
Abstract
The objective was to evaluate the relationship between the dimensions of the maxillary sinuses (MSs) and various cephalometric parameters. MS volume (MSV), MS surface (MSS), linear maximum depth (LMD), linear maximum width (LMW), and linear maximum height (LMH) were calculated on CBCT scans of 99 adults. Two sets of two-way (ANOVA) assessed the influence respectively of ANB and SNA angles and of the gender on MS dimensions. Pearson’s correlation was calculated between MS dimensions and different cephalometric variables. Reliability and accuracy of the proposed method was tested with intra-operator and inter-operator intraclass correlation coefficient (ICC). Two-way ANOVA showed no statistically significant difference in MSV, MSS and LMH between ANB groups, whilst males were associated with bigger sinuses. LMW showed statistically significant difference in both ANB and gender groups. LMD showed no statistically significant difference. The second Two-way ANOVA showed significantly larger MSV, MSS and LMD in patients with increased or reduced SNA angle but not between genders. LMW and LMH also showed a significant difference between genders. All linear measurements showed a significant interaction of the two factors. The intra-observer and inter-observer ICC scored high for all the tested measurements. MSV and MSS showed a positive correlation with S-N, PNS-A, S-Go, N-Me, N-Ans and the distance between Mx points. LMW had a negative correlation with Ba-S-N angle and N-Me, LMH with Ba-S-N angle, S-Go and Mx r-Mx l and LMD with N-Me and N-ANS. LMW had a positive correlation with Mx r-Mx l, LMH with S-N, S-N^Ans-Pns, N-Me, N-Ans and LMD with S-N, Ba-S-N, PNS-A, S-Go and distance between Mx points. In conclusion, MSV and MSS did not differ between the three skeletal classes, males showed significantly larger MS than in females. Concerning the influence of the cranio-maxillary relationship (SNA) and gender on MS dimension, subjects with a retrusion (SNA < 80°) or protusion (SNA > 84°) of the maxillary alveolar bone had larger MSV, MSS, LMW, LMH and LMD than subjects with a normal cranio-maxillary relationship (SNA 82 ± 2°). A statistically significant high positive correlation was observed between S-N, Pns-A, S-Go, Mx-R/Mx-r and MS dimension. Further studies that evaluate similar outcomes in different races may be able to enrich our knowledge on this topic.
Similar content being viewed by others

Introduction
Maxillary sinuses (MS) are the largest of the paranasal sinuses1. They are two bony chambers, located inside each maxillary bone. Being knowledgeable as to MS anatomy is a must, not only in forensics, but also in many dental and maxillofacial interventions.
The MS is the first paranasal sinus to form with growth starting during gestation, at the 12th week of pregnancy, as a lateral folding of the nasal epithelium2. Current literature3,4 reports that most of the MS postnatal growth occurs before the end of the 36th month, between seven and twelve years of age and adult size is reached between the ages of 12 and 15.
Maresh and Washburn5 were the first to assess posteroanterior teleradiographs and report observations and measurements of MS changes during adolescence. They emphasised that the growth of the MS varied according to the individual and varied widely5. Koymen et al.6 confirmed that MS dimension has individual variations and stated that facial biotype mat influence the morphology of the sinus. However, the data reported in international literature differ as to the growth and dimensions of the maxillary sinuses. This may be accounted for the fact that various methods have been applied for the evaluation of MS volume (MSV), including panoramic radiographs and lateral tele-radiographs, injection of various substances inside the MS and the application of the ellipsoid formula7,8,9.
However, advances in medical techniques have enhanced the evaluation of the maxillary sinuses. Indeed, various innovative diagnostic imaging techniques have been recently developed and have profoundly changed medical diagnostic capabilities. One such example is Cone Beam Computed Tomography (CBCT) in 199810 that allows a low-dose accurate three dimensional assessment of craniofacial bony structures11,12.
Moreover, when CBCT scans are elaborated with dedicated 3D software, precise morphometric 3D measurements can be obtained for all the craniofacial structures13.
Current literature on maxillary sinuses is scant and several studies that are published rely on two-dimensional radiographs, such as orthopantomography (OPG) and cephalometric radiographs. However, these 2D radiographs provide limited information as the MS is a 3D structure and may well lead to erroneous conclusions.
Some recent studies have reported having made a 3D evaluation of the MS and the other paranasal sinuses and the rhynopharynx for surgical and medical purposes9,14,15. Others evaluated how the MS volume differs according to age and gender16,17. CBCT has certainly become today the most used method for the evaluation of maxillary sinuses, highlighting a high reliability of the method as reported by different authors18,19,20.The literature searches in Pubmed, Scopus, EbSco performed by the authors revealed a limited number of papers investigating the relationship between MS size and cephalometric characteristics. Moreover, the only ones were performed on two-dimensional radiographs.
Oktay1 stated that the dimension of the MS was not influenced by malocclusion nor gender, and that only in Angle Class II, sex was a significant component.
Basdra et al.21 made a thorough evaluation of a subject with an asymmetric lower jaw due to changes in MS surfaces and reported that the MS may have an impact on facial growth.
The most recent study on the relationship between MS and malocclusion, has been proposed by Endo et al.22, who assessed MS dimensions and their relationship with Angle's dental classes and several cephalometric measurements using bidimensional radiographs.
Therefore, the aim of the present study is to provide a 3D assessment of the maxillary sinuses, by investigating volume (MSV), surface (MSS) and linear maximum height (LMH), width (LMW) and depth (LMD) and to perform a comparison between male and female subjects in the three different skeletal classes and cranio-maxillary relationship and to assess the relationship between the linear and volumetric measurements of the MS and the patients’ craniofacial characteristics.
Methods
The null hypothesis states that there is no difference in the maxillary sinus dimensions in male and female subjects having different skeletal classes (based on ANB) and cranio-maxillary relationships (based on SNA).
The CBCT scans of 99 MS of Caucasian patients were retrospectively examined at the Department of Biomedical Surgical and Dental Sciences, University of Milan, 20142 Milan, Italy.
The study presented herein, was approved by the Ethical Committee of Fondazione IRCCS Ca’Granda, Ospedale Maggiore, Milan—Italy (protocol n.573/15). All patients gave written informed consent for the use of medical records in anonymous form for research purposes.
Participants and inclusion criteria
This cross-sectional study was carried out by the assessment of cone beam computed tomographies taken between 2009 and 2019 at the Department of Radiology of Fondazione IRCCS Ca’Granda, Ospedale Maggiore, Milan. The patients were selected from the archives according to the following inclusion criteria: being Caucasian; nasal breathers; having all permanent teeth erupted apart from wisdom teeth; patients 16 years of age or older so as to evaluate subjects who were no longer or only slightly growing at the level of the maxillary sinus22,23.
The Exclusion criteria were: present or past pathological involvement of the maxillary sinuses; missing maxillary molars or premolars; previous orthodontic treatment; altered bone metabolism; skeletal asymmetry; alterations to the maxillofacial skeleton (acquired or congenital); mouth breathers.
A thousand five hundred fifty records were reviewed. On the basis of the exclusion/inclusion criteria, 99 Cone Beam Computed Tomographies of White subjects (47 males and 52 females), aged 20.9 ± 2.1 years, were selected for the study and categorized into three groups, according to anteroposterior skeletal classes based on Riedel’s Analysis ANB angle24: skeletal groups Class I (ANB 2 ± 2°), 34 subjects, Class II (ANB > 4°), 31 subjects, and Class III (ANB < 0°), 34 subjects. The patients were also categorized into 1 of the 3 cranio-maxillary relationships determined by the horizontal prognathism of the maxillary alveolar bone, based on Downs’ SNA angle25: Normatrusive (SNA 82 ± 2°) 35 subjects, protrusive (SNA > 84°) 33, retrusive (SNA < 80°) 31 subjects.
After assessing the absence of any asymmetries between the right and left MS in the sample, the average between the two sides was calculated and used for simplicity throughout the study. The following parameters were evaluated: MS volume (MSV), MS surface (MSS), linear maximum width (LMW), linear maximum depth (LMD) and linear maximum height (LMH). All the parameters were calculated by Mimics ResearchTM software version 21.0 (NV, Technologielaan 15, 3001 Leuven, Belgium). A cephalometric tracing has been performed for each subject to evaluate the association between craniofacial features and maxillary sinus characteristics.
CBCT examination and data processing
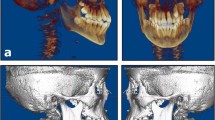
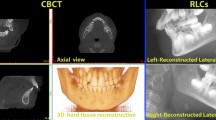
All patients received a CBCT scan using the same machine, I-CAT FLX (Imaging Sciences International, Hatfield, PA, USA). The scanning parameters were configured as follows: a 360° rotation, 300 frames, 120 kV[p], 5 mA, 3.7 s, a voxel size of 0.3 mm and one of the three field of view (FOV) 20 mm × 17 mm, 16 mm × 8 mm and 16 mm × 11 mm. The field of view was tailored for each patient to minimize radiation exposure, with a distance between the 2 slices of 0.3 mm to ensure anatomic registration accuracy. The scans were taken by one expert operator that used three position aids to correctly place the patient into natural head position and registered in the DICOM (Digital Imaging and Communications in Medicine)format. The CBCT scans were then loaded into Mimics Research™ v.16 software (NV, Technologielaan 15, 3001 Leuven, Belgium, https://www.materialise.com/en/medical/mimics-innovation-suite/mimics) to perform all the assessments.
A specific threshold was set for each MSV calculation. The threshold limits were from a minimum of − 1024 HU (minimum) to a maximum of − 526 HU (Fig. 1), as reported by Sahlstrand-Johnson et al.26.

Thresholding function of the Mimics Research™ v.16 software (NV, Technologielaan 15, 3001 Leuven, Belgium, https://www.materialise.com/en/medical/mimics-innovation-suite/mimics) was used to segment each MS: from − 1024 HU (minimum) to − 526 HU.
Using a software tool of Mimics Research known as, “edit masks,” according to a procedure already validated by Maspero et al.16 and Motro and Erverdi27, each MS was cropped along the borders, and at the level of the smallest tract of the hiatus between the processus uncinatus and the infundibulum. The segmentation tools of Materialise Mimics were used to crop the hiatus of the MS slice by slice (Fig. 2). The function “calculate 3D” was used to calculate MSV16,27 (Fig. 3).

The region growing tool was used to separate and isolate MSs using Mimics Research™ v.16 software (NV, Technologielaan 15, 3001 Leuven, Belgium, https://www.materialise.com/en/medical/mimics-innovation-suite/mimics).

Measurements of the MSs automatically generated by Mimics Research™ v.16 software (NV, Technologielaan 15, 3001 Leuven, Belgium, https://www.materialise.com/en/medical/mimics-innovation-suite/mimics).
After segmentation, the 3D volumetric structure of the MSV (right and left) of each patient was calculated separately. Flood-fill and smoothing operations were applied to the airway mask to calculate the total volume, whatever the porosity in the MSV. The volume and surface of the selected structures was then calculated by the software Mimics™. Lastly, the LMW, the LMH and the LMD parameters were automatically calculated by the Mimics Research™ software.
As regard to the correlation analysis, 11 craniofacial measurements (6 linear and 5 angular) were traced on the CBCT scans, using Mimics Research™ software, to evaluate their relationship with the MSV, MSS and LMW, LMH and the LMD. Figure 4 summarized the cephalometric points used in the present study. The cephalometric measurements used in this study are reported in Table 1.

Cephalometric landmarks used in the present study were: S = Sella (centre of sella turcica); N = Nasion (most anterior limit of the frontonasal suture on the frontal bone in the facial midline); Ba = Basion (The most anterior point of the foramen magnum); ANS = Anterior nasal spine (the tip of the anterior nasal spine); PNS = Posterior nasal spine (the most posterior point on the bony hard palate); A = Point A of Downs (Deepest bony point on the contour of the premaxilla below ANS); B = Point B of Downs (Deepest bony point of the contour of the mandible above pogonion); Me = Menton (most inferior point of mandibular symphysis); GO l/r = left/right Gonion points (located at the most posterior inferior point of the gonial angle of the mandible); MX l/r = left/right maxillare (the deepest point of the concavity formed by the lateral wall of the maxilla and the inferior border of the zygomatic process of the maxilla).
Statistical analysis
A preliminary analysis of the sample size power was carried out using G*Power (version 3.1.9, http://www.psychologie.hhu.de/arbeitsgruppen/allgemeine-psychologie-und-arbeitspsychologie/gpower.html) on 30 subjects (10 for each skeletal class); power calculation analysis was performed using the average values of the MSV for each skeletal class, the number of subjects analyzed for each group and the common standard deviation. The following data were used to calculate sample size: MSV skeletal class I = 13,339, skeletal class II = 12,632, skeletal class III = 14,924; group size = 10; σ within each group = 2460; α = 0.05; with a beta error level of 20%. Sixty-nine subjects (23 in each group) would have provided 80% power. However, according to the inclusion criteria, the authors could include 31 patients per group, thus increasing the robustness of the data. Statistics were carried out by the software SPSS v. 25.0 (IBM, Chicago, IL, USA). The Kolmogorov–Smirnov test was used to assess whether the data was normally distributed if the dataset was greater or equal to 50. It was observed that the statistical distribution of the quantitative measurements was Gaussian. Each measurement was reported as mean and standard deviation. The dimensional variations between the right and left MSV, MSS, LMW, LMH and LMD of the MS in the male and female group were analyzed. Statistically significant differences between the left and right sides in each measurement were computed by paired Student's t test.
After ensuring that the right and the left maxillary sinuses were not statistically significant different, the average values between the two sides were used for the following statistical analysis. After testing necessary assumptions, normality assessment in all the subgroups of each variable (via Shapiro–Wilk test) and homogeneity of the variances of the dependent variables in all the evaluated subgroups (via Levene’s statistics), a two-way analysis of variance (ANOVA) was used to test the influence of two different categorical independent variables, which were gender and skeletal malocclusion, on one dependent variable represented by MSV, MSS, LMW, LMH and LMD. The ANOVA was also calculated to assess the influence of gender and maxillary prognathism had on MSV, MSS, LMW, LMH and LMD.
The ANOVA test was also used to assess whether there was any interaction between the two-independent variables. The post hoc Sheffe’s test was used for within-group comparisons. Pearson’s correlation analysis was computed to investigate for any association between MSV, MSS, LMW, LMH and LMD and craniofacial morphological measurements. Intra-class correlation coefficient (ICC) was used to assess intra-examiner reliability the whilst the Dahlberg’s formula to measure the method error28.
Concerning the method error, all the maxillary and cephalometric measurements were obtained by a single expert orthodontist (A.A.) specialized in 3D radiologic imaging. After two weeks, 30 randomly selected CBCT were evaluated by a different expert orthodontist (D.C.), and then recalculated by A. A. to assess the intra-observer and inter-observer reliability. Both A.A. and D.C. were blinded to the patients’ identity and processed one scan per day to prevent fatigue errors.
Statistical significance was defined at a p-value < 0.05.
Ethical approval and consent to participate
The study protocol was approved by the Ethical Committee of the Fondazione IRCCS Ca’Granda, Ospedale Maggiore, Milan—Italy (protocol n.573/15). All procedures performed in this retrospective study involving human participants were in accordance with the ethical standards of the institutional and/or research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
For this type of study, informed consent was obtained from all parents’ patients or their guardians.
Results
Mean, standard deviation of the considered variables (MSV, MSS, LMH, LMW and LMD) and their comparison using paired t-test between the two sides and independent t test between gender are reported in Table 2. MSV, MSS, LMW, LMH and LMD did not show any statistically meaningful difference between the right and left side in the male and female groups. Whilst there was a statistically meaningful difference between genders for each variable evaluated. (Table 2).
The influence of skeletal class (ANB) and gender on MS dimension
Table 3 reports the results as to the influence the anteroposterior skeletal class ANB and gender had on the maxillary sinus.
The ANOVA test showed did not find any statistically significant result between the MSV and MSS in the three skeletal classes (ANB) group. A significant difference (p-value < 0.05) was observed between males and females for the same variables.
There was a statistically significant difference in LMW (p-value < 0.05) between the three skeletal class groups and between males and females. Skeletal classes I had a bigger LMW than class III and class II, the latter showed a shorter LMW than skeletal class III (Fig. 5).

The plot of the mean LMW measurements for each combination of groups of Gender and ANB are plotted in a line graph.
Although no statistically significant difference was observed for LMH in the three skeletal classes, there was a significantly bigger LMH in the male subjects (p-value < 0.05). There was no statistically significant difference in the LMD in the three skeletal classes and between genders.
The influence the cranio-maxillary relationship (SNA) and gender have on MS dimension
Table 4 reports the results of the influence the cranio-maxillary relationship (SNA) and gender have on the maxillary sinus. The ANOVA test evidenced a statistically significant difference (p-value < 0.05) between the MSV and MSS in the three horizontal prognathism of the maxillary alveolar bone (SNA) group. Patients with retrusive (SNA < 80°) and protrusive (SNA > 84°) maxilla had a larger MSV and surface than did subjects with normal cranio-maxillary relationships (SNA 82 ± 2°).
Males and females did not present any statistically significant difference for the same variables.
The LMW and LMH values were superimposable. There was a statistically significant difference (p-value < 0.05) in both these variables between the three cranio-maxillary relationship groups. Patients with retrusive (SNA < 80°) and protrusive (SNA > 84°) maxilla had a significant increase of the LMW and LMH (p-value < 0.05) than subjects with normal cranio-maxillary relationships (SNA 82 ± 2°). For the same variables a statistically significant differences were observed between males and females (Table 4). Moreover, the ANOVA test evidenced a statistically significant interaction (p-value < 0.05) between the two independent variables (SNA; Gender; see Fig. 6a,b). There was a statistically significant difference in linear maximum depth (LMD) (p-value < 0.05) between the three SNA group. Both the retrusive and protrusive group had significantly larger LMD (p-value < 0.05) than patients with normal SNA (Table 4). No significant difference was observed between gender for the same variable. A significant interaction (p-value < 0.05) between the two independent variables (SNA; Gender) was also noted (Fig. 6c).

The plots of respectively the mean LMW (A), LMH (B), LMD (C) measurements for each combination of groups of Gender and SNA are plotted in a line graph.
The simple main effect analysis revealed the different behavior of LMW, LMH and LMD in the SNA classes among gender groups (see Table 5). In males LMW was significantly higher in the retrusive group compared to normal and to protrusive groups, LMH and LMD were significantly lower in the normal group compared to the retrusive and to the protrusive groups. In females LMW was greater in the normal group compared to the retrusive group and was greater in the protrusive group compared to normal and to retrusive group. LMH was higher in the protrusive and normotrusive groups. LMD was greater in the retrusive group compared to normal group. The simple main effect analysis revealed the different behavior of LMW, LMH and LMD in the gender groups among SNA classes (see Table 6). In the retrusive group of LMW and LMH males showed statistically significant higher values compared to female subjects whereas the opposite occurred in the normotrusive group of LMD variable.
The correlation analysis between cephalometric values and MS dimension
Pearson’s correlation coefficients between the dimensions of the MS and craniofacial cephalometric variables are reported in Table 7. There was a medium to high positive correlation with S-N, PNS-A, Mx r-Mx l, S-Go, N-Me and N-Ans variables. MSS evidenced a significant positive correlation with S-N, Pns-A and Mx r-Mx l, N-Me and N-Ans variables. A significant negative correlation was observed between the LMW, Ba-S^-N and N-Me and there was a statistically significant positive correlation with Mx r-Mx L. There was a significant positive correlation in LMH for the following variables: S-N, S-N-Ans-Pns, N-Me, N-Ans. Whilst there was a significant negative correlation between LMH and Ba-S-N, S-Go and Mx r-Mx l. A significant positive correlation was observed between the LMD and S-N, Ba-S-N, PNS-A, S-Go and Mx r-Mx l. Furthermore, LMD was negatively correlated to N-Me and N-Ans.
The average intra-observer and inter-observer ICC (average ± SD, range) scored high: 0.975 ± 0.012, 0.946–0.993 and 0.963 ± 0.016, 0.934–0.982 respectively. According to Dahlberg’s formula, the random error for sinus volumetric and linear measurements was 446 mm3 for the MSV, 112 mm3 for the MSS and about 0.67 mm for the linear measurements. The random error for cephalometric measurements was about 0.48 mm for linear measurements and 0.23° for the angular.
Discussion
Various papers have looked into MS morphometry and MS volumetric changes in relation to several conditions, i.e., different orthodontic appliances, nasal septum deviation, and sinus pathologies29,30,31. Koppe et al.32 took into consideration the MSV and the characteristics of the maxilla-facial skeleton of adults with an untreated bilateral cleft and negative control patients and reported that bigger skulls had greater MSs and that cleft patients had larger paranasal sinuses than the control subjects. On the contrary, Erdur et al.33 found that MSs of unilateral cleft patients had no statistically significant difference between sides. Other studies also evaluated the relationship between MS size with gender and age29,30,31.
Nevertheless, to the best of authors’ knowledge, the present study is the first human CBCT investigation to make a 3D analysis of the volume, surface and linear maximum width depth and height of the MS and to compare these data between three different skeletal classes, evaluating the relationship between the shape of the maxillary sinuses and the patients’ craniofacial features in adult subjects. Bidimensional orthopantomography and lateral cephalogram presents several shortcomings in assessing three dimensional structures as already investigated in literature. Every clinician with some experience with OPG knows that even in the same patient the surface of the maxillary sinuses may vary greatly because it is strictly dependent on the inclination of the head to the x-ray beam that causes different projection on the 2D sensor of two pyramid shape volumes with a particular orientation inside the maxilla.
All papers but one investigated the surface of maxillary sinuses on bidimensional radiographs therefore providing inaccurate data and making their conclusions almost worthless.
The only other study34 that investigated the three-dimensional volume of maxillary sinuses and its correlation to cephalometric indexes was published last year. Our study aimed at giving more information on correlations between cephalometric indexes and maxillary sinuses dimensions taking into account gender differences as it was not considered in the previous publication.
The data obtained in this study evidenced no significant difference for MSV, MSS, LMW, LMH and LMD between the right and left side, demonstrating the absence of asymmetry in the MS in the present sample.
A statistically significant difference was registered between genders for the MS with males having a larger sinus than females for each variable evaluated. One paper35 described that the maxillary sinus volume continued to grow until 20 years of age and then began reducing its size and their findings were in line with those in this study, in as much as they reported no significant difference between the right and left MSVs (Table 2).
The data of the present study showed no significant difference between the three skeletal class (ANB) group for the MSV and surface, evidencing no association between these variables and the anteroposterior relationship. There was a larger volume and surface in males than in females, in contrast with previously published literature data, i.e., Endo et al.22 reported having observed no statically significant differences in the maxillary morphological measurements between genders. Oktay’s study used the Duncan’s multiple comparison test to determine the size of maxillary sinuses and reported that that Class I female subjects and Class II and III male subjects had smaller MS than Class II female subjects1. The differences in these two results may be attributable to age dependent development of the MS.
Oktay analyzed 189 patients aged between 6 and 30 years, whereas Endo et al.22 included males and females of almost the same age. However, Oktay1 and Endo22 using bi-dimensional OPGs evaluated significantly distorted images of maxillary sinuses, with huge limitations in the methods which might well have hampered the interpretation of their findings, whilst the CBCT scans evaluated in this paper were significantly more accurate for MS three dimensional measurements.
Regarding linear measurements of the MS only LMW showed a statistically significant difference in ANB groups resulting larger in class I patients compared with class II and III (Table 3).
This is allegedly due to the association between class II and III malocclusion and maxillary hypoplasia that would reveal a reduced LMW. Various studies have reported that the anteroposterior and vertical problems related to Class II and III malocclusions are not the only related factors and that there is often an association with posterior transverse discrepancy36,37,38,39.
Class II and class III patients presented a reduced transversal dimension of the MS that had never been reported before in literature. This finding is strengthened by the Pearson’s correlation coefficients of the distance between the left and right Mx points with MSV, MSS and LMW that evidenced very high positive correlation (p-value < 0.01), as reported in Table 7.
Moreover, it was observed that females had a smaller LMW and LMH than males. No statistically significant interaction was noted for MS variables between gender and skeletal classes, with a similar trend for the MSV and MSS in the three SNA classes. This finding is inconsistent with those published by Oktay1 who evaluated the MS areas on OPGs of patients with different dental malocclusions defined according to Angle classification. Oktay1 found a significant interaction between gender and Angle’s class in the dimensions of the MS.
Differently from other previous research, the authors decided to make a 3D investigation assessing the influence that the cranio-maxillary relationship (SNA) may have on MS dimension. The authors supposed that the cranio-maxillary relationship (SNA) would have influenced maxillary sinuses size more than the sagittal skeletal jaw relationship (ANB).
The data of the present study showed that subjects with a retrusion (SNA < 80°) and protrusion (SNA > 84°) of the maxillary bone had a significant increase in MSV, MSS, LMW, LMH and LMD. Whilst there was no difference between genders for MSV, MSS and LMD. Conversely, males had larger LMW and LMH.
However, the data of the present study as to the relationship between SNA and MS dimensions cannot be compared to other research data as, to the best of authors’ knowledge, this is the first time this has been calculated. Interestingly, the evaluation of the significant interaction between the SNA classes and gender demonstrated a different tendency for the three linear variables between genders (Table 4).
The statistical interaction between SNA and LMW evidenced that females with a maxillary retrusion had smaller transversal sinus dimensions than males with the same condition. Conversely, males with maxillary protrusion (SNA > 84°) had smaller LMW than females.
The significant LMH findings on the interaction between SNA and gender evidenced that there was a different pattern for the two genders, i.e., in subjects with a reduced SNA, females presented smaller MS than males. A statistically significant interaction was found for LMD in subjects with normal SNA values. Whilst males presented significantly smaller LMD in subjects with normal SNA values compared with the other two subgroups, the female groups presented similar values for LMD in patients with normal or augmented SNA values and increased values of LMD in patients presenting reduced SNA values.
Several cephalometric measurements presented a positive correlation with the dimensions of the MS. These data allegedly sustain the hypothesis for the MS to be larger in patients presenting larger maxillofacial structures. Another study32 similarly reported that the MSV was positively correlated to the dimensions of the maxillofacial structures. This finding was in line with the data of the present study, even if Koppe et al.31 considered just three cephalometric parameters, that are the distance between the Mx points, facial height, and maxillary length.
The presented data did not evidenced any significant correlation between the SNA, SNB, and ANB angles and any MS size. This finding suggested that the anteroposterior dimension of the maxilla and of the mandible had neither a positive nor a negative correlation on MS size, although the ANB and SNA angles are both the criteria for the classification of the analyzed subjects (Table 7). These findings were in agreement with those previously published by Endo et al.21 who did not report any significant correlation between SNA, SNB and ANB angles and MS dimension. The abscence of a significant correlation between SNA and all the maxillary measurments is due to a V shape distribution of data between the SNA classes, with greater maxillary values in subjects with a retrusion and protusion of the maxillary bone.
Individuals with bigger S-N and PNS-A distances did tend to present larger MS. The correlation analysis of the MS measurements and the cranial base showed a positive correlation between S-N distance and MSV, MSS and LMD. Moreover, the significant positive correlation between the Ba-S-N angle and the LMD demonstrated that the angle increased along with the increase in depth. Conversely, the height and width were negatively correlated with the Ba-S-N angle. The data presented in this paper regarding Pearson’s correlation analysis between MS dimensions and PNS-A distance are in line with the one reported by Endo et al.22, that is subjects with longer nasomaxillary complexes have deeper and greater sinus, in terms of volume and surface. To understand this relationship we should consider that the MS, a pyramid-shaped sinus within the maxillary bone, is the biggest among paranasal sinuses40,41 as previously mentioned, contributing to midfacial growth and appearance22,42,43.
Endo et al.22 also reported a strong positive correlation between total maxillary sinus area (TMSA) and upper maxillary sinus area (UMSA) and S-N-Ans-Pns, showing a tendency for steeper maxillary planes to be positevely related with TMSA and UMSA. The results of the current research differ from those of Endo et al. as no relationship was observed between the inclination of the palatal plane (S-N/Ans-Pns) and the MS dimension and only the maximum height (LMH) had a statistically significant positive correlation with S-N-Ans-Pns.
The present correlation analysis between the vertical dimension and the MS measurements showed that patients with an augmented anterior vertical dimension should have larger MSV, MSS and greater LMH, and the subjects with a higher posterior facial height should have larger MSV, in accordance with data published by Endo et al.22. However, data comparison is not reliable as those previously published by Endo et al. were calculated on subjects aged from 12 to 16, a period when the maxillary size could be affected by a peak of growth.
Most of the studies are limited to the evaluation of the sinuses during orthodontic treatment or for a particular malocclusion and are impaired by bidimensional biases as well.
The present study aimed at obtaining information on the three-dimensional characteristics of maxillary sinuses amongst nasal breathing adults that had not been given any orthodontic treatment and evaluating the relationship that different cephalometric measurements may have on MSV and MSS, in both genders. However, this study does have some limitations, i.e., the relatively small sample size, even if it did suffice for inferential statistics consideration and the fact that all the subjects were Caucasian. Therefore, the conclusions may not be extrapolated to other ethnicities. Furthermore, the use of SNA and ANB are not completely reliable to investigate skeletal pattern. The literature teaches us that none of the sagittal parameters proposed so far can be considered totally reliable. It often happens that two parameters are conflicting or over or underestimate the actual skeletal discrepancy. The SNA and the ANB angle are parameters commonly used for evaluating the sagittal relationship between the maxilla and the cranial base and between the maxilla and the mandible respectively. The ANB angle would tend to decrease with increasing age44,45 and is influenced by the position of the nasion point: both on the sagittal plane and on the vertical plane46,47,48,49.
As reported by previous studies it seems that the growth of the MS in both genders overlaps with the pubertal growth spurt, and that its development starts between the age of 9 and 11 in females and later in males, between 12 and 1416. However, one strong point of this study is the average age of the selected sample, as it ensures a three-dimensional evaluation of the MS in an age range that is no longer subject to any significant volumetric changes. Moreover, the excellent intra-operator and inter-operator agreement (Table 7) demonstrated a very high reliability and repeatability of the presented method and a very small random error for volumetric and linear measurements in the assessment of MS size. The data of the present study are in line with various other authors who demonstrated the reliability and utility of CBCT scans in a three-dimensional assessment and reconstruction of the paranasal and maxillary sinus16,17,50.
The maxillary sinuses are of particular interest in dentistry due to their proximity to the area dentists work in. Therefore, thorough knowledge of MS anatomy is a must to avoid not only maxillofacial surgery complications, but also to make a presurgical evaluation for dental implant planning, graft size estimation for sinus lift procedures and infra-zigomatic mini-screw placement. Besides common dental procedure, the study of the MS is important in forensics to determine the gender if the whole body is not be available51. In case of orthodontic treatment that includes movements of the posterior teeth at the level of the maxillary sinus, the clinician should have a special care in patients with a large dimension of the maxillary sinus(as in case of an augmented vertical dimension). Literature reports that orthodontic space closure in missing posterior maxillary teeth through the sinus is arduous and it is recommended to use light force systems for a successful effect52,53. Moreover intrusion of teeth located in posterior area associated with root apices protruding into the maxillary sinus may be difficult and slow and it also need for very slight forces54,55.
The observations made in this study as to the orthodontic malocclusions seem to be in contrast with those put forward by Sassouni and Forrest56, i.e., that sinuses do not have a bearing on facial balance and malocclusions. A more thorough knowledge of three-dimensional MS dimension in different malocclusions may well be of help in treatment planning, as it has a common relationship with patients’ craniofacial features. However, all this considered and despite the efforts, the authors encourage these preliminary results be taken with caution as no clear-cut evidence is yet available in literature as to the influence cephalometric indices and/or malocclusive traits have on MS morphology. Moreover, even if present, statistical significance does not mean clinical relevance or the presence of cause/effect relationships between the variables. Indeed, statistical significance may have several confounding factors related to sample selection or sample pooling. Therefore, the authors urge the scientific community to carry out further studies on larger samples and to investigate further into any differences between populations to enrich and hopefully confirm the findings herein.
Conclusions
In conclusion, this study demonstrated statistically significant larger volumes in males than in females. There was also a significant reduction in the transverse dimension of the MS in subjects with skeletal class II and III malocclusion. Subjects with a retrusion or protusion of the maxillary alveolar bone had larger MSV, MSS, LMW, LMH and LMD than subjects with a normal cranio-maxillary relationship. A significant interaction was observed for LMW, LMH and LMD measurements, demonstrating a different pattern between genders. A statistically significant high positive correlation was observed between S-N, Pns-A, S-Go, Mx-R/Mx-r and MS dimension. Whilst no significant correlation was noted between the MS measurements and anteroposterior skeletal classes (ANB) and the cranio-maxillary relationship (SNA).
Data availability
The data underlying this article will be shared on reasonable request to the corresponding author.
References
Oktay, H. The study of the maxillary sinus areas in different orthodontic malocclusions. Am. J. Orthod. Dentofac. Orthop. 102, 143–145 (1992).
Scuderi, A. J., Harnsberger, H. R. & Boyer, R. S. Pneumatization of the paranasal sinuses: normal features of importance to the accurate interpretation of CT scans and MR images. Am. J. Roentgenol. 160, 1101–1104 (1993).
Livas, C. et al. Maxillary sinus floor extension and posterior tooth inclination in adolescent patients with Class II. Division 1 malocclusion treated with maxillary first molar extractions. Am. J. Orthod. Dentofac. Orthop. 143, 479–485 (2013).
Tikku, T., Khanna, R., Sachan, K., Srivastava, K. & Munjal, N. Dimensional changes in maxillary sinus of mouth breathers. J. Oral Biol. Craniofacial Res. 3, 9–14 (2013).
Maresh, M. M. & Washburn, A. H. Paranasal sinuses from birth to late adolescence: II. clinical and roentgenographic evidence of infection. Am. J. Dis. Child. 60, 841–861 (1940).
Koymen, R. et al. Anatomic evaluation of maxillary sinus septa: Surgery and radiology. Clin. Anat. 22, 563–570 (2009).
Uchida, Y., Goto, M., Katsuki, T. & Akiyoshi, T. A cadaveric study of maxillary sinus size as an aid in bone grafting of the maxillary sinus floor. J. Oral Maxillofac. Surg. 56, 1158–1163 (1998).
Kanthem, R. K., Guttikonda, V. R., Yeluri, S. & Kumari, G. Sex determination using maxillary sinus. J. Forensic Dent. Sci. 7, 163–167 (2015).
Lanteri, V. et al. Volumetric changes in the upper airways after rapid and slow maxillary expansion in growing patients: A case-control study. Material. 13, 10 (2020).
De Vos, W., Casselman, J. & Swennen, G. R. J. Cone-beam computerized tomography (CBCT) imaging of the oral and maxillofacial region: A systematic review of the literature. Int. J. Oral Maxillofac. Surg. https://doi.org/10.1016/j.ijom.2009.02.028 (2009).
Nascimento, H. A. R. et al. Dosimetry in CBCT with different protocols: Emphasis on small FOVs including exams for TMJ. Braz. Dent. J. 28, 511–516 (2017).
Maspero, C., Farronato, M., Bellincioni, F., Cavagnetto, D. & Abate, A. Assessing mandibular body changes in growing subjects: A comparison of CBCT and reconstructed lateral cephalogram measurements. Sci. Rep. 10, 11722 (2020).
Abate, A. et al. A CBCT based analysis of the correlation between volumetric morphology of the frontal sinuses and the facial growth pattern in Caucasian subjects: A cross-sectional study. Head Face Med. 18, 4 (2022).
Panou, E., Motro, M., Ateş, M., Acar, A. & Erverdi, N. Dimensional changes of maxillary sinuses and pharyngeal airway in Class III patients undergoing bimaxillary orthognathic surgery. Angle Orthod. 83, 824–831 (2013).
Favato, M. N. et al. Impact of human maxillary sinus volume on grafts dimensional changes used in maxillary sinus augmentation: A multislice tomographic study. Clin. Oral Implants Res. 26, 1450–1455 (2015).
Maspero, C. et al. Three-dimensional evaluation of maxillary sinus changes in growing subjects: A retrospective cross-sectional study. Materials. 13, 1007 (2020).
AktunaBelgin, C., Colak, M., Adiguzel, O., Akkus, Z. & Orhan, K. Three-dimensional evaluation of maxillary sinus volume in different age and sex groups using CBCT. Eur. Arch. Oto-Rhino-Laryngol. 276, 1493–1499 (2019).
Pamporakis, P., Nevzatoğlu, Ş & Küçükkeleş, N. Three-dimensional alterations in pharyngeal airway and maxillary sinus volumes in Class III maxillary deficiency subjects undergoing orthopedic facemask treatment. Angle Orthod. 84, 701–707 (2014).
Kim, Y.-J., Shin, H.-K., Lee, D.-Y., Ryu, J.-J. & Kim, T. H. Decreased maxillary sinus volume is a potential predictor of obstructive sleep apnea. Angle Orthod. 90, 556–563 (2020).
Erdur, E. A., Yıldırım, M., Karatas, R. M. C. & Akin, M. Effects of symmetric and asymmetric rapid maxillary expansion treatments on pharyngeal airway and sinus volume. Angle Orthod. 90, 425–431 (2020).
Basdra, E. K., Stellzig, A. & Komposch, G. The importance of the maxillary sinuses in facial development: A case report. Eur. J. Orthod. 20, 1–4 (1998).
Endo, T. et al. Cephalometric evaluation of maxillary sinus sizes in different malocclusion classes. Odontology 98, 65–72 (2010).
Park, I.-H. et al. Volumetric study in the development of paranasal sinuses by CT imaging in Asian: A pilot study. Int. J. Pediatr. Otorhinolaryngol. 74, 1347–1350 (2010).
Riedel, R. The relation of maxillary structures to cranium in malocclusion and in normal occlusion. Angle Orthod https://doi.org/10.1043/0003-3219(1952)022%3c0142:TROMST%3e2.0.CO;2 (1952).
Downs, W. B. Variations in facial relationships: Their significance in treatment and prognosis. Am. J. Orthod. https://doi.org/10.1016/0002-9416(48)90015-3 (1948).
Sahlstrand-Johnson, P., Jannert, M., Strömbeck, A. & Abul-Kasim, K. Computed tomography measurements of different dimensions of maxillary and frontal sinuses. BMC Med. Imaging 11, 8 (2011).
Motro, M. & Erverdi, N. 3 dimensional evaluation of maxillary sinuses after rapid maxillary expansion and following one year retention period. Clin. Exp. Heal. Sci. 2, 1–10 (2014).
Dhalberg, G. Statistical methods for medical and biological students. Br. Med. J. 2, 358 (1940).
Orhan, I. et al. Morphometric analysis of the maxillary sinus in patients with nasal septum deviation. Eur. Arch. Oto-Rhino-Laryngol. 271, 727–732 (2014).
Möhlhenrich, S. C. et al. Is the maxillary sinus really suitable in sex determination? A three-dimensional analysis of maxillary sinus volume and surface depending on sex and dentition. J. Craniofac. Surg. 26, e723–e726 (2015).
Cho, S. H. et al. Factors for maxillary sinus volume and craniofacial anatomical features in adults with chronic rhinosinusitis. Arch. Otolaryngol. Head. Neck Surg. 136, 610–615 (2010).
Koppe, T. et al. Maxillary sinus pneumatization of an adult skull with an untreated bilateral cleft palate. J. Cranio-Maxillo-Facial Surg. 34(Suppl 2), 91–95 (2006).
Erdur, O., Ucar, F. I., Sekerci, A. E., Celikoglu, M. & Buyuk, S. K. Maxillary sinus volumes of patients with unilateral cleft lip and palate. Int. J. Pediatr. Otorhinolaryngol. 79, 1741–1744 (2015).
Shrestha, B. et al. Evaluation of maxillary sinus volume in different craniofacial patterns: A CBCT study. Oral Radiol. 37, 647–652 (2021).
Ariji, Y., Kuroki, T., Moriguchi, S., Ariji, E. & Kanda, S. Age changes in the volume of the human maxillary sinus: A study using computed tomography. Dentomaxillofac. Radiol. 23, 163–168 (1994).
Baratieri, C., Alves, M. J., Bolognese, A. M., Nojima, M. C. G. & Nojima, L. I. Changes in skeletal and dental relationship in Class II division I malocclusion after rapid maxillary expansion: a prospective study. Dent. Press J. Orthod. 19, 75–81 (2014).
Tollaro, I., Baccetti, T., Franchi, L. & Tanasescu, C. D. Role of posterior transverse interarch discrepancy in Class II, Division 1 malocclusion during the mixed dentition phase. Am. J. Orthod. Dentofac. Orthop. 110, 417–422 (1996).
Franchi, L. & Baccetti, T. Transverse maxillary deficiency in Class II and Class III malocclusions: A cephalometric and morphometric study on postero-anterior films. Orthod. Craniofac. Res. 8, 21–28 (2005).
Williams, S. & Andersen, C. E. The morphology of the potential Class III skeletal pattern in the growing child. Am. J. Orthod. 89, 302–311 (1986).
Emirzeoglu, M., Sahin, B., Bilgic, S., Celebi, M. & Uzun, A. Volumetric evaluation of the paranasal sinuses in normal subjects using computer tomography images: A stereological study. Auris Nasus Larynx 34, 191–195 (2007).
Graney, D. & Rice, D. Anatomy. In Otolaryngology: Head and Neck Surgery (eds Cummings, C. et al.) 901–906 (St Mosby Year Book, 1993).
Blanton, P. L. & Biggs, N. L. Eighteen hundred years of controversy: The paranasal sinuses. Am. J. Anat. 124, 135–147 (1969).
Alberti, P. W. Applied surgical anatomy of the maxillary sinus. Otolaryngol. Clin. North Am. 9, 3–20 (1976).
Bishara, S. E. Longitudinal cephalometric standards from 5 years of age to adulthood. Am. J. Orthod. 79, 35–44 (1981).
Jamison, J. E., Bishara, S. E., Peterson, L. C., DeKock, W. H. & Kremenak, C. R. Longitudinal changes in the maxilla and the maxillary-mandibular relationship between 8 and 17 years of age. Am. J. Orthod. 82, 217–230 (1982).
Taylor, C. M. Changes in the relationship of nasion, point A, and point B and the effect upon ANB. Am. J. Orthod. 56, 143–163 (1969).
Freeman, R. S. Adjusting A-N-B angles to reflect the effect of maxillary position. Angle Orthod. 51, 162–171 (1981).
Binder, R. E. The geometry of cephalometrics. J. Clin. Orthod. JCO 13, 258–263 (1979).
Farronato, M. et al. 3D cephalometry on reduced FOV CBCT: Skeletal class assessment through AF-BF on Frankfurt plane-validity and reliability through comparison with 2D measurements. Eur. Radiol. 30, 6295–6302 (2020).
Szabo, B. T. et al. Comparison of hand and semiautomatic tracing methods for creating maxillofacial artificial organs using sequences of computed tomography (CT) and cone beam computed tomography (CBCT) images. Int. J. Artif. Organs 40, 307–312 (2017).
Paknahad, M., Shahidi, S. & Zarei, Z. Sexual dimorphism of maxillary sinus dimensions using cone-beam computed tomography. J. Forensic Sci. 62, 395–398 (2017).
Park, J. H., Tai, K., Kanao, A. & Takagi, M. Space closure in the maxillary posterior area through the maxillary sinus. Am. J. Orthod. Dentofac. Orthop. 145, 95–102 (2014).
Oh, H. et al. Orthodontic tooth movement through the maxillary sinus in an adult with multiple missing teeth. Am. J. Orthod. Dentofac. Orthop. 146, 493–505 (2014).
Park, Y.-C., Lee, S.-Y., Kim, D.-H. & Jee, S.-H. Intrusion of posterior teeth using mini-screw implants. Am. J. Orthod. Dentofac. Orthop. 123, 690–694 (2003).
Ahn, N.-L. & Park, H.-S. Differences in distances between maxillary posterior root apices and the sinus floor according to skeletal pattern. Am. J. Orthod. Dentofac. Orthop. 152, 811–819 (2017).
Sassouni, V. & Forrest, E. J. Orthodontics in Dental Practice (St. CV Mosby. Co., 1971).
Funding
No specific funding was received from any funding bodies in the public, commercial or not-for-profit sectors to carry out the work described in this manuscript.
Author information
Authors and Affiliations
Contributions
Conceptualization. A.A., V.L., and C.M.; Methodology: A.A., D.C. and V.L; Investigation: A.A. and D.C.; Validation: A.A. and C.M.; Software, A.A., D.C. and V.L.; Formal Analysis: C.M.; Data Curation: A.A. and D.C.; Writing—Original Draft Preparation: A.A. and D.C.; Writing—Review and Editing: C.M., A.A., D.C., and V.L.; Supervision: C.M., and V.L. All authors have read and agreed to the published version of the manuscript. All authors equally contributed to this work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Abate, A., Cavagnetto, D., Lanteri, V. et al. Three-dimensional evaluation of the maxillary sinus in patients with different skeletal classes and cranio-maxillary relationships assessed with cone beam computed tomography. Sci Rep 13, 2098 (2023). https://doi.org/10.1038/s41598-023-29391-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-29391-5
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
