
Abstract
The objective was to examine changes in temporal trends in suicide mortality in 26 Western countries by retrospective trend analysis of the WHO mortality database on causes of deaths. From 1990 to 2010, there was a median reduction in suicide mortality of 22.7%, ranging from a 46% reduction in Estonia to a 26.2% increase in Romania. Suicide mortality decreased by ≥20% in 15 countries and the reduction tended to be greater in countries with higher mortality in 1990. In most of the central European countries mortality strongly declined. The median changes in the age groups were −25.3% (range −62.9% to 72.6%) in people aged 15–24 years, −36.9% (−60.5% to 32.4%) in 25–34 years, −3.6% (−57.1% to 92%) in 35–54 years, −12.2% (−37% to 65,7%) in 55–74 years and −16.1% (−54.5% to 166.7%) in ≥75 years. Suicide prevention programs in youths and in the elderly seem to be effective (at least in females for the elderly) and efforts should be pursued in this way. However, suicide mortality of the people aged 35–54 years has increased in half of the studied countries between 1990 and 2010. Public policies should further orientate their efforts toward this population.
Similar content being viewed by others


Introduction
The World Health Organization (WHO) published a report in 2014 stipulating that a person die every 40 seconds from suicide somewhere in the world1. In the year 2020, approximately 1.53 million people will die from suicide based on current trends and according to WHO estimates. Ten to 20 times more people will attempt suicide worldwide2. This represents on average one death every 20 seconds and one attempt every 1–2 seconds. Suicide prevention is therefore a major issue for public health policies3,4,5. Twenty-eight countries today are known to have national suicide prevention strategies, while World Suicide Prevention Day, organized by the International Association for Suicide Prevention, is observed worldwide on 10 September each year1. To be effective, these policies need to rely on exhaustive and accurate deaths rates, in order to target specific populations and assess their effectiveness as well as the impact of social context6.
To help countries monitoring their death rates and carrying effective public health programs, the WHO created an international mortality database, with all-causes mortality data from 1979 to 2010. The WHO mortality database is a compilation of mortality data by age, sex and cause of death, freely available at http://apps.who.int/healthinfo/statistics/mortality/whodpms/. The data is collected and submitted within 18 months following the census. The data is then checked and treated for an average of two years before publication on the website. This data is prospectively recorded for every country, thus virtually covering the entire population. Published data was only taken from medical certificates.
In this study we analyzed suicide mortality in 25 European countries and United States of America (USA) from 1990 to 2010 and examined temporal trends in suicide rates for both sexes, males and females and for subjects aged [15–24], [25–34], [35–54], [55–74] and 75+ to help decipher the effect of the contributing factors.
Methods
Suicide deaths registered in the World Health Organization mortality database at June 2015 were extracted for European countries and USA7. The quality of mortality data has been evaluated by the WHO8. Data quality is checked annually according to the Health Facility Data Quality Report Card (DQRC). The DQRC examines completeness of reporting; internal consistency of reported data; external consistency of population data and external consistency of coverage rates (for more details see http://www.who.int/healthinfo/DQRC_Indicators.pdf). A return to the data collectors on the quality of their entered data is sent each year. Albania, Luxembourg, Monaco, Iceland and Malta were excluded for missing data. For Slovakia data was only available since 1992, for Denmark since 1994, for Switzerland since 1995, for Serbia since 1998, for Cyprus since 1999. There were not included in our analyses. For almost all other countries, data up to 2010 were available.
We used Group-based trajectory modeling9,10 to identify distinctive group of trajectories based on the assumption that the population is composed of mixture of distinct groups defined by their developmental trajectories, while recognizing uncertainty in group membership. Using SAS proc traj9,10, we model pattern of change over time in the suicide mortality rate of 26 countries (dependent variable) between 1990 and 2010. Comparisons were made between models allowing for varying numbers of trajectory groups, as well as models including time as linear, quadratic and cubic, using the Bayesian (BIC) information criteria. More precisely, we use the BIC log Bayes factor approximation 2 log(Bij) ≈ 2*(BICi − BICj) – the BIC of the more complex (large number of group, or higher order equation) less the BIC of the null (simpler) model – to select the model that better fits the data. According to Roeder and Nagin9 classification, a value between 0 and 2 refers to “Not worth mentioning” evidence against simple model, between 2 and 6 refers to “positive evidence against the simple model”, between 6 and 10 refers to “strong evidence against the simple model” and higher than 10 refers to “very strong evidence against the simple model”.
Mortality values were adjusted by the age distribution of the European standard population to obtain European Adjusted Standardized Death Rates (ASDRs). After logarithmic transformation of rates, we fitted a linear regression from 1990 until 2010. We performed these analyses for both sexes and respectively for females and males and for subjects aged [15–24], [25–34], [35–54], [55–74] and 75+.
Results
Overall changes in suicide mortality
Figure 1A–C and Table 1 show the changes in suicide mortality in 25 European countries and USA from 1990 to 2010. Over the 20 years, suicide mortality declined by a median of 22.7%, with individual values ranging from a 46% reduction in Estonia to a 26.2% increase in Romania. The decrease was >20% in 15 countries and in 4 countries suicide mortality continued to increase.
When the 20-year mortality changes were plotted against the mean suicide mortality in 1990 (Fig. 2), countries with high suicide mortality in 1990 tended to have greater reductions in mortality. However, the decrease varied substantially. Latvia, Slovenia, Estonia and Lithuania had similar suicide mortality rates in 1990. Lithuania has a 13.6% decrease while the three other countries had a 30–45% decrease. Only a slight reduction of suicide mortality was observed in USA, Belgium, Netherlands and Portugal between 1990 and 2010 (between −2.5% and −4.8%). During this period, suicide mortality increased in 4 countries, Romania (+26.2%), Lithuania (+13.6%), Poland (+7.9%) and Ireland (+4%). There was substantial reductions >20% in Estonia, Hungary, Finland, Austria, Slovenia, Croatia, Bulgaria, Germany, Czech Republic, Latvia, Sweden, Norway, Armenia, France and Italy.
With time, suicide mortality values for different countries seemed to converge. In 1990 mortality (per 100 000) ranged from 2.9 in Greece to 33.5 in Hungary (difference 31.4), whereas in 2010 mortality ranged from 2.3 in Armenia to 27.6 in Lithuania (difference 25.3). Time series were examined in Fig. 3. Five groups were identified in regard of ASDRs evolution between 1990 and 2010. The two first groups (including Armenia and Greece, Italy, Spain, United Kingdom, Netherlands and Portugal) had relatively stable suicide rates, below 10 per 100,000 habitants. The third group (including Austria, Bulgaria, Croatia, Czech Republic, Germany, France, Norway, Sweden, Belgium, Ireland, Poland, Romania and USA) had ASDRs between 10 and 15 per 100,000 habitants, with a mean slight decrease between 1990 and 2010. The two last groups (including Estonia, Finland, Hungary, Latvia, Slovenia and Lithuania) had high rates of ASDRs in 1990 (around 30 per 100,000 or more) with a strong decrease between 1990 and 2010. Except for Lithuania, the other countries ASDRs have almost joined the suicide rates of those of group 3 in 2010.
Changes in suicide mortality by gender
Reductions in mortality were most marked in males (median change −37% (range −76% to −14%)) and reductions of 15% or more of suicide mortality in males were observed in 22 countries on 26. Reductions in female suicide mortality were more moderate (median range −20% (range −46.1% to +43%)). Increase of suicide mortality in females was observed in all countries where global suicide mortality increased (Romania (+43%), Lithuania (14.8%), Poland (+13.8%), Ireland (+12%)) and in the Netherlands (+3.6%)). In the USA, suicide mortality increased in males (+2.2%) while it decreased in females (−7.8%).
Changes in suicide mortality by age group
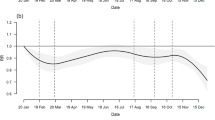
Reductions in mortality were most marked in people aged 25–34 years (median change −36.7% (range −60.5% to 32.4%). Reductions in 15–24 years were similar to all-ages (median change −25.3% (range −62.9 to 72.6%)). The median change of people aged 75+ was −16.1% (−54.5% to 166.7%) with suicide mortality continuing to increase in 8 countries. The slightest reduction in suicide mortality was found in the 35–54 years old, with a median of −3.6% (57.1% to 92%) and an increase in the half of countries (13/26 countries). In the USA, suicide mortality increased in the 35–54 years (+62.9%) (Fig. 4) and in the 55–74 years (+41.5%), while it decreased in the other age categories. More specifically, the suicide mortality in the 35–54 years old males increased regularly in the USA between 1990 and 2010 (Fig. 3).
Discussion
This study shows substantial differences between European countries in temporal trends of suicide mortality, as well as differences in mortality changes with age. USA were classified 21/26 in regard of the decrease of suicide mortality between 1990 and 2010 with a decrease of 3.5%, while the median for European countries was −23.3% (range from −46% to 26.2%). Altogether, the 35–54 years old people benefited the less from suicide mortality decrease between 1990 and 2010. The sustained decline observed in many countries after 1994 seems to indicate that suicide mortality will continue to decrease beyond 2010.
Interpretation of results
Overall, the suicide mortality has decreased between 1990 and 2010 in USA and Western European countries. Many suicide prevention programs were developed during this period11,12,13,14,15,16,17,18,19. Suicide mortality also strongly decreased between 1990 and 2010 in most of the Eastern European countries. These epidemiological patterns may be linked to rapid changes in suicide attempts and medical care that took place in these countries after the collapse of the communist regimes in the 1990 s20,21. This phenomenon may also at least in part explain the strong decrease of suicide mortality in Germany (−35.8%) that followed the German reunification of 1989.
Our analyses showed that mortality levels in 1990 could have influenced some of the relative differences in mortality reductions, but they cannot account for a large part of variations between countries (Fig. 2). Among medical factors influencing suicide rates, education of physicians was found as one of the most effective in suicide prevention22. Psychiatric disorders are present in at least 90% of suicides and more than 80% are untreated at time of death23. Depression is untreated or undertreated in general, even after suicide attempt24,25. Thus, treating mood and other psychiatric disorders may be suggested as a central component of suicide prevention26,27. The newer antidepressants, selective serotonin reuptake inhibitors (SSRIs) and new generation non-SSRIs introduced in the late 80 s were found to have fewer discontinuation rate28 and were associated with lower lethality in cases of intentional overdose29. Higher prescription rates of antidepressants correlate with decreasing suicide rates in adults or youth30,31,32. However the association between the administration of antidepressants and suicide risk remains debated to date33. The risk of an ecological fallacy, that is, inferring causality from group correlations, prevents attributing decreases in suicide rates solely to antidepressant use. However suicide is not only associated with depression, as all mental disorders have an increased risk of suicide excepting mental retardation and dementia26. Lithium showed efficacy in suicide prevention for bipolar disorders34 and clozapine for suicide prevention in schizophrenia35.
Beyond pharmacological treatments, training physicians includes also the evaluation of the risk, the emergency and the dangerousness of the suicidal episode. Restricting access to lethal means was found as a powerful tool to prevent suicide22. Promising results in reducing repetition of suicidal behavior and improving treatment adherence exist for cognitive therapy36,37,38 problem-solving therapy39, intensive care plus outreach39 and interpersonal psychotherapy40, acceptance and commitment therapy41,42 compared with standard aftercare.
Our results suggested that suicide rates were strongly influenced by age. Suicide is the second leading cause of death among persons aged 10–24 years in Western countries43. Many countries developed therefore programs targeting suicide in adolescents and young adults12,19,44,45,46,47,48,49,50,51,52,53,54. Several countries have developed school-based suicide prevention programs13,14,55,56,57. As suicide attempts were found to be higher in youths homo- and bisexuals and a specific program was also developed to prevent homophobic bullying in this population in France58. New connected technologies have been suggested to improve suicide prevention in this population and need to be further evaluated59,60,61,62. The elderly was also described as at risk for suicide63. Most elderly suicide prevention programs were centered on the reduction of risk factors (depression screening and treatment and decreasing isolation), but when gender was considered, programs were mostly efficient for women18. Overall, our results suggest that suicide prevention policies were more effective in adolescents/young adults than in the elderly. Only three countries had increased rate of suicide deaths in youths versus nine in the elderly. It may be underlined that four countries with the highest rates of suicide increase in the elderly had low quality data (Armenia +166.7%, Poland +60.6%, Portugal +81%, Greece +10.9%).
One of the major findings of the present work was that suicide mortality in males aged 35–54 years increased, or at least stagnated between 1990 and 2010 (Fig. 3). Several explanations were recently suggested in the literature to explain this phenomenon. Unemployment rate was recently found to be associated with increased suicide mortality between 2000 and 2010, in several European countries64. The impact of unemployment on suicide rates was suggested to be higher in males compared to females61,64,65,66. It may therefore be suggested that further suicide prevention policies focus on unemployed people. It was also suggested that the recent worldwide financial and economical 2008 crisis may have been associated with increased completed suicides in Western European countries61,67,68,69,70,71. However, the results for the USA suggested that the suicide mortality regularly increased between 1990 and 2010 and no significant suicide mortality increase was noted in European countries. The 2008 crisis can therefore not be argued as the unique factor implicated in suicide mortality increase in this population. The suicide mortality in middle-aged males may also be due to suicide in jail. However the studies on the jail suicide prevalence remain few in number and the studies on suicide prevention in jail are even more rare. A study assessing suicide rate in the prisons of 12 countries concluded that rates of prison suicide did not reflect general population suicide rates72. This suggested that variations in prison suicide rates reflected differences in criminal justice systems including, possibly, the provision of psychiatric care in prison. A national study in the USA concluded that there has been a significant decrease in the rate of suicide in detention facilities during this period17. To deal with this public health issue, a peer-prevention program in prisons was recently developed in France73. Low socioeconomic status, unhealthy lifestyle habits, difficulties in health care access and poor longitudinal continuity of care were also suggested as potent etiological factors of suicide mortality that could also be targeted by suicide prevention policies74,75. Finally, another explanation for the increase of suicide mortality in the 35–54 years may be due to the improvement of medical care system. Although most of the suicide deaths were associated with the first attempt76, it may be hypothesized that a better management of suicide attempts in youth may be associated with an increase of the mean age at death by suicide. Further studies should assess the impact of suicide interventions on suicide trajectories, beyond the absolute number of deaths by suicide.
When examining the suicide trajectories, we found that Armenia and Greece (group 1) reported lower stable rates of suicide compared to other countries. As quality data was evaluated as “low” for these countries, it may be hypothesized that suicide may be under-reported in these countries. In group 2, which includes countries with stable suicide rates below 10 per 100,000 habitants, only United Kingdom reported high quality data. Most of the other countries were included in group 3, with stable suicide rates between 10 and 15 per 100,000 between 1990 and 2010. Group 4 and 5 included countries with high suicide rates in 1990, with strong decrease between 1990 and 2010. Except for Finland, all these countries were Easter European countries. As suicide rates regularly decreased since 1994, it may be suggested that the collapse of Soviet Union was associated with a decrease of suicide rates in Easter European countries21. A high suicide rate (99.8%) in forensic autopsy registers in Finland had been already described77. Economic hardship was described as strongly associated with suicide mortality in Finland78. It was also recently suggested that Finland ASDRs may be explained by gender differences: In Finland, jumping in front of moving objects and firearms were frequently used by male adolescents79. The suicide mortality of Finnish women is currently the second highest in Europe80. Antidepressant consumption was not associated with increased suicide attempts in a large Finish 1966 birth cohort81. Some seasonal/weather parameters were also suggested to impact suicide death rates in Finland82,83,84 and East European countries85.
Strengths and limitations of study
The cause of death reported in national statistics may be of limited reliability and WHO quality indices displayed in the table indicate that, for all causes of death combined, data from Armenia, Greece, Poland and Portugal should be considered with caution. Suicide may often be misclassified as an accident or another cause of death. Registering a suicide is a complicated procedure involving several different authorities, often including law enforcement. Suicide mortality may have been underestimated in these countries. However trained clinicians wrote the death certificates, which may have limited the number of incorrect or incomplete certificates. These data remains mainly descriptive allowing to formulate hypotheses, but without causal certainty. In summary, we are confident that our results do reflect real trends. However, despite this data, it is still difficult to assess the efficacy of suicide programs.
Conclusion
The evaluation of the effectiveness of suicide prevention policies remains an important goal and challenge for the authorities. Overall, suicide mortality decreased between 1990 and 2010 in Europa and in the USA and the gender difference was less marked in 2010 compared to 1990. The evolution of suicide in Europa and USA suggested that suicide prevention policies were effective in youths, but less in the elderly. In contrast, suicide mortality increased in the 35–54 years old in half of the studied countries. Key elements in developing a national suicide prevention strategy are to make prevention a multisectoral priority that involves the health sector but also education, employment, social welfare, the judiciary and others. Communities play a critical role in suicide prevention. They can provide social support to vulnerable individuals and engage in follow-up care, fight stigma and support those bereaved by suicide. Health-care services need to incorporate suicide prevention as a core component. Early identification and effective management are keys to ensuring that people receive the care they need. Suicide prevention interventions should be multimodal, evidence based, guided by specific testable hypotheses and implemented among populations of sufficient size to yield generalizable and reliable results. It would be necessary to develop international assessment programs and the present work can help to get this direction.
Additional Information
How to cite this article: Fond, G. et al. Disparities in suicide mortality trends between United States of America and 25 European countries: retrospective analysis of WHO mortality database. Sci. Rep. 6, 20256; doi: 10.1038/srep20256 (2016).
References
World Health Organization (WHO). Preventing suicide: A global imperative. WHO (2014). at http://www.who.int/mental_health/suicide-prevention/world_report_2014/en/. Accessed 04/12/2015.
World Health Organization (WHO). Figures and facts about suicide. (1999). http://apps.who.int/iris/bitstream/10665/66097/1/WHO_MNH_MBD_99.1.pdf. Accessed 04/12/2015.
Patel, V., Flisher, A. J., Hetrick, S. & McGorry, P. Mental health of young people: a global public-health challenge. The Lancet 369, 1302–1313 (2007).
Fond, G., Gaman, A., Brunel, L., Haffen, E. & Llorca, P.-M. Google Trends(®): Ready for real-time suicide prevention or just a Zeta-Jones effect? An exploratory study. Psychiatry Res. 10.1016/j.psychres.2015.04.022 (2015).
Fond, G., Brunel, L., Leboyer, M. & Boyer, L. Do the treasures of ‘big data’ combined with behavioural intervention therapies contain the key to the mystery of large psychiatric issues? Acta Psychiatr. Scand. 130, 406–407 (2014).
Iacobucci, G. WHO report says countries should do more to prevent suicides. BMJ 349, g5461 (2014).
World Health Organization. Mortality database. (2015). http://www.who.int/healthinfo/mortality_data/en/. Accessed 09/10/2015.
Mathers C. D., Ma Fat D., Inoue M., Rao C. & Lopez A. Counting the dead and what they died from: an assessment of the global status of cause of death data. Bull World Health Org 83, 171–7 (2005).
Jones, B. L., Nagin, D. S. & Roeder, K. A. SAS procedure based on mixture models for estimating developmental trajectories. Sociol. Methods Res. 29, 374–393 (2001).
Nagin, D. S. & Tremblay, R. E. Analyzing developmental trajectories of distinct but related behaviors: a group-based method. Psychol. Methods 6, 18 (2001).
Haring, C. & Sonneck, G. [Suicide Prevention Austria (SUPRA) : the implementation of a national suicide prevention program]. Neuropsychiatr. Klin. Diagn. Ther. Rehabil. Organ Ges. Österr. Nervenärzte Psychiater 26, 91–94 (2012).
Klimes-Dougan, B., Klingbeil, D. A. & Meller, S. J. The impact of universal suicide-prevention programs on the help-seeking attitudes and behaviors of youths. Crisis 34, 82–97 (2013).
Valente, S. M. & Saunders, J. M. High school suicide prevention programs. Pediatr. Nurs. 13, 108–112 137–139 (1987).
Schilling, E. A., Lawless, M., Buchanan, L. & Aseltine, R. H. ‘Signs of Suicide’ shows promise as a middle school suicide prevention program. Suicide Life. Threat. Behav. 44, 653–667 (2014).
King, K. A. Developing a comprehensive school suicide prevention program. J. Sch. Health 71, 132–137 (2001).
King, K. A. & Smith, J. Project SOAR: a training program to increase school counselors’ knowledge and confidence regarding suicide prevention and intervention. J. Sch. Health 70, 402–407 (2000).
Hayes, L. M. National study of jail suicide: 20 years later. J. Correct. Health Care Off. J. Natl. Comm. Correct. Health Care 18, 233–245 (2012).
Lapierre, S. et al. A systematic review of elderly suicide prevention programs. Crisis 32, 88–98 (2011).
White, J. & Morris, J. Precarious spaces: risk, responsibility and uncertainty in school-based suicide prevention programs. Soc. Sci. Med. 1982 71, 2187–2194 (2010).
Värnik, P. et al. Massive increase in injury deaths of undetermined intent in ex-USSR Baltic and Slavic countries: hidden suicides? Scand. J. Public Health 38, 395–403 (2010).
Kõlves, K., Milner, A. & Värnik, P. Suicide rates and socioeconomic factors in Eastern European countries after the collapse of the Soviet Union: trends between 1990 and 2008. Sociol. Health Illn. 35, 956–970 (2013).
Mann J., Apter A., Bertolote J. & et al. Suicide prevention strategies: A systematic review. JAMA 294, 2064–2074 (2005).
Henriksson, S., Boëthius, G. & Isacsson, G. Suicides are seldom prescribed antidepressants: findings from a prospective prescription database in Jämtland county, Sweden, 1985–95. Acta Psychiatr. Scand. 103, 301–306 (2001).
Suominen, K. H., Isomets, E. T., Henriksson, M. M. & Ostamo, A. I. & others. Inadequate treatment for major depression both before and after attempted suicide. (2014).
Oquendo, M. A. et al. Adequacy of antidepressant treatment after discharge and the occurrence of suicidal acts in major depression: a prospective study. (2014).
Harris, E. C. & Barraclough, B. Suicide as an outcome for mental disorders. A meta-analysis. Br. J. Psychiatry 170, 205–228 (1997).
Bostwick, J. M. & Pankratz, V. S. Affective Disorders and Suicide Risk: A Reexamination. Am. J. Psychiatry 157, 1925–1932 (2000).
Anderson, I. M. & Tomenson, B. M. Treatment discontinuation with selective serotonin reuptake inhibitors compared with tricyclic antidepressants: a meta-analysis. BMJ 310, 1433–1438 (1995).
Henry, J. A., Alexander, C. A. & Sener, E. K. Relative mortality from overdose of antidepressants. BMJ 310, 221–224 (1995).
Olfson M., Shaffer D., Marcus S. C. & Greenberg T. Relationship between antidepressant medication treatment and suicide in adolescents. Arch. Gen. Psychiatry 60, 978–982 (2003).
Gibbons, R. D., Hur, K., Bhaumik, D. K. & Mann, J. J. The relationship between antidepressant prescription rates and rate of early adolescent suicide. (2006).
Carlsten, A., Waern, M., Ekedahl, A. & Ranstam, J. Antidepressant medication and suicide in Sweden. Pharmacoepidemiol. Drug Saf. 10, 525–530 (2001).
Fergusson, D. et al. Association between suicide attempts and selective serotonin reuptake inhibitors: systematic review of randomised controlled trials. BMJ 330, 396 (2005).
Cipriani, A., Hawton, K., Stockton, S. & Geddes, J. R. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis. BMJ 346, f3646 (2013).
Hennen, J. & Baldessarini, R. J. Suicidal risk during treatment with clozapine: a meta-analysis. Schizophr. Res. 73, 139–145 (2005).
Schneider, B. Behavioural therapy of suicidality. Eur. Arch. Psychiatry Clin. Neurosci. 262 Suppl 2, S123–128 (2012).
Tarrier, N., Taylor, K. & Gooding, P. Cognitive-behavioral interventions to reduce suicide behavior a systematic review and meta-analysis. Behav. Modif. 32, 77–108 (2008).
Stanley, B. et al. Cognitive-behavioral therapy for suicide prevention (CBT-SP): treatment model, feasibility and acceptability. J. Am. Acad. Child Adolesc. Psychiatry 48, 1005–1013 (2009).
Hawton, K. K. et al. Psychosocial and pharmacological treatments for deliberate self harm. Cochrane Libr. (1999).
Guthrie, E. et al. Randomised controlled trial of brief psychological intervention after deliberate self poisoningCommentary: Another kind of talk that works? Bmj 323, 135 (2001).
Ducasse, D. et al. Acceptance and commitment therapy for management of suicidal patients: a pilot study. Psychother. Psychosom. 83, 374–376 (2014).
Walser, R. D. et al. Effectiveness of Acceptance and Commitment Therapy in treating depression and suicidal ideation in Veterans. Behav. Res. Ther. 74, 25–31 (2015).
Patton, G. C. et al. Global patterns of mortality in young people: a systematic analysis of population health data. The Lancet 374, 881–892 (2009).
Goldston, D. B. et al. Cultural considerations in adolescent suicide prevention and psychosocial treatment. Am. Psychol. 63, 14–31 (2008).
Johnson, L. A. & Parsons, M. E. Adolescent suicide prevention in a school setting: use of a gatekeeper program. NASN Sch. Nurse Print 27, 312–317 (2012).
Kostenuik, M. & Ratnapalan, M. Approach to adolescent suicide prevention. Can. Fam. Physician Médecin Fam. Can. 56, 755–760 (2010).
Peña, J. B. & Caine, E. D. Screening as an approach for adolescent suicide prevention. Suicide Life. Threat. Behav. 36, 614–637 (2006).
Sher, L. Teaching medical professionals and trainees about adolescent suicide prevention: five key problems. Int. J. Adolesc. Med. Health 24, 121–123 (2012).
Bean, G. & Baber, K. M. Connect: an effective community-based youth suicide prevention program. Suicide Life. Threat. Behav. 41, 87–97 (2011).
Clifford, A. C., Doran, C. M. & Tsey, K. A systematic review of suicide prevention interventions targeting indigenous peoples in Australia, United States, Canada and New Zealand. BMC Public Health 13, 463 (2013).
Donald, M., Dower, J. & Bush, R. Evaluation of a suicide prevention training program for mental health services staff. Community Ment. Health J. 49, 86–94 (2013).
Haring, C. & Sonneck, G. [Suicide Prevention Austria (SUPRA) : the implementation of a national suicide prevention program]. Neuropsychiatr. Klin. Diagn. Ther. Rehabil. Organ Ges. Österr. Nervenärzte Psychiater 26, 91–94 (2012).
Lehman, S. & Miller, J. A. Interest and need greatly outpace resources for youth suicide prevention. N. C. Med. J. 71, 540 (2010).
Maniam, T. et al. Suicide prevention program for at-risk groups: pointers from an epidemiological study. Prev. Med. 57 Suppl, S45–46 (2013).
Wasserman, D. et al. School-based suicide prevention programmes: the SEYLE cluster-randomised, controlled trial. Lancet 385, 1536–1544 (2015).
King, K. A., Vidourek, R. A. & Strader, J. L. University students’ perceived self-efficacy in identifying suicidal warning signs and helping suicidal friends find campus intervention resources. Suicide Life. Threat. Behav. 38, 608–617 (2008).
Bridge, S., Hanssens, L. & Santhanam, R. Dealing with suicidal thoughts in schools: information and education directed at secondary schools. Australas. Psychiatry Bull. R. Aust. N. Z. Coll. Psychiatr. 15 Suppl 1, S58–62 (2007).
Pugniere, J.-M. Suicide des jeunes et homophobie en France : présentation d’une enquête et d’actions de prévention. Serv. Soc. 59, 17 (2013).
Berrouiguet, S., Gravey, M., Le Galudec, M., Alavi, Z. & Walter, M. Post-acute crisis text messaging outreach for suicide prevention: a pilot study. Psychiatry Res. 217, 154–157 (2014).
Ghoncheh, R., Kerkhof, A. J. F. M. & Koot, H. M. Effectiveness of adolescent suicide prevention e-learning modules that aim to improve knowledge and self-confidence of gatekeepers: study protocol for a randomized controlled trial. Trials 15, 52 (2014).
Fond, G. et al. Prevalence and Smoking Behavior Characteristics of Nonselected Smokers With Childhood and/or Adult Self-Reported ADHD Symptoms in a Smoking-Cessation Program: A Cross-Sectional Study. J. Atten. Disord. 10.1177/1087054713497396 (2013).
Christensen, H., Batterham, P. J. & O’Dea, B. E-Health Interventions for Suicide Prevention. Int. J. Environ. Res. Public. Health 11, 8193–8212 (2014).
Ruault, G. & Doutreligne, S. Dépression et prévention du suicide chez la personne âgée: enjeu de santé publique, en établissement comme à domicile, au sein du programme MobiQual. Rev. Gériatrie 38, 731–738 (2013).
Laanani, M., Ghosn, W., Jougla, E. & Rey, G. Impact of unemployment variations on suicide mortality in Western European countries (2000-2010). J. Epidemiol. Community Health 69, 103–109 (2015).
Cibis, A. et al. Preference of lethal methods is not the only cause for higher suicide rates in males. J. Affect. Disord. 136, 9–16 (2012).
Schrijvers, D. L., Bollen, J. & Sabbe, B. G. The gender paradox in suicidal behavior and its impact on the suicidal process. J. Affect. Disord. 138, 19–26 (2012).
Kontaxakis, V. et al. Suicide in Greece: 2001–2011. Psychiatr. Psychiatr. 24, 170–174 (2013).
Antonakakis, N. & Collins, A. The impact of fiscal austerity on suicide: on the empirics of a modern Greek tragedy. Soc. Sci. Med. 1982 112, 39–50 (2014).
Mattei, G., Ferrari, S., Pingani, L. & Rigatelli, M. Short-term effects of the 2008 Great Recession on the health of the Italian population: an ecological study. Soc. Psychiatry Psychiatr. Epidemiol. 49, 851–858 (2014).
Pompili, M. et al. Suicide in Italy during a time of economic recession: some recent data related to age and gender based on a nationwide register study. Health Soc. Care Community 22, 361–367 (2014).
Stavrianakos, K. et al. [Attempted suicide during the financial crisis in Athens]. Psychiatr. Psychiatr. 25, 104–110 (2014).
Fazel, S., Grann, M., Kling, B. & Hawton, K. Prison suicide in 12 countries: an ecological study of 861 suicides during 2003–2007. Soc. Psychiatry Psychiatr. Epidemiol. 46, 191–195 (2011).
Auzoult, L. & Abdellaoui, S. Perceptions of a peer suicide prevention program by inmates and professionals working in prisons. Crisis 34, 289–292 (2013).
Hoertel, N., Limosin, F. & Leleu, H. Poor longitudinal continuity of care is associated with an increased mortality rate among patients with mental disorders: results from the French National Health Insurance Reimbursement Database. Eur. Psychiatry J. Assoc. Eur. Psychiatr. 29, 358–364 (2014).
Laursen, T. M., Munk-Olsen, T., Nordentoft, M. & Mortensen, P. B. Increased mortality among patients admitted with major psychiatric disorders: a register-based study comparing mortality in unipolar depressive disorder, bipolar affective disorder, schizoaffective disorder and schizophrenia. J. Clin. Psychiatry 68, 899–907 (2007).
Colpe, L. J. & Pringle, B. A. Data for building a national suicide prevention strategy: what we have and what we need. Am. J. Prev. Med. 47, S130–136 (2014).
Ylijoki-Sørensen, S. et al. Autopsy rate in suicide is low among elderly in Denmark compared with Finland. Forensic Sci. Int. 244, 158–165 (2014).
Korhonen, M., Puhakka, M. & Viren, M. Economic hardship and suicide mortality in Finland, 1875–2010. Eur. J. Health Econ. HEPAC Health Econ. Prev. Care (2014). 10.1007/s10198-014-0658-5
Park, S. Brief report: Sex differences in suicide rates and suicide methods among adolescents in South Korea, Japan, Finland and the US. J. Adolesc. 40, 74–77 (2015).
Holopainen, J., Helama, S. & Partonen, T. [Finnish suicide mortality from 1950 to 2009 in an European comparison]. Duodecim Lääketieteellinen Aikakauskirja 130, 1536–1544 (2014).
Rissanen, I. et al. Use of antidepressant medication and suicidal ideation-the Northern Finland Birth Cohort 1966. Hum. Psychopharmacol. 29, 559–567 (2014).
Holopainen, J., Helama, S. & Partonen, T. Does diurnal temperature range influence seasonal suicide mortality? Assessment of daily data of the Helsinki metropolitan area from 1973 to 2010. Int. J. Biometeorol. 58, 1039–1045 (2014).
Holopainen, J., Helama, S., Björkenstam, C. & Partonen, T. Variation and seasonal patterns of suicide mortality in Finland and Sweden since the 1750 s. Environ. Health Prev. Med. 18, 494–501 (2013).
Hiltunen, L., Haukka, J., Ruuhela, R., Suominen, K. & Partonen, T. Local daily temperatures, thermal seasons and suicide rates in Finland from 1974 to 2010. Environ. Health Prev. Med. 19, 286–294 (2014).
Stoupel, E. G. et al. Space weather and human deaths distribution: 25 years’ observation (Lithuania, 1989–2013). J. Basic Clin. Physiol. Pharmacol. 26, 433–441 (2015).
Acknowledgements
We thank Dr Laurent ARNAUD, hôpital La Pitié-Salpêtrière, Paris, France. This work was supported by AP-HP (Assistance Publique des Hôpitaux de Paris), Fondation FondaMental (RTRS Santé Mentale) http://www.fondation-fondamental.org/, by programme Investissements d’Avenir under the references ANR-11-IDEX-0004-02 et ANR-10-COHO-10-01 and by INSERM (Institut National de la Santé et de la Recherche Médicale).
Author information
Authors and Affiliations
Contributions
G.F. and L.B. wrote the main manuscript text, tables and Figures 1,2,4. M.B carried out trajectory analyses and prepared the Figure 3. G.F., L.B., L.B., X.Z., P.M.L., C.L. and P.A. reviewed and approved the final manuscript.

(A) Decrease in age-standardized death rates by suicide >35% between 1990 and 2010. (B). Decrease in age-standardized death rates by suicide between 15 and 35% between 1990 and 2010 (C). Decrease in age-standardized death rates by suicide <15% between 1990 and 2010.

Percentage changes in suicide mortality in European countries and USA during 1990–2010 according to the mean suicide mortality in 1990.

Evolution of suicide mortality in the 35–54 years males.

Time series of suicide attempts between 1990 and 2010 in 26 countries (25 European countries + USA) grouped by trajectories.
ASDRs Age-standardized death rates. Group 1: Armenia and Greece. Group 2: Italy, Spain, United Kingdom, Netherlands, Portugal. Group 3: Austria, Bulgaria, Croatia, Czech Republic, Germany, France, Norway, Sweden, Belgium, Ireland, Poland, Romania, USA. Group 4: Estonia, Finland, Hungary, Latvia, Slovenia. Group 5: Lithuania.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Fond, G., Llorca, PM., Boucekine, M. et al. Disparities in suicide mortality trends between United States of America and 25 European countries: retrospective analysis of WHO mortality database. Sci Rep 6, 20256 (2016). https://doi.org/10.1038/srep20256
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep20256
This article is cited by
-
Trend of years of life lost due to suicide in Iran (2006–2015)
International Journal of Public Health (2018)
-
Spatiotemporal Suicide Risk in Germany: A Longitudinal Study 2007–11
Scientific Reports (2017)
-
Sociodemographic Antecedent Validators of Suicidal Behavior: A Review of Recent Literature
Current Psychiatry Reports (2016)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
