
Abstract
Patients with neuromuscular disease often suffer from weak and ineffective cough resulting in mucus retention and increased risk for chest infections. Different airway clearance techniques have been proposed, one of them being the insufflator/exsufflator technique. So far, the immediate physiological effects of the insufflator/exsufflator technique on ventilation distribution and lung volumes are not known. We aimed to describe the immediate effects of the insufflator/exsufflator technique on different lung volumes, forced flows and ventilation distribution. Eight subjects (age 5.8–15.2 years) performed lung function tests including spirometry, multiple breath washout and electrical impedance tomography before and after a regular a chest physiotherapy session with an insufflator/exsufflator device. Forced lung volumes and flows as well as parameters of ventilation distribution derived from multiple breath washout and electrical impedance tomography were compared to assess the short-term effect of the therapy. In this small group of stable paediatric subjects with neuromuscular disease we could not demonstrate any short-term effects of insufflation/exsufflation manoeuvres on lung volumes, expiratory flows and ventilation distribution. With the currently used protocol of the insufflation/exsufflation manoeuvre, we cannot demonstrate any immediate changes in lung function.
Similar content being viewed by others

Background
Effective cough is a protective mechanism against respiratory tract infections and an important part of mucus clearance of the lung. Ineffective cough is a major cause of morbidity and mortality in patients with neuromuscular disease (NMD). Inspiratory and expiratory muscle weakness, hypoventilation and increasingly impaired cough competence are thought to cause frequent atelectasis and chest infections1,2. Additionally, the progressive decline in lung volume is associated with ventilation inhomogeneity3. A normal cough requires the inspiratory muscles to inspire to up to 85–90% of vital capacity (VC) followed by rapid closure of the glottis. Contraction of the expiratory muscles (abdominal and intercostal) causes an intrapleural pressure of 190 cmH2O and more which, in combination with the opening of the glottis, generates transient peak cough flows (PCF) of 360–1200 l/min4,5. While normally the inspiratory volume reaches 80–90% of VC before coughing, for an effective cough at least 50% of VC must be inspired6,7. Due to muscle weakness and reduced respiratory system compliance neither the deep inspiration nor the forced expiratory manoeuvre is feasible for patients with NMD. This reduction in compliance is most probably due to micro-atelectasis caused by inspiratory muscle weakness and also due to changes in the elastic recoil of the lung and reduced chest wall compliance8,9,10.
Chest physiotherapy is an important cornerstone of the regular daily treatment in these patients. Depending on cooperation different techniques are used ranging from completely passive vibration vests to active breathing techniques11,12,13. All these techniques are time and energy consuming. During respiratory infections patients are quickly exhausted and prone to the vicious cycle of secretions, fatigue and further accumulation of secretions.
Cough assist techniques were developed for patients who present with weak cough. The therapy basically pursues two goals. First, it increases the expiratory airflow that occurs during cough, by assisting inspiration and/or expiration, thus increasing cough efficacy. Second, it aims to maintain lung volume and respiratory system compliance by active insufflation of air. A mechanical insufflator/exsufflator uses positive pressure via a facemask or mouthpiece to deliver a maximal lung inspiratory volume, followed by an abrupt switch to negative pressure to the airway for forced expiration, which should transport mucus to the central airways and out of the patient. The rapid change from positive to negative pressure simulates airflow changes experienced during a normal cough manoeuver with the high expiratory airflow carrying mucus upstream. Mellies and Goebel demonstrated that the pressure required to achieve the highest PCF in young adults with NMD was 27mbar14. Daily use of the insufflator/exsufflator device leads to a reduction in acute pulmonary exacerbations, better clearing during the exacerbations and better overall ventilation while preventing atelectasis and hypoxia3,15,16,17.
Already back in 1952 Barach and Beck demonstrated clinical and radiographic improvement in 92 out of 103 acutely ill patients with respiratory tract infections with the use of a cough assist device, in a study that included 72 patients with lung disease and 27 with skeletal or neuromuscular disease18. Greater improvements were seen in patients with NMD. A similar effectiveness in airway clearance was seen with conventional physiotherapy but the treatment time needed to clear secretions was longer with the latter treatment15.
The safety, tolerance and clinical effectiveness of the mechanical insufflation/exsufflation in 62 paediatric patients with NMD was studied by Miske et al.16 the authors concluded that the use of a cough assist device was safe, well tolerated and effective in preventing pulmonary complications in 90% of their population. A retrospective study by Veldhoen et al.17 revealed a significantly lower number of respiratory tract infections requiring hospital admission after the introduction of the mechanical insufflation/exsufflation. Stehling et al.3 could demonstrate an increase in vital capacity within one year after the introduction of the therapy and its stabilisation in the second year. In the mentioned studies, no barotrauma such as air leaks have been reported, although there are some case reports in adult patients19,20.
Despite the low level of evidence for long-term benefits the British Thoracic Society published recommendations for the use of augmented cough techniques in children with ineffective cough21.
Having only few studies on long-term effects, there is even less literature on short-term effects of mechanical insufflation/exsufflation on lung function parameters, especially in children. In a group of stable subjects with Duchenne muscular dystrophy (DMD) including some adolescents, a single treatment showed a change in breathing pattern, i.e. decreased breathing rate and less shallow breathing. No changes in lung-volume recruitment or unassisted cough peak flow could be demonstrated22. Another study in a small group of adult subjects with DMD demonstrated a short-lasting positive effect on chest-wall motion asymmetry and a small but significant increase of vital capacity23.We therefore aimed to quantitatively and qualitatively describe the short-term effect of the insufflation/exsufflation manoeuvres on ventilation distribution and other lung function parameters in subjects with NMD. We hypothesised that an insufflation/exsufflation treatment session leads to short-term changes in ventilation inhomogeneity.
Material and methods
Patients with NMD in stable conditions using a mechanical insufflator/exsufflator regularly at home were recruited at the specialised NMD outpatient clinics of a tertiary center, the University Children’s Hospital of Bern, after written informed consent by the parents. Patients were screened consecutively at each visit by the involved physiotherapist.
This observational study was approved by the Ethics committee of the Canton of Bern, Switzerland (KEK Nr. 2018-01507) and performed according to the current version of the Declaration of Helsinki and the Swiss Law for Human Research. The study was funded through a grant from the Swiss Foundation for Research on Muscle Diseases. (FSRMM; www.fsrmm.ch) The foundation was not involved in the planning or conduct of the experiments, data analysis and interpretation, the writing of the manuscript or its submission.
Inclusion criteria
-
confirmed diagnosis of a NMD
-
functional status: non-ambulatory
-
age > 5 years and < 16 years
-
able to cooperate
-
daily home-use of cough assist as reported by the caregivers
Exclusion criteria
-
acute respiratory infection (marked increase in cough, change in sputum amount or colour, fever or malaise)
-
oxygen dependency (defined as need for oxygen to achieve a transcutaneous oxygen saturation of ≥ 92%)
-
skin lesions at the chest
Observed standardised procedure
After the baseline assessment, the participants performed their usual insufflator/exsufflator therapy session under supervision of a physiotherapist. Commonly in our institution a therapy session consists of 5 series of 5 insufflation/exsufflation manoeuvres each (Cough assist E70, Philips Respironics, Hamburg, Germany). Positive and negative pressures were set at the individual level of each subject.
Measurements
Ventilation distribution was assessed by electrical impedance tomography (EIT) and multiple breath washout (MBW). Forced expiratory flows were measured by spirometry. These parameters were obtained five minutes before (baseline) and ten minutes after the treatment session (“post treatment”). Additionally EIT measurements were performed continuously during the treatment session.
Electrical impedance tomography
EIT is a non-invasive, radiation-free technique for the assessment of spatial and temporal ventilation distribution based on the changes in electrical properties of the tissue during the respiratory cycle. EIT measurements were performed using a commercially available setup (PulmoVista 500, Draeger, Germany). Image reconstruction was performed with the GREIT-algorithm using the torso mesh function24. Relative change in end-expiratory lung impedance (EELI) and a measure of ventilation inhomogeneity i.e. the global inhomogeneity (GI) index were calculated as described previously using customized software (Matlab R2013a, The MathWorks Inc., Nattick, MA, USA)25,26,27.
Multiple breath washout
All participants performed three trials of standard N2MBW until 1/40th of initial starting end-tidal N2 concentration according to the ERS consensus using an ultrasonic flowmeter equipment (Exhalyzer D, with Spiroware software, EcoMedics AG, Duernten, Switzerland)28,29. The resting time in between MBW trials was at least five minutes. The following parameters were calculated: lung clearance index (LCI), functional residual capacity (FRCMBW).
Spirometry was performed in three trials according to the ERS/ATS standards30 using the spirometer of a body plethysmograph (Jaeger Master-Screen Body/Diff device, CareFusion, Hoechberg, Germany). Forced expiratory volume in the 1st s (FEV1), forced vital capacity (FVC), peak expiratory flow (PEF), maximum expiratory flow at 50% vital capacity (MEF50) and forced mid-expiratory flow (FEF25-75) were assessed.
Outcome measures
Primary outcome measures are the change in ventilation distribution assessed by N2MBW (LCI) and EIT (GI).
Secondary outcome measures include changes in forced expiratory flows and changes in end-expiratory lung volume from before to after the treatment session, breath by breath changes in EELI during the insufflation/exsufflation manoeuvre and the ratio of EIT amplitude (i.e. tidal volume) between insufflation/exsufflation manoeuvre and normal tidal breathing.
Statistics
Given the lack of data on short-term effects on ventilation distribution, the sample size calculation was performed based on a study in subjects with cystic fibrosis investigating the effect of a physiotherapy treatment session ventilation inhomogeneity assessed by single breath washout31. The estimated sample size for a paired test was eight.
All analyses were performed in Statsdirect® Vers 3.3.3 (StatsDirect Ltd., Merseyside, UK). Data are presented as median and range. Changes in lung function parameters (primary and secondary outcomes) were assessed using Wilcoxon rank sum test. A p-value < 0.05 is considered significant. Breath by breath differences in EELI during the manoeuvre were analysed by single sample t-test assuming a mean difference of zero.
Results
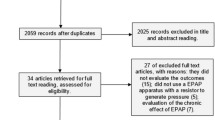
Between April 2019 and November 2019 eight subjects (age 5.8–15.2 years) fulfilling the inclusion criteria could be recruited for the study (Fig. 1). Demographic data, diagnosis and individual pressure settings of the insufflator/exsufflator device are shown in Table 1.

CONSORT Flow diagram.
EIT measurements and spirometry could be performed in all subjects, technically acceptable MBW measurements could be achieved in 6 subjects. One subject with SMA Type 1c and one subject with Muscular dystrophy Duchenne failed MBW quality criteria for leakage due to insufficient seal around the mouthpiece.
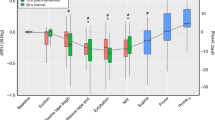
None of measured lung function parameters showed a significant difference between before and after an insufflation/exsufflation treatment session performed by a physiotherapist. All results are summarised in Table 2. The individual changes in the primary outcomes of each participant are shown in Fig. 2 and 3.

Individual changes in lung clearance index from baseline to post treatment.

Individual changes in global inhomogeneity index from baseline to post treatment.
The breath amplitudes during the treatment were median 1.53 (range 1.43–2.05) times higher than during tidal breathing. The EELI during the insufflation/exsufflation manoeuvre did not differ on a breath-by-breath basis (p = 0.73).
Discussion
In a small group of non-ambulatory subjects with neuromuscular disease, we found no changes in lung function parameters before and after a physiotherapy session with an insufflator/exsufflator device.
It is well known that subjects with NMD suffer from inspiratory and expiratory muscle weakness resulting in ventilatory failure, recurrent pulmonary infections and subsequently increased mortality32,33,34. Several studies suggest increased survival with the introduction of invasive and non-invasive ventilation33. Multiple other chest physiotherapy modalities are applied to improve airway clearance and to maintain vital capacity and effective cough35,36. Different studies investigating changes in lung volumes and cough efficacy show similar results. A small study by Katz et al.37 found that the decline in vital capacity was significantly attenuated, and assisted peak cough flow (PCF) was maintained in a clinically effective range. The same group followed 22 patients with DMD before and after the introduction of a lung volume recruitment technique (breath stacking). They demonstrated a significant reduction in loss of vital capacity over time after initiation of therapy38. Kang et al. observed an improvement of maximum inspiratory capacity in the majority of their patients trained to stacking delivered volumes of air to deep lung insufflation. Patients for whom the maximum inspiratory capacity increased also had a significant increase in assisted PCF despite having somewhat decreasing VCs and unassisted PCFs39. Stehling et al. performed a retrospective analysis of 21 patients with NMD. Before the introduction of mechanical insufflation/exsufflation vital capacity decreased from 0.71 ± 0.38 L to 0.50 ± 0.24 L in the last year and from 0.88 ± 0.45 L to 0.71 ± 0.38 L in the next to last year. In the first year, after regular use of mechanical insufflation/exsufflation vital capacity significantly increased by 28% (from 0.50 to 0.64 L). After the second year the vital capacity increase remained stable (0.64 vs. 0.65 L). The authors conclude that the regular use of mechanical insufflation/exsufflation might improve vital capacity in patients with neuromuscular disorders and severe lung volume restriction3.
The above presented studies all investigated mid- to long-term effects. Publications on short-term effects are very scarce. One study from Molgat-Seon et al. found an acute increase in respiratory system compliance immediately after lung volume recruitment (LVR) manoeuvres with a resuscitation bag in subjects with respiratory muscle weakness but not in controls. This effect could not be demonstrated any more one hour after the manoeuvre. LVR had no impact on lung volumes such as total lung capacity, functional residual capacity, inspiratory capacity and expiratory reserve volume. Peak expiratory flow was increased during LVR but not unassisted peak expiratory flow40. Another adult study by Meric et al.23 demonstrated positive effect on chest-wall motion asymmetry and a small but significant increase of vital capacity. The vital capacity return to baseline within one hour and the shallow breathing index increased significantly. Our data confirm the findings of Molgat-Seon et al. with a different LVR manoeuvre. Additionally, we can demonstrate that there is no short-term influence on ventilation distribution measured by LCI and also GIEIT. The difference of our findings to the latter study with respect to VC might be explained by the fact that an insufflation/exsufflation session can be tiring and potentially more so in children.
The main short-term aim of the insufflation/exsufflation technique is to improve cough and therefore expectoration of pulmonary secretions. Expiration is actively augmented with negative airway pressures. In doing so, airway clearance is enhanced eventually at the cost of the recruited lung volume achieved by the high inflation pressure. Therefore, short-term improvement of lung volumes and consecutively expiratory flows cannot be demonstrated in our investigation. We performed our measurement during a stable period without pulmonary exacerbations. The subjects are well trained in the application of the insufflation/exsufflation technique resulting in low amounts of secretion. The missing short-term effect of the therapy on ventilation distribution might indicate, that in these stable conditions neither secretions nor atelectasis are a major component of reversible ventilation inhomogeneity. Another explanation for our results might lie in negative pressures applied during expiration, leading to loss of a potentially recruited volume. Passive expiration after the last active insufflation or other techniques, such as air stacking might therefore be favourable in this respect. Insufflation/exsufflation manoeuvres can be tiring. This might be a further explanation for the lacking difference in VC, but not in ventilation homogeneity.
To our knowledge this is the first study evaluating not only lung volumes and expiratory flows but also measures of ventilation distribution to assess short-term effects LVR manoeuvres in subjects with NMD. Our lung function lab has a long standing experience and research interest in the applied lung function tests. All measurements hold the standard of ERS/ATS recommendations28,41.
Clearly a limitation of the presented study is the low number of subjects included. There are several reasons for this. First, for the sake of high quality lung function measurements, especially for ventilation distribution this work was designed as a single centre study. Second, to avoid heterogeneous results due to incorrect application of the insufflator/exsufflator, only subjects used to the therapy for several months were eligible for inclusion. One could argue that performing lung function measurements during a stable phase with respect to pulmonary symptoms is not the right time point to assess the therapy for short-term effects. This was a deliberate decision by the authors in order to gain insight into physiological conditions of these subjects. Furthermore, performing lung function tests during a pulmonary exacerbation is very stressful and not well tolerated at all by subjects with NMD.
Conclusion
In a small group of stable paediatric subjects with NMD we could not demonstrate any short-term effects of insufflation/exsufflation manoeuvres on lung volumes, expiratory flows and ventilation distribution. This suggests that the beneficial effects of this technique is based on repetitive airway clearance and not so on immediate changes in lung function. A theoretical short-term benefit of augmented lung volume might be achieved by passive expiration after the last insufflation of the treatment session.
Data availability
The datasets analysed during the current study are available from the corresponding author on reasonable request.
References
Finder, J. D. et al. Respiratory care of the patient with Duchenne muscular dystrophy: ATS consensus statement. Am. J. Respir. Crit. Care Med. 170, 456–465. https://doi.org/10.1164/rccm.200307-885ST (2004).
Seddon, P. C. & Khan, Y. Respiratory problems in children with neurological impairment. Arch. Dis. Childhood 88, 75–78 (2003).
Stehling, F., Dohna-Schwake, C., Mellies, U. & Grosse-Onnebrink, J. Decline in lung volume with Duchenne muscular dystrophy is associated with ventilation inhomogeneity. Resp. Care 60, 1257–1263. https://doi.org/10.4187/respcare.04025 (2015).
Dohna-Schwake, C., Ragette, R., Teschler, H., Voit, T. & Mellies, U. IPPB-assisted coughing in neuromuscular disorders. Pediat. Pulmonol. 41, 551–557 (2006).
Gregg, I. & Nunn, A. J. Peak expiratory flow in normal subjects. Br. Med. J. 3, 282–284 (1973).
Harris, R. S. & Lawson, T. V. The relative mechanical effectiveness and efficiency of successive voluntary coughs in healthy young adults. Clin. Sci. 34, 569–577 (1968).
Whittenberger, J. L. & Mead, J. Respiratory dynamics during cough. Trans. Ann. Meet. 48, 414–418 (1952).
De Troyer, A., Borenstein, S. & Cordier, R. Analysis of lung volume restriction in patients with respiratory muscle weakness. Thorax 35, 603–610. https://doi.org/10.1136/thx.35.8.603 (1980).
Estenne, M. et al. Lung volume restriction in patients with chronic respiratory muscle weakness: the role of microatelectasis. Thorax 48, 698–701. https://doi.org/10.1136/thx.48.7.698 (1993).
Estenne, M., Heilporn, A., Delhez, L., Yernault, J. C. & De Troyer, A. Chest wall stiffness in patients with chronic respiratory muscle weakness. Am. Rev. Respir. Dis. 128, 1002–1007. https://doi.org/10.1164/arrd.1983.128.6.1002 (1983).
Gauld, L. M. Airway clearance in neuromuscular weakness. Dev. Med. Child Neurol. 51, 350–355. https://doi.org/10.1111/j.1469-8749.2008.03260.x (2009).
Pryor, J. A. Physiotherapy for airway clearance in adults. Eur. Resp. J. 14, 1418–1424. https://doi.org/10.1183/09031936.99.14614189 (1999).
Strickland, S. L. Year in review 2014: airway clearance. Resp. Care 60, 603–605. https://doi.org/10.4187/respcare.04095 (2015).
Mellies, U. & Goebel, C. Optimum insufflation capacity and peak cough flow in neuromuscular disorders. Ann. Am. Thorac. Soc. 11, 1560–1568 (2014).
Chatwin, M. & Simonds, A. K. The addition of mechanical insufflation/exsufflation shortens airway-clearance sessions in neuromuscular patients with chest infection. Resp. Care 54, 1473–1479 (2009).
Miske, L. J., Hickey, E. M., Kolb, S. M., Weiner, D. J. & Panitch, H. B. Use of the mechanical in-exsufflator in pediatric patients with neuromuscular disease and impaired cough. Chest 125, 1406–1412 (2004).
Veldhoen, E. S. et al. Effect of mechanical insufflation-exsufflation in children with neuromuscular weakness. Pediat. Pulmonol. 55, 510–513. https://doi.org/10.1002/ppul.24614 (2020).
Barach, A. L., Beck, G. J., Bickerman, H. A., Seanor, H. E. & Smith, W. Physical methods simulating mechanisms of the human cough. J. Appl. Physiol. 5, 85–91 (1952).
McDonald, L. A. et al. Pneumothorax in neuromuscular disease associated with lung volume recruitment and mechanical insufflation-exsufflation. Respirol. Case Rep. 7, e00447. https://doi.org/10.1002/rcr2.447 (2019).
Suri, P., Burns, S. P. & Bach, J. R. Pneumothorax associated with mechanical insufflation-exsufflation and related factors. Am. J. Phys. Med. Rehabil. 87, 951–955. https://doi.org/10.1097/PHM.0b013e31817c181e (2008).
Hull, J. British Thoracic Society guideline for respiratory management of children with neuromuscular weakness: commentary. Thorax 67, 654–655 (2012).
Cesareo, A. et al. Acute effects of mechanical insufflation-exsufflation on the breathing pattern in stable subjects with Duchenne muscular dystrophy. Resp. Care 63, 955–965. https://doi.org/10.4187/respcare.05895 (2018).
Meric, H. et al. Short-term effect of volume recruitment-derecruitment manoeuvre on chest-wall motion in Duchenne muscular dystrophy. Chron. Respir. Dis. 14, 110–116. https://doi.org/10.1177/1479972316674413 (2017).
Adler, A. et al. GREIT: a unified approach to 2D linear EIT reconstruction of lung images. Physiol. Meas. 30, S35-55. https://doi.org/10.1088/0967-3334/30/6/S03 (2009).
Schnidrig, S., Casaulta, C., Schibler, A. & Riedel, T. Influence of end-expiratory level and tidal volume on gravitational ventilation distribution during tidal breathing in healthy adults. Eur. J. Appl. Physiol. 113, 591–598. https://doi.org/10.1007/s00421-012-2469-7 (2013).
Wettstein, M., Radlinger, L. & Riedel, T. Effect of different breathing aids on ventilation distribution in adults with cystic fibrosis. PLoS ONE 9, e106591. https://doi.org/10.1371/journal.pone.0106591 (2014).
Zhao, Z., Moller, K., Steinmann, D., Frerichs, I. & Guttmann, J. Evaluation of an electrical impedance tomography-based global inhomogeneity index for pulmonary ventilation distribution. Intens. Care Med. 35, 1900–1906. https://doi.org/10.1007/s00134-009-1589-y (2009).
Robinson, P. D. et al. Consensus statement for inert gas washout measurement using multiple- and single-breath tests. Eur. Resp. J. 41, 507–522 (2013).
Singer, F. et al. Practicability of nitrogen multiple-breath washout measurements in a pediatric cystic fibrosis outpatient setting. Pediat. Pulmonol. 48, 739–746 (2013).
Miller, M. R. et al. Standardisation of spirometry. Eur. Resp. J. 26, 319–338 (2005).
Abbas, C., Singer, F., Yammine, S., Casaulta, C. & Latzin, P. Treatment response of airway clearance assessed by single-breath washout in children with cystic fibrosis. J. Cyst. Fibros 12, 567–574. https://doi.org/10.1016/j.jcf.2013.05.010 (2013).
Dohna-Schwake, C., Ragette, R., Teschler, H., Voit, T. & Mellies, U. Predictors of severe chest infections in pediatric neuromuscular disorders. Neuromuscul. Disord. 16, 325–328. https://doi.org/10.1016/j.nmd.2006.02.003 (2006).
Ryder, S. et al. The burden, epidemiology, costs and treatment for Duchenne muscular dystrophy: an evidence review. Orphanet. J. Rare Dis. 12, 79. https://doi.org/10.1186/s13023-017-0631-3 (2017).
Toussaint, M., Steens, M. & Soudon, P. Lung function accurately predicts hypercapnia in patients with Duchenne muscular dystrophy. Chest 131, 368–375. https://doi.org/10.1378/chest.06-1265 (2007).
Chatwin, M. et al. Airway clearance techniques in neuromuscular disorders: a state of the art review. Respir. Med. 136, 98–110. https://doi.org/10.1016/j.rmed.2018.01.012 (2018).
Sheers, N., Howard, M. E. & Berlowitz, D. J. Respiratory adjuncts to NIV in neuromuscular disease. Respirology 24, 512–520. https://doi.org/10.1111/resp.13431 (2019).
Katz, S. L. et al. Long-term effects of lung volume recruitment on maximal inspiratory capacity and vital capacity in Duchenne muscular dystrophy. Ann. Am. Thor. Soc. 13, 217–222. https://doi.org/10.1513/AnnalsATS.201507-475BC (2016).
McKim, D. A., Katz, S. L., Barrowman, N., Ni, A. & LeBlanc, C. Lung volume recruitment slows pulmonary function decline in Duchenne muscular dystrophy. Arch. Phys. Med. Rehabil. 93, 1117–1122. https://doi.org/10.1016/j.apmr.2012.02.024 (2012).
Kang, S. W. & Bach, J. R. Maximum insufflation capacity. Chest 118, 61–65. https://doi.org/10.1378/chest.118.1.61 (2000).
Molgat-Seon, Y. et al. Lung volume recruitment acutely increases respiratory system compliance in individuals with severe respiratory muscle weakness. ERJ Open Res. https://doi.org/10.1183/23120541.00135-2016 (2017).
Loeb, J. S. et al. Acceptability and repeatability of spirometry in children using updated ATS/ERS criteria. Pediat. Pulmonol. 43, 1020–1024. https://doi.org/10.1002/ppul.20908 (2008).
Acknowledgements
We want to express our gratefulness to the ‘Swiss Foundation for Research on Muscle Diseases’ for financial support, to Katrin Roethlisberger for her support in study planning and ethics application, to Sharon Krattinger for the excellently performed lung function measurements and to all the children and parents for their effort and patience to achieve high quality lung function test.
Funding
The study was funded through a grant from the Swiss Foundation for Research on Muscle Diseases. (FSRMM; www.fsrmm.ch) The foundation was not involved in the planning or conduct of the experiments, data analysis and interpretation, the writing of the manuscript or its submission.
Author information
Authors and Affiliations
Contributions
C.C. and T.R. conceived and planned the study. F.M. and A.K. contributed to the subject recruitment. F.M. carried out the experiments. R.R. and T.R. carried out data and statistical analysis. C.C., A.K. and T.R. contributed to the interpretation of the results. C.C. took the lead in writing the manuscript. All authors provided critical feedback and helped shape the research, analysis and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
CC, FM, AK and RR do not have any competing interests to declare. TR does receive consulting fees from Sentec AG, Switzerland.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Casaulta, C., Messerli, F., Rodriguez, R. et al. Changes in ventilation distribution in children with neuromuscular disease using the insufflator/exsufflator technique: an observational study. Sci Rep 12, 7009 (2022). https://doi.org/10.1038/s41598-022-11190-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-11190-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
