
Abstract
Esophageal carcinoma (EC) is a serious malignancy and its epidemiologic etiology is not fully explained. We performed this review to investigate the association between teeth loss and teeth brushing and the risk of EC. A systematic search was conducted to identify all relevant studies. The Q test and I2 statistic were used to examine between-study heterogeneity. Pooled odds ratios (ORs) with corresponding 95% confidence intervals (CIs) were considered by fixed or random effects models. Furthermore, we conducted subgroup analyses based on study design, the studies’ geographic regions and case type of origin. Modified Egger linear regression test was used to estimate publication bias. Ten articles were included. Pooled analyses indicated that teeth loss was associated with an increased risk of EC for Asians (OR, 1.52; 95% CI: 1.30, 1.78) and high frequency of teeth brushing was associated with a lower incidence of EC (OR, 0.62; 95%CI: 0.43, 0.89). Subgroup analyses showed consistent results and no publication bias existed. Teeth loss and teeth brushing play potential roles in the progressing of EC. People should take care of their oral health in daily life. And large well-designed researches are needed to fully describe the association between teeth health and EC risk.
Similar content being viewed by others

Introduction
Esophageal carcinoma (EC) is the eighth most common incident cancer and the sixth leading cause of cancer death worldwide. EC affects more than 450,000 people worldwide1,2,3 and respect to prognosis and a fatal outcome in the great majority of cases, EC is considered as a serious malignancy4. For both of incidence and mortality, the rates of EC were much higher in rural areas than in urban areas, in males than in females5. The reviews on the overall age-specific incidence and mortality rates of EC showed that both rates were relatively low before 45 years old and then gradually increased, reaching peak in the seventh or eighth decades of life2,5.
Squamous cell carcinoma and adenocarcinoma are the commonly seen forms of EC worldwide. Esophageal squamous cell carcinoma (ESCC) is the predominant form in developing countries, whereas a shift in epidemiology has been seen for some developed countries, where the incidence of esophageal adenocarcinoma (EAC) now exceeds that of squamous-cell types1,6,7.
Numerous epidemiologic investigations and researches have focused on the epidemiological etiology to explain the rapid increase of this lethal cancer8,9,10. Tobacco use, alcohol consumption and mutations of enzymes that metabolizing alcohol have been the primary causes of ESCC, however, alcohol consumption is not considered as a risk factor for EAC11,12,13. For EAC, symptomatic gastro-esophageal reflux disease, Barrett’s esophagus, obesity are considered as major risk factors7,14,15. Therefore, as for teeth loss and the frequency of teeth brushing, the association with EC risk is controversial. Poor oral health has been associated with increased risk of cancer at several sites (i.e. oral cancer, gastric cancer, head and neck cancer, throat cancer etc.)16,17,18,19 and other chronic diseases such as cardiovascular disease20,21 and diabetes22 are reported to have an association with poor oral hygiene.
Studies have researched on the association between teeth loss and teeth brushing and the risk of EC, but with inconsistent results1,23,24. Thus, the aims of this study were to carry out a meta-analysis regarding the contributions of teeth brushing and teeth loss to the risk of EC.
Methods
The Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) guidelines were followed for the current study25.
Search strategy
Studies that investigated the association between teeth loss and frequency of teeth brushing and EC risk were identified using a search strategy in the following databases: Medline, Embase, Google Scholar, ISI Web of Science, Cochrane Central Register of Controlled Trials to Aug 1st, 2014. Search terms were listed as follows: “oral hygiene” or “oral care” or| “oral health” or “tooth loss” or “teeth loss” or “dental health” or “toothbrushing” or “tooth brushing” or “teeth brushing” or “mouthwash” or “mouthwashes”, “esophageal” or “esophagus” or “oesophagus” or “oesophageal”, “cancer” or “carcinoma” or “tumor” or “neoplasm”. Moreover, we reviewed the reference lists from retrieved articles to search for further relevant studies. When the same data were reported in more than one publication, only the studies with more complete data and more extensive interval of enrollment were included in the study. We followed standard criteria for conducting meta-analyses and reporting the results.
Eligibility criteria
Each identified study was independently reviewed by two investigators (Chen and Nie) to determine whether an individual study was eligible for inclusion in this meta-analysis. The inclusion criteria are as follows: (1) case-control or cohort study design; (2) exposure of interest was teeth health, including number of teeth loss and the frequency of teeth brushing; (3) outcome of interest was EC; (4) odds ratio (OR) or relative risk (RR) with 95% confidence interval (CI; or data to calculate them) had to be clearly described in the original study.; (5) only articles published in English and studies performed in humans were included. and (6) animal studies, reviews, comments and editorials were excluded. When there was disagreement between the two investigators about eligibility of the article, it was resolved by consensus with a third reviewer (Zhu).
Data extraction and quality assessment
A preset data sheet was developed to extract information from the retrieved studies. From each included study, the following data were extracted: first author, publication year, location where the study was performed, characteristics of study population, number of study sample, study results (ORs/RRs and 95% CI ). Both teeth loss and teeth brushing were categorized in 2 levels: the lowest teeth loss group (reference group) and the highest teeth loss group; the lowest frequency teeth brushing group (reference group) and the highest frequency teeth brushing group. Two reviewers extracted all the data independently.
The quality of the included studies was estimated by the 9-star Newcastle-Ottawa Scale and Agency for Healthcare Research and Quality (http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp, maximum score 9 points). This scale assessed the selection of patient, the comparability of group and the quality of the sampling process.
Statistical analysis
Pooled measure was calculated as the inverse variance-weighted mean of the logarithm of effects (RRs/HRs/ORs with 95% CI) to assess the strength of association between teeth loss and frequency of teeth brushing and EC. Tests for among-study heterogeneity were performed using the Q test and Higgins I2 statistics26. In the presence of substantial heterogeneity (I2 > 50%), the DerSimonian and Laird random effects model (REM) was adopted; otherwise, we used the fixed effects model (FEM) as the pooling method. The ‘leave one out’ sensitivity analysis was carried out using I2 > 50% as the criteria to evaluate the key studies with substantial impact on between-study heterogeneity27. Publication bias was estimated by Egger’s regression asymmetry test28. Data analyses were performed using Stata (version 13.1; Stata Corporation, College Station, TX,USA) software. All reported probabilities (p-values) were two-sided and the values less than 0.05 were considered significant.
Results
Study characteristics
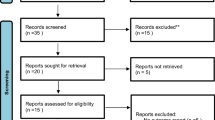
Figure 1 showed the detailed steps of literature search and for the 478 potentially relevant articles, ten articles29,30,31,32,33,34,35,36,37,38 with twelve studies ultimately met the inclusion criteria for this meta-analysis. These ten included articles were published between 1992 and 2014 and among them six articles29,30,31,34,35,36 with seven studies reported the association between teeth brushing and EC risk, eight articles29,31,32,33,35,36,37,38 with nine studies reported the association between teeth loss and EC risk. The study design of original articles reported teeth brushing and EC risk were all case-control studies. For articles reported teeth loss and the risk of EC, six were case-control design and three cohort. For the participants of the included articles, six articles included ESCC only and the remaining articles included EC patients (ECs include ESCCs and EACs. In these studies they just analyze EC as a whole and did not shown the results of ESCCs and EACs separately.) Most studies provided risk estimates that were adjusted for age (11 studies), sex (9 studies), smoking (9 studies), drinking (9 studies), fruit and vegetable consumption (7); fewer were adjusted for residence (3 studies), BMI (3 studies), education (3 studies). Quality of the included studies was assessed using the Newcastle Ottawa Scale and all the studies were scored 7 or above out of a possible nine. The details of all the included studies are shown in Table 1 and Table 2.

Flow diagram of study selection based on the eligibility criteria.
Frequency of teeth brushing and EC risk
The meta-analysis of the association between teeth brushing and EC risk consisted of six articles with seven studies. Five studies in Asia, one in America and one in Europe. The individual estimated ORs and the pooled ORs were presented in Fig. 2. High heterogeneity (I2 = 72.1%, p = 0.002) existed among the studies and the pooled meta-analysis indicated a significant association between teeth brushing and EC risk by REM with an OR = 0.62 (95% CI: 0.43,0.89). Compared with the reference group, people have more frequency of teeth brushing have a lower risk of EC.

Forest plot for the association between teeth brushing and esophageal carcinoma risk.
Four articles29,31,34,35,36 with four studies reported the association between teeth brushing and ESCC risk. Pooled results showed a decreased risk of ESCC with people who have more frequency of teeth brushing (pooled results were shown in Table 3).
Subgroup analysis was conducted based on the study’s original design and study location, respectively. Results showed that teeth brushing was associated with the risk of ESCC and people with high frequency of teeth brushing had a lower incidence of EC in Asia (details were shown in Table 3).
To further explore the potential sources of heterogeneity and the effects of study characteristics on the overall estimates, exploratory meta-regression was performed with study-location (Asia , Europe and America) and source of controls (PB or HB). However, neither of the variables was identified as potential source of between-study heterogeneity. In the sensitivity analysis, no study was found to be a key contributor to between-study heterogeneity.
Number of teeth loss and EC risk
Eight articles with nine studies regarding the relationship between teeth loss and the risk of EC were included in the meta-analysis. Five studies were conducted in Asia, two in America and two in Europe. The risk estimates for each study and the summary ORs were shown in Fig. 3. No between-study heterogeneity was observed (I2 = 29.9%, p = 0.179) and pooled results showed that teeth loss was related to the occurrence of EC, OR = 1.46 (95% CI: 1.27,1.69). Compared with people who had less teeth loss, people who had more teeth loss had a 46 percent increased incidence of EC.

Forest plot for the association between teeth loss and esophageal carcinoma risk.
Subgroup analysis was conducted based on the study’s original design, study-location and case type, respectively. Results showed that teeth loss was associated with the risk of ESCC and for both cohort studies and case-control studies the results were consistent. People with more teeth loss had a higher incidence of EC in Asia, whereas teeth loss was not significantly associated with EC risk in America and Europe (details were shown in Table 3).
The estimate OR and 95%CI in Sato et al. 2011 did not adjusted for potential confounding factors. When excluded this article in the pooled analysis, the results were stable (OR = 1.36 , 95% CI: 1.16, 1.59; I2 = 0).
Potential publication bias
No publication bias was observed in the above-mentioned analyses by the modified Egger linear regression test (with the p values 0.132, 0.974, respectively. Table 3). Figures 4 and 5 showed the funnel plots.

Funnel plot for the association between teeth brushing and esophageal carcinoma.

Funnel plot for the association between teeth loss and esophageal carcinoma.
Discussion
The results of this meta-analysis suggested that both teeth brushing and teeth loss were associated the risk of EC. People with higher frequency of teeth brushing had a lower risk of EC. People who had more teeth loss had a higher incidence of EC for Asians, but not for Americans and Europeans. Further subgroup analyses showed consistent results.
To our knowledge, the present meta-analysis is the first one to investigate association between teeth loss, teeth brushing and the risk of EC. The specific mechanisms underlying the association of teeth loss and EC risk are not fully understood. Generally, our results are, in part, consistent with other evidence of increased risk of gastric cancer, head and neck cancer, pancreatic cancer etc.16,17. For EC, one potential explanation is that teeth loss might alter the dietary pattern to one that increases the risk of disease39. Second, we hypothesized that teeth loss would cause individuals to swallow large, poorly chewed boluses of food which might irritate mechanical trauma on the esophagus. Third, teeth loss is associated with an oral flora which may reduce the process of nitrate to nitrite40,41. This nitrite can then spontaneously react with amines and be converted to carcinogenic nitrosamines, some of which be gastrointestinal organ-specific carcinogens42,43.
Between-study heterogeneity is common in meta-analyses and characteristics that vary among studies, such as published year, study-location, source of controls, design and quality of original article might act as the sources of between-study heterogeneity44,45. Our meta-analysis showed significant between-study heterogeneity for teeth brushing and EC risk. Therefore, meta-regression and “leave one out” sensitivity analysis did not find the potential contributors for between-study heterogeneity.
There are limitations in our present meta-analysis. First, our study only included articles published in English and the number of studies included in this research was limited, which might induce false or unstable results. Second, grouping methods of teeth loss and teeth brushing were varied and complex in the original studies, which made it difficult to regroup them. Therefore, we just calculated data of the high level of teeth loss or teeth brushing compared with the low level without considering the middle groups. Third, for teeth brushing and EC risk, significant between-study heterogeneity existed and we could not find potential contributors, although REM was applied, the pooled results might skewed. Forth, owing to the small number of European and American studies, the selection bias was unavoidable and the association among different regions remained unclear. Last but not least, most of the included studies utilized a case-control design (retrospective study), a design that is more vulnerable to recall bias or changes in exposure related to the disease. The results of this study should be interpreted with caution.
Despite the above disadvantages, the present meta-analysis showed a new aspect on identifying risk factors of EC. No publication bias was observed and subgroup analyses showed consistent results, which indicate that our main findings are robust and not artifact of unpublished negative studies. This meta-analysis suggests that teeth loss significantly increases the risk of EC in Asia and daily tooth brushing decreases EC risk. And large well-designed researches are needed to fully describe association between oral health and the incidence of EC.
Additional Information
How to cite this article: Chen, H. et al. Teeth loss, teeth brushing and esophageal carcinoma: a systematic review and meta-analysis. Sci. Rep. 5, 15203; doi: 10.1038/srep15203 (2015).
References
Pennathur, A., Gibson, M. K., Jobe, B. A. & Luketich, J. D. Oesophageal carcinoma. The Lancet 381, 400–412 (2013).
Zhang, Y. Epidemiology of esophageal cancer. World J Gastroenterol 19, 5598–5606 (2013).
Tang, W. R. et al. Epidemiological characteristics and prediction of esophageal cancer mortality in china from 1991 to 2012. Asian Pac J Cancer Prev 15, 6929–6934 (2014).
Mao, W. M., Zheng, W. H. & Ling, Z. Q. Epidemiologic risk factors for esophageal cancer development. Asian Pac J Cancer Prev 12, 2461–2466 (2011).
Chen, W. et al. Esophageal cancer incidence and mortality in China, 2009. J Thorac Dis 5, 19–26 (2013).
Tettey, M. et al. The changing epidemiology of esophageal cancer in sub-Saharan Africa—the case of Ghana. Pan Afr Med J 13, 6 (2012).
Lepage, C., Drouillard, A., Jouve, J. L. & Faivre, J. Epidemiology and risk factors for oesophageal adenocarcinoma. Dig Liver Dis 45, 625–629 (2013).
Zhu, J. et al. Associations of PI3KR1 and mTOR polymorphisms with esophageal squamous cell carcinoma risk and gene-environment interactions in Eastern Chinese populations. Sci Rep 5, 8250 (2015).
Wu, B. et al. Network based analyses of gene expression profile of LCN2 overexpression in esophageal squamous cell carcinoma. Sci Rep 4, 5403 (2014).
Ibiebele, T. I., Taylor, A. R., Whiteman, D. C. & van der Pols, J. C. Eating habits and risk of esophageal cancers: a population-based case-control study. Cancer Causes Control 21, 1475–1484 (2010).
Kumagai, N. et al. Heavy alcohol intake is a risk factor for esophageal squamous cell carcinoma among middle-aged men: A case-control and simulation study. Mol Clin Oncol 1, 811–816 (2013).
Tramacere, I. et al. A meta-analysis on alcohol drinking and esophageal and gastric cardia adenocarcinoma risk. Ann Oncol 23, 287–297 (2012).
Lindblad, M., Rodriguez, L. A. & Lagergren, J. Body mass, tobacco and alcohol and risk of esophageal, gastric cardia and gastric non-cardia adenocarcinoma among men and women in a nested case-control study. Cancer Causes Control 16, 285–294 (2005).
Reid, B. J., Li, X., Galipeau, P. C. & Vaughan, T. L. Barrett’s oesophagus and oesophageal adenocarcinoma: time for a new synthesis. Nat Rev Cancer 10, 87–101 (2010).
Engel, L. S. et al. Population Attributable Risks of Esophageal and Gastric Cancers. JNCI Journal of the National Cancer Institute 95, 1404–1413 (2003).
Chang, J. S. et al. Investigating the association between oral hygiene and head and neck cancer. Oral Oncol 49, 1010–1017 (2013).
Stolzenberg-Solomon, R. Z. et al. Tooth loss, pancreatic cancer and Helicobacter pylori. Am J Clin Nutr 78, 176–181 (2003).
Meyer, M. S., Joshipura, K., Giovannucci, E. & Michaud, D. S. A review of the relationship between tooth loss, periodontal disease and cancer. Cancer Causes Control 19, 895–907 (2008).
Shakeri, R. et al. Association of Tooth Loss and Oral Hygiene with Risk of Gastric Adenocarcinoma. Cancer Prevention Research 6, 477–482 (2013).
Dai, R. et al. A systematic review and meta-analysis of clinical, microbiological and behavioural aspects of oral health among patients with stroke. J Dent 43, 171–180 (2015).
Kebschull, M., Demmer, R. T. & Papapanou, P. N. “Gum bug, leave my heart alone!”—epidemiologic and mechanistic evidence linking periodontal infections and atherosclerosis. J Dent Res 89, 879–902 (2010).
Mohamed, H. G. et al. Association between oral health status and type 2 diabetes mellitus among Sudanese adults: a matched case-control study. Plos One 8, e82158 (2013).
Islami, F. et al. Oesophageal cancer in Golestan Province, a high-incidence area in northern Iran—a review. Eur J Cancer 45, 3156–3165 (2009).
Conway, D. Oral health, mouthwashes and cancer—what is the story? Evid Based Dent 10, 6–7 (2009).
Moher, D., Liberati, A., Tetzlaff, J. & Altman, D. G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol 62, 1006–1012 (2009).
Higgins, J. P. & Thompson, S. G. Quantifying heterogeneity in a meta-analysis. Stat Med 21, 1539–1558 (2002).
Patsopoulos, N. A., Evangelou, E. & Ioannidis, J. P. Sensitivity of between-study heterogeneity in meta-analysis: proposed metrics and empirical evaluation. Int J Epidemiol 37, 1148–1157 (2008).
Egger, M., Davey Smith, G., Schneider, M. & Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 315, 629–634 (1997).
Sato, F. et al. Inverse association between toothbrushing and upper aerodigestive tract cancer risk in a Japanese population. Head Neck 33, 1628–1637 (2011).
Wang, Y. P. et al. Esophageal cancer in Shanxi Province, People’s Republic of China: a case-control study in high and moderate risk areas. Cancer Causes Control 3, 107–113 (1992).
Abnet, C. C. et al. Tooth loss and lack of regular oral hygiene are associated with higher risk of esophageal squamous cell carcinoma. Cancer Epidemiol Biomarkers Prev 17, 3062–3068 (2008).
Abnet, C. C. et al. Tooth loss is associated with increased risk of gastric non-cardia adenocarcinoma in a cohort of Finnish smokers. Scandinavian Journal of Gastroenterology 40, 681–687 (2005).
Abnet, C. C. et al. Prospective study of tooth loss and incident esophageal and gastric cancers in China. Cancer Causes Control 12, 847–854 (2001).
Ahrens, W. et al. Oral health, dental care and mouthwash associated with upper aerodigestive tract cancer risk in Europe: the ARCAGE study. Oral Oncol 50, 616–625 (2014).
Dar, N. A. et al. Poor oral hygiene and risk of esophageal squamous cell carcinoma in Kashmir. Br J Cancer 109, 1367–1372 (2013).
Guha, N. et al. Oral health and risk of squamous cell carcinoma of the head and neck and esophagus: results of two multicentric case-control studies. Am J Epidemiol 166, 1159–1173 (2007).
Hiraki, A., Matsuo, K., Suzuki, T., Kawase, T. & Tajima, K. Teeth loss and risk of cancer at 14 common sites in Japanese. Cancer Epidemiol Biomarkers Prev 17, 1222–1227 (2008).
Michaud, D. S., Liu, Y., Meyer, M., Giovannucci, E. & Joshipura, K. Periodontal disease, tooth loss and cancer risk in male health professionals: a prospective cohort study. The Lancet Oncology 9, 550–558 (2008).
Daly, R. M., Elsner, R. J., Allen, P. F. & Burke, F. M. Associations between self-reported dental status and diet. J Oral Rehabil 30, 964–970 (2003).
Sanchez, G. A., Miozza, V. A., Delgado, A. & Busch, L. Total salivary nitrates and nitrites in oral health and periodontal disease. Nitric Oxide 36, 31–35 (2014).
Zetterquist, W. et al. Oral bacteria—the missing link to ambiguous findings of exhaled nitrogen oxides in cystic fibrosis. Respir Med 103, 187–193 (2009).
Jakszyn, P. & Gonzalez, C. A. Nitrosamine and related food intake and gastric and oesophageal cancer risk: a systematic review of the epidemiological evidence. World J Gastroenterol 12, 4296–4303 (2006).
Larsson, S. C., Bergkvist, L. & Wolk, A. Processed meat consumption, dietary nitrosamines and stomach cancer risk in a cohort of Swedish women. International Journal of Cancer 119, 915–919 (2006).
Higgins, J. P., Thompson, S. G., Deeks, J. J. & Altman, D. G. Measuring inconsistency in meta-analyses. BMJ 327, 557–560 (2003).
Higgins, J., Thompson, S., Deeks, J. & Altman, D. Statistical heterogeneity in systematic reviews of clinical trials: a critical appraisal of guidelines and practice. J Health Serv Res Policy 7, 51–61 (2002).
Acknowledgements
This work was supported by National Natural Science Foundation of China (Grant Number: 81273151).
Author information
Authors and Affiliations
Contributions
C.H. and L.M. contributed to the study design and manuscript drafting. C.H., N.S. and Z.Y. contributed to data collection and statistical analysis. L.M. is responsible for the whole work. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Chen, H., Nie, S., Zhu, Y. et al. Teeth loss, teeth brushing and esophageal carcinoma: a systematic review and meta-analysis. Sci Rep 5, 15203 (2015). https://doi.org/10.1038/srep15203
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep15203
This article is cited by
-
Dental health and lung cancer risk in the Golestan Cohort Study
BMC Cancer (2024)
-
Associations between missing teeth and the risk of cancer in Korea: a nationwide cohort study
BMC Oral Health (2023)
-
Environmental and life-style risk factors for esophageal squamous cell carcinoma in Africa: a systematic review and meta-analysis
BMC Public Health (2023)
-
Relationship between maximum occlusal force and gastrointestinal cancer in community-dwelling older Japanese adults
Scientific Reports (2022)
-
Oral Microbiota Variation: A Risk Factor for Development and Poor Prognosis of Esophageal Cancer
Digestive Diseases and Sciences (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
