
Abstract
This retrospective study aimed to compare the mortality and burden of respiratory syncytial virus (RSV group), SARS-CoV-2 (COVID-19 group), non-H1N1 (Seasonal influenza group) and H1N1 influenza (H1N1 group) in adult patients admitted to intensive care unit (ICU) with respiratory failure. A total of 807 patients were included. Mortality was compared between the four following groups: RSV, COVID-19, seasonal influenza, and H1N1 groups. Patients in the RSV group had significantly more comorbidities than the other patients. At admission, patients in the COVID-19 group were significantly less severe than the others according to the simplified acute physiology score-2 (SAPS-II) and sepsis-related organ failure assessment (SOFA) scores. Using competing risk regression, COVID-19 (sHR = 1.61; 95% CI 1.10; 2.36) and H1N1 (sHR = 1.87; 95% CI 1.20; 2.93) were associated with a statistically significant higher mortality while seasonal influenza was not (sHR = 0.93; 95% CI 0.65; 1.31), when compared to RSV. Despite occurring in more severe patients, RSV and seasonal influenza group appear to be associated with a more favorable outcome than COVID-19 and H1N1 groups.
Similar content being viewed by others


Introduction
Respiratory Syncytial Virus (RSV) is a single stranded RNA virus, which was described for the first time over 60 years ago1. Its burden in the pediatric population is well known as it is the major pathogen involved in acute lower respiratory infection (ALRI) such as bronchiolitis. Estimations based on several studies assume that RSV is responsible for almost 33 million ALRI and more than 100.000 deaths worldwide2,3.
However, data regarding the burden of RSV in adults, particularly in the intensive care unit (ICU) setting, remain relatively scarce due to the absence of specific clinical features in this population compared to children. Moreover, the development of specific tools for RSV identification in respiratory samples is relatively recent, further explaining the scarcity of data in adults. What has been shown is that, in elderly and high-risk adults, the virus affects about 1.5 million patients each year in industrialized countries and leads to hospitalization in 14.5% of the cases4. Moreover, a study reported that, in adults hospitalized with confirmed RSV infection, 57.8% were diagnosed with RSV-related pneumonia and 20.1% were admitted to an ICU; overall, the mortality rate was 10.7%5. RSV was also identified in 10% of respiratory samples from patients admitted to an ICU for ALRI6. Nevertheless, the characteristics and outcomes of adult patients admitted to ICU for RSV-related ALRI are not well described.
The prevalence of acute respiratory failure caused by community-acquired respiratory viruses (CARVs) has long been underestimated, although its economic burden has been suggested by some authors7,8. The two pandemics of the past decades, caused first by A(H1N1)pdm09 and then SARS-Cov-2, have reminded however, that respiratory viruses represent a major public healthcare concern8,9,10.
Data comparing the outcomes of patients infected by RSV or other CARV in the ICU are scarce.
The objective of the present study was to compare the 90-day survival and burden between the four following groups (RSV, COVID-19, Seasonal influenza and H1N1).
Methods
Study design
We conducted a retrospective study including patients with RSV, SARS-CoV-2 and influenza infections (distinguishing A(H1N1)pdm09 from other A and B influenza viruses) who were admitted to 6 ICU of the Lyon teaching hospital (Hospices Civils de Lyon, France).
This study was conducted in accordance with the amended Declaration of Helsinki and was approved by the institutional ethics committee (scientific and ethical committee of the Hospices Civils de Lyon, CSE-HCL, reference N° 21-505). It reviewed that our study was in strict compliance with the French reference methodology MR-004 established by the French national data protection commission (Commission Nationale de l’Informatique et des Libertés, CNIL, reference 21_5505). Informed consent was obtained from all subjects and/or their legal guardian(s). In accordance with French law, all patients received an information letter by post; if no objection to the use of their data was received within 30 days, the patients were enrolled. Data has been fully anonymized. No patient aged under 18 years old was included.
Patients
All adult patients hospitalized in one of the 6 ICU between January 6, 2011 and December 28, 2018 with respiratory failure and a diagnosis of RSV infection (antigen testing, or positive RT-PCR from either bronchoalveolar lavage or nasopharyngeal specimen) were included in the RSV group. All adult patients hospitalized in one of the ICU between February 27, 2020 and April 22, 2020 with respiratory failure and a PCR-confirmed diagnosis of SARS-CoV-2 infection according to WHO interim guidance (positive RT-PCR from bronchoalveolar lavage or nasopharyngeal specimen) were included in the COVID-19 group. Given the fact that this period corresponded to the first wave in France, the circulating variants were likely to be mainly pre-VOC -alpha as it was identified in England at the end of 2020. All patients hospitalized in one of the ICU between November 1, 2015 and April 30, 2019 with respiratory failure and a PCR-confirmed diagnosis of influenza according to WHO interim guidance (positive RT-PCR from bronchoalveolar lavage or nasopharyngeal specimen) were included in the influenza group. The latter group was then split into two groups: All A serotypes (mainly H3N2) except H1N1pdm09 and all B lineages (yamagata and Victoria mainly) were included in the seasonal influenza group and A serotype (H1N1)pdm09 in the H1N1 influenza group. This selection was chosen to explore differences between ‘ancient’ CARV (RSV and seasonal influenza group), former pandemic virus now seasonal (H1N1 group) and pandemic virus (COVID-19 group). Respiratory failure was defined by the need for High-Flow Nasal Oxygen therapy (HFNO), non-invasive ventilation (NIV), or invasive mechanical ventilation (MV). Follow-up was completed on June 4, 2020 for the 4 groups. The patients in the COVID-19 and influenza groups were originally included in a previous study by our group9.
Primary and secondary endpoints
The primary endpoint was survival analysis according to the type of viral infection (RSV, COVID-19, seasonal influenza, and H1N1) in patients with respiratory failure admitted to an ICU.
The secondary endpoints were related to morbidity: ICU length of stay, ICU-related complications (infection with ventilator-associated pneumonia [VAP], thromboembolism with occurrence of pulmonary embolism [PE] or deep vein thrombosis [DVT]), organ support and severity during the ICU stay (kidney failure with need for renal replacement therapy [RRT], hemodynamics with need for norepinephrine and duration of use, neurological failure according to Glasgow Coma Scale [GCS]), Sepsis-related organ failure assessment (SOFA) at Day 1, 7, 14, and SOFARANK for the first14 days10.
We also focused on respiratory failure by collecting data on respiratory support modalities (duration of HFNO, NIV or IMV, use of prone positioning, need for extra corporeal membrane oxygenation [ECMO]).
Baseline clinical and laboratory characteristics including clinical presentation were compared between groups. The condition “young and previously healthy”, which was recently reported in a study, was also used herein to allow comparison11. All variables are detailed in the supplementary information.
Data collection
All the data analyzed in the present study were recorded on an ongoing basis in the ICU electronic health record database (IntelliSpace Critical Care and Anesthesia-ICCA; Koninklijke Philips N.V.; Amsterdam, The Netherlands) and were retrospectively collected from the reporting database. Data were obtained from the reporting database using SQL server manager studio (SSMS, v18.5. Microsoft Inc., Redmond, W.A, USA). The methods for data collection and quality control have been previously described9. Methods used for detection of the 4 different viruses are detailed in the supplementary information.
Statistical analysis
Descriptive statistics were performed using median [interquartile range, IQR], and frequency (percentage) for quantitative and qualitative variables, respectively. Differences between groups were estimated using Wilcoxon Rank Sum Test for quantitative variables, and Chi-square test or Fisher’s exact test when applicable for qualitative variables. If a heterogeneity between groups was detected, a two-by-two comparison was performed to detect the group differences. The statistical threshold for two-by-two comparisons was set at 0.01.
For the survival analysis, a competing risk regression was performed, with a methodology previously described (keeping them alive approach)12. The 59 missing variables (< 3% per variable) were imputed using multivariate imputation by chained equations.
The following covariates, which were found to be associated with mortality in the literature, were selected for adjustment (see Supplementary table 1): age, sex, BMI, SOFA at day 1, simplified acute physiology score-II (SAPS-II), cancer, asthma/chronic obstructive pulmonary disease (COPD), diabetes, chronic kidney disease, immunosuppressive condition, and myocardial infarction13,14,15,16.
The competing risk regression was then used to estimate the independent effect of each virus group on mortality, adjusted on pre-specified confounding variables.
Results are expressed in adjusted sub hazard ratios (sHR) associated with their 95% CI.
Statistical significance for the p value was set at 0.05. Statistical analyses were performed using the package survival from R software V 3.6.3.
Ethics approval and consent to publications
This study was conducted in accordance with the amended Declaration of Helsinki and was approved by the institutional ethics committee (Scientific and Ethical Committee of the Hospices Civils de LYON, CSE-HCL, under reference N° 21-505). It reviewed that the study was in strict compliance with the French reference methodology MR-004 established by the French national data protection commission (Commission nationale de l’informatique et des libertés, CNIL, under reference N° 21_5505). Non-opposition for data use was obtained from the patients. All patients received an information letter by post; if no objection was received within 30 days, the patients were enrolled in accordance with French law. Data has been fully anonymized. No patients under 18 years old were enrolled.
Results
Patients
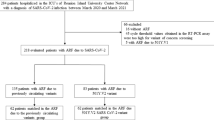
A total of 832 patients were screened and 807 were finally included (supplementary Information). In the RSV group, 56% of the positive tests were performed on nasopharyngeal specimens and 44% on bronchoalveolar fluid.
Patients admitted for RSV had more comorbidities according to Charlson Comorbidity Index (CCI). More specifically, they were more likely to have a history of myocardial infarction, congestive heart failure, active solid tumor or metastatic cancer, history of respiratory disease (asthma, COPD), and were more likely to have been hospitalized in the past 12 months (Table 1).
Patients in the COVID-19 group were less frequently active or past smokers as well as chronic alcohol consumers and less often a history of active cancers. Immunosuppressive treatments were significantly less frequent in the COVID-19 group compared to the other 3 groups. Few patients (5%) were considered as young and previously healthy, with no significant difference between groups (Table 1).
At admission, patients in the COVID-19 group were significantly less severe according to the SAPS-II and SOFA scores at admission compared with seasonal influenza, RSV, and the H1N1 group, see Table 1. Fever at admission was less frequent in the RSV group (35%) compared with the H1N1 (77%), seasonal influenza (65%) and COVID-19 groups (84%, p < 0.001; Table 1). At admission, there were significant differences among the 4 groups regarding laboratory parameters (Table 2).
Concerning specific therapies, 259 patients (77%) admitted for influenza (seasonal and H1N1) received oseltamivir, 11 patients (3%) in the COVID-19 group received remdesivir, 69 (14%) received hydroxychloroquine, 14 (4%) received ritonavir and 4 patients (3%) in the RSV group received ribavirine. Overall, 240/807 (30%) patients were treated with corticoids during their ICU stay, with no statistical difference between groups.
Survival analysis
In comparison with the RSV group, the COVID-19 group (sHR 1.61 CI.95 [1.10–2.36] p = 0.014) and H1N1 group (sHR 1.87 CI.95 [1.20–2.93] p < 0.001) were associated with a higher mortality. Conversely, seasonal influenza was not associated with a higher mortality compared to RSV (sHR 0.93 CI.95 [0.65–1.31] p = 0.67; supplementary table 1). For patients aged 65 years and older, mortality in the ICU was 35% in the RSV group, 50% in the H1N1 group, 28% in the seasonal influenza group, and 37% in the COVID-19 group (p = 0.064).
Patient severity during ICU stay
Length of stay (LOS) in ICU for patients in the H1N1 and COVID-19 group were significantly longer than in the 2 others groups, see Table 3.
Regarding organ failure and required support, patients in the H1N1 group required more frequently invasive MV (80%, p < 0.001) but its duration in the COVID-19 group was significantly longer, see Table 4. The rate of prone positioning was also higher in the COVID-19 group, see Table 4. Patients in the H1N1 and COVID-19 groups received more often neuromuscular blockade agents, see Table 4. Regarding non-invasive respiratory support, HFNO was more frequently used in the COVID-19 group and for a longer period, see Table 4. Patients in the RSV group received bronchodilators in a significantly higher proportion (intravenous and double aerosol therapy; see Table 4). Incidence of DVT and PE was higher in the COVID-19 group, see Table 4. In terms of organ support and severity, RRT was more frequent in the H1N1 group, see Table 4. There was no significant difference in vasopressor requirement between groups but when needed, it was used during a significantly longer period in the COVID-19 group, see Table 4. The evolution profile of the patients in the 4 groups differed significantly as highlighted by a negative SOFARANK on the 14 first days for the RSV and seasonal influenza groups and a positive SOFARANK the COVID-19 and H1N1 groups (Table 3).
Discussion
In this large retrospective cohort study, adjusted mortality at day-90 was significantly higher in the H1N1 and COVID-19 groups than for those in the RSV and seasonal influenza groups. At admission, the clinical presentation and laboratory parameters differed according to the infecting virus. Patients in the RSV group had more comorbidities, especially respiratory, and those in the COVID-19 group were the least severe at admission. The evolution of patients also differed as patients in the COVID-19 and H1N1 group present with more severe organ failure, especially respiratory, during the ICU stay. This strongly suggests that RSV and seasonal influenza intrinsically induce less severe pneumonia in more comorbid patients, as previously suggested9.
The present study is one of the largest comparing RSV with other CARV in an adult ICU population and the first to include SARS-CoV-2. Until now, only a few studies have compared CARV pneumonia in non-critical care patients17,18 and their results corroborate the present findings. One recent study comparing the outcomes of patients admitted to the ICU for respiratory failure related to RSV and influenza19 found an unadjusted ICU mortality rate slightly lower (19.4%) than that found herein. However, the authors reported that adjusted mortality did not differ significantly between the RSV and influenza groups (adjusted OR 0.80. CI.95 [0.49–1.30], p = 0.37), a result in line with those reported herein.
One explanation for the higher mortality rate observed herein compared to that of Coussement et al. could be that they included all patients with a positive PCR for RSV or influenza, with about a third of patients in each group receiving only low flow oxygen, whereas the present cohort included only patients with respiratory failure (i.e. need for MV, HFNO, or NIV). Moreover, 17 and 21% (RSV and influenza groups, respectively) of the patients in the study by Coussement et al. were admitted to the ICU for another reason than respiratory failure.
Further corroborating the present results, another study reported that COVID-19 and H1N1 patients had a higher 30-day mortality rate, longer ICU LOS, and longer duration of IMV although being less frail and less severe at admission when compared to an ICU population affected by other viruses including RSV and seasonal influenza20,21.
The present findings demonstrate the major burden of RSV in ICU with similar mortality and clinical outcomes than seasonal influenza. Thus, RSV should be systematically considered in patients admitted to the ICU for acute respiratory failure and this search should be carried out for a longer period than influenza, given the physiopathology of RSV22. Moreover, the present findings indicate that the clinical presentation differs according to the virus, which could allow a better identification of patients at risk. Conversely to patients affected by SARS-CoV-2 and A(H1N1)pdm09 influenza, patients with RSV are more severe at admission because of their comorbidities but have more favorable outcomes. These results suggest a higher intrinsic virulence of the most recent respiratory viruses. Since SARS-CoV-2 first appeared at the end of 2019, the world has faced successive outbreaks of the virus, which will likely stay endemic like RSV or influenza23,24,25,26. The successive variants have demonstrated a change in the course of the disease, with a trend toward a lower overall mortality, but an increase in the burden for patients with comorbidities, especially respiratory27 and immunocompromised ones28,29.
None of the specific treatment received by all the patients was associated with survival improvement. Of note, ribavirin, which is the only specific therapeutic against RSV currently available but whose benefit remains controversial30, was rarely given in the RSV group. While new drugs for RSV treatment31,32,33 are currently in development, management remains mainly supportive at this time. Although nirsevimab was recently proposed for at risk children34, no preventive strategy is available for adults. In light of the present findings regarding the burden of RSV in ICU adults, the need for new antiviral drugs and vaccines targeting RSV appears paramount.
The present study has limitations. First, data were collected retrospectively. We tried to minimize this bias by paying particular attention to the quality of the data collected, checking the diagnostic accuracy for all patients, and using the same queries and methodology for each group. Another limitation concerns the comparison of the four viruses over different periods, which could underline potential differences in patient management. However, all data were obtained from ICUs of the same teaching hospital that apply similar management approaches. Moreover, this bias is likely to concern mainly patients affected by RSV before 2013 (25/151), when the publication by Guerin et al. demonstrated the benefits of prone positioning in ARDS35. Indeed, other therapeutics (protective ventilation36,37, NMBA38,39) relied on studies older than the data collection periods considered herein. In the same way, the relatively low proportion of COVID-19 patients treated by corticoids could be a limitation. This is likely due to the fact that the inclusion of this group was made during the first wave of the pandemic, before the publication of high quality data supporting the use of corticoids in severe COVID-1940.
The choice was made to select potential confounders based on prior knowledge and not on univariate analysis, as the latter practice has been shown to be strongly biased13,14,15,16. The variables included in the model were thus chosen before any statistical analysis, explaining the non-significant differences of certain confounders entered in the model.
The major strengths of this work are its large sample size, the selection of patients with ARF admitted to the ICU, and the inclusion of four major CARV in a multicenter design.
In conclusion, the present study highlights important differences in patient characteristics according to the virus involved. RSV and seasonal influenza are associated with more severe patients at admission because of their comorbidities but a more favorable outcome, in contrast to patients in the COVID-19 and H1N1 group.
Data availability
FW takes responsibility for the content of the manuscript, including the data and analysis. Data are available to reviewers upon request to the corresponding author.
Abbreviations
- ALRI:
-
Acute lower respiratory infection
- ARDS:
-
Acute respiratory distress syndrome
- ARF:
-
Acute respiratory failure
- BMI:
-
Body mass index
- CARV:
-
Community acquired respiratory viruses
- 95% CI:
-
95% Confidence interval
- COPD:
-
Chronic obstructive pulmonary disease
- CT:
-
Computed tomography
- DVT:
-
Deep vein thrombosis
- ECMO:
-
Extra corporeal membrane oxygenation
- FiO2:
-
Fraction of inspired oxygen
- HFNO:
-
High-flow Nasal oxygen therapy
- sHR:
-
Sub Hazard ratio
- GCS:
-
Glasgow Coma Scale
- ICU:
-
Intensive care unit
- LOS:
-
Length of stay
- IMV:
-
Invasive mechanical ventilation
- NIV:
-
Non-invasive ventilation
- NMBA:
-
Neuromuscular blocking agent
- PaO2:
-
Partial pressure of oxygen in blood
- PE:
-
Pulmonary embolism
- PEEP:
-
Positive end expiratory pressure
- PCR:
-
Polymerase chain reaction
- RRT:
-
Renal replacement therapy
- RT-PCR:
-
Reverse-transcriptase polymerase chain reaction
- SAPS-II:
-
Simplified acute physiology score
- SOFA:
-
Sepsis-related organ failure assessment
- RSV:
-
Respiratory syncytial virus
- VAP:
-
Ventilator-associated pneumonia
References
Blount, R. E., Morris, J. A. & Savage, R. E. Recovery of cytopathogenic agent from chimpanzees with coryza. Proc. Soc. Exp. Biol. Med. Soc. Exp. Biol. Med. N. Y. N 92, 544–549 (1956).
Li, Y. et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: A systematic analysis. Lancet Lond. Engl. 399, 2047–2064 (2022).
Nair, H. et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: A systematic review and meta-analysis. Lancet 375, 1545–1555 (2010).
Shi, T. et al. Global disease burden estimates of respiratory syncytial virus-associated acute respiratory infection in older adults in 2015: A systematic review and meta-analysis. J. Infect. Dis. 222, S577–S583 (2020).
Yoon, J. G. et al. Clinical characteristics and disease burden of respiratory syncytial virus infection among hospitalized adults. Sci. Rep. 10, 12106 (2020).
Choi, S.-H. et al. Viral infection in patients with severe pneumonia requiring intensive care unit admission. Am. J. Respir. Crit. Care Med. 186, 325–332 (2012).
Shorr, A. F., Fisher, K., Micek, S. T. & Kollef, M. H. The burden of viruses in pneumonia associated with acute respiratory failure: An underappreciated issue. CHEST 154, 84–90 (2018).
Fendrick, A. M., Monto, A. S., Nightengale, B. & Sarnes, M. The economic burden of non-influenza-related viral respiratory tract infection in the United States. Arch. Intern. Med. 163, 487–494 (2003).
de Marignan, D. et al. A retrospective comparison of COVID-19 and seasonal influenza mortality and outcomes in the ICUs of a French university hospital. Eur. J. Anaesthesiol. 39, 427–435 (2022).
Gelissen, H. et al. Effect of low-normal vs high-normal oxygenation targets on organ dysfunction in critically Ill patients: A randomized clinical trial. JAMA 326, 940 (2021).
Coussement, J. et al. Characteristics and outcomes of patients in the ICU with respiratory syncytial virus compared with those with influenza infection: A multicenter matched cohort study. Chest 161, 1475–1484 (2022).
Vacheron, C. H. Improved 30-day survival estimation in ICU patients: A comparative analysis of different approaches with real-world data. Crit. Care Med. https://doi.org/10.1097/CCM.0000000000006097 (2023).
Breiman, L. Statistical modeling: The two cultures (with comments and a rejoinder by the author). Stat. Sci. 16, 199–231 (2001).
Sauerbrei, W. et al. State of the art in selection of variables and functional forms in multivariable analysis—Outstanding issues. Diagn. Progn. Res. 4, 3 (2020).
Vacheron, C.-H., Friggeri, A., Allaouchiche, B., Maucort-Boulch, D. & Coz, E. Quiet scandal: Variable selection in three major intensive care medicine journals. Intensive Care Med. 47, 1487–1489 (2021).
Heinze, G., Wallisch, C. & Dunkler, D. Variable selection—A review and recommendations for the practicing statistician. Biom. J. 60, 431–449 (2018).
Chorazka, M., Flury, D., Herzog, K., Albrich, W. C. & Vuichard-Gysin, D. Clinical outcomes of adults hospitalized for laboratory confirmed respiratory syncytial virus or influenza virus infection. PLOS ONE 16, e0253161 (2021).
Ackerson, B. et al. Severe morbidity and mortality associated with respiratory syncytial virus versus influenza infection in hospitalized older adults. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 69, 197–203 (2019).
Coussement, J. et al. Characteristics and outcomes of patients in the ICU with respiratory syncytial virus compared with those with influenza infection: A multicenter matched cohort study. Chest https://doi.org/10.1016/j.chest.2021.12.670 (2022).
Heo, M. et al. Comparison of clinical features and outcomes between SARS-CoV-2 and Non-SARS-CoV-2 respiratory viruses associated acute respiratory distress syndrome: Retrospective analysis. J. Clin. Med. 11, 2246 (2022).
Hedberg, P. et al. Clinical phenotypes and outcomes of SARS-CoV-2, influenza, RSV and seven other respiratory viruses: A retrospective study using complete hospital data. Thorax 77, 1–10 (2022).
Hall, C. B. et al. Occurrence of groups A and B of respiratory syncytial virus over 15 years: Associated epidemiologic and clinical characteristics in hospitalized and ambulatory children. J. Infect. Dis. 162, 1283–1290 (1990).
Callaway, E. Beyond Omicron: What’s next for COVID’s viral evolution. Nature 600, 204–207 (2021).
Looi, M.-K. Covid-19: Is a second wave hitting Europe?. BMJ https://doi.org/10.1136/bmj.m4113 (2020).
Lee, A. C. K. & Morling, J. R. Living with endemic COVID-19. Public Health 205, 26–27 (2022).
Antia, R. & Halloran, M. E. Transition to endemicity: Understanding COVID-19. Immunity 54, 2172–2176 (2021).
Jung, C. et al. Evolution of hospitalized patient characteristics through the first three COVID-19 waves in Paris area using machine learning analysis. PLOS ONE 17, e0263266 (2022).
Ameratunga, R. et al. SARS-CoV-2 omicron: Light at the end of the long pandemic tunnel or another false dawn for immunodeficient patients?. J. Allergy Clin. Immunol. Pract. 10, 2267–2273 (2022).
Hussey, H. et al. Assessing the clinical severity of the Omicron variant in the Western Cape Province, South Africa, using the diagnostic PCR proxy marker of RdRp target delay to distinguish between Omicron and Delta infections—A survival analysis. Int. J. Infect. Dis. 118, 150–154 (2022).
Domachowske, J. B., Anderson, E. J. & Goldstein, M. The future of respiratory syncytial virus disease prevention and treatment. Infect. Dis. Ther. 10, 47–60 (2021).
DeVincenzo, J. P. et al. Oral GS-5806 activity in a respiratory syncytial virus challenge study. N. Engl. J. Med. 371, 711–722 (2014).
DeVincenzo, J. P. et al. Activity of oral ALS-008176 in a respiratory syncytial virus challenge study. N. Engl. J. Med. 373, 2048–2058 (2015).
Generation and Characterization of ALX-0171, a Potent Novel Therapeutic Nanobody for the Treatment of Respiratory Syncytial Virus Infection | Antimicrobial Agents and Chemotherapy. https://doi.org/10.1128/AAC.01802-15.
Hammitt, L. L. et al. Nirsevimab for prevention of RSV in healthy late-preterm and term infants. N. Engl. J. Med. 386, 837–846 (2022).
Guérin, C. et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 368, 2159–2168 (2013).
Petrucci, N. & Iacovelli, W. Ventilation with lower tidal volumes versus traditional tidal volumes in adults for acute lung injury and acute respiratory distress syndrome. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD003844.pub2 (2004).
Burns, K. E. A. et al. Pressure and volume limited ventilation for the ventilatory management of patients with acute lung injury: A systematic review and meta-analysis. PloS One 6, e14623 (2011).
Gainnier, M. et al. Effect of neuromuscular blocking agents on gas exchange in patients presenting with acute respiratory distress syndrome. Crit. Care Med. 32, 113–119 (2004).
Forel, J.-M. et al. Neuromuscular blocking agents decrease inflammatory response in patients presenting with acute respiratory distress syndrome. Crit. Care Med. 34, 2749–2757 (2006).
Angus, D. C. et al. Effect of hydrocortisone on mortality and organ support in patients with severe COVID-19: The REMAP-CAP COVID-19 corticosteroid domain randomized clinical trial. JAMA 324, 1317–1329 (2020).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Consortia
Contributions
F.W. and A.F. had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. B.G., F.W., A.F., C.H.V., J.S.C., D.D.M. contributed substantially to the study design, data acquisition, data analysis and interpretation, and the writing of the manuscript. A.B., E.F., S.C.T., J.C.R., F.A.d contributed substantially to the data acquisition and the writing of the manuscript. J.B., B.A., V.P., L.A., A.C.L., T.R., F.A.u, F.D., J.L.F. contributed substantially to the writing of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Grangier, B., Vacheron, CH., De Marignan, D. et al. Comparison of mortality and outcomes of four respiratory viruses in the intensive care unit: a multicenter retrospective study. Sci Rep 14, 6690 (2024). https://doi.org/10.1038/s41598-024-55378-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-55378-x
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
