
Abstract
Many women suffer from urinary tract infections (UTIs). In addition to pain and increased urgency to urinate, malodour is a significant issue for these patients. The specific factors causing this malodour are unclear, and there are no targeted treatment options to counteract it effectively. We used a metabolomics approach to compare the chemical composition of metabolites in the urine of women with E. coli UTIs (n = 15) and those who are healthy (n = 10). The biogenic amines trimethylamine and putrescine, which cause malodour in other urogenital conditions, were significantly increased in UTI patients. Conversely, the precursor of trimethylamine, trimethylamine N-oxide, was lower. To further confirm the source of the malodorous compounds, in vitro experiments were conducted by incubating strains of uropathogenic E. coli in sterilized urine from healthy women. All tested strains accumulated trimethylamine and putrescine. Notably, cadaverine was also produced by E. coli strains in vitro; however, it was not significantly different between both groups. We confirmed that the malodorous amines TMA and putrescine are found in higher concentrations in the urine of patients with an E.coli-caused UTI.
Similar content being viewed by others


Introduction
Urinary tract infections (UTIs) are a highly prevalent global health problem, with over 50% of women expected to experience at least one in their lifetime1,2. Lower UTIs are more common than those infecting the kidney, and Escherichia coli (UPEC) strains are responsible for approximately 80% of the cases. These uropathogens originate from the gastrointestinal tract3 and enter the bladder via the fecal-vaginal-periurethral route4. These infections are present with dysuria, increased frequency of urination, abdominal pain, and malodour5. However, besides ammonia, which is a known cause for foul-smelling urine6,7, other sources of malodour during infection and the source of their production require further characterization. None of the currently available treatment regimens target malodour.
A better understanding of the chemical origins of malodour during this condition would enable the creation of more targeted and efficient therapies. Therefore, we aim to identify if known causes of urogenital malodour are also present during UTIs.
Biogenic amines are basic nitrogenous compounds with well-established organoleptic characteristics (Table 1) associated with malodour8. Most of them are biosynthesized from amino acids, as shown in Fig. 1. Trimethylamine (TMA), tyramine, cadaverine, and putrescine are of interest since they are known to cause urogenital malodour in conditions such as bacterial vaginosis (BV)8,9. Until now, these compounds have not been associated with urinary malodour, except for trimethylamine (TMA), which has a characteristic fishy odour and has previously been postulated by various groups as a candidate biomarker for E. coli-associated UTI10,11,12.

Biosynthetic origin of biogenic amines. Each line represents a single reaction catalyzed by the described enzyme. *Other possible sources for TMA production are described in the text, while the one depicted here is the most relevant in the context of the bladder.
Although the majority of urinary TMA derives from the reduction of trimethylamine N-oxide (TMAO) (Fig. 1), other substrates can also yield TMA8. Notably, the reverse reaction, where TMA is oxidized to form TMAO is also possible13. Other relevant TMA precursors are the products of dietary phosphatidylcholine, choline and betaine14, as well as dietary sources such as L-carnitine and ergothioneine15. However, these compounds are majorly metabolized into TMA by several taxa of the gut microbiota16,17 in the small intestine, transported through the bloodstream to the liver where they are oxidized into TMAO18 which subsequently travels to the kidneys to be excreted through the bladder19, where it can be converted back into TMA by indigenous or pathogenic bacteria.
Tyramine is synthesized via decarboxylation of tyrosine, and it is produced by uropathogens such as Enterococcus faecalis20, but it has not been reported in UPEC strains. Cadaverine, which is primarily a bacterial metabolite21, is the product of the decarboxylation of lysine, and it is thought to be synthesized by E.coli in anaerobic and low pH conditions22. Putrescine, produced both by human and bacterial cells21, is a product of amino acid catabolism23, either from ornithine or agmatine, the latter being a product of the decarboxylation of arginine (Fig. 1).
Evidence suggests these compounds play an essential role in pathogenesis. For instance, entero-invasive strains of E. coli are unable to produce cadaverine, a compound that interferes with the invasive process24. While putrescine enhances survival within oxidative environments25 and augments cell growth and proliferation26; consistent with these observations, Satink et al.27 showed that putrescine levels increased in patients with UTI before antibiotic therapy, then decreased as a result of the treatment, presumably because of the eradication of the producers. However, no differences were detected for cadaverine in either case, likely because urinary cadaverine is primarily derived from the gastrointestinal microbiota and dietary sources21.
Additionally, a vaginal strain, E. coli 83972, has the genetic machinery to produce putrescine, cadaverine, and TMA. Of note, this strain encodes two enzymes for TMA production8, a homolog of TMAO reductase, and choline trimethylamine-lyase, which is the enzyme in charge of transforming choline to TMA, suggesting that, to some extent, TMA could derive from either of these substrates in the urogenital tract. Since the vaginal and bladder microbiomes are interconnected28, it cannot be ruled out that this strain can also be present in the bladder. Contrary to common belief, the bladder has its own microbiome29, which could have a role in this TMA conversion similarly as it happens in the gut, where TMAO is reduced primarily by Enterobacteriaceae30, a family of bacteria which is present in larger proportions during a UTI.
It has been reported that cadaverine production increases when UPEC strains are grown under nitrosative stress, potentially conditioning them for enhanced colonization of the host31,32. This is of relevance since, during a UTI, there is a significant formation of nitric oxide and reactive nitrogen intermediates33,34. Nevertheless, the specific role of cadaverine in resistance to nitrosative stress is unclear. Potentially, during an infection, UPEC strains produce a significant amount of cadaverine, which would, in turn, cause malodorous urine. Yet, previous work has shown no change in cadaverine levels during UTI27.
The present study aimed to take a metabolomics approach to identify molecules responsible for urinary malodour and their biosynthetic origins.
Results
Clinical sample characterization
In total 31 human urine samples were obtained, comprising both UTI-negative (n = 10) and UTI-positive (n = 21). Of the latter, E.coli was the dominant pathogen in 15 individuals, while Staphylococcus aureus, Klebsiella pneumoniae, Pseudomonas aeruginosa were dominant in 3, 2 and 1 individuals, respectively. There were no significant associations between UTI and urinary pH or creatinine concentration (Supplementary Material, Figs. S1, 2). Only samples positive for E. coli will be discussed in the subsequent results. Analyses of samples infected by other pathogens can be found in the Supplementary section.
Metabolomics of UTI-positive clinical samples
The metabolomic profiles of the human urine samples were analyzed by high-resolution LC-MS. Biogenic amines and other small polar compounds are not well suited for chromatographic separation using a C18 reverse-phase column. Therefore, a hydrophilic interaction chromatography (HILIC) approach was used (Fig. 2).

Chromatogram of a UTI positive sample. Separation carried out using HILIC chromatography, ideally suited for polar compounds (e.g. biogenic amines and amino acids).
The features extracted by XCMS were analyzed using a principal components’ analysis (PCA) model. No distinct grouping of samples could be observed in the 1st dimension. However, separation of both UTI and healthy groups was observed in the 2nd and 4th (27.2% total explained variance). The major chemicals responsible for the separation of these groups were TMA and putrescine (Fig. 3).

TMA and one of its main precursors, TMAO, are driving the separation between UTI-positive and negative samples in multivariate analysis. (A) Principal components analysis (PCA) score plot of Healthy (black, n = 10) vs UTI-positive samples (red, n = 15), where each point represents a single sample from a single woman. The location of each point displays differences in the metabolome, with samples closer to each other being similar. Ellipses represent the 95% confidence intervals; (B) PCA loadings, which show the weights of each metabolite in the principal component cartesian plane. Each point represents a single metabolite. Biogenic amines, as well as their precursors, are colour coded.
Biogenic amines, as well as some standard amino acids, were also quantified in the clinical urine samples. Following normalization with urinary creatinine concentrations, both TMA and putrescine were significantly elevated between groups, whereas cadaverine and tyramine were not (Fig. 4).

Comparison of the concentration of biogenic amines in Healthy vs UTI positive patients. Control consists of the urine of healthy patients (n = 10). TMA and putrescine levels are higher in patients with UPEC caused UTI (n = 15). Only the samples positive for UPEC were included in this analysis. Horizontal lines indicate the median. Significant differences were determined on log-transformed values using a two-sample t-test (*p < 0.05).
The concentrations of the precursors of these amines are shown in Fig. 5; only TMAO—which is one of the possible precursors of TMA—was significantly lower in UTI patients. On the amino acid analysis, aspartic acid and glutamic acid were significantly increased in the UTI positive group, whereas serine and asparagine were decreased (Fig. 6).

Comparison of the concentration of the precursors of biogenic amines in Healthy vs UTI positive patients. Control consists of the urine of healthy patients (n = 10). TMAO, one of the precursors of TMA, was significantly lower in the positive samples. Only the samples positive for UPEC were included in this analysis (n = 15). Horizontal lines indicate the median. Significant differences were determined on log-transformed values using a two-sample t-test (*p < 0.05).

Comparison of the concentration of amino acids in Healthy vs UTI positive patients. Control consists of the urine of healthy patients (n = 10). Glutamic acid and Aspartic acid are significantly elevated in UTI patients, while Serine and Asparagine are significantly lower. Only the samples positive for UPEC were included in this analysis (n = 15). Horizontal lines indicate the median. Significant differences were determined on log-transformed values using a two-sample t-test (*p < 0.05, **p < 0.005).
in vitro analysis of UPEC strains in sterile urine
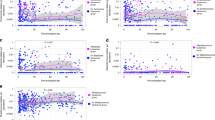
To better understand the metabolic dynamics involved in the production of biogenic amines by UPEC, the presence of metabolites from four different clinical UPEC strains grown in sterile female urine was assessed over 24 hours. Many of the biogenic amines identified in clinical samples were also found in vitro and showed significant changes within 3 hours (Figs. 7 and 8).

Time course analysis on the formation and uptake of biogenic amines and their precursors by different UPEC strains. Precursors on the left column and biogenic amines on the right. TMAO was analyzed semi-quantitatively based on the log of its peak area. Metabolite levels standardized using the control as a baseline, consisting of sterile urine with 5 µL of LB media to account for potential matrix effect. A linear mixed-effect model with repeated measures was used to calculate statistical significance. Tukey post-hoc test was used to determine individual differences (Tables S1 and S2). The horizontal significance line and p-value correspond to the main effect of Time over the concentration of each metabolite after 24 h. Vertical significance corresponds to the comparison of each strain vs the control. Data are presented as means of 3 independent experiments ± SEM. (*p < 0.05, *****p < 0.0001).

Time-course analysis of the formation and uptake of amino acids by different UPEC strains. Metabolite levels standardized using the control as a baseline, consisting of sterile urine with 5 µL of LB media to account for potential matrix effect. A linear mixed-effect model with repeated measures was used to calculate statistical significance. Tukey post-hoc test was used to determine individual differences (Tables S1 and S2). The horizontal significance line and p-value correspond to the main effect of Time over the concentration of each metabolite. Vertical significance corresponds to the comparison of each strain vs the control after 24 h. Data are presented as means of 3 independent experiments ± SEM. (**p < 0.01, *****p < 0.0001).
Similar trends in terms of metabolite changes were observed between all five tested UPEC strains (Tables S1 and S2), showing an accumulation of cadaverine and TMA, whereas a maximal amount of putrescine was produced after 3 h and diminished thereafter. Except for cystine, where an accumulation over time was observed, most amino acids were reduced in concentration by the UPEC strains during the incubation. Alanine showed significant increments at hours 3 and 6 by strains IA2 and 536 respectively and was degraded thereafter; after 24 h only strain J96 was significantly different from the control. Histidine and tyramine did not show a major change in amounts relative to their starting concentrations. The amino acids: aspartic acid, methionine, isoleucine, valine, leucine, glutamine, glycine, and threonine were not included in this analysis as they were below the detection limit of the method.
Discussion
Here, we present a comprehensive profile of the production of odorous compounds during UPEC-UTI. Only the biogenic amines TMA and putrescine were present at high concentrations in patients with UTIs compared to controls. This contrasts with results in patients with BV, where cadaverine and tyramine are also elevated8,9.
Using an in vitro model, cadaverine was found to be significantly increased, perhaps due to nitrosative stress33,35 which is higher in a steady-state culture than in the human bladder, allowing for its accumulation. The in vitro model provides a static system that allows for better appreciation of the rates of consumption and production of specific metabolites, while in vivo, there is a continuous flow of urine into the bladder from the kidneys that replenishes substrates and makes it challenging to identify the changes in metabolite concentration.
Notably, differences were also found in cadaverine levels between strains. Following reports that cadaverine production can interfere with the invasive process of UPEC, we hypothesize that its production is reduced during colonization of the bladder as a means to enhance infectivity24. Thus, the environment of the bladder may influence the expression of the genes that regulate cadaverine production and perhaps explain why previous reports have found contrasting results.
Putrescine levels were increased in vivo and in vitro in agreement with findings in patients with an overactive bladder35. This is associated with an increase in ornithine decarboxylase, which has been shown to block the calcium potassium channel. Since putrescine levels can modulate intracellular calcium levels in urothelial cells, it suggests a correlation between UTIs and overactive bladder36 and a role for putrescine in urinary urgency. This was further supported by the finding that ornithine, a major precursor of putrescine, showed a marked decrease in the in vitro samples. More studies are warranted to investigate this result.
TMA was one of the metabolites that exhibited a highly significant increase in the present study. Our method detected that TMAO, one of the precursors of TMA, was significantly lower in UTI-positive patients, which suggests that it was one of the main sources of production. However, it cannot be ruled out that, at least part of it, was derived from other dietary sources (i.e. choline, betaine, L-carnitine, ergothioneine). Furthermore, we acknowledge that some of the TMAO observed could be a direct consequence of the increase in TMA. Regardless of this fact, the difference in the concentration of TMAO between both groups is still significant.
Future studies that target other potential precursors should aim to elucidate the proportions of the sources from were TMA is being produced during the course of a UTI. It would be worth investigating whether the increase of TMA during a UTI could affect other symptoms and signs. For instance, acetylcholine present in urine can be converted into choline via the enzyme AChE, allowing TMA to be produced from choline through choline TMA lyase activity. The cholinergic system has an important role in voiding the bladder36, with acetylcholine from parasympathetic nerves and non-neuronal cells within the urothelium, affecting, directly and indirectly, muscle contraction36.
Except for cystine, most of the amino acids analyzed in our time-course were degraded over time. Previous reports have shown that when UPEC strains are grown in urine, several genes responsible for amino acid catabolism are upregulated37. It is thought that this is important in the ability of UPEC to colonize the bladder38. Notably, serine was significantly reduced both in vivo and in vitro, suggesting it is being used as a substrate by UPEC. This is consistent with previous reports showing upregulation of genes responsible for amino acid catabolism, specifically D-serine deaminase (dsdA) when UPEC were grown in human urine37,39. Both D- and L-serine are gluconeogenic amino acids that can be degraded to produce oxaloacetate or pyruvate, which can enter the TCA cycle, therefore they can be used as a carbon source38. Furthermore, the catabolism of D-serine in the urinary tract has been identified as a key signalling mechanism for virulence gene expression40,41,42.
A significant decrease in asparagine levels was also found. Asparagine metabolism by E. coli has not been extensively studied, but it is hypothesized that the organism can utilize this amino acid by conversion to aspartic acid using an asparaginase enzyme43. This agrees with our results, where asparagine was significantly reduced while aspartic acid increased.
Overall, this study revealed that the malodorous amine putrescine is higher in patients with a UTI, and confirmed previous findings10,11,12 that correlate an increase in the concentration of TMA with this condition, a compound that is well known for its fishy smell. Although malodour was not measured directly, the clear increase in the concentrations of malodorous compounds suggests that they play a significant role in the urinary malodour that patients with UTIs experience. However, we recognize that future odour metrology studies are warranted, where a trained panel could correlate specific increases of these compounds to the changes in the organoleptic properties of the urine of infected patients18.
Our findings open the door to the development of more targeted approaches to reduce urinary malodour, a problem that is particularly prevalent in urinary incontinence patients and takes days to resolve when antibiotics are administered. For instance, specific lifestyle modifications could be recommended to the patients, such as dietary changes, consumption of prebiotics or prebiotics in order to modulate the production of these compounds and their precursors; as well as the addition of specific agents that could degrade or neutralize them in hygiene products (such as diapers and pads). Ultimately, the knowledge of the specific compounds to counteract allows for specific procedures to reduce them effectively, without having to wait for antibiotics to provide some relief.
Materials and Methods
Urine samples collection and processing
Thirty-one urine samples from women with UTI were provided by Dr. Ana Cabrera from the Division of Microbiology at the Pathology and Laboratory Medicine Centre of London Health Sciences Centre (London, Ontario, Canada). All urine samples were obtained in accordance to article 2.4 of the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans – TCPS 2 (2018). All samples were provided anonymously for secondary use with ethics board approval not required. Samples were discarded after their primary use by Dr. Cabrera for standard clinical testing. These samples included 10 UTI-negative controls and 21 samples from patients clinically diagnosed with a UTI, from which 15 were positive for E. coli, 3 for Staphylococcus aureus, 2 for Klebsiella pneumoniae, and 1 for Pseudomonas aeruginosa. Diagnosis criteria were based on the presence of signs and symptoms and significant bacteriuria (bacterial growth ≥105 colony-forming units (CFU)/mL). To further characterize the samples, pH was measured using test strips and creatinine was quantified. Figure 9 shows a linear correlation between both methods used to determine hydration levels.

Validation of the methods used to measure hydration levels. Horizontal lines indicate the median. There is a positive correlation between the two methods (R2 = 0.7103).
For in vitro testing purposes, urine samples were collected for secondary use from three healthy pre-menopausal women and pooled for use in the experiment. All urine samples were obtained in accordance to article 2.4 of the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans – TCPS 2 (2018). All samples were provided anonymously for secondary use with ethics board approval not required. These were centrifuged at 4500 g for 10 min to remove any solid particles, followed by filter-sterilization using 0.22 µm syringe filters. To ensure asepsis, 10 µL of urine were plated on LB plates. To determine hydration levels, creatinine concentration was quantified using the Creatinine (urinary) Colorimetric Assay Kit (Cayman Chemical Co., Ann Arbor, MI, USA) as described by the manufacturer. Hydration levels were determined according to a validated 8-scale urine colour chart44,45.
LC-MS analysis of urine samples
Samples were prepared based on the methodology proposed by Spagou et al.46. Briefly, aliquots of 250 µL were taken of each urine culture and diluted with pure methanol (1:3 for clinical samples and 1:6 for the in vitro analysis), vortexed, incubated on ice for 30 min, and centrifuged at x16000g for 10 min. Supernatants were then filtered using 0.22 µm PTFE syringe filters and added to vials for analysis. Samples were analyzed using a Q-Exactive Quadrupole Orbitrap MS, coupled to an Agilent 1290 HPLC system with an Agilent HILIC-Z (2.1 × 100 mm, 2.7 µm; Agilent) column. Compounds were resolved with mobile phases of 20 mM ammonium formate in water (A) and 20 mM ammonium formate in 90% acetonitrile (B) operating with the following gradient: 0 min, 100% B; 0.5 min, 100% B; 5.3 min, 80% B; 9.5 min, 30% B; 13.5 min, 30% B, 14.5 min 100% B and 16.5 min, 100% B. The following conditions were used for heated electrospray ionization (HESI): HESI(+) capillary voltage, capillary voltage, 3.5 kV; capillary temperature, 250 °C; sheath gas, 30.00 units; auxiliary gas, 8.00 units; probe heater temperature, 450 °C; S-Lens RF level, 60.00. The LC-MS was operated using a top 3 data-dependent acquisition (DDA) experiment that involved a full MS scan in the mass range of m/z 58–870 at 35,000 resolution, followed by MS/MS scans at 17,500 resolution, isolation window of m/z 1.2 and collision energy of 28. The biogenic amines and amino acids quantified in the full MS scans were: cadaverine, putrescine, tyramine, spermine, spermidine, histamine, TMA, phenylalanine, leucine, tryptophan, isoleucine, methionine, valine, tyrosine, proline, alanine, threonine, glutamine, serine, asparagine, glutamic acid, aspartic acid, histidine, arginine, cystine, lysine, ornithine, glycine, and TMAO. The standards used for calibration curves were acquired from Sigma Aldrich (St. Louis MO). TMAO was analyzed semi-quantitatively using the log transformation of its peak area (Figure S7).
UPEC cultures
A time-course analysis was performed using clinical UPEC strains GR-12, IA2, 536 and J96, to assess whether there is a significant difference in polyamine production amongst strains over time. All the strains used were clinical isolates from patients with acute UTI47,48,49,50. Individual colonies of each strain were grown aerobically overnight in 5 mL of Lysogeny broth (LB) media, 5 µL of these cultures were then grown in sterile urine and incubated aerobically for 24 h at 37 °C. Control samples consisted of 5 mL of sterile urine with 5 µL of LB media; aliquots were taken at hours 0, 3, 6, 9, 12, and 24, and analyzed through HILIC-MS, post-acquisition recalibration was performed to the results, and the concentrations of the metabolites of interest was quantified. Growth was monitored measuring optic density at a wavelength of 600 nm to ensure uniform growth of the strains. Three biological replicates were used for each strain tested.
LC-MS Data analysis
Proteowizard51 was used to convert the Thermo.raw files to.mzml format, with peak peaking filter applied. Features were detected using the XCMS package52,53,54 with the centWave53 method (ppm. Tolerance 1.0). The signal to noise threshold was set to 5, the noise was set to 3 × 106 and pre-filter was set to six scans with a minimum 5,000 intensity. Retention time correction was conducted using the obiwarp55 method. Grouping of features was set to those present in at least 25% of all samples (retention time deviation 10 s; m/z width, 0.015). The ‘fillPeaks’ function with default settings. Remaining zeros values were imputed with two thirds the minimum value on a per mass basis. Large mass salt clusters and ionization artifacts were filtered using the McMillan correction56. For the targeted analysis, Xcalibur (Thermo Scientific, Waltham, MA) was used to quantify the metabolites of interest. Compounds were identified by accurate mass, comparison of retention times to authentic standards or by accurate mass and comparison of fragmentation patterns to MS/MS databases57.
The data generated were submitted to the EMBL-EBI MetaboLights database with the identifier MTBLS1294 (https://www.ebi.ac.uk/metabolights/MTBLS1294)58.
Statistical analysis
RStudio version 1.2.133556 was used for all statistical analyses. Plots were generated with the ggplot2 package59. For the untargeted metabolomics analysis, the ‘FactoMineR’60 package with Pareto scaling was used to perform a PCA. Targeted metabolomics comparisons in the clinical samples were analyzed using a two-sample two-tailed t-test analysis and defined a p-value of <0.05 as statistically significant. Time-course trials were analyzed using a linear mixed-effect model (Tukey post-hoc correction) using the ‘emmeans’ package61. Log transformation was used to correct the distribution and heteroscedasticity of the data62.
Data availability
The data generated were submitted to the EMBL-EBI MetaboLights database with the identifier MTBLS1294 (https://www.ebi.ac.uk/metabolights/MTBLS1294).
References
Tandogdu, Z. & Wagenlehner, F. M. E. Global epidemiology of urinary tract infections. Curr. Opin. Infect. Dis. 29, 73–79 (2016).
Foxman, B. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Dis. Mon. 49, 53–70 (2003).
Salvatore, S. et al. Urinary tract infections in women. Eur. J. Obstet. Gynecol. Reprod. Biol. 156, 131–136 (2011).
Moreno, E. et al. Relationship between Escherichia coli strains causing acute cystitis in women and the fecal E. coli population of the host. J. Clin. Microbiol. 46, 2529–2534 (2008).
Sj, M., Paur, R. & Lindseth, G. Urinary tract infections: does the smell really tell? J. Gerontol. Nurs. 30, 4–9 (2004).
Forsgren-Brusk, U., Yhlen, B., Blomqvist, M. & Larsson, P. Method for bacterial growth and ammonia production and effect of inhibitory substances in disposable absorbent hygiene products. J. Wound, Ostomy Cont. Nurs. 44, 78–83 (2017).
Norberg, A., Sandström, S., Norberg, B., Eriksson, S. & Sandman, P.-O. The urine smell around patients with urinary incontinence. Gerontology 30, 261–266 (1984).
Nelson, T. M. et al. Vaginal biogenic amines: biomarkers of bacterial vaginosis or precursors to vaginal dysbiosis? Front. Physiol. 6, 1–15 (2015).
McMillan, A. et al. A multi-platform metabolomics approach identifies highly specific biomarkers of bacterial diversity in the vagina of pregnant and non-pregnant women. Sci. Rep. 5, 1–14 (2015).
Lam, C. W. et al. NMR-based metabolomic urinalysis: A rapid screening test for urinary tract infection. Clin. Chim. Acta 436, 217–223 (2014).
Lam, C. W., Law, C. Y., Sze, K. H. & To, K. K. W. Quantitative metabolomics of urine for rapid etiological diagnosis of urinary tract infection: evaluation of a microbial-mammalian co-metabolite as a diagnostic biomarker. Clin. Chim. Acta 438, 24–28 (2015).
Lussu, M. et al. 1H NMR spectroscopy-based metabolomics analysis for the diagnosis of symptomatic E. coli-associated urinary tract infection (UTI). BMC Microbiol. 17, 201 (2017).
Ufnal, M., Zadlo, A. & Ostaszewski, R. TMAO: a small molecule of great expectations. Nutrition 31, 1317–1323 (2015).
Wang, Z. et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 472, 57–63 (2011).
Janeiro, M., Ramírez, M., Milagro, F., Martínez, J. & Solas, M. Implication of trimethylamine N-oxide (TMAO) in disease: potential biomarker or new therapeutic target. Nutrients 10, 1398 (2018).
Fennema, D., Phillips, I. R. & Shephard, E. A. Trimethylamine and trimethylamine N-oxide, a flavin-containing monooxygenase 3 (FMO3)-mediated host-microbiome metabolic axis implicated in health and disease. Drug Metab. Dispos. 44, 1839–1850 (2016).
Manor, O. et al. A multi-omic association study of trimethylamine N-oxide. Cell Rep. 24, 935–946 (2018).
Romano, K. A., Vivas, E. I., Amador-Noguez, D. & Rey, F. E. Intestinal microbiota composition modulates choline bioavailability from diet and accumulation of the proatherogenic metabolite trimethylamine-N-oxide. MBio 6 (2015).
Fogelman, A. M. TMAO is both a biomarker and a renal toxin. Circ. Res. 116, 396–397 (2015).
Whiteside, S. A. Contribution of Enterococcus faecalis to urinary tract infection. (The University of Western Ontario, PhD thesis, 2018).
Tofalo, R., Cocchi, S. & Suzzi, G. Polyamines and gut microbiota. Front. Nutr. 6, 1–5 (2019).
Watson, N., Dunyak, D. S., Rosey, E. L., Slonczewski, J. L. & Olson, E. R. Identification of elements involved in transcriptional regulation of the Escherichia coli cad operon by external pH. J. Bacteriol. 174, 530–540 (1992).
Tabor, C. W. & Tabor, H. Polyamines in microorganisms. Microbiol. Rev. 49, 81–99 (1985).
Maurelli, A., Fernandez, R., Bloch, C., Rode, C. & Fasano, A. ‘Black holes’ and bacterial pathogenicity: a large genomic deletion that enhances the virulence of Shigella spp. and enteroinvasive Escherichia coli. Proc. Natl. Acad. Sci. USA 95, 3943–3948 (1998).
Campilongo, R. et al. Molecular and functional profiling of the polyamine content in enteroinvasive E. coli: looking into the gap between commensal E. coli and harmful Shigella. PLoS One 9, e106589 (2014).
Igarashi, K. & Kashiwagi, K. Effects of polyamines on protein synthesis and growth of Escherichia coli. J. Biol. Chem. 293, 18702–18709 (2018).
Satink, H. et al. Microbial influences on urinary polyamine excretion. Clin. Chim. Acta 179, 305–314 (1989).
Thomas-White, K. et al. Culturing of female bladder bacteria reveals an interconnected urogenital microbiota. Nat. Commun. 9, 1557 (2018).
Thomas-White, K., Brady, M., Wolfe, A. J. & Mueller, E. R. The bladder is not sterile: history and current discoveries on the urinary microbiome. Curr. Bladder Dysfunct. Rep. 11, 18–24 (2016).
Hoyles, L. et al. Metabolic retroconversion of trimethylamine N-oxide and the gut microbiota. Microbiome 6, 73 (2018).
Bower, J. & Mulvey, M. Polyamine-mediated resistance of uropathogenic Escherichia coli to nitrosative stress. J. Bacteriol. 188, 928–933 (2006).
Bower, J., Gordon-Raagas, H. & Mulvey, M. Conditioning of uropathogenic Escherichia coli for enhanced colonization of host. Infect. Immun. 77, 2104–2112 (2009).
Carlsson, S., Wiklund, N., Engstrand, L., Weitzberg, E. & Lundberg, J. Effects of pH, nitrite, and ascorbic acid on nonenzymatic nitric oxide generation and bacterial growth in urine. Nitric Oxide - Biol. Chem. 5, 580–586 (2001).
Wheeler, M. A. et al. Bacterial infection induces nitric oxide synthase in human neutrophils. J. Clin. Invest. 99, 110–116 (1997).
Keay, S., Birder, L. & Chai, T. Evidence for bladder urothelial pathophysiology in functional bladder disorders. Biomed Res. Int. 2014, 1–15 (2014).
Tang, W. & Hazen, S. The contributory role of gut microbiota in cardiovascular disease. J. Clin. Invest. 124, 4204–4211 (2014).
Snyder, J. et al. Transcriptome of uropathogenic Escherichia coli during urinary tract infection. Infect. Immun. 72, 6373–6381 (2004).
Alteri, C. & Mobley, H. Metabolism and fitness of urinary tract pathogens. Microbiol. Spectr. 3, 1–20 (2015).
Mann, R., Mediati, D., Duggin, I., Harry, E. & Bottomley, A. Metabolic adaptations of uropathogenic E. coli in the urinary tract. Front. Cell. Infect. Microbiol. 7, 2–15 (2017).
Haugen, B. J. et al. In vivo gene expression analysis identifies genes required for enhanced colonization of the mouse urinary tract by uropathogenic Escherichia coli strain CFT073 dsdA. Infect. Immun. 75, 278–289 (2007).
Anfora, A. T., Haugen, B. J., Roesch, P., Redford, P. & Welch, R. A. Roles of serine accumulation and catabolism in the colonization of the murine urinary tract by Escherichia coli CFT073. Infect. Immun. 75, 5298–5304 (2007).
Roesch, P. L. et al. Uropathogenic Escherichia coli use D-serine deaminase to modulate infection of the murine urinary tract. Mol. Microbiol. 49, 55–67 (2003).
Willis, R. C. & Woolfolk, C. A. L-asparagine uptake in Escherichia coli. J. Bacteriol. 123, 937–945 (1975).
Armstrong, L. E. et al. Urinary indices of hydration status. Int. J. Sport Nutr. 4, 265–279 (1994).
Rolker, H., Maldonado, A., Soto-Méndes, M., Melse-Boonstra, A. & Solomons, N. Comparative evaluation of the performance of urinary biomarkers of hydration status among lactating women in the Western Highlands of Guatemala. FASEB J. 31, 650.2 (2017).
Spagou, K. et al. HILIC-UPLC-MS for exploratory urinary metabolic profiling in toxicological studies. Anal. Chem. 83, 382–390 (2011).
Edén, C. S. et al. Inhibition of experimental ascending urinary tract infection by an epithelial cell-surface receptor analogue. Nature 298, 560–562 (1982).
Clegg, S. Cloning of genes determining the production of mannose-resistant fimbriae in a uropathogenic strain of Escherichia coli belonging to serogroup O6. Infect. Immun. 38, 739–744 (1982).
Hull, R. A., Gill, R. E., Hsu, P., Minshew, B. H. & Falkow, S. Construction and expression of recombinant plasmids encoding type 1 or D-mannose-resistant pili from a urinary tract infection Escherichia coli isolate. Infect. Immun. 33, 933–938 (1981).
Müller, D., Hughes, C. & Goebel, W. Relationship between plasmid and chromosomal hemolysin determinants of Escherichia coli. J. Bacteriol. 153, 846–851 (1983).
Chambers, M. C. et al. A cross-platform toolkit for mass spectrometry and proteomics. Nat. Biotechnol. 30, 918–920 (2012).
Benton, H. P., Want, E. J. & Ebbels, T. M. D. Correction of mass calibration gaps in liquid chromatography–mass spectrometry metabolomics data. Bioinformatics 26, 2488–2489 (2010).
Tautenhahn, R., Böttcher, C. & Neumann, S. Highly sensitive feature detection for high resolution LC/MS. BMC Bioinformatics 9, 504 (2008).
Smith, C. A., Want, E. J., O’Maille, G., Abagyan, R. & Siuzdak, G. XCMS: processing mass spectrometry data for metabolite profiling using nonlinear peak alignment, matching, and identification. Anal. Chem. 78, 779–787 (2006).
Prince, J. T. & Marcotte, E. M. Chromatographic alignment of ESI-LC-MS proteomics data sets by ordered bijective interpolated warping. Anal. Chem. 78, 6140–6152 (2006).
McMillan, A., Renaud, J. B., Gloor, G. B., Reid, G. & Sumarah, M. W. Post-acquisition filtering of salt cluster artefacts for LC-MS based human metabolomic studies. J. Cheminform. 8, 44 (2016).
Smith, C. A. et al. METLIN: a metabolite mass spectral database. Ther. Drug Monit. 27, 747–751 (2005).
Haug, K. et al. MetaboLights—an open-access general-purpose repository for metabolomics studies and associated meta-data. Nucleic Acids Res. 41, D781–D786 (2013).
Wickham, H. ggplot2: Elegant Graphics for Data Analysis. (Springer, New York, 2009).
Lê, S., Josse, J. & Husson, F. FactoMineR: an R package for multivariate analysis. J. Stat. Softw. 25 (2008).
Lenth, R. emmeans: Estimated Marginal Means, aka Least-Squares Means. R package version 1.4.2. https://cran.r-project.org/package=emmeans.
Di Guida, R. et al. Non-targeted UHPLC-MS metabolomic data processing methods: a comparative investigation of normalisation, missing value imputation, transformation and scaling. Metabolomics 12, 93 (2016).
The Good Scents Company. TGSC Information System. Trimethylamine. http://www.thegoodscentscompany.com/data/rw1009301.html.
Leonardos, G., Kendall, D. & Barnard, N. Odor threshold determinations of 53 odorant chemicals. J. Air Pollut. Control Assoc. 19, 91–95 (1969).
The Good Scents Company. TGSC Information System. Tyramine. http://www.thegoodscentscompany.com/data/rw1051461.html (2006).
The Good Scents Company. TGSC Information System. Cadaverine. http://www.thegoodscentscompany.com/data/rw1149431.html.
Wang, L., Thomas, B., Warner, K., Wolf, W. & Kwolek, W. Apparent odor thresholds of polyamines in water and 2% soybean flour dispersions. J. Food Sci. 40, 274–276 (1975).
The Good Scents Company. TGSC Information System. 1,4-diaminobutane. http://www.thegoodscentscompany.com/data/rw1148651.html#toeuus.
Acknowledgements
We would like to thank Dr. Ana Cabrera for providing the urine samples used in this study. Also, Shannon Seney and for her technical assistance. As well as Dr. Jeremy Burton and Dr. Elizabeth Gillies, for providing feedback. S.P.B. was funded by a scholarship from the Mexican council for science and technology (CONACyT).
Author information
Authors and Affiliations
Contributions
Conceptualization, G.R. and S.P.B.; methodology, G.R., M.S., J.R. and S.P.B.; software, J.R. and S.P.B.; validation, J.R and S.P.B.; formal analysis, J.R. and S.P.B.; investigation, J.R. and S.P.B.; resources, G.R., M.S., and, J.R.; data curation, S.P.B.; writing (original draft preparation), S.P.B.; writing (review and editing), G.R., M.S., J.R.; visualization, S.P.B; supervision, G.R.; project administration, S.P.B.; funding acquisition, G.R.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Puebla-Barragan, S., Renaud, J., Sumarah, M. et al. Malodorous biogenic amines in Escherichia coli-caused urinary tract infections in women—a metabolomics approach. Sci Rep 10, 9703 (2020). https://doi.org/10.1038/s41598-020-66662-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-66662-x
This article is cited by
-
Rapid LC–MS assay for targeted metabolite quantification by serial injection into isocratic gradients
Analytical and Bioanalytical Chemistry (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
