
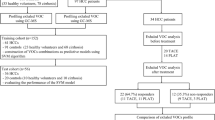
Abstract
In this study, single-lung ventilation was used to detect differences in the volatile organic compound (VOCs) profiles between lung tissues in healthy and affected lungs. In addition, changes that occurred after lung cancer resection in both the VOCs profiles of exhaled breath from ipsilateral and contralateral lungs and the VOCs profiles of exhaled breath and blood sample headspaces were also determined. Eighteen patients with non-small cell carcinoma were enrolled. Alveolar breath samples were taken separately from healthy and diseased lungs before and after the tumor resection. Solid phase microextraction–gas chromatography/mass spectrometry was used to assess the exhaled VOCs of the study participants. The VOCs exhibited significant differences between the contralateral and ipsilateral lungs before surgery, the contralateral and ipsilateral lungs after surgery, the ipsilateral lungs before and after surgery and the blood samples from before and after surgery; 12, 19, 12 and 5 characteristic metabolites played decisive roles in sample classification, respectively. 2,2-Dimethyldecane, tetradecane, 2,2,4,6,6-pentamethylheptane, 2,3,4-trimethyldecane, nonane, 3,4,5,6-tetramethyloctane and hexadecane may be generated from lipid peroxidation during surgery. Caprolactam and propanoic acid may be more promising exhaled breath biomarkers for lung cancer.
Similar content being viewed by others


Introduction
The analysis of volatile organic compounds (VOCs) in exhaled air is a newly developed method for screening and diagnosing diseases. This approach has drawn increasing attention from researchers because of its advantages of convenience, non-invasiveness and good patient tolerance. The analysis of a number of different VOCs in the exhaled breaths of lung cancer (LC) patients has revealed that LC-specific VOCs can be detected not only in the exhaled breaths of these patients but also in the headspaces of blood from LC patients, LC tissues and LC cells1,2,3,4,5,6,7,8,9,10.
In most studies addressing the exhaled breath of LC patients, the exhaled breath samples typically consisted of mixed gas from both lungs (without separating the air from the ipsilateral and contralateral lungs). In addition, sample comparisons were performed between healthy individuals and patients (rather than samples from the same individual) and a few comparisons have been made of the VOC differences between the exhaled breath and the headspace of blood cells2,3,4. As previously established, the optimal method to validate or determine the pathophysiologic pathways of LC VOCs is to compare VOC profiles from different sources (organs or clinical samples) in the same LC patient11. Within this approach, the simplest starting point would be a comparison between VOC profiles collected from the headspace of the LC tumor, the (headspace of) blood samples and the breath samples. In this study, we used a double-lumen endobronchial tube to separate the contralateral and ipsilateral lungs. Using this approach, we sought to perform single-lung ventilation to detect differences in VOC profiles between the lung tissues in healthy and affected lungs. In addition, changes that occurred after LC resection in both the VOC profiles of exhaled breath from ipsilateral and contralateral lungs and the VOC profiles of exhaled breath and blood sample headspaces were determined, enabling the identification of LC-specific VOC profiles of exhaled breath and the explanation of both the pathophysiological pathways involved in the generation of LC VOCs and the characteristics of changes in these VOCs.
Results
In total, 18 LC patients participated in this study, including 13 male patients and 5 female patients. The average age of these patients was 58.67 ± 6.34 years. Using the TNM (tumor, node and metastasis) staging approach, the examined LC cases included 13 cases of stage I LC, 4 cases of stage II LC and 1 case of stage IV LC.
In the corresponding PCA score plot, the exhaled air samples from contralateral and ipsilateral lungs before lung tumor resection could be separated into two different categories (R2X = 0.869 and Q2 = 0.601; Figure 1A). To provide a more detailed explanation, PLSDA was performed. Using three orthogonal components, a prediction model was obtained (R2X = 0.56, R2Y = 0.9 and Q2 = 0.624; Figure 1B). After 100 iterations of permutation testing, the intercept for R2 was 0.458 and the intercept for Q2 was −0.362 (Figure 1C). In the PLSDA model, 12 characteristic metabolites played decisive roles in the sample classification, as indicated by VIP values >1 and P<0.05 in the t-tests (Table 1).

(A): PCA results for exhaled breath samples from contralateral and ipsilateral lungs before lung tumor resection (8 components, R2X = 0.869, Q2 = 0.601). (B): PLSDA results for exhaled breath samples from contralateral and ipsilateral lungs before lung tumor resection (3 components, R2X = 0.56, R2Y = 0.9, Q2 = 0.624). (C): Y-intercepts: R2 = (0.0, 0.458), Q2 = (0.0, −0.362).
In the corresponding PCA score plot, the exhaled air samples from contralateral and ipsilateral lungs after surgery could be separated into two different categories (R2X = 0.692 and Q2 = 0.471; Figure 2A). PLSDA was performed and a prediction model was established (R2X = 0.486, R2Y = 0.952 and Q2 = 0.815; Figure 2B). After 100 iterations of permutation testing, the intercept for R2 was 0.486 and the intercept for Q2 was −0.435 (Figure 2C). In the PLSDA model, there were 19 characteristic metabolites for which the VIP values were >1 and P<0.05 in the t-tests (Table 1).

(A): PCA results for exhaled breath samples from contralateral and ipsilateral lungs after surgery (4 components, R2X = 0.692, Q2 = 0.471). (B): PLSDA results for exhaled breath samples from contralateral and ipsilateral lungs after surgery (3 components, R2X = 0.486, R2Y = 0.952, Q2 = 0.815). (C): Y-intercepts for gas samples from contralateral and ipsilateral lungs after surgery: R2 = (0.0, 0.566), Q2 = (0.0, −0.435).
In the corresponding PCA score plot, there were no significant differences between the preoperative and postoperative exhaled breath samples; thus, the PCA score plot could not be divided into two categories (R2X = 0.729 and Q2 = 0.561). PLSDA was performed and a model was established (R2X = 0.331, R2Y = 0.316 and Q2 = −0.21). These PCA and PLSDA examinations revealed that the exhaled breath profile of the contralateral lung did not change after tumor resection.
In the corresponding PCA score plot, the preoperative and postoperative exhaled breath samples from the ipsilateral lungs could be separated into two different categories (R2X = 0.865 and Q2 = 0.6; Figure 3A). To provide a more detailed explanation, PLSDA was performed, leading to the establishment of a prediction model containing two components (R2X = 0.375, R2Y = 0.818 and Q2 = 0.544; Figure 3B). After 100 iterations of permutation testing, the intercept for R2 was 0.334 and the intercept for Q2 was −0.274 (Figure 3C). The PLSDA model identified 12 characteristic metabolites for which the VIP values were >1 and P<0.05 in the t-tests (Table 1).

(A): PCA results for gas samples from ipsilateral lungs before and after surgery (6 components, R2X = 0.865, Q2 = 0.6). (B): PLSDA results for gas samples from the ipsilateral lungs before and after surgery (2 components, R2X = 0.375, R2Y = 0.818, Q2 = 0.544). (C): Y-intercepts for gas samples from ipsilateral lungs before and after surgery: R2 = (0.0, 0.334), Q2 = (0.0, −0.274).
In the corresponding PCA score plot, R2X was 0.84 and Q2 was 0.414 for the blood samples from before and after surgery (Figure 4A). PLSDA was performed using a single main component. In the prediction model that was obtained, R2X = 0.112, R2Y = 0.715 and Q2 = 0.426 (Figure 4B). In addition, 100 iterations of permutation testing produced an R2 intercept of 0.277 and a Q2 intercept of −0.13 (Figure 4C). The PLSDA model identified five characteristic metabolites for which VIP values were >1 and P<0.05 in the t-tests (Table 2).

(A): PCA results for blood samples from before and after surgery (8 components, R2X = 0.84, Q2 = 0.414). (B): PLSDA results for the blood samples from before and after surgery (1 component, R2X = 0.112, R2Y = 0.715, Q2 = 0.426). (C): Y-intercepts for blood samples from before and after surgery: R2 = (0.0, 0.277), Q2 = (0.0, −0.1–0.13).
Discussion
To the best of our knowledge, Sabine et al. first applied the single-lung ventilation technique for collecting exhaled breath in order to separate exhaled breath from the contralateral and ipsilateral lungs, thereby providing a new method for the more accurate collection of alveolar air12. In this study, we also used the single-lung ventilation technique. However, in contrast with Sabine et al., we directly placed a specially designed gas collection tube on the tracheal bifurcation, thereby enabling the maximal exclusion of dead space gas and ensuring that the collected gas was alveolar gas. Sabine et al. observed the end-tidal carbon dioxide curve and collected exhaled breath at the plateau phase of this curve. Although this approach is currently a more scientific alveolar gas collection method, there are inevitable time deviations in this process: 1) the CO2 waveform is generated by the extraction of exhaled breath by an instrument through a breathing loop; after detection, there is a degree of reaction and the waveform is presented on a screen. This process takes a certain amount of time. In other words, the waves seen are already time delayed; thus, any plateau phase that is observed will have actually begun some time earlier. (2) If gas is collected manually through observation, it is difficult to stop collection at the end of the plateau phase because this procedure only provides several seconds of reaction time. Our gas collection method avoids the aforementioned problems by directly collecting gas at a location that is extremely close to the alveoli, thus providing maximal assurance that the collected gas is alveolar gas. Furthermore, we used a double-lumen endobronchial tube to separate gases from the contralateral and ipsilateral lungs; therefore, the exhaled breath from these two lungs can be collected separately to conduct autologous comparisons.
The comparison between postoperative exhaled breath samples from contralateral and ipsilateral lungs revealed 19 chemicals that differed between these two types of samples (Table 1), whereas a comparison of breath samples from the ipsilateral lung before and after tumor resection detected 11 such substances. From the results of the comparison between contralateral and ipsilateral exhaled breath samples before surgery, the comparison between contralateral and ipsilateral exhaled breath samples after surgery and the comparison of ipsilateral exhaled breath samples from before and after surgery, we speculate that the following alkanes and branched alkanes are produced by processes related to oxidative stress and lipid peroxidation: 2,2-dimethyldecane, tetradecane, 2,2,4,6,6-pentamethylheptane, 2,3,4-trimethyldecane, nonane, 3,4,5,6-tetramethyloctane and hexadecane13. During the surgical procedures of this study, single-lung ventilation was used until the tumor was resected; thus, the ipsilateral lung collapsed, experiencing blood flow but no ventilation or gas exchange, thereby resulting in an imbalanced ventilation/perfusion ratio. When the ipsilateral lung was reventilated with gas (oxygen), ischemia-reperfusion injury occurred; therefore, a large quantity of free radicals was generated, causing lipid peroxidation of unsaturated fatty acids.
The comparison between exhaled air samples from the contralateral and the ipsilateral lung before tumor resection revealed a higher propanoic acid content in the ipsilateral samples than in the contralateral samples; however, this difference did not occur after tumor resection. Therefore, it is speculated that propanoic acid may originate from LC cells and has a derivation that is unrelated to the process of tumor resection.
The elevated propanoic acid levels in the ipsilateral samples that were observed in this study may be associated with inhibition of the propanoic acid metabolic pathway in LC cells. The elevated levels may also be associated with the increased aldehyde dehydrogenase (ALDH) activity in the LC cells. The ALDH family includes the major metabolic enzymes for acetaldehyde and ethanol, which have been extensively studied. There are numerous enzymes in the ALDH family. Many of these enzymes, such as ALDH2, ALDH9A1 and ALDH1B1, are involved in both the propanoic acid and the fatty acid metabolic pathways. Enzymes from the ALDH family play important roles in the metabolism of both endogenous and exogenous ethanol and acetaldehyde.
In a study of the exhaled breaths of cancer patients, Patel et al. demonstrated that elevated levels of ALDH activity were observed in these patients Therefore, these researchers speculated that acetaldehyde and hexanaldehyde could be used as biomarkers for breast cancer14,15. Many in vitro studies of LC cells have demonstrated that the expression of ALDH is upregulated in different LC cells and that aldehydes may be used as biomarkers for LC16,17,18. In this study, no differences in the aldehyde levels in the exhaled air from contralateral and ipsilateral lungs were observed. The function of ALDH is to oxidize acetaldehyde into acetic acid; thus, increased in vivo ALDH activity should be associated with reduced aldehyde levels.
Filipiak et al. revealed that LC cells can release ethers in vitro19. However, in this study, an elevated butyl glycol content was observed both before and after tumor resection, indicating that butyl glycol may not be associated with the tumor or the tumor resection process and that this compound was likely to be an exogenous substance. Butyl glycol is commonly used as a paint or ink solvent, a component of metal cleaning agents and a raw material for dye dispersants; thus, this compound might be an exogenous contaminant.
In our study, a comparison between exhaled breath samples from contralateral and ipsilateral lungs prior to tumor resection revealed a lower caprolactam content in the contralateral samples than in ipsilateral the samples; however, after the tumor surgery, no differences in the caprolactam content between the ipsilateral and contralateral samples were observed. Similarly, a comparison of exhaled breath samples from ipsilateral lungs before and after tumor surgery revealed differences in caprolactam and analyses of the VOCs released by serum samples demonstrated that the caprolactam levels decreased after tumor surgery. These data indicated an association between in vivo caprolactam metabolism and LC. From the results of the current study, LC cells might be able to inhibit caprolactam metabolism, increasing both local and systemic caprolactam contents.
Ethylaniline is present in the stoppers of the airtight bottles used for sample collection. Ulsaker et al. found that GC/MS results may be affected by ethylaniline contamination20. In addition, other studies have demonstrated that ethylaniline levels are elevated among long-term smokers. Therefore, it is possible that changes in ethylaniline that were observed in the exhaled breath analyses of this study were produced by ethylaniline contamination emitted by the rubber stoppers of analysis bottles.
The comparison of exhaled gas samples from ipsilateral lungs before and after tumor resection revealed lower isolongifolene-5-ol levels after surgery than before surgery; in addition, decreases isolongifolene-5-ol levels after tumor resection were observed in the analysis of VOCs emitted by serum samples. However, comparisons of exhaled breath samples from the contralateral and ipsilateral lungs revealed no differences in the isolongifolene-5-ol levels either before or after the surgery, indicating that isolongifolene-5-ol may not be associated with LC cells. Isolongifolene-5-ol is present in tobacco; therefore, decreased in vivo isolongifolene-5-ol concentrations may reflect the normal metabolic processes of smoking patients.
Dimethylphenylcarbinol is an aromatic compound. Seńczuk and Litewka demonstrated that approximately 50% of inhaled cumene is secreted in the urine in the form of dimethylphenylcarbinol21. The comparison of exhaled breath samples from contralateral and ipsilateral lungs before and after tumor surgery did not reveal differences in dimethylphenylcarbinol; therefore, dimethylphenylcarbinol is likely an exogenous substance that is unrelated to LC tumors.
This study did not analyze the diagnostic accuracy of biomarkers for LC in exhaled breath. In addition, stronger conclusions regarding biomarkers in exhaled breaths may be obtained by combining these results with area under the curve (AUC) analyses. Furthermore, based on the results of this study, the molecular biological mechanisms underlying LC require additional study; this investigation represents our next research endeavor.
In conclusion, by combining the use of double-lumen tubes and multivariate data analysis, we can exclude the influence of exogenous substances and individual differences in our assessments of LC biomarkers in exhaled air. It is speculated that certain alkanes and branched alkanes, namely, 2,2-dimethyldecane, tetradecane, 2,2,4,6,6-pentamethylheptane, 2,3,4-trimethyldecane, nonane, 3,4,5,6-tetramethyloctane and hexadecane, are generated from oxidative stress and lipid peroxidation processes. Although many studies suggest that these substances may be used as biomarkers in the exhaled breath of LC patients and that LC cells may also exhibit elevated levels of oxygen radicals, this study demonstrated that the aforementioned alkanes and branched alkanes are likely products of the ischemia-reperfusion process; therefore, their accuracy as biomarkers of LC is debatable. By contrast, caprolactam and propanoic acid may be more promising exhaled breath biomarkers for LC.
Methods
Human subjects
The present experiments were conducted in accordance with the Declaration of Helsinki. The protocol in this study was approved by the Ethics Committee at Harbin Medical University (No.201314) and written informed consent was obtained from the patients prior to the study enrollment. Eighteen patients who underwent thoracotomy and tumour resection at the First Affiliated Hospital of Harbin Medical University between April 2011 and September 2012 were selected as study subjects. The surgery and anesthesia for this group of patients were performed by the same group of doctors. All of the selected patients had a history of smoking. These 18 patients all suffered from non-small cell carcinoma, including 13 cases of adenocarcinoma, 4 cases of squamous cell carcinoma and 1 case of adenosquamous carcinoma.
The collection of exhaled breath:
Gas samples from the ipsilateral and contralateral lungs were collected before and after tumor resection. Before the gas sample collection, a fiberoptic bronchoscopy was performed to measure the distance between the opening of the double-lumen tube and the tracheal bifurcation. Based on the results of this bronchoscopy, a specially designed sample collection tube (made of Teflon) was inserted through a tracheal tube and placed on the tracheal bifurcation (Figure 5). In total, 2 ml of gas was drawn using a 50-ml gastight syringe (Agilent, PN 5190-147, Agilent Technologies Inc., Australia) and then ejected to remove the gas that was originally in the sample collection tube. Subsequently, 10 ml of gas was collected and injected into an airtight vial (Agilent Technologies Inc., Australia) to ensure that the collected gas was unilateral alveolar gas. All vials were thoroughly flushed and cleaned with nitrogen gas (purity of 99.999%, Liming Gas Inc., China) before being evacuated for breath sampling to remove any residual contaminants3 All gas samples were processed within 3 h of collection.

Aschematic diagram of gas collection from a single lung (This diagram was drawn by CS.W).
The collection of blood samples:
Peripheral veins were opened and 2 ml of venous blood was collected from the patients at the start of surgery and after tumor resection. After collection, the blood samples were stored in 20-ml airtight vials (Agilent Technologies Inc., Australia) and immediately sent to a laboratory for analysis.
Solid-phase microextraction (SPME) procedure
A manual SPME holder with 75-μm-thick carboxen/polydimethylsiloxane fibers was purchased from Supelco (Bellefonte, USA). The SPME fiber was inserted into the vial and exposed to the gaseous sample or the headspace of the blood sample for 20 min at 40°C. Subsequently, the desorption of volatiles occurred in the hot GC injector at 200°C for 2 min.
GC/MS analysis
All samples were subjected to gas chromatography (GC)/mass spectrometry (MS) analysis (GCMS-QP2010, Shimadzu, Japan). The following GC conditions were employed: an A DB-5MS (30 m length × 0.250 internal diameter (ID) × 0.25 µm film thickness) (Agilent Technologies, USA) plot column was used and high-purity helium (≥99.999%) was used as the carrier gas with a flow rate of 2.0 ml/min. A splitless injector was employed with an inlet temperature of 200°C. The column temperature was 40°C. The temperature was increased in accordance with the following program: the initial temperature of 40°C was maintained for 2 min; the temperature was increased to 200°C at a speed of 7°C/min and maintained at this temperature for 1 min; and finally, the temperature was increased to 230°C at a speed of 20°C/min and maintained for 3 min. The MS conditions included a 70-eV ionization voltage and a 300°C ion source temperature. The MS was conducted in full scan mode and the mass-to-charge ratio (m/z) was 35-200.
Extraction and pretreatment of GC/MS raw data
Raw GC/MS data were converted into CDF format (NetCDF) files and subsequently processed by the XCMS toolbox. The XCMS parameters were the default settings, with the following exceptions: xcmsSet (fwhm = 8, snthresh = 6 and max = 200), retcor (method = “linear”, family = “gaussian” and plottype = “mdevden”) and a bandwidth of 8 for the first grouping command and 4 for the second grouping command22,23.
Statistical analysis
Normalized data were exported to SIMCA-p 11.5 for principal component analysis (PCA) partial least-squares discriminant analysis (PLSDA) and orthogonal partial least-squares discriminant analysis (OPLSDA). To guard against overfitting, the default seven-round cross-validation in the SIMCA-p software was applied and permutation tests with 100 iterations were performed to further validate the supervised model. In addition, the nonparametric Kruskal-Wallis rank sum test was performed for each metabolite and the corresponding false discovery rate (FDR) based on p-values was calculated to correct for multiple comparisons. Based on variable importance in the projection (VIP) values calculated from the OPLSDA model and FDR values, potential metabolic biomarkers were selected using thresholds of 1.0 and 0.01, respectively.
References
Phillips, M. et al. Volatile organic compounds in breath as markers of lung cancer: a cross-sectional study. Lancet. 353, 1930–1933 (1999).
Phillips, M. et al. Detection of lung cancer with volatile markers in the breath. Chest. 123, 2115–2123 (2003).
Bajtarevic, A. et al. Noninvasive detection of lung cancer by analysis of exhaled breath. BMC. Cancer. 9, 348–363 (2009).
Deng, C. et al. Investigation of volatile biomarkers in lung cancer blood using solid-phase microextraction and capillary gas chromatography-mass spectrometry. J. Chromatogr. B. Analyt. Technol. Biomed. Life. Sci. 808, 269–277 (2004).
Broza, Y. et al. A nanomaterial-based breath test for short-term follow-up after lung tumor surgery. Nanomedicine. 9, 15–21 (2013).
Barash, O. et al. Classification of lung cancer histology by gold nanoparticle sensors. Nanomedicine. 8, 580–589 (2012).
Chen, X. et al. A study of the volatile organic compounds exhaled by lung cancer cells in vitro for breath diagnosis. Cancer. 110, 835–844 (2007).
Filipiak, W. et al. Release of volatile organic compounds (VOCs) from the lung cancer cell line CALU-1 in vitro. Cancer. Cell. Int. 8, 17 (2008).
Sponring, A. et al. Release of volatile organic compounds from the lung cancer cell line NCI-H2087 in vitro. Anticancer. Res. 29, 419–426 (2009).
Mazzone, P. et al. Exhaled breath analysis with a colorimetric sensor array for the identification and characterization of lung cancer. J. Thorac. Oncol. 7, 137–142 (2012).
Hakim, M. et al. Volatile organic compounds of lung cancer and possible biochemical pathways. Chem. Rev. 112, 5949–5966 (2012).
Kischkel, S. et al. Breath analysis during one-lung ventilation in cancer patients. Eur. Respir. J. 40, 706–713 (2012).
Wang, Y. et al. The analysis of volatile organic compounds biomarkers for lung cancer in exhaled breath, tissues and cell lines. Cancer. Biomark. 11, 129–137 (2012).
Patel, M. et al. ALDH1A1 and ALDH3A1 expression in lung cancers: correlation with histologic type and potential precursors. Lung. Cancer. 59, 340–349 (2008).
Sponring, A. et al. Release of Volatile Organic Compounds from the Lung Cancer Cell Line NCI-H2087 In Vitro. Anticancer. Res. 29, 419–426 (2009).
Shin, H. et al. Acetaldehyde and hexanaldehyde from cultured white cells. J. Transl. Med. 7, 31–42 (2009).
Filipiak, W. et al. Release of volatile organic compounds (VOCs) from the lung cancer cell line CALU-1 in vitro. Cancer. Cell. Int. 8, 17–28 (2008).
Xue, R. et al. Investigation of volatile biomarkers in liver cancer blood using solid-phase microextraction and gas chromatography/mass spectrometry. Rapid. Commun. Mass. Spectrom. 22, 1181–1186 (2008).
Filipiak, W. et al. TD-GC-MS Analysis of Volatile Metabolites of Human Lung Cancer and Normal Cells In vitro. Cancer. Epidemiol. Biomarkers. Prev. 19, 182–195 (2010).
Ulsaker, G. et al. Gas chromatographic - mass spectrometric analysis of polyethylene bottle packed intravenous solutions contaminated with N-ethylaniline from the rubber part of the two-component closure. Analyst. 104, 580–582 (1979).
Seńczuk, W. et al. Absorption of cumene through the respiratory tract and excretion of dimethylphenylcarbinol in urine. Br. J. Ind. Med. 33, 100–105 (1976).
Gao, X. et al. Metabolite analysis of human fecal water by gas chromatography/mass spectrometry with ethyl chloroformate derivatization. Anal. Biochem. 393, 163–175 (2009).
Trygg, J. et al. Chemometrics in metabonomics. J. Proteome. Res. 6, 469–479 (2007).
Acknowledgements
Supported by grants from the National Natural Science Foundation of China (No. 81402462), the China Postdoctoral Science Foundation (No. 2013M531069), Foundation of Heilongjiang Educational Committee (No. 12531245) and Doctoral Fund of the First Affiliated Hospital of Harbin Medical University (No. 2012B006).
Author information
Authors and Affiliations
Contributions
C.W., E.L. and G.X. conceived and designed the research; C.W., R.D. and A.L. wrote the manuscript. X.W., C.C., L.G., S.L. and W.Z. performed the experiments; K.C. analyzed the experimental data. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article's Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder in order to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Wang, C., Dong, R., Wang, X. et al. Exhaled volatile organic compounds as lung cancer biomarkers during one-lung ventilation. Sci Rep 4, 7312 (2014). https://doi.org/10.1038/srep07312
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep07312
This article is cited by
-
Volatolomics in healthcare and its advanced detection technology
Nano Research (2022)
-
Modification of an atmospheric pressure photoionization source for online analysis of exhaled breath coupled with quadrupole time-of-flight mass spectrometry
Analytical and Bioanalytical Chemistry (2020)
-
Emerging coronavirus diseases and future perspectives
VirusDisease (2020)
-
Human beings as islands of stability: Monitoring body states using breath profiles
Scientific Reports (2019)
-
Machine learning for the meta-analyses of microbial pathogens’ volatile signatures
Scientific Reports (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
