hoencamp, E., Judith Haffmans, P. M. & Spinhoven, P. A stepped care relapse prevention program for depression in older people: A randomized controlled trial. Int J Geriatr Psychiatry. 27, 583–591 (2012).
Apil, S. R. A., Spinhoven, P., Haffmans, P. M. J. & Hoencamp, E. Two-year follow-up of a randomized controlled trial of stepped care cognitive behavioral therapy to prevent recurrence of depression in an older population. Int J Geriatr Psychiatry. 29, 317–325 (2014).
Dozeman, E. et al. Contradictory effects for prevention of depression and anxiety in residents in homes for the elderly: A pragmatic randomized controlled trial. Int Psychogeriatr. 24, 1242–1251 (2012).
van’t Veer-Tazelaar, P. J. et al. Stepped-care prevention of anxiety and depression in late life: A randomized controlled trial. Arch. Gen. Psychiatry. 66, 297–304 (2009).
van’t Veer-Tazelaar, P. J. et al. Prevention of late-life anxiety and depression has sustained effects over 24 months: A pragmatic randomized trial. Am. J. Geriatric. 19, 230–239 (2011).
Zhang, D. X. et al. Prevention of anxiety and depression in Chinese: A randomized clinical trial testing the effectiveness of a stepped care program in primary care. J Affect Disord. 169, 212–220 (2014).
Oosterbaan, D. B. et al. Collaborative stepped care v. care as usual for common mental disorders: 8-month, cluster randomised controlled trial. Br. J. Psychiatry. 203, 132–139 (2013).
Lewinsohn, P. M., Antonuccio, D. O., Breckenridge, J. S. & Teri, L. In The ‘Coping with Depression’ Course. (Castalia Publishing Companym 1984).
Bosmans, J. E. et al. Cost-effectiveness of a stepped care programme to prevent depression and anxiety in residents in homes for the older people: A randomised controlled trial. Int. J. Geriatr. Psychiatry. 29, 182–190 (2014).
van’t Veer-Tazelaar, P. et al. Cost-effectiveness of a stepped care intervention to prevent depression and anxiety in late life: Randomised trial. Br. J. Psychiatry. 196, 319-325 (2010).
Altman, D. G., Deeks, J. J., Higgins, J. P. T. & Thompson, S. G. Measuring inconsistency in meta-analyses. BMJ. 327, 557–560 (2003).
Cuijpers, P. et al. A meta-analysis of cognitive-behavioural therapy for adult depression, alone and in comparison with other treatments. Can. J. Psychiatry. 58, 376–385 (2013).
Hofmann, S. G. & Smits, J. A. Cognitive-behavioral therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials. J. Clin. Psychiatry. 69, 621–632 (2008).
Bell, A. C. & D’Zurilla, T. J. Problem-solving therapy for depression: A meta-analysis. Clin Psychol Rev. 29, 348–353 (2009).
Cuijpers, P., van Straten, A. & Warmerdam, L. Behavioral activation treatments of depression: A meta-analysis. Clin Psychol Rev. 27, 318–326 (2007).
Hofmann, S. G., Sawyer, A. T., Witt, A. A. & Oh, D. The effect of mindfulness-based therapy on anxiety and depression: A meta-analytic review. J. Consult. Clin. Psychol. 78, 169–183 (2010).
Radloff, L. S. The CES-D scale a self-report depression scale for research in the general population. Appl. Psychol. Meas. 1, 385–401 (1977).
Beck, A. T., Steer, R. A. & Carbin, M. G. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin Psychol Rev. 8, 77–100 (1988b).
Beck, A. T., Epstein, N., Brown, G. & Steer, R. A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 56, 893–897 (1988a).
Zigmond, A. S. & Snaith, R. P. The hospital anxiety and depression scale. Acta Psychiat. Scand. 67, 361–370 (1983).
Luxton, D. D., McCann, R. A., Bush, N. E., Mishkind, M. C. & Reger, G. M. Health for mental health: Integrating smartphone technology in behavioral healthcare. Prof Psychol Res Pr. 42, 505–512 (2011).
Saxena, S., Thornicroft, G., Knapp, M. & Whiteford, H. Global mental heath 2:Resources for mental health: Scarcity, inequity and inefficiency. The Lancet. 370, 878–889 (2007).
Acknowledgements
The authors wish to thank Nate Thoma for his helpful comments on an earlier draft of this article.
Author information
Authors and Affiliations
Contributions
F.Y.H. – Paper search, quality assessment, statistics and manuscript preparation. W.F.Y. – Quality assessment, statistics and manuscript preparation. T.H.N. – Paper search and manuscript preparation. C.S.C. – Coordination and manuscript preparation.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Ho, FY., Yeung, WF., Ng, TY. et al. The Efficacy and Cost-Effectiveness of Stepped Care Prevention and Treatment for Depressive and/or Anxiety Disorders: A Systematic Review and Meta-Analysis. Sci Rep 6, 29281 (2016). https://doi.org/10.1038/srep29281
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep29281
This article is cited by
-
Culturally sensitive stepped care for adolescent refugees: efficacy and cost–utility of a multicentric randomized controlled trial
European Child & Adolescent Psychiatry (2024)
-
A randomized controlled trial on using predictive algorithm to adapt level of psychological care for community college students: STAND triaging and adapting to level of care study protocol
Trials (2023)
-
Feasibility of a video-delivered mental health course for primary care patients: a single-group prospective cohort study
BMC Primary Care (2023)
-
Systematic review of structured care pathways in major depressive disorder and bipolar disorder
BMC Psychiatry (2023)
-
Technology-Assisted Stepped-Care to Promote Adherence in Adolescents with Asthma: A Pilot Study
Journal of Clinical Psychology in Medical Settings (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
