
Abstract
Several studies propose that Retinopathy of Prematurity (ROP) is a multifactorial disorder implicating many prenatal and postnatal factors. The objective of our study was to determine the incidence and the risk factors that influenced ROP development and progression. We retrospectively compiled data of preterms with birth weight (BW) ≤ 1.500 g and/or gestational age (GA) < 32 weeks, or BW between 1.501 and 2.000 g and/or GA ≥ 32 weeks with oxygen supply > 72 h or unstable clinical course screened for ROP in Regional University Hospital of Málaga from 2015 to 2018. 202 infants (44.7%) developed ROP and 66 exhibited progression (32.7% of ROP infants). In the univariate analysis, many risk factors were associated with ROP. In the subsequent multivariate analysis, GA, oxygen therapy and weight at 28 days of life, mechanical ventilation duration, non-invasive ventilation, surfactant administration and late-onset sepsis were independently associated with the development. However, oxygen therapy duration, late-onset sepsis and weight at 28 days were associated with the progression. The ROP development and progression risk factors were different. Our results are important to facilitate screening, early diagnosis and ROP treatment while reducing unneeded examinations.
Similar content being viewed by others

Introduction
Retinopathy of prematurity (ROP), first described in 1942 by Terry1, is a vasoproliferative disorder of the premature infants retina and one of the major causes of childhood blindness worldwide2.
The retinal vasculature development starts at gestation (16 weeks) and completes at term3. ROP is a two-stage disorder that begins with the retinal vessels arrest in preterm babies exposed to high oxygen levels at birth3. The successive hypoxia brings about the angiogenic growth factors upregulation and the neovascularization risk4.
With the advancement in the preterm infants survival rate, the number of babies with higher ROP risk has increased, so early detection and treatment are becoming essential. Eye examinations are planned according to gestational age (GA), birth weight (BW) and ROP stage5.
Numerous studies suggest that ROP is a multifactorial disease involving a lot of prenatal and postnatal factors6 but the results are often controversial and few studies have discerned the ROP development risk factors from those of ROP progression.
The aim of this study was to determine the potential risk factors of ROP and establish their influence in ROP development and progression in order to find out the reason why in certain cases ROP progresses and in others it shows improvement.
Methods
Ethical approval and informed consent
The present study was approved by the Biomedical Research Ethics Committee of Andalusia and was carried out in accordance with the ethical principles for medical research outlined in the Declaration of Helsinki. Therefore, all medical data collected anonymously prior informed consent.
Patient selection and study design
An observational retrospective study was conducted on 452 premature newborns who were examined between January 1, 2015 and December 31, 2018, at the level three Neonatal Intensive Care Unit (NICU) of the Regional University Hospital of Málaga (Spain).
Inclusion criteria were: BW ≤ 1.500 g and/or GA < 32 weeks, or BW between 1.501 and 2.000 g and/or GA ≥ 32 weeks with oxygen supply > 72 h or unstable clinical course as determined by the NICU neonatologist (apnea, neonatal acidosis, twin death, intraventricular hemorrhage, patent ductus arteriosus, sepsis, necrotizing enterocolitis or concurrent surgical interventions).
Participants were excluded from the study when they could not be examined until complete retinal vascularization, they presented severe systemic diseases, congenital anomalies or other ocular abnormalities that could affect ROP development or progression, died before eye examination or had incomplete medical data.
Patient exam
All patients were examined under pharmacological mydriasis and topical anaesthesia by the same pediatric ophthalmology team using indirect ophthalmoscopy with indentation and a 20 diopter lens5. The RetCam Imaging System III (Clarity Medical Systems, Pleasanton, CA) was used to control the disease and treatment response5.
The infants were first examined at 4 to 6 weeks after birth. Subsequently, routine re-examination was performed every week depending on the retinal findings5. ROP was classified according to the International Classification of Retinopathy of Prematurity7, including the stage, zone and presence or absence of plus disease. ROP development was defined as the occurrence of any stage of ROP, and ROP progression was defined as prethreshold ROP or type-1 ROP (zone I, any stage ROP with plus disease, or zone I, stage 3 ROP without plus disease, or zone II, stage 2 or 3 ROP with plus disease), Threshold ROP (at least 5 contiguous clock-hours of extraretinal neovascularization or 8 cumulative clock-hours of extraretinal neovascularization in association with plus disease and location of the retinal vessels within zone I or II) or Aggressive Posterior ROP (AP-ROP) (vascularization ends in zone I or very posterior zone II and is accompanied by plus disease); treated conforming to Spanish ROP protocol8. The most advanced ROP stage recorded was assigned to each infant, without ROP differences between eyes. All patients were followed up until full retina vascularization5.
We considered 55 potential risk factors that may influence ROP and they were divided into birth, maternal, neonatal, hospitalization and ophthalmological factors. The full list of factors evaluated is given in Table 1.
These variables were defined with regard to the criteria established by the Vermont Oxford working group9. Sepsis was defined as sepsis clinical signs and/or suggestive laboratory test results with a confirmatory blood culture, either early (in the first 72 h of life) or late (after the first 72 h of life).
Statistical analysis
The enrolled neonates were divided into two subgroups: neonates who developed ROP or those who did not. Neonates who developed ROP were subsequently divided into: neonates who showed ROP progression or those who did not. To identify risk factors, each one was initially analysed by univariate analysis. The Pearson χ2 test and the T student test were used for categorical and numerical variables, respectively. Numerical variables were expressed as means ± standard deviation and categorical variables as absolute and relative frequencies.
Multivariate analysis using tree-building algorithms was then performed to identify the independent risk factors for ROP development and progression. Firstly, risk factors were divided into several groups (oxygen, ventilation, nutrition, anemia, comorbidities, resuscitation, ophthalmological factors and respiratory disease) and tree-building algorithm multivariate analysis was done. Secondly, we repeated the analysis including only the significative variables that we obtained in the previous analysis. Progression analysis was performed exclusively on patients who develop ROP.
All analyses were performed using the Statistical Package for Social Sciences (SPSS software version 25.0 (IBM Corp., Armonk, NY, USA). Statistically significance was defined as a p value < 0.05.
Results
Demographic characteristics
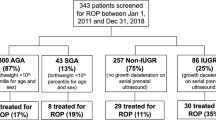
A total of 620 premature newborns were screened, of which 168 were excluded because they not meet the inclusion criteria (Fig. 1). The diagnoses of the 11 patients excluded due to ocular or systemic diseases were: 1 Down syndrome, 1 maternal human immunodeficiency virus infection, 1 congenital syphilis, 2 congenital cataracts that underwent surgery, 1 cystic fibrosis, 1 absent septum pellucidum, 1 fetal umbilical-porta-systemic venous shunt, 1 nephromegaly, 1 aorta coarctation. The mean GA at birth was 29.38 ± 2.53 weeks, the mean BW was 1187.19 ± 322.27 g, and the sex distribution was 228 (50.4%) males and 224 (49.6%) females.

Flow diagram of the study. The chart on the left of the figure shows the exclusion reasons by year.
ROP characteristics
Of the 452 newborns ultimately included in the study, 202 (44.7%) developed ROP: 24 had zone I disease, 169 had zone II disease, and 9 had zone III disease; 45 had stage 1 (22.3%), 120 had stage 2 (59.4%), 33 had stage 3 (16.3%), 4 had stage 4 (2%). None of the neonates presented ROP at stage 5. AP-ROP was detected in 29 infants (14.4%).
Among the 202 infants that developed ROP, 66 progressed to ROP requiring treatment (14.6% of all of screened newborns and 32.7% of ROP developed newborns). There were 57 (12.6%) babies who underwent ROP treatment (14 intravitreal anti-VEGF, 33 laser photocoagulation therapy and 10 needed both treatments). The remaining 9 patients didn’t need treatment due to spontaneous improvement of retinopathy in ophthalmological exam. Table 2 shows the rates of ROP development and progression, AP-ROP and treatment of the time lapse under research.
Univariate analysis for ROP development and progression
After univariate analysis, various factors were identified as significant risk factors for ROP development and progression (Tables 3, 4 and 5). There were no differences in sex, race, fetal heart rate, early sepsis, phototherapy, IVF, maternal age, maternal hypertensive stages, GDM, gestation, mode of delivery, antenatal steroid therapy and PVL for ROP development and progression. In addition to, no differences were found in GA and weight at ROP maximum stage for ROP progression.
Multivariate analysis for ROP development and progression
All the significant variables obtained in the different groups trees exposed previously were included in the following tree algorithm for ROP development (Fig. 2) (GA, oxygen at 28 days of life, NIV, MV duration, BW, weight at 28 days of life, late-onset sepsis, CMV, treatment for CMV, NEC, hypotension, intubation, steroids for BDP, apneas, surfactant administration, IVH and anemia) and progression (Fig. 3) (duration of oxygen therapy, nasal high-flow therapy, HFOV, weight at 28 days of life, late-onset sepsis, ROM, weight at ROP diagnosis, hypotension, PDA, intubation, steroids for BDP, surfactant administration, IVH and anemia).

Tree algorithm for ROP development. GA gestational Age (weeks), MV mechanical Ventilation, NIV non-invasive ventilation. *p < 0.005.

Tree algorithm for ROP progression. *p < 0.005.
Final multivariate analysis with the significative risk factors of each group for ROP development (Fig. 2) evidenced that the GA have the strongest influence on the development of ROP; increasing the risk of ROP development as the GA decreases. In those patients with GA between 25–27 weeks the need of supplemental oxygen therapy increases the ROP development risk to 94.4%, and it reaches 100% in those babies who need more than 3 days of MV. In preterms with 27–28 weeks of GA, surfactant administration decreases the risk of ROP development until 56.5% and in those with 28–29 weeks of GA the late-onset sepsis increases ROP risk (69.6%). However, in GA > 29 weeks group, the weight at 28 days of life is the risk factor that firstly influence on the development, showing lower risk those with more than 1660 g, with an increased risk of ROP if they need NIV.
Final multivariate analysis with the significative risk factors of each group for ROP progression (Fig. 3) demonstrated that the supplemental oxygen therapy duration has the strongest influence on the progression of ROP; increasing the ROP progression risk as the number of days of oxygen increases. In preterms who need oxygen between 2–48 days, the late-onset sepsis diagnosis increases the risk of ROP progression to 28.9%. In preterms who need oxygen more than 99 days with ≤ 975 g of weight at 28 days of life ensures ROP progression.
Discussion
The ROP incidence differs between countries with screening criteria guidelines ranging from < 30 to 37 weeks of GA and from 1.000 to 2.500 g of BW10. Our study showed ROP development in 44.7% of screened newborns and ROP progression in 32.7% of ROP newborns, as well as differences in the risk factors that influenced ROP development and progression.
Low GA and BW are the two strongest known risk factors for ROP development11. In our study, the mean GA was 27.69 ± 2.32 weeks among infants with ROP development and 26.39 ± 1.95 weeks among infants with ROP progression, significantly lower that among infants without ROP development or progression. Also, GA and weight at ROP diagnosis were significantly lower among infants with ROP progression; instead, we didn’t find significantly association between GA and weight at ROP maximum stage and risk of ROP.
Similar to other studies, the mean weight at 28 days of life was significantly lower among those who showed ROP development or progression in this study. Although Chaves-Samaniego et al.12 reported that the risk of developing ROP requiring treatment decreased with increasing weight gain ≥ 14 g/day in the first 4 weeks of life, they recommend to take into account GA, BW, time of MV and comorbidity to evaluate ROP risk. Other neonatal demographic risk factors such as sex and race were not significantly associated with risk of ROP.
Omega-3 long-chain polyunsaturated fatty acids have been shown to reduce pathological angiogenesis in a ROP animal model13. Several studies have associated fish oil lipid emulsion for parenteral nutrition with lower incidence of any stage of ROP13,14,15. We found that infants with PN showed lower rate of ROP progression. However, prolonged PN has been suggested as a ROP risk factor16,17.
Several studies have reported that lower Apgar scores, as a general indicator of poor neonatal health, may be associated with higher rates of ROP11. However, on multivariate regression analysis, the relationship was not significant in most cases, as occurs in our work. Further, neonatal CPR was associated with increased ROP development and progression risk. It is likely that, in addition to the underlying systemic disease that made resuscitation necessary, the worsening patient general condition or the possibility of hypoxia periods followed by hyperoxia after CPR are related to the anormal retinal vasculature development in these patients. Similarly, the presence of arterial hypotension during first week of life was related to a higher frequency of ROP development and progression, it could be possibly associated with patient worsening general condition as well as hypoperfusion and subsequent reperfusion problems.
Many studies have indicated that sepsis was closely related to the appearance of any stage of retinopathy and associated with AP-ROP18,19. In our work, there were no differences in early-onset sepsis. However, late-onset sepsis was risk factor for ROP development and progression. Systemic inflammation may impare angiogenesis as well as hypotension and oxygen saturation fluctuation might affect the retinal perfusion and lead to retinal ischemia. The pathophysiology of NEC may implicate innate immune responses to intestinal microbiota, inducing inflammation that affects retinal angiogenesis therefore many studies have shown that it may increase ROP risk20,21, as in our work.
The mechanism that describes CMV influence on retinal vasculature remains unknown but recent studies show how the virus can activate the cytokines paracrine pathway that influences endothelial cells function and stimulates the liberation of pro-angiogenic factors, stimulating retinal inflammation and angiogenesis and leading to ROP development or progression22. In our study, there was an association with ROP development, being ROP more frequent in infection confirmed cases and in those requiring treatment.
It has been suggested that neonatal respiratory diseases are closely related to the development of ROP. Infants with apnea are more likely to require MV and supplementary oxygen, and may be more likely to develop ROP. Also, BPD and RDS have been associated with ROP. RDS is caused by surfactant deficiency so newborns with RDS may require MV and oxygen therapy. Not surprisingly, RDS is associated with increased risk of ROP. In this work all of them were risk factors for development and progression of the disease and pneumothorax was found to be associated with ROP progression. Many infants with RDS require surfactant administration. Some studies have suggested that surfactant therapy is closely related to ROP23,24, which can be interpreted as higher ROP risk in infants with RDS requiring treatment. In our work, we stated that surfactant administration is associated with higher risk of ROP development and lesser risk of progression.
The mean duration of oxygen therapy was significantly higher among infants with ROP development and progression as well as minimum and highest FiO2 levels. Regarding assisted ventilation, we found that any modality (HFOV, MV or NIV) and its duration were related to the development and progression of ROP. Similarly, the need of ventilatory support and/or oxygen at 36 weeks, which defines moderate/severe BDP, was also associated with an increased risk of ROP development and progression. These cases are patients with chronic respiratory disease in whom episodes of desaturation and subsequent hyperoxia are frequent during oxygen treatment, this could explain the increased risk.
Longer length of stay has been associated with ROP17. This may be due to length of stay is an indicative for cumulative illness. Our work revealed higher risk of ROP development and progression.
In addition, anemia and blood transfusions have also been implicated as ROP risk factors. A possible explanation could be that adult-type hemoglobin has a lower oxygen affinity and may cause excess oxygen release in the retinal tissue25. Other explanation could be that the iron load from transfusions may catalyze the formation of reactive oxygen species and accelerate oxidative damage, leading to ROP25. In our work, anemia and blood transfusions were associated with ROP development and progression but were no longer associated after multivariate analysis, as occurs in most of the recent studies26.
In infants with PDA, reduced perfusion due to systemic blood flow by-pass might result in retina hypoxia and might predispose to ROP development or progression. It has been reported associations between PDA and neonatal diseases such as NEC, IVH and BDP27,28 Similar to other studies29, PDA was an independent risk factor of ROP in our work. Furthermore, management of PDA may also be associated with ROP. Beharry et al.30 found that indomethacin, used as PDA treatment, could influence retinal neovascularization in animal models.
Regarding IVH, we observed a higher risk of ROP development without higher progression risk associated. IVH and ROP are both associated with immature vasculature and unstable oxygen supply31. In this context, iron molecules are released, which especially in the presence of oxygen excess, produce free radicals liberation.
Various studies have suggested that the pathophysiologic events that predispose preterm neonates to ROP may begin before delivery6. Ahn et al.32 reported the association of chorioamnionitis with ROP and AP-ROP. A meta-analysis of 27 studies revealed that chorioamnionitis was significantly associated with ROP by univariate analyses, but no association was found on multivariate analysis correcting for GA, as in our work33. Woo et al.34 investigated the relationship between cytokine levels in cord blood and perinatal factors and ROP in GA-matched preterm babies showing that cord blood cytokine levels are not associated with the risk of ROP, whereas increased maternal blood leukocyte count and low Apgar score are associated with an elevated risk of ROP. They also found that increased levels of inflammatory and angiogenic mediators in the amniotic fluid are independently associated with the development and progression of ROP35.
From one standpoint, multivariate analysis for ROP development showed that the GA has the strongest influence on the development of ROP; increasing the risk of ROP development as the GA decreases. That risk was subsequently modified depending on the GA group and the presence or not of other variables such as oxygen and weight at 28 days of life, MV duration, NIV, surfactant administration and late-onset sepsis. Otherwise, multivariate analysis for ROP progression demonstrated that the duration of supplemental oxygen therapy has the strongest influence on the progression of ROP; increasing the risk as the number of oxygen days increases and being modified depending on the association or not of other variables such as late-onset sepsis and weight at 28 days of life.
The main strength of our study is the large representative sample, which gives more faithful results. However, our results should be interpreted taking into consideration the following limitations: First, all the known risk factors could not be added to this study. Second, it was conducted in a single NICU, although it is a level three unit; nonetheless, this study provides relevant data on the ROP incidence and risk factors of the Spanish population and it may be used as a basis for future multicenter trials. Additional investigation is necessary to identify the risk factors role and validate them in other populations ( Supplementary Information).
Conclusions
The reason why ROP development factors differs from ROP progression factors remains unclear. GA, MV duration, supplemental oxygen therapy at 28 days of life, NIV, surfactant administration, late-onset sepsis and weight at 28 days of life influence ROP development, whereas duration of supplemental oxygen therapy, late-onset sepsis and weight at 28 days of life are risk factors for ROP progression.
Our study suggests that, on one hand, GA is the first risk factor to determine ROP development risk; on the other hand, the duration of supplemental oxygen therapy is the first predictor of ROP worsening. These findings may help pediatricians and ophthalmologists to evaluate the risk of ROP development and progression and determine the appropriate timing of examinations and treatment.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Terry, T. L. Extreme prematurity and fibroplastic overgowth of persistent vascular sheath behind each crystal-line lens I preliminary report. Am. J. Ophthalmol. 25, 203–204 (1942).
Blencowe, H., Lawn, J., Vazquez, T., Fielder, A. & Gilbert, C. Preterm-associated visual impairment and estimates of retinopathy of prematurity at regional and global levels for 2010. Pediatr. Res. 74, 35–49 (2013).
American Academy of Ophthalmology. Chapter 4: Eye development, (Ed. American Academy of Ophthalmology) BCSC Basic and Clinical Science Course, Section 2: Fundamentals and principles of ophthalmology. Embriol. Genet. 1–16 (2017).
Fleck, B. W. & McIntosh, N. Pathogenesis of retinopathy of prematurity and possible preventive strategies. Early Hum. Dev. 84, 83–88 (2008).
Ferrer Novella, C. et al. Screening program for retinopathy of prematurity in Spain. Arch. Soc. Esp. Oftalmol. 88, 184–188 (2013).
Damman, O., Rivera, J. & Chemtob, S. The prenatal phase of retinopathy of prematurity. Acta Paediatr. 110, 2521–2528 (2021).
International Committee for the Classification of Retinopathy of Prematurity. The international classification of retinopathy of prematurity revisited. Arch. Ophthalmol.. 123, 991–999 (2005).
Ferrer Novella, C. et al. A protocol for the treatment of retinopathy of prematurity in Spain. Arch. Soc. Esp. Oftalmol. 88, 231–236 (2013).
Horbar, J. D. et al. Trends in mortality and morbidity for very low birth weight infants, 1991–1999. Pediatrics 110, 143–151 (2002).
Mora, J., Waite, C., Gilbert, C., Breidenstein, B. & Sloper, J. A worldwide survey of retinopathy of prematurity screening. Br. J. Ophthalmol. 102, 9–13 (2018).
Kim, S. et al. Retinopathy of prematurity: A review of risk factors and their clinical significance. Surv. Ophthalmol. 63, 618–637 (2018).
Chaves-Samaniego, M. J., Chaves-Samaniego, M. C., Muñoz Hoyos, A. & García Serrano, J. L. New evidence on the protector effect of weight gain in retinopathy of prematurity. An. Pediatr. 95, 78–85 (2021).
Connor, K. et al. Increased dietary intake of omega-3- polyunsaturated fatty acids reduces pathological retinal angiogenesis. Nat. Med. 13, 868–873 (2007).
Beken, S. et al. The influence of fish-oil lipid emulsions on retinopathy of prematurity in very low birth weight infants: A randomized controlled trial. Early Hum. Dev. 90, 27–31 (2014).
Vayalthrikkovil, S. et al. Parenteral fish-oil lipid emulsions in the prevention of severe retinopathy of prematurity: A systematic review and meta-analysis. Am. J. Perinatol. 34, 705–715 (2017).
Porcelli, P. & Weave, R. Jr. The influence of early postnatal nutrition on retinopathy of prematurity in extremely low birth weight infants. Early Hum. Dev. 86, 391–396 (2010).
Ali, A., Gomaa, N., Awadein, A., Al-Hayouti, H. H. & Hegazy, A. I. Retrospective cohort study shows that the risks for retinopathy of prematurity included birth age and weight, medical conditions and treatment. Acta Paediatr. 106, 1919–1927 (2017).
Lundgren, P. et al. Aggressive posterior retinopathy of prematurity is associated with multiple infectious episodes and thrombocytopenia. Neonatology 111, 79–85 (2017).
Bonafiglia, E. et al. Early and late onset sepsis and retinopathy of prematurity in a cohort of preterm infants. Sci. Rep. 12, 11675 (2022).
Tremblay, S. et al. Systemic inflammation perturbs developmental retinal angiogenesis and neuroretinal function. Investig. Ophthalmol. Vis. Sci. 54, 8125–39 (2013).
Hong, H. et al. Neonatal systemic inflammation in rats alters retinal vessel development and simulates pathologic features of retinopathy of prematurity. J. Neuroinflamm. 11, 87 (2014).
Wilkerson, I., Laban, J., Mitchell, J., Sheibani, N. & Alcendor, D. J. Retinal pericytes and cytomegalovirus infectivity: Implications for HCMV-induced retinopathy and congenital ocular disease. J. Neuroinflamm. 12, 2 (2015).
Seiberth, V. & Linderkamp, O. Risk factors in retinopathy of prematurity. A multivariate statistical analysis. Ophthalmologica 214, 131–135 (2000).
Mehmet, S. et al. One-year experience in the retinopathy of prematurity: frequency and risk factors, short-term results and follow-up. Int. J. Ophthalmol. 4, 634–640 (2011).
Hirano, K. et al. Blood transfusion increases radical promoting non-transferrin bound iron in preterm infants. Arch. Dis. Child Fetal Neonatal 84, 188–193 (2001).
Ghirardello, S. et al. Effects of red blood cell transfusions on the risk of developing complications or death: An observational study of a cohort of very low birth weight infants. Am. J. Perinatol. 34, 88–95 (2017).
Capozzi, G. & Santoro, G. Patent ductus arteriosus: Patho-physiology, hemodynamic effects and clinical complications. J. Matern. Fetal Neonatal. Med. 24, 15–16 (2011).
Hamrick, S. & Hansmann, G. Patent ductus arteriosus of the preterm infant. Pediatrics 125, 1020–1030 (2010).
Aydemir, O. et al. Adjusted poor weight gain for birth weight and gestational age as a predictor of severe ROP in VLBW infants. Eye 25, 725–729 (2011).
Beharry, K. et al. Comparative effects of early postnatal ibuprofen and indomethacin on VEGF, IGF-1 and CH during rat ocular development. Investig. Ophthalmol. Vis. Sci. 47, 3036–3043 (2006).
Procianoy, R., Garcia-Prats, J., Hitner, H., Adams, J. M. & Rudolph, A. J. An association between retinopathy of prematurity and intraventricular hemorrhage in very low birth weight infants. Acta Paediatr. Scand. 70, 473–477 (1981).
Ahn, Y. J. et al. Characteristic clinical features associated with aggressive posterior retinopathy of prematurity. Eye 31, 924–930 (2017).
Mitra, S., Aune, D., Speer, C. P. & Saugstad, O. D. Chorioamnionitis as a Risk factor for retinopathy of prematurity: A systematic review and meta-analysis. Neonatology 105, 189–199 (2014).
Woo, S. et al. The relationship between cord blood cytokine levels and perinatal factors and retinopathy of prematurity: A gestational age-matched case-control study. Investig. Ophthalmol. Vis. Sci. 54, 3434–3439 (2013).
Woo, S. et al. Inflammatory and angiogenic mediators in amniotic fluid are associated with the development of retinopathy of prematurity in preterm infants. Investig. Ophthalmol. Vis. Sci. 61, 42 (2020).
Author information
Authors and Affiliations
Contributions
Conceptualization: R.R.N., L.A.G., R.D.F., P.F.FJ., S.T.T. (All authors) Methodology: L.A.G., P.F.FJ., S.T.T. and R.R.N. Analysis and interpretation of data: R.D.F. and R.R.N. Writing the main manuscript text: R.R.N. Figures: R.D.F. and R.R.N. All authors reviewed the manuscript and agreed to the published version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
de las Rivas Ramírez, N., Luque Aranda, G., Rius Díaz, F. et al. Risk factors associated with Retinopathy of Prematurity development and progression. Sci Rep 12, 21977 (2022). https://doi.org/10.1038/s41598-022-26229-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-26229-4
This article is cited by
-
Critical period of oxygen supplementation and invasive ventilation: implications for severe retinopathy of prematurity
Italian Journal of Pediatrics (2024)
-
Predictive role of systemic immune-inflammation index and neutrophil/lymphocyte ratio values in infants with retinopathy of prematurity
Graefe's Archive for Clinical and Experimental Ophthalmology (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
