
Abstract
The objective of this study is to assess whether statin use is associated with beneficial effects on COPD outcomes. We conducted a systematic review and meta-analysis of all available studies describing the association between statin use and COPD mortality, exacerbations and cardiovascular events. Medline, Embase, Web of Science and the Cochrane Central Register of Controlled Trials were searched, with no restrictions. The hazard ratio (HR) with 95% confidence interval (CI) was estimated. Fifteen studies with a total of 238,459 patients were included. Nine articles provided data on all-cause mortality (124,543 participants) and they gave a HR of 0.62 (95% CI 0.52 to 0.73). Three studies provided data on cancer mortality (90,077 participants), HR 0.83 (0.65 to 1.08); four studies on COPD mortality (88,767 participants), HR 0.48 (0.23 to 0.99); and three studies on cardiovascular mortality (90,041 participants), HR 0.93 (0.50 to 1.72). Six articles provided data on COPD exacerbation with or without hospitalization (129,796 participants), HR 0.64 (0.55 to 0.75). Additionally, the use of statins was associated with a significant reduction risk of myocardial infarction, but not for stroke. Our systematic review showed a clear benefit of statins in patients with COPD.
Similar content being viewed by others


Introduction
Statins, 3-hydroxy-3-methyl glutaryl coenzyme A (HMG-CoA) reductase inhibitors, are commonly used in clinical practice to treat dyslipidemia1. In addition to the lowering of serum cholesterol, recent data indicated that statins have potent anti-inflammatory and immunomodulatory properties called “pleiotropic effects”2. Due to these properties, it has been suggested that these drugs may have beneficial effects in patients with chronic obstructive pulmonary disease (COPD)3,4,5. Most population-based observational studies have reported associations between statins and a reduced risk of mortality and hospitalization among COPD patients6,7,8,9,10,11,12,13,14,15,16,17,18,19,20. In vitro and animal studies convincingly show that statins can reduce airway inflammation by mechanisms that are unrelated to their effects on cholesterol metabolism21,22.
There is an increasing interest in determining whether statins improve the prognosis of patients with COPD. In 2009, two reviews suggested that statins might have a beneficial role in the treatment of COPD23,24. Since then, several additional trials have been conducted in this setting7,8,9,11,12,17,19,20,25. Overall, the results of some of the trials showed a beneficial effect, but the results were inconsistent when all trials were considered. We therefore conducted a systematic review and meta-analysis of all available studies describing the association between statin use and COPD mortality, exacerbations and cardiovascular events.
Results
Study selection
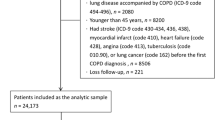
The electronic database search yielded 806 publications (Fig. 1). Another 4 studies were identified by manual searching. After exclusion of duplicates and studies that did not fulfil the inclusion criteria, 34 remaining articles were relevant for this meta-analysis. On more detailed review, an additional 19 studies were excluded for the following reasons: no outcome of interest, duplicate data, fewer than 100 participants and the inclusion of patients with other pulmonary disease. We finally included 15 studies in our systematic review and meta-analysis.

Details of literature search and study selection.
Study characteristics
Fifteen articles with a total of 238,459 participants with COPD were included in our study (Table 1)7,8,9,10,11,12,13,14,15,16,17,18,19,20. All patients The selected studies were published between 2006 and 2013. Most of the studies enrolled more than 1,000 participants6,7,8,9,12,13,14,15,16,17,19 and some of them were nationwide studies7,8,9,12,13,14,17,19. The length of follow-up and risk factors adjusted for each study are provided in Supplementary Table 1. The results of the study quality assessment showed moderate to high quality for all studies (Supplementary Tables 2, 3 and 4). Ten studies were prospective designes6,7,8,9,11,12,15,16,19,20 and five were retrospective cohorts10,13,14,17,18. Among these studies, one report included data from a matched cohort study and a separate case-control study and each group was considered as a separate study in the analyses15. Nine studies reported all-cause mortality6,7,8,9,10,11,12,13,14, three reported cancer mortality12,15,16, four reported COPD mortality12,15 and three reported cardiovascular mortality7,12,15. Six cohort studies detected the effect of statin treatment on the risk of COPD exacerbation with or without hospitalization11,14,17,18,19,20. These trials were conducted in 9 countries: Canada, Norway, the Netherlands, New Zealand, Sweden, Turkey, China, the United Kingdom and the United States.
Effects of intervention
All-cause and cause-specific mortality
Table 2 shows the HRs for total and cause-specific mortality and major coronary events. The hazard ratio (HR) for all-cause mortality was significantly reduced in the statin-exposed group compared with individuals in the statin-unexposed group (HR 0.62, 95% CI 0.52 to 0.73; Fig. 2). However, no significant association of statin use with a decrease risk of cancer mortality was observed (HR 0.83, 95% CI 0.65 to 1.08; Supplementary Figure 1). In the meta-analyses of the two trials with four comparisons in COPD mortality, the HR for patients treated with statins was 0.48 (95% CI 0.23 to 0.99; Supplementary Figure 1) compared with statin non-users. For cardiovascular mortality, the HR for statin users versus statin non-users was 0.93 (95% CI 0.50 to 1.72; Supplementary Figure 1).

Forest plot showing effect of statins on all-cause mortality.
COPD exacerbation, hospitalization and cardiovascular events
The meta-analysis of six cohort studies detected a protective effect of statin treatment on the risk of COPD exacerbation with or without hospitalization (HR 0.64, 95% CI 0.55 to 0.75; Fig. 3). In the subgroup analysis, patients receiving statins presented both a lower risk of mild COPD exacerbation (HR 0.64, 95% CI 0.55 to 0.75) and a lower risk of severe COPD exacerbation requiring hospitalization (HR 0.64, 95% CI 0.55 to 0.75). Additionally, the use of statins was associated with a significantly reduced risk of myocardial infarction (HR 0.69, 95% CI 0.49 to 0.99).

Forest plot showing effect of statins on COPD exacerbation with or without hospitalization.
Sensitivity analysis
For all-cause mortality, the pooled result remained robust when omitting one study at a time and calculating the pooled HRs for the remainder of the studies. In a sensitivity analysis that included 7 prospective cohort studies, the pooled HR for all-cause mortality was 0.65 (95% CI 0.54 to 0.79). The study by Ekstrom et al.8 was the main origin of heterogeneity for all-cause mortality. After exclusion of this study, the heterogeneity was significantly decreased (P = 0.122, I2 = 38.6%; HR 0.58, 95% CI 0.51 to 0.66). For COPD exacerbation with or without hospitalization, the result of the meta-analysis was not affected by any single study. There was evidence of statistical heterogeneity of HR across studies (P = 0.011, I2 = 66.1%). A subgroup analysis by the severity of COPD exacerbation was performed. The heterogeneity between studies was eliminated in the severe COPD exacerbation requiring hospitalization group (P = 0.586, I2 = 0%). Three studies presented the impact of statins on all-cause mortality by relative risk (RR)12,13,14. After exclusion of these studies, the pooled HR for all-cause mortality was 0.71 (95% CI 0.63 to 0.81). In addition, after exclusion of moderate quality studies10,13, a statistically similar result was obtained (HR 0.65, 95% CI 0.54 to 0.79; Supplementary Figure 2).
Analysis of publication bias
Visual inspection of the funnel plot for each outcome did not show asymmetry, suggesting no substantial evidence of publication bias. This was further confirmed by Egger's linear regression asymmetry test for each outcome (for all-cause mortality, P = 0.83, Supplementary Figure 3; COPD exacerbation with or without hospitalization, P = 0.16, Supplementary Figure 4). Funnel plots were not evaluated for secondary objectives because no other outcome had five or more available studies.
Discussion
In this systematic review and meta-analysis of 238,459 cases of COPD from 15 articles, we found a beneficial, statistically significant association between statin treatment and COPD outcomes. Statin use was associated with a 38% reduction in all-cause mortality (95% CI 0.52 to 0.73) and a 52% reduction in COPD mortality (95% CI 0.23 to 0.99). Patients receiving statins presented a 36% lower risk of COPD exacerbation with or without hospitalization (95% CI 0.55 to 0.75).
The results observed in our review for statin use and COPD outcomes may have several alternative explanations. It is possible that there are potential beneficial effects of statins on cardiovascular comorbidities. It is known that smoking is a causative factor in the majority of patients with COPD and is a causative factor in the development of coronary artery disease. Cardiovascular comorbidities are common in COPD patients. A large cohort study involving 384,888 subjects observed that the prevalence of coronary artery disease was significantly higher among COPD patients than those in matched non-COPD controls (33.6% vs. 27.1%)26. In subjects with mild to moderate airways obstruction, every 10% reduction of forced expiratory volume in one second (FEV1) was associated with a 28% increase in cardiovascular mortality and a 20% increase in the risk for non-fatal coronary events27. The protective effect of statins could be explained by their pleiotropic effects, including anti-inflammatory, antithrombotic and immunomodulatory effects28,29,30,31. In a randomized controlled trial, the investigators demonstrated that treatment with statins caused a significant decrease in systemic inflammation markers such as C-reactive protein (CRP) and interleukin-6 (IL-6) in patients with COPD28. In another report, Undas et al.30 observed that fibrin clots became more permeable, less compact and faster lysable following three-month statin therapy in COPD patients. Additionally, it should be noted that statins could regulate the balance of Th1/Th2 cells by inhibition of Th1 development and augmentation of Th2 development of CD4 + T cells31. Improvements in pulmonary haemodynamics may be another potential benefit of statins in COPD32,33. Pulmonary hypertension (PH) is a common complication of COPD and it is associated with increased risks of exacerbation and decreased survival34. In patients with severe COPD, statin use was associated with significantly lower pulmonary arterial wedge pressure (PAWP) and mean pulmonary arterial pressure (mPAP)32. Specifically, statins have been shown to inhibit the progression of PH by inhibiting endothelin-1 synthesis33.
The findings from our study that statins reduced mortality in patients with COPD were consistent with most of the included studies6,7,9,10,12,13,14. However, a large multi-centre RCT showed that statins had no effect on COPD exacerbations, which was inconsistent with our findings25. Several reasons might be accountable for this. Only moderate-to-severe COPD patients were included in this RCT and it is unclear whether statins were beneficial for patients with less impairment. In addition, the mean followed-up time of this RCT was less than 2 years, which might be a significantly different compared to the long term effect. However, in this RCT, the authors did not evaluate effect of statin in the form of HR or RR, which limit our quantitative analysis with this study.
To the best of our knowledge, this is the most comprehensive systematic review and meta-analysis to date to quantitatively evaluate whether statin use is associated with beneficial effects in COPD patients. Compared with previous systematic reviews24,25,35,36, our findings extend the evidence in four ways. First, three previous studies identified half the number of studies compared with our study and did not evaluate some clinically significant outcomes such as cause-specific mortality and cardiovascular events24,25,35. Second, the relationship between statins and COPD exacerbation was only investigated in our meta-analysis. Thirdly, we included only large scale studies involving a minimum of 100 participants. Eleven of the studies in our review enrolled more than 1,000 participants and eight were nationwide studies. Finally, we performed sensitivity analyses and used clinically relevant subgroups to explore the potential heterogeneity not previously reported.
The validity of a meta-analysis mostly depends on the quality of the included studies. The strengths of this meta-analysis included the large sample size of the component studies, which significantly increased the statistical power to detect potential associations. Additionally, most established risk factors for COPD were adjusted for in the fully-adjusted models in the included studies. The quality across various outcomes was moderate or high for the interested outcomes.
Several limitations of this meta-analysis are worth discussing. First, heterogeneity was observed among the included studies, although the results were generally consistent for the frequently reported outcomes. This may reflect differences in sample sizes, severity of disease, treatment strategy and many other factors among the studies. Second, all individual studies were observational in nature but some small sample size studies (less than 100 participants) were not included in our analysis, which might lead to residual confounding or other biases. Third, three studies presented the impact of statins on all-cause mortality by RR. Considering this limitation, we further performed a sensitivity analysis, in which three studies presented with RR were removed at a time while the rest were analysed. However, statistically similar results were obtained. Fourth, optimized search strategies were required to increase the statistical power of the meta-analysis. However, to avoid missing some available publications, we used broad search strategies for studies during this step. Most studies did not report the type of statin and statin dose, which limited our further assessment of dose-response relation between statins and COPD outcomes. Nevertheless, because all studies were conducted in recent years, we believe that the patients were treated similarly based on current clinical practice recommendations. Finally, RCT is considered to be the highest-quality evidence and the gold standard for a clinical trial. However, few RCT was conducted on statins in COPD and no RCT met the inclusion criteria. Well-designed RCT of statins therapy in COPD are needed.
Our systematic review and meta-analyses showed that statin use was associated with a reduction in all-cause mortality and COPD mortality. In addition, patients receiving statins presented a lower risk of COPD exacerbation with or without hospitalization. Given the lack of evidence from multicentre randomized controlled trials, there remains a need for well-designed clinical studies on the important clinical outcomes identified, including the long term effects of statins in COPD.
Methods
Search strategy
We conducted the systematic review in accordance with the 2009 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement (Supplementary Text 1) and the MOOSE guidelines for reporting meta-analyses of observational studies37,38. We conducted a literature search in the MEDLINE (1966 to April 2014), Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library Issue 1, 2014), Web of Science (1994 to April 2014) and EMBASE databases (1980 to April 2014), using the following search terms: hydroxymethylglutaryl-CoA reductase inhibitors or anticholesteremic agents or statin or atorvastatin or cerivastatin or fluvastatin or pravastatin or pitavastatin or rosuvastatin or simvastatin and chronic obstructive pulmonary disease or COPD, as well as combinations of these terms. No language restriction was applied. The abstracts of relevant scientific meetings were examined to ensure complete review of the available studies. To ensure that all relevant trials were included, we screened bibliographies of relevant review articles and searched the clinical trial registry (www.clinicaltrials.gov) for additional studies.
Study selection
Two investigators (CC, YW) identified suitable trials from the literature search and independently reviewed the titles and abstracts of the articles. Studies were included if they reported statin therapy in patients with COPD. We used broad inclusion criteria in this step and studies could be included by either of the two investigators. Further screening was based on full-text review. To be included, studies had to report at least one outcome of interest (mortality, acute episode of COPD, hospitalization, or cardio-cerebrovascular events) and had to enroll a minimum of 100 participants. In quantitative synthesis analysis, the outcomes that were included had at least two reports and were excluded when there was only one study. Differences between the reviewers were resolved by discussion and, if necessary, in consultation with a senior investigator (HS). In the case of multiple publications, we included the first published or more comprehensive study in the analysis.
Data extraction and quality assessment
We abstracted information related to study design, study’s characteristics (the first author’s surname, year of publication, country and number of participants), participants’ characteristics (age and sex), characteristics of the exposure or intervention evaluated and information on the reported outcomes. The multivariate adjusted HR or RR and corresponding 95% CI of time-to-event data were directly extracted from the original study. When studies reported mortality at several time intervals, the longest follow-up period was selected for analysis.
Quality assessment was performed by two individual authors according to the 9-star Newcastle-Ottawa scale, which was developed to assess the quality of nonrandomized studies39. This scale is judged on three perspectives: the selection of the study groups (4 scores); the comparability of the groups (2 scores); and the exposure or outcome of interest (3 scores). We assigned scores of 0–3, 4–6 and 7–9 for low, moderate and high quality of studies, respectively. Moreover, the Downs and Black scoring system was used to assess the quality of each study using the subscales involving reporting, external validity, internal validity-bias, internal validity-confounding and power40.
Statistical analysis
We used the inverse variance method where the weight of each study was proportional to the variance of the observed minus expected number of events. Patient characteristics, statin dose and length of follow-up differed across studies, thus the multivariate adjusted outcome data were analysed to assess the HRs. For each outcome, we first assessed study heterogeneity with the Cochran Q statistic, with P < 0.10 indicating evidence of heterogeneity. The degree of heterogeneity was measured by the I2statistic, with suggested thresholds for low (25%–49%), moderate (50%–74%) and high ( 75%) values41. We conducted additional sensitivity analyses to explore the influence of the quality and risk of bias found in the included studies. We assessed publication bias for outcomes with funnel plots, both visually and formally with Egger’s test42. All analyses were performed with Stata version 12 (StataCorp, College Station, Texas). Statistical tests were judged statistically significant if the two-sided P value was less than 0.05.
75%) values41. We conducted additional sensitivity analyses to explore the influence of the quality and risk of bias found in the included studies. We assessed publication bias for outcomes with funnel plots, both visually and formally with Egger’s test42. All analyses were performed with Stata version 12 (StataCorp, College Station, Texas). Statistical tests were judged statistically significant if the two-sided P value was less than 0.05.
Additional Information
How to cite this article: Cao, C. et al. The effect of statins on chronic obstructive pulmonary disease exacerbation and mortality: a systematic review and meta-analysis of observational research. Sci. Rep. 5, 16461; doi: 10.1038/srep16461 (2015).
References
Baigent C. et al. Cholesterol Treatment Trialists’ (CTT) Collaborators. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 366, 1267–78 (2005).
Liao J. K. & Laufs U. Pleiotropic effects of statins. Annu. Rev. Pharmacol. Toxicol. 45, 89–118 (2005).
Ishida W. et al. Decrease in mortality rate of chronic obstructive pulmonary disease (COPD) with statin use: a population-based analysis in Japan. Tohoku. J. Exp. Med. 212, 265–73 (2007).
Cazzola M., Matera M. G., Rogliani P. & Page C. Treating systemic effects of COPD. Trends. Pharmacol. Sci. 28, 544–50 (2007).
Young R. P., Hopkins R. & Eaton T. E. Potential benefits of statins on morbidity and mortality in chronic obstructive pulmonary disease: a review of the evidence. Postgrad. Med. J. 85, 414–21 (2009).
van Gestel Y. R. et al. Effect of statin therapy on mortality in patients with peripheral arterial disease and comparison of those with versus without associated chronic obstructive pulmonary disease. Am. J. Cardiol. 102, 192–6 (2008).
Sheng X. et al. Effect of statins on total cholesterol concentrations, cardiovascular morbidity and all-cause mortality in chronic obstructive pulmonary disease: a population-based cohort study. Clin. Ther. 34, 374–84 (2012).
Ekström M. P., Hermansson A. B. & Ström K. E. Effects of cardiovascular drugs on mortality in severe chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care. Med. 187, 715–20 (2013).
Lawes C. M. et al. Statin use in COPD patients is associated with a reduction in mortality: a national cohort study. Prim. Care. Respir. J. 21, 35–40 (2012).
Søyseth V., Brekke P. H., Smith P. & Omland T. Statin use is associated with reduced mortality in COPD. Eur. Respir. J. 29, 279–83 (2007).
Bartziokas K. et al. Statins and outcome after hospitalization for COPD exacerbation: a prospective study. Pulm. Pharmacol. Ther. 24, 625–31 (2011).
Lahousse L. et al. Statins, systemic inflammation and risk of death in COPD: the Rotterdam study. Pulm. Pharmacol. Ther. 26, 212–7 (2013).
Mortensen E. M. et al. Impact of statins and ACE inhibitors on mortality after COPD exacerbations. Respir. Res. 10, 45 (2009).
Mancini G. B. et al. Reduction of morbidity and mortality by statins, angiotensin-converting enzyme inhibitors and angiotensin receptor blockers in patients with chronic obstructive pulmonary disease. J. Am. Coll. Cardiol. 47, 2554–60 (2006).
Frost F. J., Petersen H. & Tollestrup K. & Skipper B. Influenza and COPD mortality protection as pleiotropic, dose-dependent effects of statins. Chest. 131, 1006–12 (2007).
van Gestel Y. R. et al. COPD and cancer mortality: the influence of statins. Thorax. 64, 963–7 (2009).
Wang M. T. et al. Statin use and risk of COPD exacerbation requiring hospitalization. Am. J. Med. 126, 598–606.e2 (2013).
Blamoun A. I. et al. Statins may reduce episodes of exacerbation and the requirement for intubation in patients with COPD: evidence from a retrospective cohort study. Int. J. Clin. Pract. 62, 1373–8 (2008).
Huang C. C. et al. Statin use and hospitalization in patients with chronic obstructive pulmonary disease: a nationwide population-based cohort study in Taiwan. Clin. Ther. 33, 1365–70 (2011).
Ozyilmaz E., Kokturk N., Teksut G. & Tatlicioglu T. Unsuspected risk factors of frequent exacerbations requiring hospital admission in chronic obstructive pulmonary disease. Int. J. Clin. Pract. 67, 691–7 (2013).
Ou X. M. et al. Simvastatin attenuates experimental small airway remodelling in rats. Respirology. 14, 734–45 (2009).
Chen Y. J. et al. Simvastatin attenuates acrolein-induced mucin production in rats: involvement of the Ras/extracellular signal-regulated kinase pathway. Int. Immunopharmacol. 10, 685–693 (2010).
Janda S., Park K., FitzGerald J. M., Etminan M. & Swiston J. Statins in COPD: a systematic review. Chest. 136, 734–43 (2009).
Dobler C. C., Wong K. K. & Marks G. B. Associations between statins and COPD: a systematic review. BMC. Pulm. Med. 9, 32 (2009).
Criner G. J. et al. Simvastatin for the prevention of exacerbations in moderate-to-severe COPD. N. Engl. J. Med. 370, 2201–10 (2014).
Mapel D. W., Dedrick D. & Davis K. Trends and cardiovascular co-morbidities of COPD patients in the Veterans Administration Medical System, 1991–1999. COPD. 2, 35–41 (2005).
Anthonisen N. R., Connett J. E., Enright P. L. & Manfreda J. Lung Health Study Research Group: Hospitalizations and mortality in the Lung Health Study. Am. J. Respir. Crit. Care. Med. 166, 333–9 (2002).
Lee T. M., Lin M. S. & Chang N. C. Usefulness of C-reactive protein and interleukin-6 as predictors of outcomes in patients with chronic obstructive pulmonary disease receiving pravastatin. Am. J. Cardiol. 101, 530–5 (2008).
Rezk N. A. & Elewa A. Anti inflammatory effects of statin in COPD. Egypt. J. Chest. Dis. Tuberc. 62, 65–9 (2013).
Undas A. et al. Fibrin clot properties are altered in patients with chronic obstructive pulmonary disease. Beneficial effects of simvastatin treatment. Thromb. Haemost. 102, 1176–82 (2009).
Hakamada-Taguchi R. et al. Inhibition of hydroxymethylglutaryl-coenzyme a reductase reduces Th1 development and promotes Th2 development. Circ. Res. 93, 948–56 (2003).
Reed R. M. et al. Statin therapy is associated with decreased pulmonary vascular pressures in severe COPD. COPD. 8, 96–102 (2011).
Lee T. M., Chen C. C., Shen H. N. & Chang N. C. Effects of pravastatin on functional capacity in patients with chronic obstructive pulmonary disease and pulmonary hypertension. Clin. Sci (Lond). 116, 497–505 (2009).
Chaouat A., Naeije R. & Weitzenblum E. Pulmonary hypertension in COPD. Eur. Respir. J. 32, 1371–85 (2008).
Beri A., Sural N. & Mahajan S. B. Non-atheroprotective effects of statins: a systematic review. Am. J. Cardiovasc. Drugs. 9, 361–70 (2009).
Horita N. et al. Statins reduce all-cause mortality in chronic obstructive pulmonary disease: a systematic review and meta-analysis of observational studies. Respir. Res. 15, 80 (2014).
Moher D., Liberati A., Tetzlaff J. & Altman D. G. The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS. Med. 6, e1000097 (2009).
Stroup D. F. et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 283, 2008–12 (2000).
Wells G. A., de Sousa M. R., Fereguetti T. O. & Rabello A. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.htmAccessed. (Date of access: 2 Apr 2012).
Downs S. H. & Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community. Health. 52, 377–84 (1998).
Higgins J. P., Thompson S. G., Deeks J. J. & Altman D. G. Measuring inconsistency in meta-analyses. BMJ. 327, 557–60 (2003).
Egger M., Davey Smith G., Schneider M. & Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 315, 629–34 (1997).
Acknowledgements
This work was funded by the Key Program of National Natural Science Foundation of China (No. 81130001), National Key Technologies R&D Program for the 12th Five-year Plan (No. 2012BAI05B01) and Sector Funds, Health Ministry of China (No. 201002008).
Author information
Authors and Affiliations
Contributions
C.C., Y.F.W. and H.H.S. designed the experiments. C.C., Y.F.W., Z.W.X., D.L., C.Z., T.W.L., W.L. and H.H.S. carried out the experiments and calculations. C.C., Y.F.W., Z.W.X., D.L., C.Z. and H.H.S. wrote and edited the paper.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Cao, C., Wu, Y., Xu, Z. et al. The effect of statins on chronic obstructive pulmonary disease exacerbation and mortality: a systematic review and meta-analysis of observational research. Sci Rep 5, 16461 (2015). https://doi.org/10.1038/srep16461
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep16461
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
