
Abstract
Cancer incidence and survival rates have increased in the last decades and as a result, the number of working age people diagnosed with cancer who return to work. In this study the probability of accumulating days of employment and employment participation trajectories (EPTs) in a sample of salaried workers in Catalonia (Spain) who had a sickness absence (SA) due to cancer were compared to salaried workers with SA due to other diagnoses or without SA. Each individual with SA due to cancer between 2012 and 2015 was matched by age, sex, and onset of time at risk to a worker with SA due to other diagnoses and another worker without SA. Accumulated days of employment were measured, and negative binomial models were applied to assess differences between comparison groups. Latent class models were applied to identify EPTs and multinomial regression models to analyse the probability of belonging to one EPT of each group. Men and women without SA or with SA due to other diagnoses had at least a 9% higher probability of continuing in employment compared to workers who had a SA due to cancer, especially among men without SA (adjusted IRR 1.27, 95% CI 1.06‒1.53). Men without SA had the highest probability of having high stable EPT compared to workers who had a SA due to cancer (adjusted RRR 3.21, 95% CI 1.87‒5.50). Even though workers with SA due to cancer continue working afterwards, they do it less often than matched controls and with a less stable employment trajectory. Health and social protection systems should guaranty cancer survivors the opportunity to continue voluntary participation in the labour market.
Similar content being viewed by others


Introduction
The effect of cancer on paid work is a growing problem that needs adequate collaborative responses between health and social protection systems. Cancer is becoming a highly prevalent chronic disease with a 28% increase in its global incidence in the past few decades1,2,3. The survival rate is also increasing 3% per year4, 5, but cancer survivors suffer from long-lasting symptoms after the acute stage due to the disease and its treatment. In 2017, cancer caused an estimated 3,204,000 disability-adjusted life-years (DALYs)6, 7, impacting all dimensions of survivors’ life including their future working life.
Almost half of individuals diagnosed with cancer are of working age8. According to IARC estimations, the number of new cases among individuals aged 15–69 years worldwide was 221.6 per 100,000 in 20209. Although cancer is more likely to appear in older populations, the risk increases from 45 years of age10. Therefore, the steady increase in working age individuals diagnosed with cancer are expected to increase the number of people returning to work after treatment. Especially considering the delay in legal retirement age and the increasing tendency of workers to work beyond it11, although for workers with cancer after or close to legal retirement age , ending their working life is more likely than for cancer free workers12.
Return to work (RTW) could be beneficial for survivors´ health due to an increased sense of purpose, higher self‐confidence, and stronger sense of social belonging associated with employment13. RTW after a cancer diagnosis and treatment is considered a good prognostic sign. A successful RTW process is influenced by disease and treatment-related factors14,15,16, sociodemographic variables (age, sex, education level, marital status), and work and employment conditions, such as size and ownership of the organisation, physical and emotional job demands, working hours, type of job, attitudes of colleagues, type of contract, sick leave duration, and previous periods of unemployment17,18,19. Most cancer survivors attempt to RTW after treatment20, and studies have shown a steady increase in RTW as time after diagnosis increases21.
There is a growing consensus that work after cancer-survivorship research should address long-term work-related factors to understand the impact of cancer on the whole labour trajectory22. Previous studies have shown how surviving cancer has negative effects on labour market participation and employability. For example, compared to cancer-free controls of similar age, cancer survivors present reduced work ability, leading to higher unemployment rates23. Moreover, a recent study found that, among cancer survivors, low-educated males and workers employed in jobs requiring manual skills have the lowest probability of employment 4 years after diagnosis24. However, the future long term employment consequences and their shape over time hasn’t been addressed with life course approach methodologies while comparing the future working life after cancer with both workers with and without a disease.
Our hypothesis is that salaried workers who had cancer, recognised by a sickness absence (SA), are less likely to accumulate employment days in a stable trajectory when RTW than workers with SA due to other diagnoses or workers without SA. The objective of the present study was to evaluate differences in the probability of accumulating days of employment and employment participation trajectories (EPTs) in a sample of salaried workers in Catalonia (Spain) who had a SA due to cancer and compare them to workers who had a SA due to other diagnoses or no SA.
Methods
We performed a register-based cohort study among 1,548 salaried workers living in Catalonia (675 men and 873 women) from the Spanish WORKss cohort25, which is part of the Continuous Working Life Sample (CWLS), an annual random representative sample of 4% of affiliates of the Spanish social security system. Data available from the CWLS enables reconstruction of working life since 2006 based on the known information, such as occupational category, economic activity, employment status, and employment conditions (i.e., employment, unemployment, type of contract, income, and working time), social benefits (i.e., unemployment, permanent disability, and retirement), other work-related variables (i.e., company ownership and size), and date of death. Moreover, the Catalan Institute for Medical and Health Evaluations provided information related to SA records, including the medical diagnosis of the episode coded according to the 10th edition of the International Classification of Diseases (ICD-10), as well as the starting and ending date26.
The final sample included salaried workers who had had a SA due to a malignant neoplasm (ICD-10, C00-C97) between 2012 and 2015 (N = 516, 225 men and 291 women). For each individual from the WORKss cohort, we selected two comparison workers from the same week of that the SA due to cancer ended (i.e., similar onset of time at risk) and also matched by age (within a 5-year range) and sex. First, a salaried worker with a SA due to a medical diagnosis different from cancer (ICD-10: A00-U99, except C00-C97; N = 516, 225 men and 291 women) was selected, and then another salaried worker without a SA at that moment (N = 516, 225 men and 291 women; Supplementary Table 1). The average age of each of the three comparison groups in 2012 was 49.8 for men (standard deviation: 9.96) and 47.0 for women (standard deviation: 9.44).
The study period covered from the date the workers entered the cohort until December 31, 2018. The length of the study period for salaried workers who RTW after SA ranged from 3 to 6 years considering complete years (the final part of the period was censored). Each worker was followed until they ended employment because they became unemployed, retired, were recognised as having a permanent disability, or died, or until the end of the follow-up. If workers had discontinued employment periods during the study, all of them were added. We also had information about working life since 2006 until the end of the follow-up period.
RTW was assessed by the accumulated days of employment during the follow-up period (entrance to 31/12/2018). Potential confounders considered in our analysis were the occupational category (non-manual skilled, non-manual non-skilled, manual skilled, or manual non-skilled); working time categorised as a percentage of weekly hours (full-time [> 87.5%], part-time [50–87.5%], or short and marginal part-time [≤ 37.5%-49%]); type of contract (permanent or temporary); monthly average income in tertiles (high [> 2370.0 €], medium [1450.0–2370.0 €], or low [≤ 1450.0 €]); company size (small/medium [up to 100 employees] and big [> 100 employees]); company ownership (private and public); and economic activity (primary sector [agriculture, hunting, forestry, fishing, mining, and quarrying]; manufacturing, and services). We also considered the previous 5-year employment ratio expressed as a percentage of employed days to the total potential working days, including working or unemployed or not affiliated days. Workers who changed categories over time were assigned the category in which they spent most of the follow-up period.
Patients were not involved in any stage of the study. Confidentiality was maintained in both databases. The authors received data that were previously anonymised.
Statistical analysis
The sample was described according to response, explicative variables, and covariates mentioned above, and the chi-squared test was applied to assess significance between comparison groups. Negative binomial regression models were used to compare the probability of accumulating days of employment in salaried workers with SA due to cancer to workers with SA due to other diagnoses and without SA after testing for overdispersion through goodness-of-fit, which reports deviance, and Pearson chi-squared statistics. The estimator of this analysis, taking SA due to cancer as the reference group, was the incidence rate ratio (IRR), either the crude ratio or the ratio adjusted by all potential confounders mentioned above, and its 95% confidence interval (CI).
A second analysis was carried out to assess employment participation trajectories (EPTs) during follow-up in the three groups, applying latent class growth analysis (LCGA)27. The EPTs were obtained based on annually accumulated days of employment and estimated by assuming that they followed a quadratic function because it fit our data better than a linear function28. The optimal number of trajectories was chosen by considering the lowest Bayesian information criterion (BIC) and using the Lo-Mendell-Rubin adjusted and bootstrap likelihood ratio test (LMR-LRT)29. These tests indicated that the 4- and 3-trajectory model well-represented the EPT of our sample in both sexes. Nevertheless, due to the size of some of the trajectories and the principle of parsimony, we chose 3-trajectory models (Supplementary Table 2). The resulting EPT trajectories were described according to all potential confounders mentioned above, and chi-squared was applied to assess significance between EPTs. Finally, to measure the association between having a SA due to cancer and EPTs versus the comparison groups, we applied multinomial logistic regression with its relative risk ratio (RRR) and 95% CI.
All analyses were stratified by sex. Stata v.13 software was used for negative binomial models and multinomial regression models, and R version 4.1.0 and Mplus v.7 software were used for LCGA.
Ethics approval and consent to participate
This study was performed in accordance with the standards of Good Clinical Practice and the principles of the Declaration of Helsinki. The study protocol guaranteed the fulfilment of Regulation (EU) 2016/679 of the European Parliament and the Council of 27 April 2016 on the protection of natural persons regarding the processing of personal data and the free movement of such data. It also fulfilled Spanish Organic Law 3/2018 of 5 December on the Protection of Personal Data and the Guarantee of Digital Rights. This study was approved by the Parc de Salut Mar Ethics Committee in Barcelona (Research Protocol no. 2020/9119) and exempted from informed consent requirements owing to its register-based design. The research team committed itself to the strict use of data for the present study. In addition, a linkage protocol agreement between the Centre for Research in Occupational Health at Pompeu Fabra University, the National Social Security Institute, and the Catalonian Institute for Medical Evaluations guaranteed the maintenance of confidentiality in providing the identified datasets to the authors.
Results
Workers with SA due to cancer accumulated the fewest number of days of employment (3.2 years average for men and 3.7 years for women), whereas salaried workers without SA accumulated the highest number of days of employment (4.0 years average for men and 4.1 for women; Table 1). Salaried workers without SAs had a higher crude probability of continuing employment than those who had a SA due to cancer, especially among men (IRR 1.25, 95% CI 1.03‒1.52 vs. 1.10, 95% CI 0.97‒1.25 in women). A higher probability of continuing employment was also found among salaried workers who had a SA due to other diagnoses compared to those with SA due to cancer (men IRR 1.09, 95% CI 0.90‒1.32; women IRR 1.08, 95% CI 0.95‒1.23; Table 2). When IRR was adjusted individually, as well as by all potential confounders, the probability of employment remained higher in both men and women, but was only significant for men without SA.
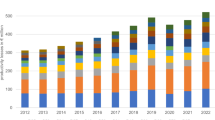
When we assessed trends of the annual accumulation of days of employment, men and women exhibited different EPTs. Among men, the three EPTs were: Low (28.1% of workers), Decreasing (11.6%), and High Stable (60.3%; Fig. 1, Table 3). The Low EPT was characterised by the lowest accumulation of days of employment during the follow-up period, which coincided with the lowest 5-year previous employment (87.2%), the lowest ratio among trajectories and the highest proportion of temporary workers (26.2%), and working in small-medium companies (72.7%). The Decreasing trajectory represented the smallest group of people (11.6%), who tended to have a decreased number of annual accumulated days until reaching zero, with the highest proportion of short part-time arrangements (16.7%), manual non-skilled occupations (12.8%), and lowest income (28.2%). In contrast, the High Stable trajectory depicted high accumulation of days annually, with the best employment conditions among the three trajectories. In women, we identified three EPTs: Low Fluctuating (6.4% of workers), Middle Fluctuating (18.8%), and High Stable (74.8%; Fig. 1, Table 3). Unlike the trajectories found in men, women exhibited patterns of accumulation of days with steeper U shapes in both Low Fluctuating and Middle Fluctuating EPTs, which started with a higher accumulation of days that decreased steadily and then increased yearly. The Low Fluctuating trajectory was the least common EPT among women (6.4%) and showed the lowest accumulation of days of employment during the follow-up period, coinciding with the lowest 5-year previous employment (83.1%), the lowest proportion of high income (16.1%), and non-manual skilled workers (7.1%). The Middle Fluctuating trajectory represented older women, with the highest proportion of short and marginal part-time arrangements (17.9%) and the highest proportion of low-income workers (65.6%). Similar to the observation in men, among women, the High Stable trajectory was the most frequent EPT (74.8% of women) with the best employment conditions.

Observed and expected trajectories considering number of days in employment per year in a sample of salaried men (top) and women (bottom) in Catalonia (2012–2018).
In Table 4, we examine the probability of belonging to each EPT for individuals who had a SA due to other diagnoses or no SA compared to those who had a SA due to cancer. Among men, we found that individuals without a SA had 2.78 (95% CI 1.77‒4.36) times the probability of belonging to the High Stable EPT than the Low EPT compared to men who had a SA due to cancer, and 2.52 (95% CI 1.31‒4.85) times the probability of belonging to the Decreasing EPT than the Low EPT (Table 4). When adjusted for all potential confounders, the probability of men without a SA belonging to the High Stable EPT rather than the Low EPT was found 3.21 (95% CI 1.87‒5.50) times higher than for men who had a SA due to cancer. In contrast to men, women without a SA had less probability of belonging to a Middle Fluctuating EPT than to a Low Fluctuating EPT than women who had a SA due to cancer (RRR 0.45, 95% CI 0.24‒0.97). Adjusting for potential confounders did not vary the direction of the association. Workers with SA due to other diagnoses followed the same trend as workers without SAs but had lower estimates and weaker evidence, especially when adjusted for potential confounders.
Discussion
This study shows that salaried workers with a SA due to cancer were less likely to accumulate employment days after ending the absence than those without a SA. This association exhibited a clearer positive pattern in men than in women. In women, we found weaker evidence with lower estimates than men. Similarly, both men and women with SA due to other diagnoses were more likely to be employed than workers with SA due to cancer. Furthermore, trajectories of employment showed that male salaried workers without a SA were 3-times more likely to be part of a stable employment trajectory than men with a SA due to cancer. These association patterns persisted after adjusting for company characteristics and employment-related factors.
Employability differences between cancer survivors and comparison groups were what we expected. The RTW population that has survived cancer have a lower probability of maintenance and accumulation of days of employment than the rest of the working population. These results did not substantially vary when adjusted for employment-related factors and company characteristics, which indicates that the lower employability is probably due to side effects provoked by cancer and its treatment (physical and psychological). Previous studies have shown that most cancer survivors RTW after treatment30, 31, but not whether they continued employed in the long-term after RTW. One prior review found that cancer survivors are more likely to be unemployed than the general working population23. However, the authors also found that the unemployment rate among cancer survivors was 34%, meaning that, even though it was higher than in the general working population, most of them continue in employment after a cancer diagnosis.
Men with SA due to other diagnoses present a gradient of future employability that is more favourable in terms of future employment accumulation than in workers with a SA due to cancer but worse compared to workers without SAs. Very few studies have addressed differences in work consequences among other diseases versus cancer. Nonetheless, there is a growing body of literature about chronic diseases as a whole, including cancer and RTW32, 33, which is much more action oriented (i.e., comparison of RTW interventions) than cancer research. Our results suggest differences between cancer and other chronic diseases. Furthermore, a qualitative study of employers’ perspectives of RTW among cancer survivors, found that this condition has a different status than others due to a lack of questioning the diagnosis, the immediate thought of the risk of death, and high psychological demands of the disease34. In this study, we considered all types of diagnoses in the comparison group regardless of the chronicity or duration of the SA to assess the overall effect of SA on future employment.
Studies carried out in northern European countries have found that younger age, higher levels of education, absence of surgery, fewer physical symptoms, shorter duration of sick leave, male gender, and Caucasian ethnicity are variables associated with RTW21, but their effect on employment in the long-term has not been studied. Regarding work-related factors, perceived employer accommodation has been found to be a strong predictor30.
EPTs revealed differences regarding employment trajectories after RTW. Most workers with a SA due to cancer, both men and women, go back to their jobs and stay employed, which is in agreement with previous literature30. The trajectory that represented the most stable labour life in our study (High Stable trajectory) included the highest proportion of young workers with a more stable working life in terms of the type of contract and employment before the follow-up period, which could explain the continuation in employment. Younger patients with cancer, even with side effects, may have remained in the labour market longer because they were too young to retire or to give up their professional career compared to older people. In addition, this stable labour life after cancer could represent less severe cancer, less aggressive treatments, and a better response in younger cancer patients. Other studies have found that younger age and locations associated with younger ages are factors associated with the likelihood of being employed and RTW30. We found higher levels of stable employment among women compared to men with SAs due to cancer, which is not what we expected. Previous studies have shown that female gender is a barrier to employment after cancer30. One explanation could be that some female cancer survivors may discontinue work because their partner is the main wage earner and provider of health insurance35, or can ensure the household’s financial stability alone36, so this results may vary by socioeconomic status. Existing literature shows discrepancies on the effect of survivors’ marital and relationship status, while some studies claim that marital status and gender don’t affect the probability of RTW37, 38, others find that marriage affects RTW positively in men. A recent study found that married women with breast cancer returned more to work than non-married ones, only among women over 50 years of age. In this same study, living with a partner showed decreasing trends of RTW and working time after RTW among women with equal household, highlighting the important role of financial support through higher freedom for a more flexible process of RTW39. Furthermore, there is also literature that has found higher odds of divorce when cancer diagnoses affected female comparing to men40, which could also be affecting women’s choice to go back and remain employed. Differences found with previous literature could be partly explained by age, as the women in our sample were younger, and as previously mentioned younger age is related to a greater employment likelihood. Previous research on the field has been carried out in countries where labour market dynamics and welfare state characteristics differ from the Spanish one, such as northern European countries. In fact, the gender gap in workforce participation is higher in Catalonia, as in the rest of Spain, than in these countries. In 2020, in Catalonia women employment rate was 63.3% and 70.9% in men41, contrasting Nordic countries such as Sweden with 78.3% in women and 83.2% in men42. This lower participation of women in employment could explain the differences with other studies since the ones that are on the labour market may have a higher engagement.
In men, we found a trajectory of reduced days of employment throughout the years until accumulating none (Decreasing trajectory). This trajectory represented the smallest proportion of the sample but comprised a group of manual workers. We think that they probably tried to return and maintain their jobs but cancer and its treatment affected their physical capacity, so they reduced their working time until they decided to exit the labour market. Previous studies have shown less probability of being employed in lower occupational categories due to high physical demands43, 44, and probably also due to more unstable employment trajectories. In women, this pattern exhibited a different evolution and depicted a more frequent future labour market trajectory characterised by women in a more precarious employment situation in terms of shortest working time and manual non-qualified occupations which could have made them reduce employment in the early years of cancer and increase it later, maybe because they needed the jobs in the first place.
We also identified a third trajectory comprising a group of men and women who accumulated the fewest number of days (Low and Low Fluctuating trajectories, respectively). In men, this sample stopped accumulating days of employment the third year, with a slight increase in the sixth year from the end of the SA due to cancer, probably because workers who were older preferred an exit from the labour market because working with side effects when they are just about to reach retirement age is not worthwhile. In this sense, a study carried out in the UK in men who survived prostate cancer found early retirement to be 9-times more likely in older men (aged 55–60 years) than men aged < 50 years45.
The main limitation of the present study is that the only information that we had regarding cancer is the SA diagnosis for the period 2012–2015. Therefore, we could not account for clinical features, such as type of treatment, stage of cancer, and the effects of prior health status regarding other comorbidities or cancer (first diagnosis, previous cancers, etc.) on the course of future employability. In addition, many individuals shifted between categories over the follow-up period and, in these cases, we assigned them to the category of explanatory and adjustment variables in which they spent most of their time during the follow-up. This could have led to a misclassification bias that underestimates the accumulation of SA days in other categories.
We also lacked information on workplace accommodations or support that have been proven to be determinant factors in employment sustainability and RTW30. Our sample size is small in relation to cancer cases certified by SAs, which could compromise the significance of our results. The self-employed were not included in the study, since by not being included in the general social security scheme, they are not entitled to sickness benefits.In addition, the methodology applied to employment trajectories involved group-based analyses that classified individuals according to similar characteristics. Consequently, some of the resulting groups had a very small number of observations, and these results should be interpreted with caution. However, some authors argue that a minimum of 5% should be enough to consider a pattern, and our results are above these recommendations46. The comparison groups resulted from matching show higher differences in men than in women regarding employment conditions and company characteristics. These differences shouldn’t be affecting our results since models are adjusted by them.
Our study also has numerous strengths. The study was conducted using a large administrative database, allowing us to select diagnosis subgroups and longitudinally study their trajectories with an extensive time window. Moreover, the size of the database allowed us to match our workers with SAs due to cancer to two comparison groups by age, sex, and follow-up time. This match allowed us to compare the working life of cancer survivors to the general working population with or without SAs, allowing us to account not only for the disease, but for the effect of SA. The diagnoses causing SAs were medically certified by primary doctors rather than self-reported, enhancing the validity of our results47.
To the best of our knowledge, employment continuation in a longitudinal sample of workers up to 6 years after the end of the SA has not previously been compared to the general salaried working population and workers who had a SA due to cancer for the same follow-up length and calendar days. More research is needed to understand the consequences of the disease and design interventions that address working difficulties caused by chronification of cancer in the long-term, not only at the beginning of the process of RTW.
Conclusions
Focusing on RTW after cancer treatment as a binary decision ignores the complexity of relationships between health and work in the development of working life at a later stage of survivorship. Our study shows that workers with SA due to cancer continue working after SA, though in a lower proportion than matched controls and with a less stable employment trajectory. Thus, this study constitutes a step towards further understanding the relationship between cancer and employment in the long-term and encourages future research in this area.
Data availability
The data that support the findings of this study are available but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Administrative data come from an annual sample of Spanish Social Security affiliates that are part of the Continuous Working Life Sample (CWLS) provided by the General Directorate of Social Security (DGOSS) and linked records of sickness absence episodes certified in Catalonia provided by Catalan Institute for Medical and Health Evaluations (ICAM). The record linkage was possible thanks to an agreement signed between DGOSS, ICAM, and CiSAL-UPF, maintaining data confidentiality.
References
Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. https://doi.org/10.3322/caac.21660 (2021).
Institution of Occupational Safety and Health (IOSH). Returning to work following cancer [Internet]. [cited 2021 Mar 12]. Available from: https://iosh.com/resources-and-research/our-resources/occupational-health-toolkit/returning-to-work-following-cancer/
Fitzmaurice, C. Supplemental content. JAMA Oncol [Internet]. 2018 [cited 2021 May 19];4:1553–68. Available from: https://jamanetwork.com/
Allemani, C. et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 391, 1023–1075 (2018).
Guzzinati, S. et al. Characteristics of people living in Italy after a cancer diagnosis in 2010 and projections to 2020 BMC Cancer. BMC Cancer 18, 1–13 (2018).
Gegechkori, N., Haines, L. & Lin, J. J. Long-term and latent side effects of specific cancer types. Med. Clin. North Am. 101, 1053–1073 (2017).
Bosetti, C. et al. National burden of cancer in Italy, 1990–2017: A systematic analysis for the global burden of disease study 2017. Sci. Rep. 10, 1–10. https://doi.org/10.1038/s41598-020-79176-3 (2020).
Miller, K. D. et al. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 69, 363–385 (2019).
International Agency for Research on Cancer (IARC). Cancer Today [Internet]. [cited 2021 Apr 5]. Available from: https://gco.iarc.fr/today/online-analysis-table?v=2020&mode=cancer&mode_population=continents&population=900&populations=900&key=asr&sex=0&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=3&ages_group%5B%5D=13&group_cancer=1&i
White, M. C. et al. Age and cancer risk: A potentially modifiable relationship. Am. J. Prev. Med. 46, S7-15 (2014).
OECD. Pensions at a Glance. OECD and G20 Indicators 2017 (OECD Publishing, 2017).
Sesto, M. E., Faatin, M., Wang, S., Tevaarwerk, A. J. & Wiegmann, D. A. Employment and retirement status of older cancer survivors compared to non-cancer siblings. Work 46, 445–453 (2013).
Ekenga, C. C., Pérez, M., Margenthaler, J. A. & Jeffe, D. B. Early-stage breast cancer and employment participation after 2 years of follow-up: A comparison with age-matched controls. Cancer 124, 2026–2035. https://doi.org/10.1002/cncr.31270 (2018).
Paltrinieri, S. et al. Return to work in European cancer survivors: A systematic review. Support Care Cancer 26, 2983–2994 (2018).
Den Bakker, C. M. et al. Prognostic factors for return to work and work disability among colorectal cancer survivors. A systematic review. PLoS ONE 13, 1–18 (2018).
Sun, Y., Shigaki, C. L. & Armer, J. M. Return to work among breast cancer survivors: A literature review Support Care Cancer [Internet]. Supportive Care Cancer 25, 709–718. https://doi.org/10.1007/s00520-016-3446-1 (2017).
European Agency for Safety and Health at Work (EU-OSHA). Rehabilitation and return to work after cancer [Internet]. 2017. Available from: www.designcouncil.org.uk
Sharipova, A., Baert, S. Labour market outcomes for cancer survivors: A review of the reviews. Bonn; 2019. Report No.: 12856.
Van Maarschalkerweerd, P. E. A. et al. Changes in employment status, barriers to, and facilitators of (return to) work in breast cancer survivors 5–10 years after diagnosis. Disabil. Rehabil. 42, 3052–3058. https://doi.org/10.1080/09638288.2019.1583779 (2020).
Saunders, S. L. & Nedelec, B. What work means to people with work disability: A scoping review. J. Occup. Rehabil. 24, 100–110 (2013).
Mehnert, A., De Boer, A. & Feuerstein, M. Employment challenges for cancer survivors. Cancer 119, 2151–2159 (2013).
Gem De Boer, A. et al. Long-term work retention after treatment for cancer: A systematic review and meta-analysis. J. Cancer Surviv. 14, 135–150. https://doi.org/10.1007/s11764-020-00862-2 (2020).
De Boer, A. G. E. M., Taskila, T., Ojajärvi, A., Van Dijk, F. J. H. & Verbeek, J. H. A. M. Cancer survivors and unemployment a meta-analysis and meta-regression. JAMA 301, 753–762 (2009).
Heinesen, E., Imai, S. & Maruyama, S. Employment, job skills and occupational mobility of cancer survivors. J. Health Econ. 58, 151–175. https://doi.org/10.1016/j.jhealeco.2018.01.006 (2018).
Gómez, M.A.L., Durán, X., Zaballa, E., Sanchez-Niubo, A., Delclos, G.L., Benavides, F.G. Cohort profile: The Spanish WORKing life social Security (WORKss) cohort study. BMJ Open. 2016;6.
Durán, A., La Muestra, C., de Vidas, L., de La Seguridad, S. Rev del Minist Trab y Asuntos Soc [Internet]. 2007 [cited 2018 Oct 24];10. Available from: http://www.mitramiss.gob.es/es/publica/pub_electronicas/destacadas/revista/numeros/ExtraSS07/Est09.pdf
Muthén, B. O. & Muthén, L. K. Integrating person-centered and variable-centered analyses: Growth mixture modeling with latent trajectory classes. Alcohol. Clin. Exp. Res. 24, 882–891 (2000).
Skrondal, A., Rabe-Hesketh, S. Generalized Latent Variable Modeling. Multilevel, Longitudinal, and Structural Equation Models. N. Keiding, B. Morgan, T. Speed P van der H, editor. New York. Chapman & Hall/CRC; 2004.
Van de Schoot, R., Sijbrandij, M., Winter, S. D., Depaoli, S. & Vermunt, J. K. The GRoLTS-checklist: Guidelines for reporting on latent trajectory studies. Struct. Equ. Model 24, 451–467. https://doi.org/10.1080/10705511.2016.1247646 (2017).
Mehnert, A. Employment and work-related issues in cancer survivors. Crit. Rev. Oncol. Hematol. 77, 109–130 (2011).
Spelten, E. R., Sprangers, M. A. G. & Verbeek, J. H. A. M. Factors reported to influence the return to work of cancer survivors: A literature review. Psychooncology. 11, 124–131 (2002).
Nazarov, S. et al. Chronic diseases and employment: Which interventions support the maintenance of work and return to work among workers with chronic illnesses? a systematic review. Int. J. Environ. Res. Public Health. 16, 1–14 (2019).
Snippen NC, De Vries HJ, Van Der Burg-Vermeulen SJ, Hagedoorn M, Brouwer S. Influence of significant others on work participation of individuals with chronic diseases: A systematic review. BMJ Open. 2019;9.
de Rijk, A. et al. The challenge of return to work in workers with cancer: Employer priorities despite variation in social policies related to work and health. J. Cancer Surviv. 14, 188–199 (2020).
Chan, F. et al. State vocational services and employment in cancer survivors. J. Cancer Surviv. 2, 169–178 (2008).
Salonen, P., Rantanen, A., Kellokumpu-Lehtinen, P. L., Huhtala, H. & Kaunonen, M. The quality of life and social support in significant others of patients with breast cancer—A longitudinal study. Eur. J. Cancer Care (Engl). 23, 274–283 (2014).
Arndt, V. et al. Return to work after cancer A multi-regional population-based study from Germany. Acta Oncol. 58, 811–818. https://doi.org/10.1080/0284186X.2018.1557341 (2019).
Van Muijen, P. et al. Predictors of return to work and employment in cancer survivors: A systematic review. Eur. J. Cancer Care (Engl). 22, 144–160 (2013).
Caumette, E., Vaz-luis, I., Pinto, S., Havas, J., Bovagnet, T., de Azua, G.R. The challenge of return to work after breast cancer : The role of family situation. CANTO Cohort. Curr Oncol. 2021;3866–75.
Glantz, M. J. et al. Gender disparity in the rate of partner abandonment in patients with serious medical illness. Cancer 115, 5237–5242 (2009).
Idescat. Statistical Yearbook of Catalonia. Employment rate. By sex. Provinces [Internet]. [cited 2021 Nov 1]. Available from: https://www.idescat.cat/pub/?id=aec&n=303&lang=en
Eurostat. Employment - annual statistics - Statistics Explained [Internet]. [cited 2021 Nov 1]. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Employment_-_annual_statistics
Taskila-Åbrandt, T. et al. The impact of education and occupation on the employment status of cancer survivors. Eur. J. Cancer 40, 2488–2493 (2004).
Bradley, C. J. & Bednarek, H. L. Employment patterns of long-term cancer survivors. Psychooncology 11, 188–198 (2002).
Bennett, D. et al. Factors influencing job loss and early retirement in working men with prostate cancer—findings from the population-based Life After Prostate Cancer Diagnosis (LAPCD) study. J. Cancer Surviv. 12, 669–678 (2018).
Farrants, K., Friberg, E., Sjölund, S. & Alexanderson, K. Trajectories of future sickness absence and disability pension days among individuals with a new sickness absence spell due to osteoarthritis diagnosis ≥ 21 days: A prospective cohort study with 13-month follow-up. BMJ Open 9, 1–11 (2019).
Castejón, J. et al. Quality of medical diagnosis in sick leave certificates for non-occupational diseases and injuries. Aten. Primaria 37, 142–147 (2006).
Acknowledgements
This work would not have been possible without the Spanish National Social Security Institute and the Catalonian Institute for Medical Evaluations.
Funding
The study was financed by the State Plan for Investigation, Development, and Innovation, 2021–2023, by the Health Institute Carlos III- FIS_FEDER—Subdirection General of Evaluation and Promotion of Investigation (Grants FIS PI20/00101 and FIS PI17/00220). The study was also supported by the Spanish Society of Epidemiology and the CIBER of Epidemiology and Public Health.
Author information
Authors and Affiliations
Contributions
All listed authors fulfil authorship criteria. A.A.G. and F.G.B. participated in the study conception and design. A.A.G. and L.S. performed the main data management and analysis with support from J.C.H.R., A.A.G., F.G.B., L.S., and J.C.H.R. interpreted the data. A.A.G. drafted the first version of the manuscript with close help from F.G.B. L.S. and J.C.H.R. made subsequent revisions to the manuscript and all authors revised the final version, agreed with the text and findings, and approved this final version. L.S. and J.C.H.R. contributed equally to the manuscript. The corresponding author certifies that all listed authors meet authorship criteria. A.A.G. is the guarantor.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ayala-Garcia, A., Serra, L., Hernando-Rodriguez, J.C. et al. Returning to work after a sickness absence due to cancer: a cohort study of salaried workers in Catalonia (Spain). Sci Rep 11, 23953 (2021). https://doi.org/10.1038/s41598-021-03368-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-03368-8
This article is cited by
-
Return to work after cancer–the impact of working conditions: A Norwegian Register-based Study
Journal of Cancer Survivorship (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
