
Abstract
Fibers remain undigested until they reach the colon, where some are fermented by gut microbiota, producing metabolites called short-chain fatty acids (SCFAs), such as acetate and butyrate1. SCFAs lower blood pressure in experimental models2,3,4,5, but their translational potential is unknown. Here we present the results of a phase II, randomized, placebo-controlled, double-blind cross-over trial (Australian New Zealand Clinical Trials Registry ACTRN12619000916145) using prebiotic acetylated and butyrylated high-amylose maize starch (HAMSAB) supplementation6. Twenty treatment-naive participants with hypertension were randomized to 40 g per day of HAMSAB or placebo, completing each arm for 3 weeks, with a 3-week washout period between them. The primary endpoint was a reduction in ambulatory systolic blood pressure. Secondary endpoints included changes to circulating cytokines, immune markers and gut microbiome modulation. Patients receiving the HAMSAB treatment showed a clinically relevant reduction in 24-hour systolic blood pressure independent of age, sex and body mass index without any adverse effects. HAMSAB increased levels of acetate and butyrate, shifted the microbial ecosystem and expanded the prevalence of SCFA producers. In summary, a prebiotic intervention with HAMSAB could represent a promising option to deliver SCFAs and lower blood pressure in patients with essential hypertension.
Similar content being viewed by others


Main
Uncontrolled high blood pressure (BP), also known as hypertension, is the primary cause of non-communicable diseases and global deaths7. It is estimated that over 1 billion people worldwide have hypertension8. The overwhelming majority of patients with hypertension remain with uncontrolled or suboptimal BP9, which leads to cardiovascular disease (CVD)7. Western-style diets, which are low in fiber and high in saturated fats and sodium, raise the risk of developing hypertension and CVD10. Conversely, those with a high intake of fruits and vegetables have lower BP11. A recent systematic review and meta-analysis assessed the health impact of dietary fiber intake in 185 prospective studies and 58 clinical trials12. Increased fiber intake, especially between 25 g and 29 g per day, led to a 15–30% reduction in all-cause and cardiovascular mortality and was associated with lower BP12.
Mounting evidence supports that gut dysbiosis is a common feature and contributor to experimental and clinical hypertension13,14. Dietary fiber is defined as a carbohydrate that is not absorbed nor digested in the small intestine, thus reaching the large intestine undigested15. Specific types of fiber are fermented by the gut microbiota, which produce metabolites called short-chain fatty acids (SCFAs), predominantly acetate, butyrate and propionate1. These are energy sources for intestinal epithelial cells16. Using experimental models, we discovered that the beneficial effects of dietary fiber to lowering BP and preventing CVD are due to SCFAs2. These findings were subsequently validated in further experimental models3,4,5, with acetate and butyrate having the most pronounced effects, lowering BP by 35% and 20%, respectively5. Secondary analysis of the SPIRIT trial supports these findings, with hypertensive fecal and plasma butyrate levels inversely correlated with systolic blood pressure (SBP)17. However, there is no causal evidence that SCFAs may lower BP in patients with hypertension. A considerable challenge in translating these findings has been the sustained delivery of SCFAs over a long period18.
We hypothesized that increased production of gut microbiota-derived metabolites acetate and butyrate reduce BP in untreated patients with hypertension. To overcome the challenge of delivering these SCFAs to the systemic circulation, we used high-amylose maize starch (HAMS), a type of resistant starch II that can be acetylated (HAMSA) and butyrylated (HAMSB)19. Intestinal microbial fermentation of HAMSAB releases high levels of acetate and butyrate in the colon, which are subsequently absorbed and delivered to the systemic circulation20. Importantly, the levels of acetate and butyrate delivered by HAMSAB are significantly higher than achieved with non-acetylated and non-butyrylated HAMS alone20. Thus, we aimed to conduct a randomized clinical trial to determine if delivery of HAMSAB lowers BP in untreated patients with hypertension. Although we cannot exclude other secondary effects due to the higher content and different composition of dietary fibers in HAMSAB compared to the control diet, we provide evidence that the SCFAs acetate and butyrate, delivered as HAMSAB, lower SBP in humans and could be employed as a new BP-lowering strategy.
Results
Participant characteristics
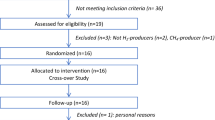
Recruitment started in July 2019 and finished in September 2021. Between 9 July 2019 and 28 August 2021, we received 157 expressions of interest and screened 31 participants. Of these, 21 were randomized to either the SCFA-enriched diet (HAMSAB) or placebo (Fig. 1). Therefore, 20 participants completed the trial. Due to the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic, recruitment was challenging and took longer than expected. As a result, the study stopped at the end of the allocated budget and staffing time. Thus, we stopped the trial at 21 participants recruited, with one dropout who started the trial on the Diet B (placebo) arm and whose BP reached >165/100 mmHg, requiring medication (Fig. 1). Therefore, although we used a 1:1 randomization, more participants were first allocated to Diet A than Diet B, and the calculated sample size was not reached.

This study attracted 143 expressions of interest. Thirty-one individuals met the inclusion criteria and were screened, and, of these, 20 successfully completed the trial.
Baseline characteristics of the participants, including age, body mass index (BMI), biochemical profile and BP, are shown in Extended Data Table 1. The baseline mean ± s.d. 24-hour SBP was 136 ± 6 mmHg, and diastolic blood pressure (DBP) was 87 ± 7 mmHg. Participants randomized to either the placebo or HAMSAB first had no significant differences in age, sex, BMI, office and 24-hour BP and biochemical profiles. However, participants randomized into the placebo arm had higher baseline non-high-density lipoprotein (HDL) cholesterol (P = 0.02) and low-density lipoprotein (LDL) cholesterol (P = 0.04) and triglycerides (P = 0.03) (Extended Data Table 2). This resulted in an observed increase in LDL and non-HDL cholesterol and triglycerides with HAMSAB compared to its baseline (Extended Data Table 3), as there was no difference between placebo and HAMSAB arms. Compared to baseline measurements, biochemical parameters remained unchanged in the placebo arm of the study, whereas there was a reduction in bilirubin in the HAMSAB arm (Extended Data Table 3). All other parameters tested remained unchanged, including BMI (Extended Data Table 3).
Dietary adherence and gastrointestinal tolerance
HAMSAB and placebo diets were matched in macronutrient content, including protein, fat and carbohydrates (Extended Data Table 4). The only difference was in overall dietary fiber (placebo 4.6 g versus HAMSAB 19.7 g) and resistant starch content (placebo 0.4 g versus HAMSAB 15.8 g). The HAMSAB and placebo diets were well tolerated, with participants consuming 93% of the meals provided. Analysis of food diaries showed that there was no difference in nutritional intake, specifically protein, total fat, sodium and potassium, between visits (Extended Data Table 5). The only difference observed was an increase in fiber (+40%, P = 0.0003) and resistant starch (+566%, P < 0.0001) between baseline and HAMSAB (Extended Data Table 5), as expected. Participants in the HAMSAB arm scored higher for abdominal pain (P = 0.024), whereras, in the placebo arm, they scored lower symptoms of bloating (P = 0.022) on the Visual Analogue Scale (VAS) (Extended Data Table 6).
BP
We observed no differences in SBP in the placebo arm (Table 1 and Extended Data Table 3). In the HAMSAB arm, we observed a significant decrease in 24-hour SBP (baseline-to-HAMSAB: P = 0.03; Table 1), with a placebo-subtracted mean difference of –6.1 mmHg (95% confidence interval (CI): –1.4 to –10.7 mmHg, P < 0.0001; Fig. 2a,b). We validated these using a generalized linear model (GLM), adjusted for sex, BMI, age and study arm, with baseline-to-HAMSAB having a decrease of 4.1 mmHg (P = 0.027). In comparison, baseline-to-placebo had no difference (+2 mmHg, P = 0.176). We also observed a significant decrease in both day and night SBP (respective placebo-subtracted mean difference: –6.4 mmHg (95% CI: –0.7 to –12.2 mmHg), P = 0.01; –6.32 mmHg (–1.1 to –10.3 mmHg), P = 0.02; Extended Data Table 3) and central 24-hour SBP (placebo-subtracted mean difference: –7.3 mmHg (–1.6 to –16.2 mmHg), P = 0.005; Table 1). We then examined changes to 24-hour DBP and observed no statistically significant change with HAMSAB (baseline-to-HAMSAB difference: P = 0.23; Table 1 and Extended Data Table 3), with a placebo-subtracted mean difference of –1.7 mmHg (P = 0.179; Fig. 2c,d). In the placebo group, there was an increase in 24-hour DBP (+3.84 mmHg, P < 0.0001; Table 1). Interestingly, we did not observe a change in stroke volume, cardiac output or heart rate; however, HAMSAB significantly reduced total vascular resistance (P = 0.049; Table 1). However, we acknowledge that these parameters are calculated and strongly BP dependent.

Individual changes in 24-hour SBP (a) and mean change in 24-hour SBP (b) between placebo and HAMSAB and placebo-subtracted mean difference. Individual change in 24-hour DBP (c) and mean change in 24-hour DBP (d) between placebo and HAMSAB and placebo-subtracted mean difference. Plasma concentrations of acetic acid (e), butyric acid (f) and combined total acetic acid and butyric acid (g). n = 20 per treatment group. Error bars represent ± s.e.m. Showing results of two-tailed paired t-test and estimation plots.
We did not observe a change in office SBP or DBP (Table 1). However, similarly to ambulatory blood pressure monitoring (ABPM), home SBP decreased over the 21-day intervention with the HAMSAB diet, particularly around day 9 and day 14 after the intervention started (Extended Data Fig. 1a). Participants on the HAMSAB diet achieved a –4.6-mmHg reduction in SBP when we compared the first 3 days of the intervention to the last 3 days (P = 0.117; Extended Data Fig. 1b). Moreover, when we compared the first 3 days to day 14, SBP dropped by –4.8 mmHg (P = 0.029; Extended Data Fig. 1c). Conversely, participants on the placebo had no difference in SBP through the intervention (Extended Data Fig. 1d,e). Overall, the placebo-subtracted mean difference in home SBP was –1.48 mmHg (P = 0.001; Extended Data Fig. 1g). Participants on the HAMSAB diet also had a modest non-significant drop in DBP (Extended Data Fig. 1h,i) with a –2.4-mmHg decrease at day 14 (P = 0.055) and no change in home DBP in the placebo arm (Extended Data Fig. 1k–m). The placebo-subtracted mean difference in home DBP was –0.79 mmHg (P = 0.0295; Extended Data Fig. 1n). Together, these data support that HAMSAB successfully reduced 24-hour and home SBP. A larger number of participants may be needed to achieve statistical significance in DBP changes.
Plasma SCFAs
Compared to the placebo intervention, HAMSAB increased circulating acetate by 1.8-fold, but it did not reach statistical significance (P = 0.076; Fig. 2e). This may be explained by the bloods being collected more than 12 hours after the last HAMSAB meal. HAMSAB significantly increased the levels of butyrate 14-fold (P = 0.0178; Fig. 2f) as well as the combined plasma levels of acetate and butyrate by 7.8-fold compared to the placebo (P = 0.0156; Fig. 2g). There was no change in the levels of the other major SCFA, propionate (Extended Data Fig. 2a). These data confirm that HAMSAB delivers systemically high levels of the SCFAs acetate and butyrate.
Gastrointestinal pH and transit
We characterized the whole gastrointestinal transit and pH using real-time tracking in a subset of the cohort. We found no significant differences in regional transit times when comparing baseline, HAMSAB and placebo diet (Extended Data Fig. 3a–d). The colon is susceptible to changes in pH due to microbial communities releasing acidic metabolic byproducts, such as SCFAs, thus providing an in vivo quantification of SCFAs. Given that HAMSAB delivers high levels of SCFAs, we wanted to determine if this would be reflected in colonic pH. We observed no difference in colonic minimum and median pH (Extended Data Fig. 3e,f). However, there was a significant decrease in maximum colonic pH on the HAMSAB diet compared to baseline (Extended Data Fig. 3g), with a significant reduction in the baseline-subtracted mean difference in pH in the HAMSAB arm (–0.45, P = 0.033; Extended Data Fig. 3h).
Fecal microbiome
We first compared the baseline fecal microbiome before starting the trial and after the 3-week washout period. We observed no significant difference in microbial α-diversity (Chao1, P = 0.594; observed species, P = 0.594; Shannon, P = 0.870) and β-diversity (Bray–Curtis index, P = 0.952) (Fig. 3a,b). These data suggest that the restoration of baseline microbiota was achieved during the washout period. Next, we compared the fecal microbiota composition of the HAMSAB diet and placebo. HAMSAB supplementation significantly decreased species richness (Chao1, P = 0.009; observed species, P = 0.009) but not evenness (Shannon, P = 0.117) (Fig. 3c). There was no difference between the microbiome at baseline and after the placebo arm (Extended Data Fig. 2b). Moreover, 3 weeks on the HAMSAB diet was sufficient to shift the β-diversity (Bray–Curtis index, P = 0.037; Fig. 3d). HAMSAB significantly increased the relative abundance of six taxonomic features (Extended Data Table 7), including two SCFA producers, Parabacteroides distasonis (log2 fold change (FC) = 2.8, false discovery rate (FDR) q = 0.003) and Ruminococcus gauvreauii (log2FC = 3.5, FDR q = 0.0029), compared to placebo (Fig. 3e,f). These species were present in 94% and 77% of the participants after the HAMSAB arm and were significantly reduced after the washout period in participants who were randomized into the HAMSAB arm first (Extended Data Fig. 2c–f). These findings support that HAMSAB treatment fosters the expansion of microbes that produce SCFAs in conjunction with releasing high levels of the pre-conjugated acetate and butyrate.

16S rRNA sequences were obtained from fecal samples and analyzed using QIIME2. a, Chao1, observed and Shannon α-diversity indices were analyzed using MicrobiomeAnalyst software comparing the first and second baselines (n = 40 samples, two-tailed paired t-test). b, Principal coordinate analysis (PCoA) plot showing weighted Bray–Curtis index at baseline of participants randomized to HAMSAB or placebo diet (n = 40 samples). c, Chao1, observed and Shannon α-diversity indices comparing HAMSAB and placebo diet (n = 39 samples, two-tailed paired t-test). d, PCoA plot showing β-diversity measured by Bray–Curtis index of baselines of participants after HAMSAB or placebo diet (n = 39 samples). Filtered count and log-transformed count showing relative abundances of P. distasonis (e) and R. gauvreauii (f) (n = 39 samples) (edgeR analysis). Box plots in a, c, e and f show the median and interquartile range of each group. Shaded ellipsis in PCoA plots represent the 95% CI for each group.
Plasma cytokines
SCFAs are thought to have anti-inflammatory properties16, whereas hypertension is associated with increased pro-inflammatory markers, including IL17A, IL1β and IL6, and reduced anti-inflammatory marker IL1021. Thus, we used a highly sensitive immunoassay to quantify the levels of plasma IL17A, IL1β, IL10 and IL6 between the HAMSAB and placebo treatment groups. We found no statistically significant difference in these cytokines (IL10: P = 0.29, IL6: P = 0.51, Il1β: P = 0.46, IL17A: P = 0.11; Extended Data Fig. 2g–j), suggesting that 3 weeks on the HAMSAB intervention did not impact plasma cytokine levels.
Discussion
Adequate BP control remains poorly achieved globally, contributing to the rise in cardiovascular death8. In recent years, SCFAs have emerged as potential therapeutic agents to treat hypertension in experimental models2,5. We investigated if a 3-week intervention with HAMSAB, a specialized high-fiber supplement delivering high quantities of the SCFAs acetate and butyrate, can lower BP in untreated hypertensive patients. We provide clinical evidence that delivering SCFAs lowers home, 24-hour and central SBP in patients with essential hypertension, independently of sex, age and BMI. HAMSAB diet also modulated the fecal microbiome, increasing SCFA producers and raising SCFA levels in the systemic circulation. As a result, this proof-of-concept study demonstrates the feasibility of employing supplementation to deliver high doses of microbial-derived metabolites to lower BP in essential hypertension. The reduction in SBP observed was equivalent to that achieved with conventional anti-hypertensive mono-treatment22 and is calculated to reduce coronary death by 9% and stroke death by 14%23.
SCFAs are metabolites produced by commensal gut microbiota1. These metabolites can be absorbed into the bloodstream and affect the host’s physiology16. Current evidence suggests that SCFAs orchestrate several complex signaling pathways that alter systemic transcriptional regulation2 and activate SCFA receptors, such as GPR435. In experimental models, these culminate in reduced inflammation, lower BP and prevention of hypertensive-induced end organ damage2,5. Recent clinical evidence suggests that the prevalence of hypertension is inversely associated with fecal and plasma butyrate levels17. Our findings add to this by showing that HAMSAB increases levels of acetate and butyrate in the plasma and that they indeed have BP-lowering effects in humans. This effect was larger than that reported for dietary fiber interventions alone12. This finding is important because hypertension is associated with decreased circulating SCFAs24 and reduced SCFA-sensing receptor GPR43 mRNA25. Although we did not measure SCFA levels in the feces, our data from in vivo real-time monitoring using the SmartPill supports that HAMSAB reduced the maximum pH in the colon. This is reflective of the distal colon and suggests an increase in fermentation of dietary fiber in this area, where carbohydrate fermentation rates are usually low due to depletion of fibrous substrates.
Increasing evidence supports the role of the gut microbiome in BP regulation13. Dysbiosis, or functional and compositional abnormalities in the gut microbiota, have been described in clinical and experimental hypertension2,5,13,24,25. Evidence supports that the hypertensive gut microbiota has a depletion of SCFA-producing bacteria24,25. Subsequently, this depletion may impair SCFA-dependent pathways necessary for adequate BP control. Intervention with HAMSAB supported the expansion of SCFA-producing commensal microbes P. distasonis and R. gauvreauii and supported the restoration of local production of SCFAs by these microbes. Belonging to the Lachnospiraceae family, decreased abundance of R. gauvreauii is associated with lower levels of SCFAs and poorer cardiovascular outcomes26,27. Ruminococcus sp. has a lower prevalence in untreated patients with hypertension25 and heart failure28 and is negatively associated with 24-hour SBP25. Similarly, P. distasonis is commensal bacteria that metabolizes carbohydrates in the colon and mediates local inflammation29. Parabacteroides genus is considered a member of the 20 core microbes in the human gut30. P. distasonis ferments dietary oligosaccharides to produce acetate and propionate31. Our findings suggest that HAMSAB modulated SBP by increasing SCFA production and prevalence of SCFA producers, such as Ruminococcus sp. and Parabacteroides sp. Further studies are needed to determine if these taxa are required for the SBP-lowering effect that we observed.
Contrary to our hypothesis, we did not observe a reduction in cytokines with HAMSAB intake. These findings are consistent with 5-day and 21-day high-fiber interventions, which did not change the frequencies of T cells in healthy participants18,32. However, although of borderline significance, HAMSAB reduced another well-known factor that regulates BP: total peripheral resistance. This is consistent with findings in experimental hypertension5. Vascular tone is an essential contributor to total vascular resistance. Early studies in rat and human arteries showed that acetate and butyrate have a non-specific vasorelaxation effect33,34. The mechanism was independent of traditional BP-lowering effects, including endothelial and sympathetic activation33,34. Given the large quantities of acetate and butyrate delivered through HAMSAB, it is possible that these metabolites influence vascular tone, resulting in lower total peripheral resistance. Further studies are needed to determine the specific mechanisms involved.
The main limitations of our study are the small sample size, lack of long-term follow-up and the differences in dietary fiber content between treated and control groups. To adequately conclude the benefits of supplementary delivery of SCFAS to control BP, larger and longer-term trials need to be conducted. Moreover, a non-acetylated and non-butyrylated HAMS should be added as an additional control diet. Although our study detected significant changes in SBP, a larger sample size could yield more conclusive results for other variables, such as DBP. However, recruiting untreated patients with hypertension during the pandemic was a substantial barrier, as most appointments were being carried out via telehealth, where BP was not measured. Moreover, given the differences in fiber content between HAMSAB and control diet, we cannot exclude that the higher amount of resistant starches delivered as HAMSAB could alter BP via microbiota/SCFA-independent pathways, which are yet to be described. Our trial also had strengths, including the cross-over design, the double-blinding (which is rare in dietary studies), the use of HAMSAB to deliver high levels of SCFAs and the use of ABPM and home BP monitoring.
In conclusion, our study provides evidence that delivering high levels of the microbial metabolites acetate and butyrate reduces SBP and total vascular resistance in patients with essential hypertension. Furthermore, HAMSAB enriched essential SCFA-producing microbes, which compounds the overall levels of SCFAs. Consumption of SCFAs directly, via the use of HAMSAB or other strategies, may represent a therapeutic option for patients with hypertension.
Methods
Study design
Human ethics approval was obtained from the Monash University Human Research Ethics Committee (study ID: 19203). The study was registered at the Australian New Zealand Clinical Trials Registry (ACTRN12619000916145) and followed the Declaration of Helsinki. All participants provided written informed consent before commencing the trial. A detailed protocol on the rationale and study design was previously published6. In brief, this study was a double-blind, randomized, placebo-controlled cross-over trial conducted in Melbourne, Australia, at Monash University within the Alfred Research Alliance.
Participants
Participants were recruited through printed advertisements on notice boards, social media, tabloid print media or direct e-mails from a database of participants who approved to be contacted for trial consideration. Untreated individuals with hypertension were recruited by the study coordinator and screened for eligibility before being randomized. Inclusion criteria included being untreated for hypertension (as defined by the Australian National Heart Foundation guidelines, determined during the first study visit with 24-hour SBP ≥ 130 mmHg and/or 24-hour DBP ≥ 80 mmHg), being of either sex (self-reported), 18–70 years of age and having a BMI of 18.5–35 kg/m2. Exclusion criteria included any anti-hypertensive medication, an office BP measurement >165/100 mmHg, antibiotic treatment in the last 3 months or probiotic intake over the previous 6 weeks. Those presenting with comorbidities (including type 1 or type 2 diabetes or any gastrointestinal disease), pregnancy or specific dietary requirements (for example, plant-based, gluten-free) or food intolerances were also excluded.
Randomization and masking
Study participants were randomized and stratified using REDCap software (version 9.1.0) in a 1:1 ratio based on age, BMI and sex using a custom randomization list; the randomization on REDCap was automated once the study coordinator entered their age, BMI and sex. This study was double-blinded; concealment of the allocated diet was labeling all food and material related to the trial, including randomization outcome, as ‘Diet A’ and ‘Diet B’. The study coordinator was unblinded only after the trial was completed, when the analysis of the data was completed by the other researchers.
HAMSAB
Our study used a modified version of HAMS, a type 2 resistant starch, which is considered highly fermentable by the gut microbiota, leading to the release of SCFAs15. This supplement underwent further modification through esterification of the SCFAs acetate and butyrate (HAMSAB). This ensured the targeted delivery and release of high levels of acetate and butyrate in the large intestines and systemic circulation20,35 and further fermentation of the residual HAMS in the colon35.
Intervention
We worked with a research chef and dieticians to develop a suite of foods (described in ref. 6) with similar appearance and taste that could be frozen and reheated and contained the placebo or HAMSAB. After successful screening and randomization, participants were assigned to Diet A or Diet B for 3 weeks. Diet A contained HAMSAB (obtained from Ingredion) delivered as 40 g per day divided into two portions of 20 g in the morning meal and 20 g in the evening meal, and Diet B contained 40 g per day of placebo (corn starch or regular flour with no added resistant starches) delivered in a similar manner for 3 weeks. All other nutritional components (including energy, fat and protein) were the same. A complete breakdown of the nutritional content of the diets is given in Extended Data Tables 4 and 5. The 3-week intervention was chosen based on a previously published paper5. After a 3-week washout period, participants were placed on the opposite arm for 3 weeks. All study food was stored in a –20 °C freezer at Monash University. Participants were provided with a list of foods that were naturally high in resistant starches and SCFAs and were instructed to avoid them for the duration of the study. All participants were required to document dietary intake in a 3-day food diary immediately before commencement and at the end of each arm of the study for assessment of their habitual diet and in a daily food diary for the consumption of study meals for the duration of the study. Food diaries were then analyzed for changes in dietary intake using FoodWorks Professional software (version 7.01, Xyris) and resistant starch using an in-house database built into FoodWorks (J.M.). Adherence to the study diets was assessed as excellent using previously published criteria36.
BP measurements
An average of three office BP measurements were taken by the trial coordinator using standard protocol under resting conditions (>5-minute sitting with the researcher not in the room, seated, with back supported and arms and legs uncrossed) using an automated digital BP monitor (Omron Healthcare, HEM-907). Participants were given a demonstration and detailed instructions following the Australian National Heart Foundation guidelines on performing at-home BP monitoring using a calibrated and STRIDE-approved BP monitor (Omron Healthcare, HEM-7121). Participants were instructed to take consecutive two measurements at the same time each day under rested conditions for the duration of the study. Participants were also fitted with an ambulatory blood pressure monitor (Mobil-O-Graph BP device, IEM) before and after the 3-week dietary intervention, in a total of four visits. These devices measured BP every 15 minutes during the day and every 30 minutes at night. These measurements were used to confirm the office hypertensive diagnosis before enrollment in the trial. Participants were instructed to maintain a regular schedule and document any factors that may influence their BP readings (for example, change in medication, stress or illness, bed time).
Gastrointestinal transit and pH
Regional gastrointestinal transit times and pH were measured using the SmartPill Motility Testing System (Medtronic), as previously described37. This was implemented later in the trial and, thus, was performed in only a subset of participants (n = 7 baseline, placebo and HAMSAB). After collecting blood samples, fasting participants were asked to eat a SmartBar and then swallow the SmartPill capsule (Medtronic), according to the manufacturer’s protocol. This allows real-time measurement, transmitted wirelessly to a wearable data receiver, of intraluminal pH through the whole gastrointestinal tract as well as assessment of gastrointestinal transit. Participants fasted for 6 hours before resuming normal food and drink. Additionally, they had to always keep the receiver within 1.5 m of the body until the SmartPill capsule was passed. Data were then downloaded from the receiver on the SmartPill Motility Program and analyzed for gastric emptying and small intestinal, colonic and whole gut transit time independently by two trained investigators (D.R.-J. and C.K.Y.). Any discrepancies were resolved via discussion and consensus between the two. As microbial fermentative activities differ across the different colonic regions, colonic pH profiles were further defined using median, minimum and maximum pH, using a previous protocol37.
SCFA measurements
Fasting blood was collected in the morning, at least 12 hours after the last HAMSAB or placebo meal. Plasma SCFAs were quantified using mass spectrometry, as previously described38. In brief, 20 µl of plasma was analyzed in duplicates in a Q-Exactive Orbitrap mass spectrometer (Thermo Fisher Scientific) in conjunction with a Dionex UltiMate 3000 RS high-performance liquid chromatography (HPLC) system (Thermo Fisher Scientific). We accepted a coefficient of variability <15%. Standard curves were constructed using the area ratio of the target analyte, and the internal standard in the range of each analyte was used. The levels of butyrate in some samples were below detection level of the standard curve; in this case, they were considered half of the lowest measurable value, equivalent to 0.05 ng ml−1.
Fecal DNA extraction and 16S sequencing
Our study followed guidelines for fecal microbiota studies in hypertension39 and the Strengthening The Organization and Reporting of Microbiome Studies (STORMS) reporting40. Stool samples were collected in tubes containing DNA/RNA Shield (Zymo Research) for microbial DNA extraction. Tubes were brought to the clinic immediately after a sample was produced or were stored at –20 °C for less than 24 hours and then brought to the clinic, where they were stored at –80 °C until further processing. DNA was extracted using the DNeasy PowerSoil DNA Isolation Kit (Qiagen). The V4–V5 region of the bacterial 16S rRNA was amplified by polymerase chain reaction (PCR) using the 515F and 926R primers (Bioneer; sequences and protocol from the Earth Microbiome Project41) and was sequenced in an Illumina MiSeq sequencer (300-bp paired-end reads), as we recently described25,38.
Bioinformatic analyses of the fecal microbiome
Sequence reads from samples were first analyzed using the QIIME2 framework42, as we previously described38. Identification of changes in α-diversity (using indices Chao1, Shannon and observed), β-diversity (Bray–Curtis index) and differentially abundant taxa analyses were performed on MicrobiomeAnalyst43. We used edgeR to identify differential abundant taxa, and this was adjusted for multiple comparisons using an FDR, where q < 0.05 was considered significant.
Inflammatory markers
High-sensitivity ProQuantum immunoassays for cytokines IL10 (A35590), IL1β (A35574), IL17A (A35611) and IL6 (A355735) were performed according to the manufacturer’s protocol in a QuantStudio 7 qPCR Instrument (Thermo Fisher Scientific) in duplicates from placebo and HAMSAB timepoints. The quantification was calculated based on the standard curve.
Adverse effects
Adverse effects were closely monitored during the trial and discussed at each visit. Diets were well tolerated, and no adverse effects were reported. We also used a 100-mm VAS to quantify gastrointestinal symptoms as previously described36, where >30 mm out of a scale of 100 mm is considered a clinically significant increase in symptoms.
Outcomes
The primary outcome of this study was a decrease in 24-hour SBP measured using ABPM measurements. Secondary outcomes included changes in plasma SCFA levels, circulating markers of inflammation and fecal microbial composition. We have further expanded changes to BP to analyze day, night and central SBP and home SBP.
Sample size
In this proof-of-principle study, we estimated that we would require 26 participants to achieve 80% power with α = 0.05 (calculated effect size 0.8) to determine a 7-mmHg difference in 24-hour SBP after intake of modified HAMSAB for 3 weeks. We initially aimed to recruit 33 participants per group to allow a 20% dropout rate.
Missing data
One participant randomized into Diet A first had to take antibiotics between their third and study final visit while they were on the Diet B (placebo). Thus, their last data point was imputed using the multiple imputation function in SPSS software. We did not impute their data for the SmartPill data due to the small subsample size studied (n = 7).
Statistical analyses
Clinical data were analyzed using SPSS software (version 25), and SCFAs, gastrointestinal pH and cytokine data were analyzed in GraphPad Prism (version 9). No clinical data were excluded. Clinical data were checked for normality, and then paired two-tailed t-tests (for normally distributed data) or Wilcoxon tests (for non-normally distributed data) were used between baselines and between each baseline and its intervention (placebo or HAMSAB). Sensitivity analyses adjusted by baseline covariates were performed for 24-hour SBP and DBP, which were further analyzed using a GLM with repeated measures between and within participants, adjusted for sex, BMI, age and study arm. These are shown as placebo-subtracted or baseline-subtracted mean differences. All other data were analyzed using GraphPad Prism (version 9) built-in paired two-tailed t-tests (with a CI of the mean of differences shown as estimation plots, for all data excluding SmartPill data) or one-way ANOVA with Benjamini–Hochberg FDR adjustment for multiple comparisons (SmartPill data). All data are presented as mean ± s.e.m. or mean ± s.d., as detailed in figures and tables. P < 0.05 was considered statistically significant.
Role of the funding source
The funder of this study had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The microbiome data described in this article are available at the GenBank Nucleotide Database (BioProject ID PRJNA903679). We did not obtain patient consent for all the data to be available publicly. However, the data underlying this article can be shared for selected research questions upon reasonable request to the corresponding author. Please email F.Z.M. at francine.marques@monash.edu, who will respond within 4 weeks.
Code availability
The microbiome coding used is described at https://github.com/michael-nakai/waterway.
References
Maslowski, K. M. & Mackay, C. R. Diet, gut microbiota and immune responses. Nat. Immunol. 12, 5–9 (2011).
Marques, F. Z. et al. High-Fiber diet and acetate supplementation change the gut microbiota and prevent the development of hypertension and heart failure in hypertensive mice. Circulation 135, 964–977 (2017).
Bartolomaeus, H. et al. The short-chain fatty acid propionate protects from hypertensive cardiovascular damage. Circulation 139, 1407–1421 (2019).
Kim, S. et al. Imbalance of gut microbiome and intestinal epithelial barrier dysfunction in patients with high blood pressure. Clin. Sci. (Lond.) 132, 701–718 (2018).
Kaye, D. M. et al. Deficiency of prebiotic fibre and insufficient signalling through gut metabolite sensing receptors leads to cardiovascular disease. Circulation 141, 1393–1403 (2020).
Rhys-Jones, D. et al. Microbial interventions to control and reduce blood pressure in Australia (MICRoBIA): rationale and design of a double-blinded randomised cross-over placebo controlled trial. Trials 22, 496 (2021).
Collaborators, G. B. D. R. F. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 396, 1223–1249 (2020).
Collaboration, N. C. D. R. F. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 398, 957–980 (2021).
Beaney, T. et al. May Measurement Month 2019: the Global Blood Pressure Screening Campaign of the International Society of Hypertension. Hypertension 76, 333–341 (2020).
Benjamin, E. J. et al. Heart disease and stroke statistics—2019 update: a report from the American Heart Association. Circulation 139, e56–e528 (2019).
Appel, L. J. et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N. Engl. J. Med. 336, 1117–1124 (1997).
Reynolds, A. et al. Carbohydrate quality and human health: a series of systematic reviews and meta-analyses. Lancet 393, 434–445 (2019).
Marques, F. Z., Mackay, C. R. & Kaye, D. M. Beyond gut feelings: how the gut microbiota regulates blood pressure. Nat. Rev. Cardiol. 15, 20–32 (2018).
Muralitharan, R. R. et al. Microbial peer pressure: the role of the gut microbiota in hypertension and its complications. Hypertension 76, 1674–1687 (2020).
Gill, S. K., Rossi, M., Bajka, B. & Whelan, K. Dietary fibre in gastrointestinal health and disease. Nat. Rev. Gastroenterol. Hepatol. 18, 101–116 (2021).
Gill, P. A., van Zelm, M. C., Muir, J. G. & Gibson, P. R. Review article: short chain fatty acids as potential therapeutic agents in human gastrointestinal and inflammatory disorders. Aliment Pharmacol. Ther. 48, 15–34 (2018).
Tilves, C. et al. Increases in circulating and fecal butyrate are associated with reduced blood pressure and hypertension: results From the SPIRIT trial. J. Am. Heart Assoc. 11, e024763 (2022).
Gill, P. A., Bogatyrev, A., van Zelm, M. C., Gibson, P. R. & Muir, J. G. Delivery of acetate to the peripheral blood after consumption of foods high in short-chain fatty acids. Mol. Nutr. Food Res. 65, e2000953 (2021).
Clarke, J. M., Bird, A. R., Topping, D. L. & Cobiac, L. Excretion of starch and esterified short-chain fatty acids by ileostomy subjects after the ingestion of acylated starches. Am. J. Clin. Nutr. 86, 1146–1151 (2007).
Marino, E. et al. Gut microbial metabolites limit the frequency of autoimmune T cells and protect against type 1 diabetes. Nat. Immunol. 18, 552–562 (2017).
Norlander, A. E., Madhur, M. S. & Harrison, D. G. The immunology of hypertension. J. Exp. Med. 215, 21–33 (2018).
Heran, B. S., Wong, M. M., Heran, I. K. & Wright, J. M. Blood pressure lowering efficacy of angiotensin converting enzyme (ACE) inhibitors for primary hypertension. Cochrane Database Syst. Rev. CD003823 (2008).
Stamler, J. et al. INTERSALT study findings. Public health and medical care implications. Hypertension 14, 570–577 (1989).
Calderon-Perez, L. et al. Gut metagenomic and short chain fatty acids signature in hypertension: a cross-sectional study. Sci. Rep. 10, 6436 (2020).
Nakai, M. et al. Essential hypertension is associated with changes in gut microbial metabolic pathways: a multisite analysis of ambulatory blood pressure. Hypertension 78, 804–815 (2021).
Vacca, M. et al. The controversial role of human gut lachnospiraceae. Microorganisms 8, 573 (2020).
Toya, T. et al. Coronary artery disease is associated with an altered gut microbiome composition. PLoS ONE 15, e0227147 (2020).
Beale, A. L. et al. The gut microbiome of heart failure with preserved ejection fraction. J. Am. Heart Assoc. 10, e020654 (2021).
Ezeji, J. C. et al. Parabacteroides distasonis: intriguing aerotolerant gut anaerobe with emerging antimicrobial resistance and pathogenic and probiotic roles in human health. Gut Microbes 13, 1922241 (2021).
Falony, G. et al. Population-level analysis of gut microbiome variation. Science 352, 560–564 (2016).
Lei, Y. et al. Parabacteroides produces acetate to alleviate heparanase-exacerbated acute pancreatitis through reducing neutrophil infiltration. Microbiome 9, 115 (2021).
Gill, P. A., Muir, J. G., Gibson, P. R. & van Zelm, M. C. A randomized dietary intervention to increase colonic and peripheral blood short-chain fatty acids modulates the blood B- and T-cell compartments in healthy humans. Am. J. Clin. Nutr. 116, 1354–1367 (2022).
Nutting, C. W., Islam, S. & Daugirdas, J. T. Vasorelaxant effects of short chain fatty acid salts in rat caudal artery. Am. J. Physiol. 261, H561–H567 (1991).
Mortensen, F. V., Nielsen, H., Mulvany, M. J. & Hessov, I. Short chain fatty acids dilate isolated human colonic resistance arteries. Gut 31, 1391–1394 (1990).
Annison, G., Illman, R. J. & Topping, D. L. Acetylated, propionylated or butyrylated starches raise large bowel short-chain fatty acids preferentially when fed to rats. J. Nutr. 133, 3523–3528 (2003).
So, D. et al. Supplementing dietary fibers with a low FODMAP diet in irritable bowel syndrome: a randomized controlled crossover trial. Clin. Gastroenterol. Hepatol. 20, 2112–2120 (2021).
Yao, C. K. et al. Effects of fiber intake on intestinal pH, transit, and predicted oral mesalamine delivery in patients with ulcerative colitis. J. Gastroenterol. Hepatol. 36, 1580–1589 (2021).
Jama, H. et al. Maternal diet and gut microbiota influence predisposition to cardiovascular disease in the offspring. Preprint at https://www.biorxiv.org/content/10.1101/2022.03.12.480450v1.full (2022).
Marques, F. Z. et al. Guidelines for transparency on gut microbiome studies in essential and experimental hypertension. Hypertension 74, 1279–1293 (2019).
Mirzayi, C. et al. Reporting guidelines for human microbiome research: the STORMS checklist. Nat. Med. 27, 1885–1892 (2021).
Caporaso, J. G. et al. Ultra-high-throughput microbial community analysis on the Illumina HiSeq and MiSeq platforms. ISME J 6, 1621–1624 (2012).
Bolyen, E. et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 37, 852–857 (2019).
Chong, J., Liu, P., Zhou, G. & Xia, J. Using MicrobiomeAnalyst for comprehensive statistical, functional, and meta-analysis of microbiome data. Nat. Protoc. 15, 799–821 (2020).
Acknowledgements
We would like to acknowledge the Monash Proteomics and Metabolomics Facility for SCFA measurement and the Monash Bioinformatics Platform for access to M3 servers. We also would like to acknowledge M. Schlaich and J. Sesa-Ashton for their help with recruitment and T. Veitch for help developing the recipes used in the trial. This work was supported by a National Heart Foundation Vanguard grant (102182), a National Health & Medical Research Council (NHMRC) of Australia project grant (GNT1159721) and NHMRC fellowships to D.M.K., G.A.H., J.M. and R.E.C. F.Z.M. is supported by a Senior Medical Research Fellowship from the Sylvia and Charles Viertel Charitable Foundation Fellowship and by National Heart Foundation Future Leader Fellowships (101185 and 105663). The Baker Heart & Diabetes Institute is supported, in part, by the Victorian Government’s Operational Infrastructure Support Program.
Author information
Authors and Affiliations
Contributions
F.Z.M., D.M.K., C.R.M. and J.M. conceived and designed the study. H.A.J. wrote the first draft of the report, with input from F.Z.M. Both H.A.J. and F.Z.M. accessed and verified the data and performed the statistical analyses. D.R.-J. (supervised by F.Z.M. and J.M.) coordinated the trial, recruited participants and collected samples and data. Y.S. helped with recruitment. M.N. (microbiome), R.E.C. and G.A.H. (blood pressure), D.A. and D.J.C. (metabolites) and H.A.J. (cytokines) contributed with methods. All authors had full access to all data in the study, revised the manuscript critically, approved the version to be published and had final responsibility for the decision to submit for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Cardiovascular Research thanks Levi Waldron, Noel T. Mueller and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 HAMSB diet reduces in home systolic and diastolic blood pressure (BP).
a, Mean home systolic BP over 21-day HAMSAB intervention. b, Mean change in systolic BP relative to baseline and the mean difference in HAMSAB treated participants at b, Day1–3 and Day 17–20 and c, Day 1–3 and Day 14. d, Mean change in systolic BP relative to baseline and the mean difference in placebo treated participants at e, Day1–3 and Day 17-20 and f, Day 1-3 and Day 14. g, Overall drop in systolic BP relative to baseline and placebo-subtracted mean difference. h, Mean home diastolic BP over 21-day HAMSAB intervention. mean change in diastolic BP relative to baseline and the mean difference in HAMSAB treated participants at i, Day1-3 and Day 17-20 and j, Day 1-3 and Day 14. k, Mean change in diastolic BP relative to baseline and the mean difference in placebo treated participants at l, Day1-3 and Day 17-20 and m, Day 1-3 and Day 14. n, overall drop in diastolic BP relative to baseline and placebo-subtracted mean difference. n = 20/treatment group. Error bars represent ±SEM. Two-tail paired t-test.
Extended Data Fig. 2 Propionate, changes to the gut microbiome and plasma cytokines between placebo and HAMSAB.
a, HAMSAB diet did not change plasma propionate levels. n = 20/treatment group. Error bars represent ±SEM. Two-tail Wilcoxon test. b, Bray Curtis β diversity test showing principal coordinate analysis plot between baseline and the placebo arm. n = 18-19/treatment group. Shaded ellipsis representing the 95% confidence interval for each group. c-f, In participants randomised to the HAMSAB arm first, Ruminococcus gauvreauii (c-d) and Parabacteroides distasonis (e-f) prevalence was significantly reduced after the 3-week washout period. Showing n = 11 after data from 3 participants randomised into HAMSAB first were removed due to low number of reads. Mean ±SEM. Two-tail Wilcoxon test. Plasma levels of g, IL-6; h, IL-17A; i, IL-10; and j, IL-1b in placebo and HAMSAB treated participants. n = 20/treatment group. Error bars represent mean ± SEM. Two-tail paired t-test for panels g and i, two-tail Wilcoxon test for panels h and j.
Extended Data Fig. 3 The impact of HAMSAB diet on gastrointestinal pH and transit times measured by Smart Pill.
We observed no difference in a, gastric emptying time; b, small intestinal transit time; c, colonic transit, and d, whole gut transit time in hours. We observed no difference in colonic e, minimum and f, median pH, but observed a decrease in g, maximum pH. h, Summary of maximum colonic pH in placebo and HAMSAB relative to baseline. Placebo data from a participant who had antibiotics between visits 3 and 4 was removed, resulting in n = 6 for placebo and n = 7 for baseline and HAMSAB groups. One-way ANOVA adjusted for multiple comparisons, showing adjusted P-values. Error bars represent mean ± SEM.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Jama, H.A., Rhys-Jones, D., Nakai, M. et al. Prebiotic intervention with HAMSAB in untreated essential hypertensive patients assessed in a phase II randomized trial. Nat Cardiovasc Res 2, 35–43 (2023). https://doi.org/10.1038/s44161-022-00197-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s44161-022-00197-4
This article is cited by
-
Immune and inflammatory mechanisms in hypertension
Nature Reviews Cardiology (2024)
-
Salty Subjects: Unpacking Racial Differences in Salt-Sensitive Hypertension
Current Hypertension Reports (2024)
-
The gut microbiome and hypertension
Nature Reviews Nephrology (2023)
-
Microbial metabolites reduce SBP in patients with resistant hypertension
Nature Reviews Cardiology (2023)
-
Gut Microbiota and Its Role in the Brain-Gut-Kidney Axis in Hypertension
Current Hypertension Reports (2023)
