
Abstract
Patients with cancer have been identified in several studies to be at high risk of developing severe COVID-19; however, rates of SARS-CoV-2 IgG seroconversion and its association with cancer types and anticancer therapy remain obscure. We conducted a retrospective cohort study in patients with cancer who underwent SARS-CoV-2 IgG testing. Two hundred and sixty-one patients with a cancer diagnosis underwent SARS-CoV-2 IgG testing and demonstrated a high rate of seroconversion (92%). However, significantly lower seroconversion was observed in patients with hematological malignancies (82%), patients who received anti-CD-20 antibody therapy (59%) and stem cell transplant (60%). Notably, all 17 patients who received immunotherapy, including 16 that received anti-PD-1/PD-L1 monoclonal antibodies, developed SARS-CoV-2 IgG antibodies (100% seroconversion). These data show differential rates of seroconversion in specific patient groups and bear importance for clinical monitoring and vaccination strategies that are being developed to mitigate the COVID-19 pandemic.
Similar content being viewed by others


Main
The coronavirus pandemic that started in December 2019 in Wuhan, China continues to send waves of COVID-19 disease throughout the world1,2. Several observational studies have identified patients with cancer as being at higher risk of contracting the virus with higher rates of manifesting a severe form of COVID-19 disease3,4,5. We have previously reported a higher case fatality rate in patients with hematological malignancies compared to solid malignancies in patients with cancer6. A pooled meta-analysis of 52 studies involving patients with cancer and COVID-19 reported a mortality rate of 25.6%7. While the mortality rates of patients with cancer are higher than the general population, it seems that about 70–80% of patients with cancer survive COVID-19 and therefore, it is important to understand the natural history of COVID-19 in this high-risk patient population. Of particular importance is the fact that this patient population often receives immunosuppressive cancer-directed therapy, which may impact their ability to mount a humoral immune response to the virus. It is therefore prudent to study the rate of formation of such antibodies to SARS-CoV-2 in patients with cancer who survived the illness to properly inform and develop treatment, surveillance and monitoring strategies in this vulnerable patient population.
Results
Patient selection
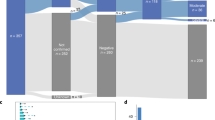
We collected data for all patients with a cancer diagnosis cared for at the Montefiore Health System (MHS) starting 1 March 2020 (first observed COVID-19 infection at MHS) until 15 September 2020. Figure 1 represents cohort selection for this study. A total of 4,302 patients were identified, of which 3,562 were excluded as they did not have a SARS-CoV-2 PCR with reverse transcription (RT–PCR) test result in our system, leaving 740 patients. Of the 740 patients, 460 were excluded as 8 patient records were duplicates and 452 did not have a SARS-CoV-2 IgG test. After excluding the aforementioned patients, 280 patients were identified of which, 15 were excluded as they did not have a confirmed diagnosis of malignancy. Three more patients were excluded as they had a negative SARS-CoV-2 PCR and a negative SARS-CoV-2 IgG and one patient was excluded as negative SARS-CoV-2 IgG test preceded a positive SARS-CoV-2 PCR. Finally, 261 patients with a confirmed diagnosis of malignancy and at least one SARS-CoV-2 IgG test performed during their care at MHS were included for analysis.

a, Consort diagram representing patient selection into the final cohort, listing selection criteria for inclusion into the present study (n = number of patients at each step). b, Diagram representing patients undergoing serial SARS-CoV-2 PCR testing.
Baseline characteristics
A total of 261 patients with a confirmed diagnosis of malignancy were included in this study. The median age of the cohort was 64 years (range 20–90 years). Seventy-seven percent (201 of 261) had a diagnosis of solid malignancy and 23% (60 of 261) had a hematological malignancy. Fifty-one percent (134 of 261) of patients were female and 49% (127 of 261) were male. Forty-one percent (106 of 261) of patients were African-American, 37% (98 of 261) were Hispanic, 13% (33 of 261) were white, 3% (8 of 261) were Asian and 6% (16 of 261) belonged to other ethnicities.
As expected, we had a preponderance of patients with solid malignancies; 22% (58 of 261) had breast cancer, 22%(57 of 261) had genitourinary cancer, 17% (44 of 261) had gastrointestinal cancer, 9% (24 of 261) had thoracic and head and neck cancer, 4% (10 of 261) had gynecological cancer, 2% (5 of 261) had central nervous system cancer and 1% (3 of 261) had skin/musculoskeletal cancer. Among patients with hematological malignancies 10% (26 of 261) had lymphoid disorders, 8% (20 of 261) had plasma cell disorders and 5% (14 of 261) had myeloid disorders.
We divided our cohort into patients who had active malignancy within 90 d of a SARS-CoV-2 test and those who did not. Of 261 patients, 68% (177 of 261) patients had active malignancy and 32% (84 of 261) did not. Of the patients with active malignancy, 135 had an initial diagnosis, 23 had progressive disease and 19 had relapsed disease. Of the inactive malignancy subgroup, 71 patients were in remission and 13 patients had malignancy that did not warrant therapy (for example monoclonal gammopathy of unknown significance). Patients were divided into three categories based on their comorbidities, 0–1, 2–3 and >3 comorbidities (comorbidities curated by chart review). Cancer diagnosis itself was not included as a comorbidity. The distribution of patients in the comorbidity categories was 26% (68 of 261), 30% (78 of 261) and 44% (115 of 261), respectively.
In addition, we also calculated a modified Charlson Comorbidity Index (CCI) for all included patients. Given that malignant conditions comprise 4 out of 19 criteria for the CCI, these were excluded while calculating the CCI for our patients, an approach that has been used in a previous study focused on patients with cancer diagnoses8. We then divided the entire cohort into three categories: CCI 0–1, 2–3 and 4+. The distribution of patients by CCI category is as follows: 0–1, 26% (68 of 261); 2–3, 38% (100 of 261) and 4+, 36% (93 of 261).
Overall, 92% of patients (239 of 261) had a positive SARS-CoV-2 IgG test and 8% (22 of 261) of patients had a negative SARS-CoV-2 IgG test. Fifty-six percent (147 of 261) had symptomatic SARS-CoV-2 infection while 44% (114 of 261) of patients had an asymptomatic infection. Symptomatic infection rate was 53% (106 of 201) among patients with solid malignancies and 68% (41 of 60) among those with hematological malignancies. There was a significant association seen between patients with hematological malignancy and symptomatic infection compared to solid malignancies (P = 0.04).
Twenty-three percent of patients (61 of 261) had steroid use at baseline. Of these, 21 patients were on steroids daily and 40 patients received steroids occasionally. The indications and frequencies of steroid use are available in the supplement. The median time between SARS-CoV-2 PCR and SARS-CoV-2 IgG test was 40 d and mean was 46 d.
Baseline characteristics and frequencies of asymptomatic infection of the cohort are summarized in Table 1 and Supplementary Table 2, respectively.
Cancer treatment history
We collected data for all cancer treatment that was received by each patient. We classified the treatments into the following categories: chemotherapy, immunotherapy, tyrosine kinase inhibitors, anti-HER therapy, antibody–drug conjugate, anti-CD20 antibody, anti-CD38 antibody, proteasome inhibitors, immunomodulator, BTK inhibitor, IDH1 inhibitor, BCL2 inhibitor, mTOR inhibitors, PARP inhibitor, TGF-β inhibitor, AR-targeted therapy, bispecific-T-cell-engager (BiTE) therapy, anti-EGFR monoclonal antibody, anti-VEGF monoclonal antibody therapy and history of stem cell transplant and CAR-T and cellular therapy. If a patient received two agents falling in the same category, they were classified only once (for example, if a patient received both degarelix and leuprolide, we classified them once in ‘endocrine therapy’). Combination and sequential treatment was classified in the appropriate category (for example, a patient receiving rituximab-based chemoimmunotherapy would be classified as received anti-CD-20 antibody, chemotherapy and steroids). CAR-T and cellular therapy included two patients who received CAR-T-cell therapy and one patient who received sipuleucel-T for prostate cancer. The most common treatment modality was cytotoxic chemotherapy in 46% (119 of 261) of patients followed by endocrine therapy in 27% (71 of 261) of patients. In the 90 d preceding a SARS-CoV-2 test, 110 patients had received medical cancer treatment, including 89 patients with a solid malignancy and 21 patients with a hematological malignancy. The frequencies of all treatments and treatments within 90 d of a COVID test have been summarized in Table 2. The median lines of therapy in the seropositive and seronegative cohorts is 1.
Clinical course of patients with absent seroconversion
All 22 patients who had a negative SARS-CoV-2 IgG had a preceding SARS-CoV-2 PCR that was positive. Sixteen of 22 patients had symptomatic infections, whereas 6 were asymptomatic. In the symptomatic subgroup, 11 patients were treated on a general medical floor, 1 patient needed intensive care unit (ICU) level of care, 3 patients were quarantined at home and details of the treatment setting for 1 patient are unknown. In the asymptomatic group, one patient was on the general medical floor for a different acute issue, one patient was transferred to ICU for close observation despite no symptoms, one patient was quarantined at home and details of three patients’ treatment settings are not available. Overall, in the seronegative cohort of patients, we observed a high symptomatic infection rate and high rates of hospitalization, with some needing ICU level of care.
Eleven of 22 patients had a hematological malignancy and 11 had a solid malignancy. In the seronegative group, 14 patients had chemotherapy, 7 had received anti-CD-20 antibody, 4 had received stem cell transplant, 3 had received a tyrosine kinase inhibitor, 2 patients each had received BiTE and CAR-T and 1 patient each had received an immunomodulator, proteasome inhibitor, antibody–drug conjugate, PARP inhibitor and BTK inhibitor. These treatments are summarized in Supplementary Table 3.
Association between seroconversion and cancer type
Given that patients with hematological malignancies tend to be more immunosuppressed and as several series have suggested, carry higher morbidity with COVID-19, we wanted to investigate differences in seroconversion in patients with hematological versus solid malignancies. Among 60 patients with hematological malignancies, 49 (81.7%) manifested SARS-CoV-2 IgG positivity, whereas 190 of 201 (94.5%) patients with solid malignancy manifested SARS-CoV-2 IgG positivity (Fisher’s exact test odds ratio (OR) 3.8; P = 0.005). Taken together, in our cohort, patients with hematological malignancies had a higher frequency of manifesting symptomatic COVID-19 infection and significantly lower likelihood of seroconversion.
Association between seroconversion and cancer therapy
Furthermore, we aimed to investigate whether seroconversion was associated with the type of cancer therapy received by a patient. In our analysis, we observed a significant association between previous use of anti-CD20 therapy and SARS-CoV-2 IgG. A total of 17 patients had received anti-CD20 therapy, of which 7 patients had a negative SARS-CoV-2 IgG (Fisher’s exact test, OR 0.09; P = 0.00013). A similar finding was observed in the cohorts of patients who had a history of stem cell transplant. Ten patients had received a stem cell transplant in our cohort of which, four remained negative for SARS-CoV-2 IgG (Fisher’s exact test, OR 0.1; P = 0.0057). The above ORs refer to comparisons with the entire cohort of patients with cancer. The P values are not adjusted for multiple hypothesis testing; however, false discovery rate (FDR) correction is provided for variables with more than two levels of analysis in Supplementary Tables 9, 11 and 12. We also noted reduced seroconversion in patients who received CAR-T-cell therapy (33%) and BiTE therapy (0%); however, given the small number of patients in these cohorts, statistical analysis was not performed.
In contrast, we observed very high seroconversion rates in patients who received immunotherapy or endocrine therapy. Seventeen patients received previous immunotherapy for their cancer and all 17 of them manifested a positive SARS-CoV-2 antibody response. Despite this 100% seroconversion rate, the OR did not reach statistical significance (P = 0.38), likely due to high baseline frequency of seroconversion for the entire patient population. Of 71 patients who received endocrine therapy for their cancer, 70 manifested a positive SARS-CoV-2 IgG (Fisher’s exact test, OR 8.6 = 0.01 compared to those without endocrine therapy). These results are summarized in Table 3.
The above results indicate that patients with hematological malignancies, anti-CD-20 therapy, CAR-T-cell therapy and stem cell transplant are associated with reduced seroconversion in patients with SARS-CoV-2. On the other hand, endocrine therapy has a strong association with positive antibody response in patients with SARS-CoV-2.
Active cancer and treatment within 90 days of SARS-CoV-2 IgG
We aimed to investigate potential confounders in the differential seroconversion rates noted for solid and hematological malignancies. We identified cancer status and cancer-directed therapy received within 90 d as potential key confounders and performed a multivariate logistic regression analysis. These variables were chosen as these would be biologically plausible to have an effect on seroconversion. Results indicate that the association between solid versus hematological malignancy and SARS-CoV-2 remain significant after accounting for active cancer and active cancer-directed treatment in the preceding 90 d of the COVID test, OR 4.004, P = 0.0026 (Table 3 and Supplementary Table 10).
Association of steroid use and SARS-CoV-2 IgG test
We investigated baseline use of corticosteroids in our cohort. Twenty-three percent (61 of 261) of patients had steroid exposure before the SARS-CoV-2 test. Of these, 40 patients had occasional steroid use, whereas 21 patients had daily steroid use. Ten additional patients received steroids for COVID-19 infection. In a univariate analysis, steroid use at baseline showed a notable trend with lack of seroconversion (P = 0.06). Similarly, while the low numbers limit strong conclusions, steroid use for COVID-19 management also showed an association with absent seroconversion. The indications, frequencies and results of this analysis are summarized in the supplement.
Persistent SARS-CoV-2 PCR positivity
Eighteen percent (47 of 261) of patients underwent serial SARS-CoV-2 PCR testing as per institutional policies to document clearance of infection (Fig. 1). Thirty-five patients had a solid malignancy and 12 had hematological malignancy. The mean shedding time, calculated as the time between first and last positive SARS-CoV-2 PCR, was significantly higher in patients with hematological than in patients with solid malignancies (61 d versus 33 d, P = 0.007; Table 4). Seropositivity was noted in 31 patients with a solid malignancy and 9 with a hematological malignancy. The remaining four patients with a solid malignancy and three with a hematological malignancy remained seronegative (Table 4). This observation again stresses the importance of close follow-up and monitoring of patients with hematological malignancies and may be impactful in designing quarantine strategies for these patients after clinical improvement from acute COVID-19 illness.
Serial SARS-CoV-2 IgG testing
Fifty-six patients underwent serial SARS-CoV-2 IgG testing. Of these, 53 had an initial positive test and 3 patients had an initial negative test. We collected data for time between first and last test available in our system. In this cohort, 44 of 53 patients remained persistently positive, whereas 9 patients turned seronegative. Eight of nine patients had a solid malignancy and one had a hematological malignancy. Seven of nine patients received treatment for cancer in the 90 d preceding a COVID test. Of the three initial patients who were seronegative, one patient turned seropositive and two remained persistently seronegative. The median time between first and last test in this cohort was 49 d (Supplementary Table 13).
Outcomes
Twenty-nine of 261 patients had died by the time of data cutoff date. Among them, 14 died due to progressive malignancy and 1 died of sequelae of COVID-19 infection (Supplementary Table 14).
Discussion
COVID-19 disease caused by SARS-CoV-2 has now affected more than 68 million humans worldwide, including over 27 million in the United States and has caused more than 400,000 deaths in the United States alone (Johns Hopkins Coronavirus Resource Center as of 5 February 2021). Older age and having multiple comorbid conditions have been identified as predictors of mortality in this disease9. Several observational cohorts have identified that patients with cancer have a longer, protracted course with COVID-19 necessitating hospitalization and intensive care. Patients with hematological malignancies have been reported in many series, including our own, to have higher mortality compared to solid malignancies6,10. While it was hypothesized in many cohorts that a diagnosis of cancer predicts mortality, data on this particular aspect are still evolving as recent matched studies report similar mortality in patients with cancer compared to age-matched controls without a diagnosis of cancer11. Nevertheless, concern about seroconversion in this patient population, which often receives immunosuppressive treatments, has been raised as mounting a humoral immunity is crucial not only in recovery from the infection, but to also establish and maintain herd immunity through effective vaccination strategies.
This large cancer cohort reports seroconversion rates following SARS-CoV-2 infection. Ninety-two percent of patients manifested a positive antibody response in our study that was focused on a large cohort of ethnically diverse patients who survived SARS-CoV-2 infection. With the same SARS-CoV-2 IgG assay, seroconversion rates in the general population have been reported as 90–100%12,13,14. Indeed, in an unselected cohort of 1,008 patients with SARS-CoV-2 PCR positivity in our health system who had subsequent antibody testing, the seroconversion rate was 91%, nearly identical to the overall seroconversion rate of our cohort of patients with cancer, providing reassurance that most patients with cancer are able to mount an antibody response to SARS-CoV-2 similar to the general population (Supplementary materials).
In an observational study from Spain involving 43 patients with cancer, seroconversion was noted in 83% patients and was absent in 17% (6) patients. Four of the six patients were on immunosuppressive therapy, of which two received rituximab and two received cisplatin-based therapy15. Studies comparing seroconversion in patients with cancer versus controls, report seroconversion rates ranging from 72.5%16 (retrospective) to 87.9 % (prospective)17. A similar finding in an anti-CD20-treated patient was noted in a recently published case report18.
In our study, we observed significant and clinically meaningful differences in seroconversion rates in patients who had received anti-CD20 therapy and stem cell transplants. The biological basis of this can be explained by the fact that anti-CD-20 therapy, such as rituximab, depletes native B cells not only in lymphoid tissue but also in bone marrow19. A statistically significant association was also seen with CAR-T-cell therapy (Supplementary Material) and BiTE therapy; however, given the small sample size, further validation in prospective cohorts is needed. CAR-T cells directed toward CD-19 also deplete native B cells, leading to hypogammaglobulinemia, often needing intravenous immunoglobulin replacement20. Patients who are recipients of stem cell transplantation are often subject to myeloablative doses of chemotherapy and total body irradiation, which contributes to profound immunosuppression in these patients. Our study in conjunction with existing literature highlights that patients with hematological malignancies who have received the aforementioned therapies, will need close follow-up and monitoring to document clearance of infection. Among these patients, seroconversion might not occur, possibly raising the concern of recurrent infections. As vaccines against SARS-CoV-2 are planned to be distributed on a large scale, monitoring SARS-CoV-2 IgG, immunoglobulin levels and lymphocyte subsets may be warranted in this patient population. Booster dosing may need to be studied in future trials and considered for this patient population should initial antibody responses be blunted.
Encouragingly, our study demonstrated high rates of seroconversion in patients with solid malignancies, in particular those who received immunotherapy and endocrine therapy for cancer treatment. Immunotherapy continuation has been specifically raised as a concern for patients with COVID-19 as immune-mediated pneumonitis is a significant side effect. Moreover, immunotherapy, specifically among patients with lung cancer, was associated with increased risk of ICU admission in one series of 275 patients21. On the contrary, two large cohorts, the UK Coronavirus Cancer Monitoring Project and the COVID-19 and Cancer Consortium (CCC 19) reported that mortality was not affected in patients with cancer and COVID-19 by type of anticancer therapy, including immunotherapy4,22. It is also hypothesized that immune-checkpoint inhibitors may induce immunocompetence in patients infected with SARS-CoV-2 (ref. 23) based on previous data from human immunodeficiency virus and immunotherapy and ongoing trials with nivolumab in patients with sepsis24,25. Our 100% seroconversion rate provides supportive evidence that immunotherapy is not deleterious and rather, may support the hypothesis of restoring immunocompetence in patients with COVID-19. In addition, we note strong trends toward inferior seropositivity rates among patients receiving steroid therapy both before SARS-CoV-2 infection as well as for the management of COVID-19.
It is worth highlighting that patients receiving endocrine therapy for their malignancy (mostly breast cancer and prostate cancer) typically tend to have limited or no other cancer therapy exposure and therefore, less immunosuppression. This may explain our observation of strong positive seroconversion in patients treated with endocrine therapy.
A subset of patients in our cohort underwent serial SARS-CoV-2 IgG testing at provider discretion and 9 of 53 patients who were initially seropositive turned seronegative over time. These observations clearly need further validation in a larger cohort. Notably, these may have implications for guidelines and possible advocacy for continued vaccination of this vulnerable population.
Asymptomatic infection has been identified as a important factor in the community spread of SARS-CoV-2, which in turn, continues to propagate the pandemic26. As discussed previously, patients with cancer are prone to more symptomatic and serious illness. However, in our cohort, we found a surprisingly high rate of asymptomatic infections, with a higher frequency noted among patients with solid tumors. This finding is logical as patients with hematological malignancies are known to be prone to more serious illness and poorer outcomes. Many patients in our cohort tested positive as part of routine screening before procedures or during admission for unrelated acute problems. In some cases, patients who had contact with family members who were symptomatic with COVID-19 remained asymptomatic themselves. In a recent small study, seroconversion was noted in patients with cancer only if they had a symptomatic infection27. In our cohort 41% patients were defined as asymptomatic (114 of 261). Of these, 108 had positive SARS-CoV-2 IgG (Supplementary Table 4) and 6 had negative SARS-CoV-2 IgG. This finding suggests that asymptomatic infection also leads to seroconversion in the majority of cases and possibly contributes to expansion of the pandemic and herd immunity.
Another notable finding noted in our study is the tendency toward more persistent shedding of SARS-CoV-2 in patients with hematological malignancies, with a mean of 61 d despite clinical improvement in many cases. While we are unable to confirm whether virus was live in each patient, our findings seem concordant with a recent study that reported patients who had received stem cell transplant and CAR-T-cell therapy shed viable virus for up to 2 months from onset of symptoms28.
Our study has a few limitations warranting discussion, including its retrospective design and a small cohort among patients who received specific therapies that predicted seroconversion, calling for further validation in larger cohorts focused on these unique associations. Another limitation of the study may be a slight overestimation of the asymptomatic infection rate given the manner of asymptomatic infection needed to be defined in a retrospective design. Our cohort also represents standard of care practice wherein testing was performed at provider discretion and not as part of a prospective, controlled study; however, as PCR negativity was required for patients to be able to resume cancer management in our practices, testing was frequent in the majority of patients.
In summary, we present a large cohort of patients with malignancy who underwent SARS-CoV-2 IgG testing. Statistically significant absent seroconversion was observed in patients with hematological malignancies, patients receiving anti-CD-20 therapy, CAR-T-cell therapy and stem cell transplant. These findings may be impactful not only for clinical monitoring and surveillance, but also in designing and tailoring vaccination for this high-risk patient population. These findings should be investigated in larger, prospective studies for further validation but should provide immediate guidance for clinicians and researchers.
Methods
Study objectives
The primary objectives were to study the rate of seroconversion for SARS-CoV-2 IgG for patients with cancer and its association with type of malignancy and type of anticancer therapy. Additionally, we also aimed to study patterns in the natural history of COVID-19 and patients with cancer. Specifically, we studied the rate of symptomatic and asymptomatic infection in patients with cancer and COVID-19 and its association with type of malignancy and treatment received.
Study design
This was a real-world, observational, retrospective exploratory cohort study of the entire pool of patients with a cancer diagnosis managed at our institution with the prespecified criterion of positivity of one COVID test without previous hypotheses testing/power analyses. We collected data on demographic variables (age, sex, cancer diagnosis), comorbidities (excluding cancer itself), SARS-CoV-2 IgG result, SARS-CoV-2 RT–PCR result, cancer treatment history, onset of symptoms of COVID-19, subsequent disease course, treatment setting, complications and outcomes. The data were extracted through a retrospective chart-level medical record review using Montefiore Medical Center’s EPIC electronic health record system. All patient information was de-identified. The study was approved by the Institutional Review Board of Albert Einstein College of Medicine/MHS. Informed consent was waived by Montefiore-Einstein Institutional Review Board as this was a retrospective chart review study. The Institutional Review Board (IRB) at Montefiore-Einstein provided ethics oversight (IRB no. 2020-11814).
Definitions
Asymptomatic infection
Patients were classified as having an asymptomatic infection if (1) there was clear documentation at the time of a positive SARS-CoV-2 test that patient had no symptoms; (2) if there was documentation at the time of a SARS-CoV-2 IgG test that patient had no symptoms; or (3) a test result of SARS-CoV-2 PCR or IgG was present in the patient’s chart and documentation was unable to confirm that patient had any symptoms (symptoms unknown, as these patients could not have had more than minimal symptoms they were clustered with the asymptomatic cohort).
Active cancer
We noted patient’s malignancy status within 90 d preceding a SARS-CoV-2 test. Patients were classified as having an active malignancy if it was their initial diagnosis, relapsed or progressive disease. Patients were classified as having an inactive malignancy if their cancer was in remission or if they carried a diagnosis that did not warrant therapy (such as monoclonal gammopathy of unknown significance).
COVID-19 test methods (assay)
SARS-CoV-2 RT–PCR
Real-time RT–PCR for SARS-CoV-2 was performed on nasopharyngeal swabs collected in viral transport medium using one of three testing platforms. These included the Hologic Panther Fusion, Abbott m2000 and Cepheid GenXpert SARS-COV-2 assays. All testing was performed in accordance with manufacturer or laboratory emergency use authorization instructions. Each assay was designed to amplify two separate regions within the SARS-CoV-2 viral genome and one amplification control in a single multiplex reaction. The target regions of amplification differ by platform with Hologic amplifying two separate regions of ORF1a, Abbott amplifying RdRp and N genes and Cepheid amplifying portions of the N and E genes.
SARS-CoV-2 IgG test
IgG testing was performed using the Abbott SARS-COV-2 IgG assay, which has received emergency authorization from the US Food and Drug Administration. The assay is a high throughput chemiluminescent microparticle immunoassay designed to detect IgG antibodies to the nucleocapsid of SARS-CoV-2. Recombinant SARS-CoV-2 antigen is incubated with a patient serum or plasma sample. IgG in a patient’s sample reacts with an anti-human IgG acridinium-labeled conjugate to produce a chemiluminescent reaction measured as relative light units (RLUs). The greater the IgG level, the higher the RLU value. This relationship is reflected in the calculated signal-to-cutoff (S/C) index produced upon comparing patient RLU to the assay calibrator. Positive results for IgG antibodies are determined when the S/C is ≥1.4
Statistics and reproducibility
Associations between pairs of variables were assessed with standard statistical procedures. In the case of two-level categorical variables, a Fisher’s exact test was used. For a two-level categorical and one numerical variable, we used a two-sample Student’s t-test and results were then re-analyzed by Wilcoxon testing. For a multilevel categorical and one numerical variable, an analysis of variance test was carried out and results re-tested by nonparametric Kruskal–Wallis rank-sum test. Pairings between a two-level and a multilevel categorical variable were summarized in a table where each row tests the association of a single multilevel category to the remaining categories, split by the two-level categories. We also performed a multivariate logistic regression analysis to account for key confounding variables, such as active cancer treatment and active versus inactive malignancy. Multiple hypothesis adjustments were not made for all analyses, however, to account for multiple testing; an FDR correction is provided in the supplement where more than two-level testing was performed. Statistical analyses were not performed on cohorts of fewer than five individuals given instability of results in such small groups. Data were collected using Microsoft Excel and all analyses were run in R software v.3.6.2.
Reporting Summary
Further information on research design is available in the Nature Research Reporting Summary linked to this article.
Data availability
Primary data will be made available from the corresponding authors upon request to protect patient privacy. Data availability may be subject to consultation with and contingent of approval from the Montefiore-Einstein IRB.
Code availability
The utilized computer code has been deposited in GitHub (https://github.com/kith-pradhan/CovidCancerReport). All analyses were conducted with built-in and freely available R packages. Further information on research design is available in the Nature Research Reporting Summary linked to this article.
References
Liu, J. et al. Clinical outcomes of COVID-19 in Wuhan, China: a large cohort study. Ann. Intensive Care 10, 99 (2020).
Guan, W.-j et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 382, 1708–1720 (2020).
Zhang, L. et al. Clinical characteristics of COVID-19-infected cancer patients: a retrospective case study in three hospitals within Wuhan, China. Ann. Oncol. 31, 894–901 (2020).
Kuderer, N. M. et al. Clinical impact of COVID-19 on patients with cancer (CCC19): a cohort study. Lancet 395, 1907–1918 (2020).
Dai, M. et al. Patients with cancer appear more vulnerable to SARS-CoV-2: a multicenter study during the COVID-19 outbreak. Cancer Discov.10, 783–791 (2020).
Mehta, V. et al. Case fatality rate of cancer patients with COVID-19 in a New York hospital system. Cancer Discov. 10, 935–941 (2020).
Saini, K. S. et al. Mortality in patients with cancer and coronavirus disease 2019: a systematic review and pooled analysis of 52 studies. Eur. J. Cancer 139, 43–50 (2020).
Jørgensen, T. L. et al. Comorbidity in elderly cancer patients in relation to overall and cancer-specific mortality. Br. J. Cancer 106, 1353–1360 (2012).
Du, R.-H. et al. Predictors of mortality for patients with COVID-19 pneumonia caused by SARS-CoV-2: a prospective cohort study. Eur. Resp. J. 55, 2000524 (2020).
Lee, L. Y. W. et al. COVID-19 prevalence and mortality in patients with cancer and the effect of primary tumour subtype and patient demographics: a prospective cohort study. Lancet Oncol. 21, 1309–1316 (2020).
Brar, G. et al. COVID-19 severity and outcomes in patients with cancer: a matched cohort study. J. Clin. Oncol. 38, 3914–3924 (2020).
Bryan, A. et al. Performance characteristics of the Abbott Architect SARS-CoV-2 IgG assay and seroprevalence in Boise, Idaho. J. Clin. Microbiol. https://doi.org/10.1128/JCM.00941-20 (2020).
Manalac, J. et al. Evaluation of Abbott anti-SARS-CoV-2 CMIA IgG and Euroimmun ELISA IgG/IgA assays in a clinical lab. Clin. Chim. Acta 510, 687–690 (2020).
Chew, K. L. et al. Clinical evaluation of serological IgG antibody response on the Abbott Architect for established SARS-CoV-2 infection. Clin. Microbiol. Infect. 26, 1256.e9–1256 (2020).
Garde-Noguera, J. et al. Impact of SARS-CoV-2 infection on patients with cancer: retrospective and transversal studies in Spanish population. Cancers https://doi.org/10.3390/cancers12123513 (2020).
Liu, T. et al. Low prevalence of IgG antibodies to SARS-CoV-2 in cancer patients with COVID-19. Int. J. Cancer 147, 3267–3269 (2020).
Marra, A. et al. Seroconversion in patients with cancer and oncology health care workers infected by SARS-CoV-2. Ann. Oncol. https://doi.org/10.1016/j.annonc.2020.10.473 (2020).
Yasuda, H. et al. Persistent COVID-19 pneumonia and failure to develop anti-SARS-CoV-2 antibodies during rituximab maintenance therapy for follicular lymphoma. Clin. Lymphoma Myeloma Leuk. 20, 774–776 (2020).
Houot, R. et al. Could anti-CD20 therapy jeopardise the efficacy of a SARS-CoV-2 vaccine? Eur. J. Cancer 136, 4–6 (2020).
Brudno, J. N. & Kochenderfer, J. N. Toxicities of chimeric antigen receptor T cells: recognition and management. Blood 127, 3321–3330 (2016).
Robilotti, E. V. et al. Determinants of COVID-19 disease severity in patients with cancer. Nat. Med. 26, 1218–1223 (2020).
Lee, L. Y. et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: a prospective cohort study. Lancet 395, 1919–1926 (2020).
Vivarelli, S. et al. Cancer management during COVID-19 pandemic: is immune checkpoint inhibitors-based immunotherapy harmful or beneficial? Cancers https://doi.org/10.3390/cancers12082237 (2020).
Day, C. L. et al. PD-1 expression on HIV-specific T cells is associated with T-cell exhaustion and disease progression. Nature 443, 350–354 (2006).
Hotchkiss, R. S. et al. Immune checkpoint inhibition in sepsis: a phase 1b randomized study to evaluate the safety, tolerability, pharmacokinetics, and pharmacodynamics of nivolumab. Intensive Care Med. 45, 1360–1371 (2019).
Nikolai, L. A. et al. Asymptomatic SARS coronavirus 2 infection: invisible yet invincible. Int. J. Infect. Dis. 100, 112–116 (2020).
Fuereder, T. et al. SARS-CoV-2 seroprevalence in oncology healthcare professionals and patients with cancer at a tertiary care centre during the COVID-19 pandemic. ESMO Open https://doi.org/10.1136/esmoopen-2020-000889 (2020).
Aydillo, T. et al. Shedding of viable SARS-CoV-2 after immunosuppressive therapy for cancer. N. Engl. J. Med. https://doi.org/10.1056/NEJMc2031670 (2020).
Acknowledgements
We acknowledge Cancer Center grant P30 CA013330 and NCORP grant 2UG1CA189859-06 in providing funding for this project. This work was supported partly by the Jane A. and Myles P. Dempsey fund and the Pelka Family fund. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
The author contributions were as follows: conception, A.T., A.V., S.G. and B.H.; data collection, A.T., S.J., Z.C. and B.R.; statistical analysis, K.P.; and manuscript writing, A.T., A.P.S., S.P., R.A.S., J.S., D.Y.G., A.V., S.G. and B.H. All authors contributed to manuscript revisions and final approval.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Peer review information Nature Cancer thanks Fabrice Barlesi, Justin Gainor, and Samuel Rubinstein for their contribution to the peer review of this work.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary Information
IRB-approved protocol for the study.
Supplementary Tables
Supplementary Tables 1–18
Rights and permissions
About this article

Cite this article
Thakkar, A., Pradhan, K., Jindal, S. et al. Patterns of seroconversion for SARS-CoV-2 IgG in patients with malignant disease and association with anticancer therapy. Nat Cancer 2, 392–399 (2021). https://doi.org/10.1038/s43018-021-00191-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s43018-021-00191-y
This article is cited by
-
Repeated SARS-CoV-2 vaccination in cancer patients treated with immune checkpoint inhibitors: induction of high-avidity anti-RBD neutralizing antibodies
International Journal of Clinical Oncology (2023)
-
Incidence and immunomic features of apyretic COVID-19 in patients affected by solid tumors: a prospective cohort study
Journal of Translational Medicine (2022)
-
Patterns of neutralizing humoral response to SARS-CoV-2 infection among hematologic malignancy patients reveal a robust immune response in anti-cancer therapy-naive patients
Blood Cancer Journal (2022)
-
Efficacy and impact of SARS-CoV-2 vaccination on cancer treatment for breast cancer patients: a multi-center prospective observational study
Breast Cancer Research and Treatment (2022)
-
Correlation between BNT162b2 mRNA Covid-19 vaccine-associated hypermetabolic lymphadenopathy and humoral immunity in patients with hematologic malignancy
European Journal of Nuclear Medicine and Molecular Imaging (2021)
