
Abstract
Adequate hand hygiene practices throughout the continuum of care of maternal and newborn health are essential for infection prevention. However, the hand hygiene compliance of facility-based birth attendants, parents and other caregivers along this continuum is low and behavioural-science informed interventions targeting the range of caregivers in both the healthcare facility and home environments are scarce. We assessed the limited efficacy of a novel multimodal behaviour change intervention, delivered at the facility, to improve the hand hygiene practices among midwives and caregivers during childbirth through the return to the home environment. The 6-month intervention was implemented in 4 of 8 purposively selected facilities and included environmental restructuring, hand hygiene infrastructure provision, cues and reminders, and participatory training. In this controlled before-and-after study, the hand hygiene practices of all caregivers present along the care continuum of 99 women and newborns were directly observed. Direct observations took place during three time periods; labour, delivery and immediate aftercare in the facility delivery room, postnatal care in the facility ward and in the home environment within the first 48 h following discharge. Multilevel logistic regression models, adjusted for baseline measures, assessed differences in hand hygiene practices between intervention and control facilities. The intervention was associated with increased odds of improved practice of birth attendants during birth and newborn care in the delivery room (Adjusted odds ratio [AOR] = 4.7; 95% confidence interval [CI] = 2.7, 7.7), and that of parental and non-parental caregivers prior to newborn care in the post-natal care ward (AOR = 9.2; CI = 1.3, 66.2); however, the absolute magnitude of improvements was limited. Intervention effects were not presented for the home environment due COVID-19 related restrictions on observation duration at endline which resulted in too low observation numbers to warrant testing. Our results suggest the potential of a facility-based multimodal behaviour change intervention to improve hand hygiene practices that are critical to maternal and neonatal infection along the continuum of care.
Similar content being viewed by others


Introduction
Globally, infections acquired during birth and the first days of post-natal care account for an estimated 11–19% of all neonatal deaths1 and 10% of maternal deaths2, the majority of which occur in low and middle income countries (LMIC). Adequate hand hygiene practices are an essential maternal and newborn infection prevention strategy3,4,5,6 and should be delivered throughout the continuum of care7,8,9,10. The continuum of care for maternal, newborn and child health is typically defined to include care during pregnancy, delivery and postnatal care (PNC)11,12.
Hand hygiene compliance of birth attendants and caregivers along this care continuum remains low13,14,15,16. A recent systematic review of facility-based birth attendants’ hand hygiene compliance in LMIC estimated compliance ranging from 1 to 38%13. Observational studies of facility-based births in LMIC have identified multiple risks of infection to mothers and newborns due to inadequate hand hygiene practices during post-natal care in the facility through to the return to the household14,15,16,17,18,19. While global estimates are not available, both qualitative and quantitative studies suggest that hand hygiene compliance specific to newborn care is very low in low-resource settings—as low as 1% in Nigeria among healthcare workers and family members and 2.3–9.1% among mothers in Bangladesh15,20,21,22,23.
Hygiene interventions spanning both healthcare facility (HCF) and home environments are scarce with limited evidence around their effectiveness at changing handwashing behaviour11,24. Hand hygiene studies to-date mostly focus on individual care periods, particularly birth13,17,18,25,26,27 or the late post-natal period (> 7 days of life)8,20,21,28. Postnatal care in the critical days following facility-based birth remains under investigated11,12. The role and engagement of paternal and non-parental caregivers in LMIC in the provision of care across both environments has been documented8,15,19,20,29,30, however hand hygiene improvement strategies commonly only target birth attendants and mothers’ practices, leaving other important caregiver groups’ practices unaddressed24. There is a need for contextualised hand hygiene strategies that can span both the HCF and the home and effectively target hand hygiene practices of the multiple caregivers that lie along this pathway.
We tested the feasibility of a facility-based intervention targeting hand hygiene practices of caregivers of women and new-borns during institutional births and post-natal care, and the return to the home environment. For the purposes of this intervention, caregivers included midwives during childbirth, midwives, mothers, and non-maternal caregivers during post-natal care of the new-born, and mothers and other non-maternal caregivers in the home environment. Formative work in this setting documented low hand hygiene compliance in both the facilities and in the home and identified various psychosocial, physical and contextual factors influencing these practices18,19. Despite availability of functioning hand hygiene infrastructure and materials and demonstrated understanding of infection risk due to inadequate hand hygiene, barriers to effective hand hygiene adherence from midwives included limited understanding of hand or glove recontamination risk, habits and norms around inappropriate gloving practices, perceived lack of time from high workloads and low staffing, and low perception of newborn infection risk18. Among household members, barriers to effective hand hygiene included inadequate and inaccessible hygiene infrastructure in the facility, inadequate knowledge around hand hygiene opportunities and adequate hygiene protocol during newborn care, bypassing handwashing steps due to excitement or rushing to alleviate the newborn’s perceived distress (nurture), and restrictive gender norms and family hierarchies resulting in limited influence of the mother to inform other relatives’ hand hygiene practices19.
These findings informed the design of a multimodal behaviour change intervention delivered at facility level and aimed at improving hygiene behaviours related to maternal and neonatal care at both healthcare facilities and the home environment. The objective of this controlled before and after study was to assess the effect of this intervention on hand hygiene behaviours among birth attendants and other caregivers across eight HCFs in rural Cambodia.
Methods
Study setting and participants
The study was conducted in Kampong Chhnang Province, Cambodia. The study included eight purposively selected healthcare facilities (HCF), six primary health centres (PHC) and two referral hospitals, that were initially observed in the formative phase of the project18,19. Four HCFs were assigned to receive the intervention and the remaining four assigned to serve as comparison facilities. The six participating PHCs represented three different settings; rural/low facility-birth volume, rural/high facility-birth volume, and peri-urban/high facility-birth volume. One facility from each setting was assigned to receive the intervention. The referral hospital with the higher number of monthly deliveries was selected to receive the intervention. The sample size was considered sufficient for the exploratory nature of the study.
Any woman who presented to the HCF for delivery prior to entering the second stage of labour and was not already in excess pain and distress was eligible for recruitment. Patients considered by clinical staff to have complicated labour or delivery, or those under 18 and unaccompanied by a parent/guardian were excluded from the study. In the six PHCs, new women were recruited and enrolled over a 14-day period or until a total of five women had been enrolled; whichever came first. In the referral hospitals, new women were recruited and enrolled over a 14-day period with no limit on the total number of women enrolled per facility. Details on data collection procedures are described below.
Written consent was obtained from the women, health care workers and all accompanying members who were present with the woman at any point during the observation period. We obtained verbal consent in addition to a witness signature in the case of a participant with low literacy. Participation was voluntary and the recruitment was done in a private area and the women were encouraged to have someone else with them during the recruitment process. To minimise reactivity, the explicit mention of handwashing was avoided and participants were informed that the aim of the study was to observe care giving practices during childbirth and postnatal care. The data collector discussed and agreed verbal or non-verbal cues with each participant that they could use to pause or terminate the observation at any time.
Intervention package
The design and development of the intervention was informed by earlier formative research conducted in the 8 HCFs18,19. In brief, the intervention design followed The Behaviour Centred Design (BCD) process31. Details on the formative research and how the BCD process was used to identify potential interventions are described in previous publications18,19.
Potential interventions were tested and refined through a participatory creative process using the Human-Centred Design approach led by 17 Triggers32, an in-country creative agency. Following a three-day co-creation workshop with key stakeholders in Phnom Penh, rapid field testing and prototyping was conducted with 15 mothers, 10 midwives, two facility directors and seven family members in two non-study HCFs and catchment communities over 3 weeks in November 2019. The final intervention design was based on the level of acceptability by users and HCF management, degree of alignment of the intervention components with formative research findings31 and logistic and financial constraints. The final intervention was a multimodal intervention targeting midwives, mothers, fathers and non-parental caregivers that included physical environment restructuring, provision and improved access to hand hygiene infrastructure and materials, visual cues and reminders, social influence, and participatory training.
The intervention was delivered in two locations within the maternity ward; the labour and delivery (LD) room and PNC room. The intervention components in the LD room aimed to improve hand hygiene practices of birth attendants, primarily midwives, during birth and the intervention components in the PNC room aimed to improve the hand hygiene practices of primarily mothers and caregivers providing early newborn care in both the post-natal care ward and the household following discharge. Table 1 provides an overview of the intervention components and content.
The intervention was delivered to selected facilities in July 2020 and ran for 24 weeks. Throughout the 6-month implementation period, the intervention HCFs were responsible for refilling the liquid soap and maintaining the handwashing sinks. The study project team was responsible for restocking and maintaining all other intervention components. Final data collection ran from November to December 2020.
Study design and evaluation
Outcomes
The study was designed as a non-randomised controlled before-and-after feasibility study. The behavioural outcomes of interest were hand hygiene practices of (1) Birth attendants during labour, delivery and immediate newborn care in the delivery room; (2) Health care workers (HCW) and other caregivers in post-natal care facility ward during newborn care and (3) Caregivers in the home environment during newborn care. Previously reported observational data on hand hygiene18,19 served as the baseline measures for this evaluation.
Data collection procedures
Data (baseline) was collected in all eight participating facilities (February–July 2019) as part of the formative research study and were repeated at the end of the implementation period (endline). All study methods, data collection procedures, tools and baseline findings are detailed in earlier publications18,19. The tools for structured assessments adapted from standard tools; WHO WASHFIT33 and Soap-Box WASH & Clean toolkit34 to assess the facility-level and household hygiene conditions. Hand hygiene practices were assessed via direct observation over three periods; childbirth in the delivery ward, post-natal period in the facility PNC ward and post-natal period in the home. The key events for each of the three observation periods included in the direct observation tool were selected based on previous observations of hygiene during childbirth14, WHO’s Five Moments for Hand hygiene35,36 WHO postnatal care recommendations4,37 and the three moments adapted for neonatal hand hygiene in the community described by Ditai et al.38.
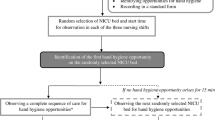
Labour and delivery observations began when the woman was admitted to the facility and the first vaginal examination occurred and terminated either after 6 h or when the woman-newborn pair was discharged from the delivery room, whichever came first. Data collectors recorded key events including birth attendants’ handwashing and gloving practices and any observed contact of the birth attendants with the mother, newborn, objects and surfaces and other individuals during the observation period.
Observations during the post-natal period in the facility began when the mother-newborn pair was transferred to the PNC room of participating facilities and were terminated after a period of four continuous hours. Home observations were conducted within 72 h following discharge from the HCF and began after the household structured assessment was completed and lasted 1 h. Home observations were only completed for women who delivered in the six PHCs. During both the PNC period at the facility and the home, newborn care practices included diaper changes, cord care, breastfeeding and general newborn handling and were recorded along with any corresponding hand hygiene practices of any individuals providing newborn or maternal care.
All women were given a 15-min break from observations every 2 h, but any of the participants could pause or terminate the observations at any time either by saying so or using agreed nonverbal cues such as waving a raised hand or putting a thumbs down.
Data were collected on tablets used pre-coded observation tools by trained data collectors. Across all observations, data collectors positioned themselves in an unobtrusive location and recorded key events of all individuals present in each respective period. Five of the six study observers had prior experience with the study protocol and data collection methods having participated in the baseline data collection. All observers received a 3-day in house refresher training of the study protocol, ethical research practices and role play sessions. All observations tools and protocols were piloted in the field prior to data collection, however due to COVID-19 risk measures, the pilots were conducted in the study referral hospitals where the midwives observed four deliveries. Study observers were paired up during the pilot period to increase interrater reliability. Given the small sample size, rather than use statistical techniques to formally test reliability, observers worked independently to gather data and the observation data was compared at the end of each delivery. Any discrepancies between the pairs were discussed with the study manager for clarification and discussion.
Data analysis
All quantitative data was analysed using StataSE 15 (Stata Corp, College Station, TX, USA)39. All Qualitative notes recorded during the observations were reviewed and where applicable, recoded into quantitative data using StataSE 1539. Data from the home and facility level assessments were analysed descriptively and triangulated to provide context to the structured observations.
Analysis of labour and delivery structured observations
We defined labour, delivery and newborn aftercare flows according to the analysis described in the methods by Nalule et al.18. For each flow, we assigned time-specific hand hygiene categories (Table 2) to each birth attendant around hand hygiene opportunities prior to the initiation of the flow and within the flow when invalidation of aseptic technique occurred. Detailed definitions and descriptions of flows and aseptic procedures used for the analysis have been previously described18.
Descriptive statistics were used to calculate the frequency and proportion of flows initiated and aseptic procedures within the flows that were conducted under each respective hand hygiene category. Results were provided by data collection rounds (endline, baseline) and study group assignment (intervention, comparison).
Multilevel logistic regression models accounting for multiple observations clustered within the same facility were used to calculate difference-in-difference (DID) estimates to assess the effect of the intervention between intervention and comparison facilities after adjusting for baseline observations. To facilitate interpretability of results, the three-level primary outcome for hand hygiene during childbirth was collapsed into a series of binary outcome measures with each measure coded either as adequate hand hygiene category = 1, or aseptic technique invalidated hand hygiene category = 1 to provide better interpretation of the results to clinicians.
The outcome measures for this analysis were:
-
(1)
Adequate hand hygiene prior to the initiation of a flow or prior to any key event related to newborn care (adequate hand hygiene category = 1; aseptic technique invalidated or inadequate hand hygiene categories = 0)
-
(2)
Adequate hand hygiene during aseptic procedures within the flow (adequate hand hygiene category = 1; aseptic technique invalidated or inadequate hand hygiene categories = 0)
-
(3)
Invalidated hand hygiene prior to the initiation of a flow (aseptic technique invalidated hand hygiene category = 1; inadequate or adequate hand hygiene categories = 0).
We ran models separately for each outcome measure. Unadjusted DID models were used to calculate odds ratios without adjustment for any potential confounding variables. The second set of DID models for outcome measures was used to calculate an adjusted odds ratio and co-variates identified a priori for adjustment: working shift time, facility type (referral hospital vs primary health facility) and professional qualification (midwife vs. Doctor + Nurse vs. Midwife intern).
Analysis of PNC and home observation structured observations
Only hand hygiene opportunities pertaining to newborn care were analysed for the PNC and home observations. Detailed descriptions of newborn-care related hand hygiene opportunities used for this analysis are previously described19. Caregivers of the newborns were categorised into four groups; mothers, fathers, healthcare workers (midwives, nurses, doctors and interns) or non-parental caregivers (all other individuals observed providing care to the newborn). For each caregiver, hand hygiene actions associated with each hand hygiene opportunity were coded into two categories for the analysis; adequate and inadequate (Table 2).
Analysis procedures for PNC and the household observations differed from observations in the labour and delivery wards. At baseline, we observed no hand hygiene action in relation to a hand hygiene opportunity in either the PNC or the home environment19 and difference-in-difference analyses were not possible. Instead, we focus on results from endline data only. Descriptive statistics were used to calculate the frequency and proportion of hand hygiene opportunities under each respective hand hygiene category by caregiver and treatment group at endline only. For the PNC, multilevel logistic regression models; unadjusted and adjusted for working shift time, facility type (referral hospital vs. primary health facility) and professional qualification (midwife vs. Doctor + Nurse vs. Midwife intern). For home observations, the limited numbers of observed hand hygiene actions did not warrant significance testing.
Ethics approval and consent to participate
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board at the London School of Hygiene and Tropical Medicine (Reference 16128, 21 November 2018, 22 May 2019—Amendment & Reference 19103, 04 March 2020, 01 May 2020—Amendment) and the Cambodia National Ethics Committee for Health research (NECHR Number 13, 28/01/2019, NECHR Number 134, 24 May 2019-Amendment, NEHCR Number 131, 15 June 2020). All participants provided written informed consent prior to participation.
Results
Baseline data were collected in February—July 2019 and endline data in November—December 2020 (Table 3).
Facility and household hygiene conditions
The delivery room hygiene conditions were similar between study groups at both baseline and endline (Table 3).
All delivery rooms had functional handwashing facilities (HWF). In the PNC room, none of the facilities had functional HWF or hand hygiene messaging at baseline. At endline, functional HWF were available in 100% (4/4) of the PNC rooms of the intervention facilities and 0% of comparison facilities. Hand hygiene messaging was present in 100% (4/4) of intervention and 25% (1/4) of comparison facilities.
At baseline, functioning HWF were present in 45% (5/11) of the households of the women who had given birth at the comparison facilities (comparison households) and 54% (6/11) of the households of the women who had given birth at the intervention facilities (intervention households). The presence of functioning HWF dropped to 9% (1/11) in the comparison households and increased to 73% (8/11) in the intervention households at endline. Over 90% of the households in both groups had soap and detergent available in the household at both endline and baseline. At endline, alcohol-based hand rub (ABHR) was present was in 92% (9/11) of the intervention households and 9% (1/11) of the comparison households. All ABHR present in the intervention households was from the facility.
Participant characteristics
At baseline, 45 mothers (n = 16 comparison; n = 29 intervention) were enrolled and observed during the labour and delivery observations, 46 (n = 17 comparison; n = 29 intervention) during facility PNC observations and 22 (n = 11 comparison; n = 11 intervention) during the household observations. These details can be found in the supplementary tables provided (see Supplementary Table S1). At endline, 54 mothers (n = 19 comparison; n = 35 intervention) were observed during the labour and delivery observations, 53 (n = 18 comparison; n = 35 intervention) during facility PNC observations and 22 (n = 11 comparison; n = 11 intervention) during the household observations.
Baseline and endline characteristics of the mothers were similar between study facilities although there were some differences in working shift times at endline, number of PNC visitors at baseline and HCF staff presence in both time periods. More details showing the baseline and endline characteristics by intervention group and observation period can be found in the supplementary table (see Supplementary Table S1).
Only one additional participant was recruited for post-natal observations at baseline. At endline, one observation had to be terminated at endline due to newborn complications in the facility PNC ward.
Structured observations in the delivery room
All flows
We observed a total of 251 (n = 88 comparison; n = 163 intervention) flows initiated under adequate hand hygiene at baseline and 375 (n = 122 comparison; n = 252 intervention) at endline.
When combined, the proportion of flows initiated under adequate hand hygiene declined by 10% (24% to 14%) in comparison facilities and increased by 11% (16% to 27%) in intervention facilities between baseline and endline (Table 4). After adjusting for baseline differences and potential confounders, this corresponds to an adjusted odds ratio (AOR) of 4.7 (95% confidence interval CI = 2.9, 7.7).
Labour flow
We observed a total of 95 (n = 26 comparison; n = 69 intervention) labour flows initiated under adequate hand hygiene at baseline and 108 (n = 35 comparison; n = 73 intervention) at endline.
At endline, 45% of labour flows in intervention facilities were initiated by the healthcare worker with hands washed and clean gloves worn compared to 17% in the comparison facilities (Table 4). The proportion of labour flows initiated under adequate hygiene in the comparison facilities declined by 14% between baseline and endline and increased by 25% in the intervention facilities. After adjusting for baseline measures and potential confounders, midwives in intervention facilities had almost 7 times greater odds of practicing adequate hand hygiene prior to initiating a labour flow than midwives in comparison facilities (AOR = 6.6; CI = 1.4, 32.1).
Delivery flow
We observed a total of 102 (n = 39 comparison; n = 63 intervention) delivery flows initiated under adequate hand hygiene at baseline and 116 (n = 37 comparison; n = 79 intervention) at endline.
Between baseline and endline, the proportions of delivery flows initiated under adequate hand hygiene increased in the intervention facilities (17–20%) and declined in the comparison facilities (26–19%) (Table 4). We found no evidence of difference in the odds of birth attendants initiating delivery flows with adequate hand hygiene between the intervention and comparison facilities (AOR = 1.8; CI = 0.5, 6.5).
Hygiene within the delivery flow
Within the delivery flows, we observed 340 (n = 108 comparison; n = 232 intervention) unique aseptic events at baseline and 398 (n = 131 comparison; n = 267 intervention) at endline. The frequency and proportion of individual aseptic events in detail can be found in the supplementary information (see Supplementary Table S2). At baseline, 19% and 11% of aseptic events within the delivery flow were conducted under adequate hand hygiene in comparison and intervention facilities (Table 4). This proportion declined to 12% in comparison facilities and increased by 4% points to 15% in the intervention facilities. We found no evidence of differences in the odds of conducting any aseptic procedure within the delivery flow under adequate hygiene between the intervention and comparison group after adjusting for baseline observation and potential confounders (AOR = 2.6; CI = 0.9, 7.6). More details on the proportion of individual aseptic events conducted under adequate hand hygiene can be found in the supplementary information (see Supplementary Table S3).
Newborn aftercare flow
We observed a total of 54 (n = 23 comparison; n = 31 intervention) newborn aftercare flows initiated under adequate hand hygiene at baseline and 151 (n = 50 comparison; n = 101 intervention) at endline.
The proportion of newborn aftercare flows initiated under adequate hand hygiene declined from 13 to 8% in the comparison facilities and increased from 6 to 20% in intervention facilities between baseline and endline (Table 4). Midwives in an intervention facility had 10 times the odds of practicing adequate hand hygiene prior to initiating a newborn aftercare flow than midwives in the comparison facilities after adjusting for baseline observations and potential confounders (AOR = 9.7; CI = 1.2, 75.7).
Invalidated hand hygiene
We calculated the odds of initiating each of the flow categories under invalidated hand hygiene, coded as invalidated aseptic technique category, compared with either adequate or inadequate hand hygiene categories (Table 2).
The adjusted odds of initiating delivery flow were 70% lower (AOR = 0.3, CI = 0.1–0.7) and newborn aftercare flow 60% lower (AOR = 0.4; CI = 0.2, 0.9) for midwives in intervention facilities after adjusting for baseline observations and potential confounders. There was no evidence of differences in the odds of initiating the labour flow (AOR = 1.5; CI = 0.7, 3.4) with invalidated hand hygiene between intervention and comparison facilities. All details of this can be found in the supplementary information (see Supplementary Table S4).
Structured observations in the PNC ward
At endline, the four-hour observation period began an average of 1.6 h (range: 1–3) in comparison facilities and 1.1 h (1–3) in intervention facilities after the mother-newborn pair was discharged from the LD room (see Supplementary Table S1). The mean number of PNC visitors present during the observations was similar across the groups (4; range 1–9). In 39% (n = 7) of the observations in the comparison facilities, there was no HCW present throughout the 4-h observation period. Within the intervention facilities only, the installed sinks were functional in 94% (n = 33) of the observations and ABHR stations were functional 100% (n = 35) of the observations. 80% (n = 28) of the mothers had their personal ABHR and 86% (n = 29) of the newborns were wearing their intervention hat.
A total of 659 hand hygiene opportunities during newborn care were observed in the PNC ward at endline; 30% (n = 198) in the comparison group and 70% (n = 461) in the intervention group (Table 5).
9% (42/462) of all hand hygiene opportunities were met with adequate hand hygiene practice in the intervention group by all caregiver groups except the health care workers. In the comparison group, only 1% (2/198) of all hand hygiene opportunities were conducted under adequate hand hygiene practice all of which were conducted by non-parental caregivers. After adjusting for shift time, facility type and professional qualification, caregivers in the intervention group had 9 times the odds of practicing adequate hygiene during newborn care than those in comparison group (AOR = 9.2; CI = 1.3–66.2).
Structured observations in the home
In the home environment, the one-hour observation period took place the same day the mother-newborn pair was discharged across both study groups. The mean number of non-maternal caregivers present at home was similar and ranged from 2 to 11 in the comparison households and 3–12 in the intervention households.
A total of 262 hand hygiene opportunities were observed at home; 137 (52%) in the comparison households and 125 (48%) in the intervention households (Table 5). Non-parental caregivers accounted for over half of the hand hygiene opportunities in both comparison and intervention households. Only 2% (3/125) of the hand hygiene opportunities were conducted under adequate hand hygiene in the intervention households. No adequate hand hygiene was observed being conducted across the caregivers in the comparison households.
Discussion
Our analyses show the potential impact of a facility-based intervention to improve hand hygiene practices among birth attendants and other caregivers during childbirth and early post-natal care in the healthcare facility environment. Compared to baseline observations and comparison facilities, birth attendants’ hand hygiene in the delivery ward improved throughout the childbirth process (all flows combined), and in particular prior to initiating maternal care during early and active labour and initiating newborn care during the 1st hour of life. The intervention was also effective in increasing adequate hand hygiene practices of mothers, fathers and non-parental caregivers prior to newborn care in the post-natal care room of the facility.
Similar to wider literature on hygiene practices in HCF16,40,41,42,43,44,45 and domestic settings7,8,16,20,41, hand hygiene practices in our context were influenced by several factors and performed by various people18,19. Our intervention addressed multiple identified determinants of a wide range of relevant target groups which may explain its apparent success13,43,46,47,48,49. Our findings are in line with multiple systematic reviews showing that interventions to improve hand hygiene behaviours are more effective when they target the context and behaviour-specific determinants of hand hygiene46,47,48. Our intervention facilitated and reinforced handwashing practice of target groups through the creation of an enabling environment (physical and social), the incorporation of several nudges & cues and leveraging the teachable moments of pregnancy/new parenthoods and facility attendance. A detailed process evaluation exploring the factors associated with the intervention success and their potential mechanisms of change is under-development.
Our intervention was successful at reducing the odds of birth attendants initiating a delivery flow with invalidated aseptic technique. However, the odds of initiating delivery flows following full hygiene protocol (hands washed with soap AND glove change) did not change. This result suggests that suboptimal hand hygiene practice, specifically glove changing without intermediate hand washing with soap, was a common occurrence in the facilities. This finding is consistent with other studies in other health care settings36,47,50,51,52,53 and specifically during delivery18,40,44,45,54 that have identified institutional factors (human resource shortages, high workload) as influencing the inadequate practice of gloving as a timesaving hand hygiene substitute. Due to limited study scope and funding, our intervention did not directly address factors at the institution level which may explain its limited effectiveness at changing gloving practices54.
Our findings suggest an improvement in hand hygiene compliance after events that invalidated aseptic technique, however confidence intervals overlapped the null value. Despite the persistent challenge avoiding glove/hand recontamination presents to infection control efforts in both High Income Countries (HIC)55,56,57 and LMIC17,44,58, its contribution to overall HCW hand hygiene compliance and subsequently nosocomial transmissions remains under investigated17,55,59. In labour wards in Tanzania, Gon and colleagues17 found that aseptic technique was invalidated almost immediately after gloving or hand hygiene action approximately half the time (227/501) A qualitative study by Hor et al.55 across two hospitals in Australia documented frequent risk of hand and glove recontamination during HCW team ward rounds. Further research is warranted to establish the frequency of aseptic invalidation in health care settings and understand the corresponding behavioural determinants to adapt current hand hygiene interventions to specifically address these behaviours.
Overall we observed large relative estimates of effect of the intervention among HCW and household members in the facility; however, the absolute magnitude of change was limited. Additionally, our intervention resulted in significant improvements in hand hygiene of parental and non-parental caregivers in the intervention group but the improved hand hygiene compliance was still very low (< 10%). Linking our hand hygiene intervention to the antenatal care (ANC) period may provide more opportunities to reinforce and address barriers to hand hygiene prior to childbirth. A recent systematic review found that that interventions that linked antenatal care (ANC), birth, and post-natal care were more effective in improving health outcomes compared to those with fewer linkages12.
Our study employed a one-time onsite training to midwives, delivered remotely over 3 days at the start of the 6-month intervention. However, multiple targeted, repetitive short on-site training sessions delivered in appropriately spaced time periods focusing on practical skill development and application have been associated with improvements in HCW knowledge and skills competency compared to the traditional concentrated one-time training approaches and has been shown to be effective in multiple LMIC context60,61,62,63.
Our intervention had no effect on improving hand hygiene practices in the home environment. This finding should be interpreted with caution. In alignment with the Royal Government of Cambodia’s national COVID guidelines for household data collection, the endline observation period were limited to only one hour (compared to six hours at baseline). The resulting number of observations due to this reduced observation duration period was too low for our study to sufficiently explore hygiene behaviour change across and within study groups during this critical period64. A longer observation period at the households would allow for sufficient data to adequately analyse our intervention effects64. Facility-based interventions have shown promising results as a scalable delivery platform for changing water, sanitation and hygiene (WASH) behaviours at the household level65,66,67,68. The HCF is hypothesized to be a uniquely placed setting to trigger behaviour change as patients and visitors are more likely to be receptive to adopting or improving health behaviours due to heightened perceptions of health risks and the benefits of prevention69,70. The period of pregnancy and early parenthood have also been identified as similar situations with high motivation and receptivity of those affected to improve health behaviours70,71,72. Taken together, the time spent at the facility during antenatal care, labour, delivery and post-natal care remains an opportune setting for targeting expectant parents and non-parental caregivers for sustained behaviour change at the household level64.
Limitations
The measurement of behaviour could be prone to reactivity during observation. It was not possible to mask the target recipients or data collectors to the study group status of the facilities due to the visibility of the intervention. Differential reactivity between study groups could result in over- estimation of the effect of the intervention9. The same team of observers were used for the baseline and endline structured observations and this may have introduced observer bias during the endline data collection.
The study design, methodology and sample size limits the generalisability of our findings to the study HCFs and particularly to women with uncomplicated vaginal births in the facility. Furthermore, the non-randomisation of the facilities means that unobserved confounders may have had an effect on outcomes. We also cannot say if our intervention led to sustained adoption of the desired behaviours and a longer observation period would allow the exploration of the sustained adoption of behavioural outcomes.
As this is a limited efficacy/proof of concept study, it was not appropriate to measure maternal or newborn health related outcomes. Future larger-scale trials using measures of health impact are encouraged to determine whether the observed increases in handwashing with soap are sufficient to reduce infection.
Conclusion
The study suggests the potential of a multi modal behaviour change intervention to improve hygiene behaviours–specifically hand hygiene- linked to maternal and neonatal infection during labour, delivery and post-natal care. More rigorous and larger scale studies are warranted to inform practice and policy change recommendations related to maternal and neonatal infection prevention.
Data availability
The protocols, datasets used and/or analysed during this study are available from the corresponding author upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Abbreviations
- LMIC:
-
Low and middle income countries
- HCW:
-
Health care worker
- PNC:
-
Postnatal care
- LD:
-
Labour and delivery
- HCF:
-
Healthcare facility
- PHC:
-
Primary health centres
- BCD:
-
Behaviour centred design
- ABHR:
-
Alcohol based hand rub
- ANC:
-
Antenatal care
- WASH:
-
Water, sanitation and hygiene
- OR:
-
Odds ratio
- AOR:
-
Adjusted odds ratio
- CI:
-
Confidence interval
- HIC:
-
High income country
References
Fleischmann-Struzek, C. et al. The global burden of paediatric and neonatal sepsis: A systematic review. Lancet Respir. Med. 6(3), 223–230 (2018).
Say, L. et al. Global causes of maternal death: A WHO systematic analysis. Lancet Glob. Health. 2(6), e323–e333 (2014).
WHO. A guide to the implementation of the WHO multimodal hand hygiene improvement strategy. 2009. Available at: whqlibdoc who int/hq/2009/WHO_IER_PSP_2009 02_eng pdf. 2011.
WHO, UNICEF, UNFPA. Pregnancy, childbirth, postpartum, and newborn care: a guide for essential practice: World Health Organization; 2003.
World Health Organization. Every Newborn: An Action Plan to End Preventable Deaths 2014 1–55 (World Health Organization, 2019).
Blencowe, H. et al. Clean birth and postnatal care practices to reduce neonatal deaths from sepsis and tetanus: a systematic review and Delphi estimation of mortality effect. BMC Public Health 11(Suppl 3), S11 (2011).
Curtis, V. A., Danquah, L. O. & Aunger, R. V. Planned, motivated and habitual hygiene behaviour: An eleven country review. Health Educ. Res. 24(4), 655–673 (2009).
Parveen, S. et al. Barriers to and motivators of handwashing behavior among mothers of neonates in rural Bangladesh. BMC Public Health 18(1), 483 (2018).
Ram, P. K. et al. Is structured observation a valid technique to measure handwashing behavior? Use of acceleration sensors embedded in soap to assess reactivity to structured observation. Am. J. Trop. Med. Hyg. 83(5), 1070–1076 (2010).
de Graft-Johnson J. et al. The maternal, newborn and child health continuum of care. in Opportunities for Africa's newborns. Partnership for Maternal, Newborn and Child Health (eds Lawn, J. & Kerber, K.) 23–36 (WHO, Cape Town, South Africa 2006) http://www.who.int/pmnch/media/publications/africanewborns/en/index.html.
Kerber, K. J. et al. Continuum of care for maternal, newborn, and child health: From slogan to service delivery. Lancet 370(9595), 1358–1369 (2007).
Kikuchi, K. et al. Effective linkages of continuum of care for improving neonatal, perinatal, and maternal mortality: A Systematic review and meta-analysis. PLoS ONE 10(9), e0139288 (2015).
Gon, G., de Barra, M., Dansero, L., Nash, S. & Campbell, O. M. Birth attendants’ hand hygiene compliance in healthcare facilities in low and middle-income countries: A systematic review. BMC Health Serv. Res. 20(1), 1–16 (2020).
Buxton, H. et al. Hygiene during childbirth: An observational study to understand infection risk in healthcare facilities in Kogi and Ebonyi states, Nigeria. Int. J. Environ. Res. Public Health 16(7), 1301 (2019).
Nalule, Y. et al. Hygiene along the continuum of care in the early post-natal period: An observational study in Nigeria. BMC Pregnancy Childbirth 20(1), 1–11 (2020).
Bazzano, A. N., Taub, L., Oberhelman, R. A. & Var, C. Newborn care in the home and health facility: Formative findings for intervention research in Cambodia. Healthcare (Basel). 4(4), 94 (2016).
Gon, G. et al. Hands washing, glove use, and avoiding recontamination before aseptic procedures at birth: A multicenter time-and-motion study conducted in Zanzibar. Am. J. Infect. Control 47(2), 149–156 (2019).
Nalule, Y. et al. Hand hygiene during facility-based childbirth in Cambodia: A theory-driven, mixed-methods observational study. BMC Pregnancy Childbirth 21(1), 429 (2021).
Nalule, Y. et al. Hand Hygiene during the early Neonatal period: A mixed-methods observational study in healthcare facilities and households in rural Cambodia. Int. J. Environ. Res. Public Health 18(9), 4416 (2021).
Greenland, K., Iradati, E., Ati, A., Maskoen, Y. Y. & Aunger, R. The context and practice of handwashing among new mothers in Serang, Indonesia: A formative research study. BMC Public Health 13(1), 1–11 (2013).
Ram, P. K. et al. Impact of an intensive perinatal handwashing promotion intervention on maternal handwashing behavior in the neonatal period: Findings from a randomized controlled trial in rural Bangladesh. Biomed. Res. Int. 2017, 6081470 (2017).
Darmstadt, G. L. et al. Practices of rural Egyptian birth attendants during the antenatal, intrapartum and early neonatal periods. J. Health Popul. Nutr. 26(1), 36–45 (2008).
Darmstadt, G. L., Syed, U., Patel, Z. & Kabir, N. Review of domiciliary newborn-care practices in Bangladesh. J. Health Popul. Nutr. 24(4), 380–393 (2006).
Var, C. et al. A linked community and health facility intervention to improve newborn health in Cambodia: The NICCI stepped-wedge cluster-randomized controlled trial. Int. J. Environ. Res. Public Health 17(5), 1559 (2020).
Huttinger, A. et al. Evaluation of membrane ultrafiltration and residual chlorination as a decentralized water treatment strategy for ten rural healthcare facilities in Rwanda. Int. J. Environ. Res. Public Health 12(10), 13602–13623 (2015).
Mathai, E., Allegranzi, B., Kilpatrick, C. & Pittet, D. Prevention and control of health care-associated infections through improved hand hygiene. Indian J. Med. Microbiol. 28(2), 100–106 (2010).
Danda, G., Dube, K., Dube, P., Mudokwenyu-Rawdon, C. & Bedwell, C. An observational study of midwives’ practices to prevent peripartum sepsis in Zimbabwe. Afr. J. Midwifery Women’s Health 9(1), 17–21 (2015).
Rhee, V. et al. Maternal and birth attendant hand washing and neonatal mortality in Southern Nepal. Arch. Pediatr. Adolesc. Med. 162(7), 603–608 (2008).
Park, J. Y., Pardosi, J. F. & Seale, H. Examining the inclusion of patients and their family members in infection prevention and control policies and guidelines across Bangladesh, Indonesia, and South Korea. Am. J. Infect. Control 48(6), 599–608 (2020).
Horng, L. et al. Healthcare worker and family caregiver hand hygiene in Bangladeshi healthcare facilities: Results from the Bangladesh National Hygiene Baseline Survey. J. Hosp. Infect. 94(3), 286–294 (2016).
Aunger, R. & Curtis, V. Behaviour centred design: Towards an applied science of behaviour change. Health Psychol. Rev. 10(4), 425–446 (2016).
17 Triggers. Seventeen Triggers 2022 [updated 2022; cited 2022 01/09/2022]. https://www.17triggers.com/.
WHO, UNICEF. Water and Sanitation for Health Facility Improvement Tool (WASH FIT): A Practical Guide for Improving Quality of Care Through Water, Sanitation and Hygiene in Health Care Facilities (World Health Organization, 2017).
The Soapbox Collaborative. Training in Environmental Hygiene and Cleaning in Healthcare (TEACH CLEAN) Package Aberdeen2019 [cited 2020 09/11/2020]. www.soapboxcollaborative.org.
Sax, H. et al. ‘My five moments for hand hygiene’: A user-centred design approach to understand, train, monitor and report hand hygiene. J. Hosp. Infect. 67(1), 9–21 (2007).
World Health Organisation. WHO Guidelines on Hand Hygiene in Health Care: First Global Patient Safety Challenge: Clean Care is Safer Care (World Health Organization, 2009).
World Health Organisation. WHO Recommendations on Postnatal Care of the Mother and Newborn (World Health Organization, 2014).
Ditai, J. et al. BabyGel pilot: A pilot cluster randomised trial of the provision of alcohol handgel to postpartum mothers to prevent neonatal and young infant infection-related morbidity in the community. Pilot Feasibility Stud. 5(1), 49 (2019).
Stata Corp. Stata Statistical Software: Release 15. College Station, TX.: StataCorp LLC; 2017.
Buxton, H. et al. Barriers and opportunities experienced by staff when implementing infection prevention and control guidelines during labour and delivery in healthcare facilities in Nigeria. J. Hosp. Infect. 103(4), 428–434 (2019).
Bazzano, A. N., Oberhelman, R. A., Potts, K. S., Gordon, A. & Var, C. Environmental factors and WASH practices in the perinatal period in Cambodia: Implications for newborn health. Int. J. Environ. Res. Public Health 12(3), 2392–2410 (2015).
White, S., Thorseth, A. H., Dreibelbis, R. & Curtis, V. The determinants of handwashing behaviour in domestic settings: An integrative systematic review. Int. J. Hyg. Environ Health 227, 113512 (2020).
Gaube, S., Fischer, P. & Lermer, E. Hand(y) hygiene insights: Applying three theoretical models to investigate hospital patients’ and visitors’ hand hygiene behavior. PLoS ONE 16(1), e0245543 (2021).
Gon, G. et al. Behavioural determinants of hand washing and glove recontamination before aseptic procedures at birth: A time-and-motion study and survey in Zanzibar labour wards. Int. J. Environ. Res. Public Health 17(4), 1438 (2020).
de Barra, M. et al. Understanding infection prevention behaviour in maternity wards: A mixed-methods analysis of hand hygiene in Zanzibar. Soc. Sci. Med. 272, 113543 (2021).
Huis, A. et al. A systematic review of hand hygiene improvement strategies: A behavioural approach. Implement. Sci. 7(1), 92 (2012).
Smiddy, M. P., O’Connell, R. & Creedon, S. A. Systematic qualitative literature review of health care workers’ compliance with hand hygiene guidelines. Am. J. Infect. Control 43(3), 269–274 (2015).
Srigley, J. A. et al. Applying psychological frameworks of behaviour change to improve healthcare worker hand hygiene: A systematic review. J. Hosp. Infect. 91(3), 202–210 (2015).
Naikoba, S. & Hayward, A. The effectiveness of interventions aimed at increasing handwashing in healthcare workers—A systematic review. J. Hosp. Infect. 47(3), 173–180 (2001).
Kuzu, N., Ozer, F., Aydemir, S., Yalcin, A. N. & Zencir, M. Compliance with hand hygiene and glove use in a university-affiliated hospital. Infect. Control Hosp. Epidemiol. 26(3), 312–315 (2005).
Pittet, D. Hand hygiene: Improved standards and practice for hospital care. Curr. Opin. Infect. Dis. 16(4), 327–335 (2003).
Erasmus, V. et al. Systematic review of studies on compliance with hand hygiene guidelines in hospital care. Infect. Control Hosp. Epidemiol. 31(3), 283–294 (2010).
O’Boyle, C. A., Henly, S. J. & Larson, E. Understanding adherence to hand hygiene recommendations: The theory of planned behavior. Am. J. Infect. Control 29(6), 352–360 (2001).
Puchalski Ritchie, L. M. et al. Low- and middle-income countries face many common barriers to implementation of maternal health evidence products. J. Clin. Epidemiol. 76, 229–237 (2016).
Hor, S.-y et al. Beyond hand hygiene: A qualitative study of the everyday work of preventing cross-contamination on hospital wards. BMJ Qual. Saf. 26(7), 552 (2017).
Loftus, R. W. et al. Hand contamination of anesthesia providers is an important risk factor for intraoperative bacterial transmission. Anesth. Analg. 112(1), 98–105 (2011).
Wilson, J. et al. The misuse and overuse of non-sterile gloves: Application of an audit tool to define the problem. J. Infect. Prev. 16(1), 24–31 (2015).
Cronin, W. A., Quansah, M. G. & Larson, E. Obstetric infection control in a developing country. J. Obstet. Gynecol. Neonatal. Nurs. 22(2), 137–144 (1993).
Gon, G., Dancer, S., Dreibelbis, R., Graham, W. J. & Kilpatrick, C. Reducing hand recontamination of healthcare workers during COVID-19. Infect. Control Hosp. Epidemiol. 41(7), 870–871 (2020).
Sutton, R. M. et al. Low-dose, high-frequency CPR training improves skill retention of in-hospital pediatric providers. Pediatrics 128(1), e145–e151 (2011).
Evans, C. L. et al. Peer-assisted learning after onsite, low-dose, high-frequency training and practice on simulators to prevent and treat postpartum hemorrhage and neonatal asphyxia: A pragmatic trial in 12 districts in Uganda. PLoS ONE 13(12), e0207909 (2018).
Gomez, P. P. et al. Accelerating newborn survival in Ghana through a low-dose, high-frequency health worker training approach: A cluster randomized trial. BMC Pregnancy Childbirth 18(1), 72 (2018).
Ugwa, E. et al. Simulation-based low-dose, high-frequency plus mobile mentoring versus traditional group-based trainings among health workers on day of birth care in Nigeria; a cluster randomized controlled trial. BMC Health Serv. Res. 20(1), 586 (2020).
Halder, A. K., Molyneaux, J. W., Luby, S. P. & Ram, P. K. Impact of duration of structured observations on measurement of handwashing behavior at critical times. BMC Public Health 13(1), 705 (2013).
George, C. M. et al. Randomized controlled trial of hospital-based hygiene and water treatment intervention (CHoBI7) to reduce cholera. Emerg. Infect. Dis. 22(2), 233 (2016).
Loharikar, A. et al. Long-term impact of integration of household water treatment and hygiene promotion with antenatal services on maternal water treatment and hygiene practices in Malawi. Am. J. Trop. Med. Hyg. 88(2), 267–274 (2013).
Briere, E. C. et al. Impact of integration of hygiene kit distribution with routine immunizations on infant vaccine coverage and water treatment and handwashing practices of Kenyan mothers. J. Infect. Dis. 205(suppl_1), S56–S64 (2012).
Parker, A. A. et al. Sustained high levels of stored drinking water treatment and retention of hand-washing knowledge in rural Kenyan households following a clinic-based intervention. Epidemiol. Infect. 134(5), 1029–1036 (2006).
McBride, C. M., Emmons, K. M. & Lipkus, I. M. Understanding the potential of teachable moments: The case of smoking cessation. Health Educ. Res. 18(2), 156–170 (2003).
Ogden, J. & Hills, L. Understanding sustained behavior change: The role of life crises and the process of reinvention. Health 12(4), 419–437 (2008).
Phelan, S. Pregnancy: A “teachable moment” for weight control and obesity prevention. Am. J. Obstet. Gynecol. 202(2), 135.e1-135.e8 (2010).
Joy, E. A., Van Hala, S. & Marshall, E. Pregnancy as an opportunity for behavior change. Curr. Sports Med. Rep. 3(6), 327–329 (2004).
Acknowledgements
We would like to give a very special thanks to the women who agreed to participate in this study without benefit to themselves as well as the staff and management of the participating HCF. Special thanks go to the following institutions and individuals for their participation and support: MoH—Cambodia, the National Institute of Public Health (NIPH), the National Centre for Maternal and Child Health, the Provincial Health Department and Operational District-Kampong Chhnang, WaterAid Cambodia, WaterAid Australia and other development partners. A very special thanks to WaterAid Cambodia and NIPH team for coordinating the study, and the special contributions of Saray Vannat, Bouth Seyha, Dip Bopha, Hem Navy, Ol Sokhoeun, Ul Pisey, and Vouchnea Tang. All views expressed in this manuscript are those of the authors and do not necessarily reflect those of the funding organisations or affiliated institutions.
Funding
This research was funded by the Australian Government’s Department of Foreign Affairs and Trade (DFAT) under Water for Women fund, grant number WRA089. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the funding organisations or affiliated institutions. The funder played no role in the study design, in the collection, analysis or interpretation of the data, in the writing of the paper or in the decision to submit the article for publication. All authors were independent from the funders.
Author information
Authors and Affiliations
Contributions
Conceptualisation, A.M., C.S., P.I. and R.D.; methodology, H.B. and R.D.; formal analysis, P.P. and Y.N.; investigation, H.B., P.P., S.L. and Y.N.; resources, C.S., P.I., and S.L.; data curation, P.P. and Y.N.; writing—original draft preparation, Y.N.; writing—review and editing, A.M., C.S., H.B., P.I., P.P., R.D., S.L. and Y.N.; supervision, R.D.; project administration, Y.N. and C.S.; funding acquisition, C.S. and R.D. All authors have read and agreed to the published version of the manuscript. All authors had full access to all of the study data and take responsibility for the integrity of the data and the accuracy of the data.
Corresponding author
Ethics declarations
Competing interests
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nalule, Y., Pors, P., Samol, C. et al. A controlled before-and-after study of a multi-modal intervention to improve hand hygiene during the peri-natal period in Cambodia. Sci Rep 12, 19646 (2022). https://doi.org/10.1038/s41598-022-23937-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-23937-9
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
