
Abstract
Migraine is a disease characterized by cerebral vasodilation. While diabetes has previously been associated with a lower risk of migraine, it is not known if diabetic retinopathy (DR), a retinal peripheral vascular occlusive disease, is a potential biomarker of protection against migraine. Therefore, we aimed to examine diabetic retinopathy as a marker of prevalent and 5-year incident migraine. In a national cohort, we compared patients with diabetes attending DR screening from The Danish National Registry of Diabetic Retinopathy (cases, n = 205,970) to an age- and gender-matched group of patients without diabetes (controls, n = 1,003,170). In the cross-sectional study, a multivariable model demonstrated a lower prevalence of migraine among cases compared with controls (OR 0.83, 95% CI 0.81–0.85), with a lower risk in cases with DR than in those without (OR 0.69, 95% CI 0.65–0.72). In the prospective study, a lower risk of incident migraine was found in a multivariable model in cases (HR 0.76, 95% CI 0.70–0.82), but this did not depend upon the presence of DR. To conclude, in a national study of more than 1.2 million people, patients screened for DR had a lower risk of present migraine, but DR was not a protective marker of incident migraine.
Similar content being viewed by others

Introduction
Migraine is a comprehensive and disabling disease that affects around 11% of the adult population worldwide1. It is believed to originate from a combination of environmental, genetic, and hormonal causes, with an overrepresentation in women2,3,4. Diseases such as heart disease and hypertension are associated with an increased the risk of developing migraine5. Previous findings have reported a relation between migraine and the occurrence of hypoglycemia attacks and longer duration of type 1 diabetes6. However, there are conflicting results in this field as both type 1 and type 2 diabetes have been associated with a decreased risk of migraine, especially in older patients7,8,9. The pathophysiological explanation for this is not entirely clarified, but a proposed mechanism involves both a neurogenic and a vascular component10.
It is commonly known that diabetes leads to long term macro- and microvascular complications such as cardiovascular disease (including hypertension), peripheral neuropathy, nephropathy and diabetic retinopathy (DR)11. The vascular damage includes endothelial dysfunction and increased angiogenesis that consequently cause arteriosclerosis and reduced blood flow to nerves12,13. Migraine is believed to be caused by a combination of vasogenic and neurogenic factors with vasodilation of vessels and overactivation of impulses from sensory nerves10. In diabetes and in patients with retinal vascular abnormalities, the damage of nerves and the alteration of vessels from arteriosclerosis could be a plausible explanation of the lower prevalence of migraine in patients with diabetes14,15. The level of DR is known to increase in severity with longer duration of disease, poorly controlled HbA1c, increased blood lipids and hypertension16,17,18,19,20, making DR a good indicator of disease severity in diabetes. An insight into the association between level of DR and migraine could contribute to a better understanding of the overall impact of DR and the interaction between DR and extraocular diseases.
Therefore, the purpose of this study was to examine DR as a marker of prevalent and 5-year incident migraine in a national cohort of patients, who have attended DR-screening in comparison with an age- and gender-matched group of non-diabetec controls.
Research design and methods
This study was a matched register-based cohort study. The study population consisted of Danish patients with diabetes registered in The Danish National Registry of Diabetic Retinopathy (DiaBase)21. The DiaBase is a national quality database containing data of 205,970 patients with diabetes, who attend the national screening program for DR. Patients are screened by ophthalmologists according to evidence-based national clinical guidelines, and it is mandatory to report screening results to the database. Data includes the level of DR, which is graded according to the International Clinical DR severity scale22 as levels 0 (no DR), 1–3 (mild, moderate, and severe non-proliferative DR) or 4 (proliferative DR). The level of DR was determined by the worse eye. Grading of DR was performed as a combination between evaluation by fundus photos and fundus evaluation by slit-lamp bio microscopy or with one of the methods alone. The following registers and databases were used to collect and link data: the Danish National Prescription Registry (DNPR)23, National Patient Register (NPR), and the Danish Civil Registration System (CPR)24. A further description of each database can be found elsewhere25.
Patients with diabetes (cases) were included from the date of first registration in DiaBase between 2013 and 2018 (index date) and matched 1:5 by year of birth and gender (controls). Controls were assigned the same index date as their matching cases and subsequently excluded if they were registered with a diabetes International Classifications of Disease (ICD)-10 code (E10 or E11) and/or Anatomical Therapeutic Chemical Classification (ATC) = A10A* or A10B*. This exclusion was performed after the 1:5 matching to exclude the diagnosis of diabetes in the control group. Persons with missing data in exposure, outcome or selected confounders were not included in this study, thus we only used a complete data set.
Patients with migraine were identified in NPR through ICD codes for migraine (G43) and treatment of migraine (BAHY2). The DNPR was searched for ATC codes for treatment of migraine, including triptans (N02CC), pizotifen (MN02CX08), and galcanezumab (MN02CX08) with inclusion if the presence of more than one redeemed prescription within a year. Data were linked on person-level from the registers used in this study (NPR, CPR, ITC/ATC). Linked data from the various registers was performed by using the pseudonymized civil registration number (CPR), which is uniquely identifiable, and which is assigned to all citizens in Denmark. This minimizes the risk of bias associated with linkage of data.
The primary endpoint was 5-year incident migraine measured with adjusted hazard ratio (HR) by level of DR at baseline. The secondary endpoint was migraine at index date measured with adjusted odds ratio (OR) by level of DR.
The selection of possible confounders was based on a priori decision. We included data regarding age at first screening for DR, gender, type and duration of diabetes, marital status, Charlson Comorbidity Index (CCI) score26, and use of specific medication (insulin, other glucose lowering drugs, and cholesterol lowering drugs). The definition of types of diabetes and codes can be found in supplementary Table S1.
Statistical analyses
Continuous variables are presented as median with interquartile range (IQR) and categorical variables as frequencies and percentages. We tested for trend with Cuzick's extension of the Wilcoxon rank-sum test for all groups (Table 1). Odds ratios (OR) with 95% confidence interval (CI) for migraine in the cross-sectional study (Tables 3, 4 and Supplementary Table S3) were estimated in crude, age and gender adjusted, and multivariable logistic regression models. Cox proportional hazards regression was used to estimate hazard ratios (HR) with 95% CI for the association between DR and migraine in the prospective study (Tables 3 and 4) in a crude, age and gender adjusted, and a multivariable model. In Tables 2 and 4, we used patients with level 0 as the control group to compare with all other levels of DR. We performed these sub-analyses to eliminate diabetes as the cause of lower prevalence and incidence of migraine and focus on the association between migraine and DR alone. For the analyses, patients with diabetes were stratified according to the level of DR. Cases and controls were both excluded from the prospective study if they were diagnosed with migraine before the index date. We also performed a sub analysis on both HR and OR in the part of the study cohort younger than 55 years, as prevalence of migraine is known to decline above this age27. We performed this analysis in both cases and controls to examine, if an assumed higher prevalence of migraine in this younger part of the study cohort reveals additional differences between cases and controls. prevalence of migraine would increase in a younger population.
P-values below 0.05 and CI’s that did not include 1.0 were considered statistically significant. All statistics were performed using Stata version 16.1 (StataCorp LLC, College Station, TX, USA). All authors had access to the database population in this study.
Ethics
This project was approved by The Danish Data Protection Agency before conduction. All data applied were pseudo-anonymized. All methods were carried out in accordance with The Danish Data Protection Agency guidelines and regulations.
Results
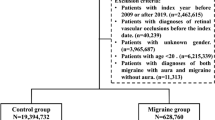
In this study, we included 205,970 cases from the DiaBase and 1,003,170 matched controls without a diabetes diagnose and no prescriptions of antidiabetic drugs. A flow chart showed in- and exclusion of the study population is presented in Fig. 1.

Flow chart of inclusion and exclusion. Flowchart showing patient progression in the study. Diabase: Danish Registry of Diabetic Retinopathy; DR: Diabetic Retinopathy; CPR: The Danish Civil Registration System; ICD: International Classification of Disease; ATC: Anatomical Therapeutic Chemical Classification System.
Characteristics of patients with diabetes are shown in Supplementary Table S2. The study population, who participated in the Danish eye screening program for DR, were more likely to be men, they were more likely diagnosed with type 2 diabetes, married, and having a lower score on CCI. Patients registered with migraine were more likely to be registered with DR level 0, and median age decreased with increasing levels of DR. Patients with type 1 diabetes had a higher level of DR compared to patients with type 2 diabetes and the median duration of diabetes was highest for patients with level 4 DR and type 1 diabetes (20.5 ± 2.7 years). CCI score 1–3 was more likely in patients with level 4 DR, and use of insulin increased with higher levels of DR. The opposite was present for glucose lowering treatment, excl. insulins. The use of antihypertensive drugs was similar for levels 0–3 DR (74.1–76.9%) but higher in level 4 DR (86.0%). The prevalence of migraine was lower in patients with higher levels of DR.
The OR and prevalence for migraine for patients with diabetes in the DiaBase according to the level of DR in comparison with controls are eluded in Table 1. We found a lower prevalence of 17% lower prevalence of migraine in patients with diabetes (OR (95% CI): 0.83 (0.81;0.85)) compared to age- and gender matched controls without diabetes in the multivariable model with prevalence increasing with increasing levels of DR. The same results were present when dividing patients with diabetes into type 1 and type 2 diabetes (Supplementary Tables S3 and S4). We found an interaction between age and DR at index date and therefore present results stratified by age in Supplementary Table S5. When using patients with DR level 0 as the reference group (Table 2), we observed a lower presence of migraine overall (OR (95% CI): 0.69 (0.65–0.72)) and for all levels (1–4) of DR individually compared to level 0.
The HR for developing migraine for patients screened for DR by level of DR and controls are displayed in Table 3. Patients with diabetes (cases) had a lower risk of developing migraine (level 1–4 HR (95% CI): 0.66 (0.55–0.80)) compared to controls (Table 3). This was especially apparent for DR level 4 in the multivariable model (HR: 0.53 95% CI: 0.32–0.88). Furthermore, this risk was especially low in patients with type 1 diabetes (level 1–4 HR (95% CI): 0.55 (0.42–0.73)) (Supplementary Table S6). When using patients with DR level 0 as the reference group, there were no statistically significant differences in risk of migraine in any of the groups (Table 4). This was also apparent when dividing patients into type 1 and type 2 diabetes, except for the crude model in type 2 diabetes, where there was a 33% less risk of developing migraine in the 5-year prospective study (level 0 vs. level 1–4 HR (95% CI): 0.67 (0.47–0.97)) (Supplementary Table S7).
Sub analyses on both HR and OR on the population (also divided into type 1 and type 2 diabetes) where we excluded patients older than 55 years did not alter the above-mentioned results (results not shown).
Discussion
In this study, we found a lower prevalence of migraine amongst patients with diabetes within all levels of DR (including level 0) compared to age- and gender matched controls without diabetes. We also found a lower incidence of migraine among patients with diabetes, but this did not depend upon the presence of DR, suggesting that diabetes may act as a protecting marker of migraine.
This is partly in line with previous findings of a lower prevalence of migraine in patients with diabetes compared to matched controls without7,8,9. However, these studies did not explore the relation with DR which this study adds new insights into. Though the complete pathophysiology is not known in detail, a proposed mechanism behind migraine includes a combination of vasogenic and neurogenic factors, including vasodilation and overactivation of nerves10,28. It could be hypothesized that arteriosclerosis of vessels present in patients with diabetes and DR15, leads to increased stiffness29 with reduced ability to dilate the vessels30, which in turn will cause an inadequate response to impulses in brain vessels associated with migraine. Furthermore, DR also possesses neurodegenerative aspects, which could, furthermore, lead to a weaker response31,32,33. Activation of glial cells via cellular pathways have shown to increase the pain-response in migraine34. Müller cells are thought to be the principal glial cell of the retina, and dysfunction of these cells has been proposed to play an important part in the development of DR35. Furthermore, hyperglycemia have shown to cause apoptosis of retinal Müller cells in a rat model36. However hypothetical, dysfunction and apoptosis of these cells may represent similar mechanisms present in glial cells in migraine causing decreased pain response. The degree of DR could perhaps act as a predictor of the development of migraine with more severe stages being protective because of the aforementioned pathophysiological mechanisms. However, as the results presents, it is not quite clear yet whether diabetes or the degree of DR is the main cause for a lower prevalence of migraine.
Calcitonin gene-related peptide (CGRP) is thought to play an important role in inducing the response occurring during a migraine attack by its vasodilating effect37. In rats, it has been shown that the apoptosis of retinal cells that is present in DR was confined to the ganglion cell layer. CGRP is normally located in the ganglion cell layer38 of the retina. As this layer is often affected by apoptosis in DR, it is possible the production of CGRP may decline. It can be speculated whether this mechanism is also present in other cells in the body, with the general metabolic stress that is present in diabetes39. This could possibly reduce the production of CGRP and therefore be protective against migraine attacks, as CGRP normally causes vasodilation.
When applying level 0 DR as the reference group the prevalence of migraine was lower overall (31%) making the association between DR and migraine evident (Table 2). This implies that diabetes is not the sole cause of less prevalent migraine, as other aspects such as HbA1c could also play a role. In the prospective study, where level 1–4 DR was compared to level 0, there were no associations between migraine and DR.
A previous study by Hagen et al. only found an inverse relationship between prevalent migraine in patients with type 1 diabetes but not in those with type 2 diabetes7. In our study we found that prevalent migraine was lower in both type 1 and type 2 diabetes. Although the age of patients in Hagen’s study population was similar to ours, the sample size was much smaller. Our results are furthermore supported by another previous study by Berge et al. that found lower prevalent migraine in both persons using insulin alone and persons using non-insulin diabetes medication only; however, this was only present in patients from the age of 508. Conversely, our study found that this was present in patients with diabetes both above and under 55 years of age in incident migraine. Berge et al. only used prescriptions of medication to categorize patients, where our study participants were categorized by a clinical diagnosis of type of diabetes. Both types of categorizations of diabetes offer uncertainties, and it is difficult to conclude why results are conflicting. We did not find any differences between prevalent migraine when dividing patients into type 1 and type 2 diabetes, although these results should be analyzed with caution, because of the low number of patients.
The prevalence of migraine is presumably underestimated, both because of under-diagnosis by health care staff, but also because patients do not always seek professional health care for their symptoms and self-medicate instead1. This underestimation could very well be present in this study as well, as we relied on the registered prescription of migraine medication. It cannot be excluded that there are patients that suffer from migraine but sufficiently manage to self-medicate with non-prescription medicine. These would not be accounted for in this study, which could have caused an underrepresentation of patients with a mild degree of migraine. This underestimation would most likely be present among controls, as patients with diabetes are regularly in contact with health care systems and may have a higher probability to be treated for migraine.
Limitations of this study included that we did not have data of hemoglobin A1c (HbA1c) and racial background. Likewise, migraine is in particular present in younger persons40, and given that the average age for our cohort was 65 years, migraine may be underrepresented compared to the general population. Furthermore, a course of 5 years may not be enough to follow a development in migraine. Another possible cause of underestimation of migraine in the diabetes population of this study could be the use of angiotensin-converting enzyme inhibitors which in some studies has been suggested to work beneficial in reducing migraine symptoms41. Another possible limitation involves the fact that our data did not include information about body mass index (BMI), as obesity have previously been associated with migraine with increased prevalence and increased number of attacks in both a Norwegian and Chinese population42,43. Finally, our study may not have been powered to associate migraine with higher levels of DR, as we had a relatively low number of those patients. Misclassification bias should always be taken into consideration when completing a register-based study. Patients in the control group could potentially have diabetes without this being registered and this may be a limitation as well.
Strengths of this study included the large sample size with the inclusion of a full national cohort of patients attending the national eye screening program for DR. Furthermore, access to well-established databases and national registers gave us relevant and important information about the level of DR comorbidities and medication use.
Conclusively, in a national study of more than 1.2 million people, patients screened for DR had a lower risk of present migraine. However, we could not demonstrate that the presence and degree of DR was a biomarker of protection of incident migraine. These results suggest that DR and especially diabetes, in combination, acts as a protector against developing migraine. Furthermore, it provides important insight into the degree to which DR is associated with other components of the body, in this instance the brain. These results provide new insights into the complex aspects of the pathophysiological mechanisms in diabetes and DR which provide further knowledge in the understanding of these diseases.
Data availability
Protocol, raw data, and computing code required to replicate the results in our report can be obtained by contacting corresponding author upon reasonable request.
Abbreviations
- ATC:
-
Anatomical Therapeutic Chemical Classification
- CCI:
-
Charlson Comorbidity Index
- CGRP:
-
Calcitonin gene-related peptide
- Diabase:
-
The Danish National Registry of Diabetic Retinopathy
- DNPR:
-
Danish National Prescription Registry
- DR:
-
Diabetic retinopathy
- ICD:
-
International Classifications of Disease
- NPR:
-
National Patient Register
References
World Health Organization and Lifting the burden: Atlas of Headache Disorders and Resources in the World (2011).
Broner, S. W., Bobker, S. & Klebanoff, L. Migraine in women. Semin. Neurol. 37(06), 601–610 (2017).
Stovner, L. J., Zwart, J. A., Hagen, K., Terwindt, G. M. & Pascual, J. Epidemiology of headache in Europe. Eur. J. Neurol. 13(4), 333–345 (2006).
Piane, M. et al. Genetics of migraine and pharmacogenomics: Some considerations. J. Headache Pain 8(6), 334–339 (2007).
Fernández-de-las-Peñas, C. et al. Has the prevalence of migraine changed over the last decade (2003–2012)? A Spanish population-based survey. PLoS ONE 9(10), e110530 (2014).
Haghighi, F. S. et al. Migraine and type 2 diabetes; is there any association?. J. Diabetes Metab. Disord. 15(1), 37 (2016).
Hagen, K. et al. Inverse relationship between type 1 diabetes mellitus and migraine. Data from the Nord-Trøndelag Health Surveys 1995–1997 and 2006–2008. Cephalalgia 38(3), 417–426 (2017).
Berge, L. I. et al. Does diabetes have a protective effect on migraine?. Epidemiology 24(1), 129–134 (2013).
Kurth, T. et al. Migraine and risk of cardiovascular disease in women: Prospective cohort study. BMJ 353, i2610 (2016).
Cutrer, F. M. & Charles, A. The neurogenic basis of migraine. Headache J. Head Face Pain 48(9), 1411–1414 (2008).
Federation ID: IDF Diabetes Atlas, 9th edn. https://www.diabetesatlas.org (2019).
Martin, A., Komada, M. R. & Sane, D. C. Abnormal angiogenesis in diabetes mellitus. Med. Res. Rev. 23(2), 117–145 (2003).
Sawada, N. & Arany, Z. Metabolic regulation of angiogenesis in diabetes and aging. Physiology 32(4), 290–307 (2017).
Hosoda, K. et al. Prediction of hyperperfusion after carotid endarterectomy by brain SPECT analysis with semiquantitative statistical mapping method. Stroke 34(5), 1187–1193 (2003).
Rose, K. M. et al. Migraine and retinal microvascular abnormalities. Neurology 68(20), 1694 (2007).
Cheung, N., Mitchell, P. & Wong, T. Y. Diabetic retinopathy. Lancet 376(9735), 124–136 (2010).
Group UPDS. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. BMJ 317(7160), 703 (1998).
Trial DCaC. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N. Engl. J. Med. 329(14), 977–986 (1993).
Chew, E. Y. et al. The effects of medical management on the progression of diabetic retinopathy in persons with type 2 diabetes: The Action to Control Cardiovascular Risk in Diabetes (ACCORD) Eye Study. Ophthalmology 121(12), 2443–2451 (2014).
Aiello, L. P., Cahill, M. T. & Wong, J. S. Systemic considerations in the management of diabetic retinopathy. Am. J. Ophthalmol. 132(5), 760–776 (2001).
Andersen, N. et al. The Danish Registry of diabetic retinopathy. Clin. Epidemiol. 8, 613–619 (2016).
Wilkinson, C. P. et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology 110(9), 1677–1682 (2003).
Wallach Kildemoes, H., Toft Sørensen, H. & Hallas, J. The Danish National Prescription Registry. Scand. J. Public Health 39(7), 38–41 (2011).
Pedersen, C. B. The Danish Civil Registration System. Scand. J. Public Health 39(7), 22–25 (2011).
Grauslund, J. et al. Interactions between ocular and systemic disease using national register-based data in the Danish Excellence Centre in Ophthalmic Epidemiology (DECODE-EYE): Study perspective. Acta Ophthalmol. 98, 573–578 (2020).
Quan, H. et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 173(6), 676–682 (2011).
Buse, D. C. et al. Chronic migraine prevalence, disability, and sociodemographic factors: Results from the American Migraine Prevalence and Prevention Study. Headache 52(10), 1456–1470 (2012).
Babayan, L., Mamontov, O. V., Amelin, A. V., Bogachev, M. & Kamshilin, A. A. Arterial hypertension in migraine: Role of familial history and cardiovascular phenotype. Auton. Neurosci. 203, 103–107 (2017).
Díez, J. Arterial stiffness and extracellular matrix. Atheroscler. Large Arteries Cardiovasc. Risk. 44, 76–95 (2007).
Kaur, R., Kaur, M. & Singh, J. Endothelial dysfunction and platelet hyperactivity in type 2 diabetes mellitus: Molecular insights and therapeutic strategies. Cardiovasc. Diabetol. 17(1), 121–121 (2018).
Mendonca, H. R., Carpi-Santos, R., da Costa, C. K. & Blanco Martinez, A. M. Neuroinflammation and oxidative stress act in concert to promote neurodegeneration in the diabetic retina and optic nerve: Galectin-3 participation. Neural Regen. Res. 15(4), 625–635 (2020).
Rolev, K. D., Shu, X. S. & Ying, Y. Targeted pharmacotherapy against neurodegeneration and neuroinflammation in early diabetic retinopathy. Neuropharmacology 187, 108498 (2021).
Mrugacz, M., Bryl, A. & Zorena, K. Retinal vascular endothelial cell dysfunction and neuroretinal degeneration in diabetic patients. J. Clin. Med. 10(3), 458 (2021).
Iyengar, S., Johnson, K. W., Ossipov, M. H. & Aurora, S. K. CGRP and the trigeminal system in migraine. Headache 59(5), 659–681 (2019).
Coughlin, B. A., Feenstra, D. J. & Mohr, S. Müller cells and diabetic retinopathy. Vis. Res. 139, 93–100 (2017).
Jiang, Y. et al. Pioglitazone normalizes insulin signaling in the diabetic rat retina through reduction in tumor necrosis factor α and suppressor of cytokine signaling 3. J. Biol. Chem. 289(38), 26395–26405 (2014).
Haanes, K. A. & Edvinsson, L. Pathophysiological mechanisms in migraine and the identification of new therapeutic targets. CNS Drugs 33(6), 525–537 (2019).
Yang, J.-H. et al. STZ treatment induced apoptosis of retinal cells and effect of up-regulation of calcitonin gene related peptide in rats. J. Diabetes Complicat. 27(6), 531–537 (2013).
Nolan, C. J., Damm, P. & Prentki, M. Type 2 diabetes across generations: From pathophysiology to prevention and management. Lancet 378(9786), 169–181 (2011).
Lipton, R. B. & Bigal, M. E. Migraine: Epidemiology, impact, and risk factors for progression. Headache 45(Suppl 1), S3-s13 (2005).
Sadat-Ebrahimi, S. R. et al. An evidence-based systematic review of the off-label uses of lisinopril. Br. J. Clin. Pharmacol. 84(11), 2502–2521 (2018).
Kristoffersen, E. S., Børte, S., Hagen, K., Zwart, J. A. & Winsvold, B. S. Migraine, obesity and body fat distribution—A population-based study. J. Headache Pain 21(1), 97 (2020).
Huang, Q., Liang, X., Wang, S. & Mu, X. Association between Body Mass Index and migraine: A survey of adult population in China. Behav. Neurol. 2018, 6585734 (2018).
Funding
Source of funding for this study was guaranteed by The Velux Foundation, Denmark. The funding body had no role in the design or execution of this study and had no part in the writing of the manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to (1) conception and design, acquisition of data or analysis and interpretation of data, and (2) drafted or revised the article, and (3) gave their final approval of the version to be published. First author, A.S.V. is the guarantor of this work, and each author had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Vergmann, A.S., Stokholm, L., Rubin, K.H. et al. Investigation of the correlation between diabetic retinopathy and prevalent and incident migraine in a national cohort study. Sci Rep 12, 12443 (2022). https://doi.org/10.1038/s41598-022-16793-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-16793-0
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
