
Abstract
Most diseases might be associated with acute or chronic inflammation, and the role of vitamin D in diseases has been extensively explored in recent years. Thus, we examined the associations of one of the best markers for inflammation ― C-reactive protein (CRP) with 25-hydroxyvitamin D [25(OH)D] in 24 specific diseases. We performed cross-sectional analyses among 9,809 subjects aged ≥18 years who participated in the U.S. National Health and Nutrition Examination Survey (NHANES) in 2007~2010. The generalized additive model (GAM) was used to explore the associations of CRP with 25(OH)D in different diseases, adjusted for the age, gender, examination period and race. Distributions of CRP were significantly different (P < 0.05) in gender, examination period and race, and distributions of 25(OH)D were different (P < 0.05) in the examination period and race. Generally, CRP was negatively associated with 25(OH)D for majority diseases. 25(OH)D was negatively associated with CRP generally, and the associations were disease-specific and disease category-specific. In respiratory, gastrointestinal and mental diseases, the associations tended to be approximately linear. While in metabolic diseases, the associations were nonlinear, and the slope of the nonlinear curve decreased with 25(OH)D, especially when 25(OH)D < 30 μg/L.
Similar content being viewed by others



Introduction
The exploration and understanding of disease mechanisms involved lots of aspects, for instance, the steady state decomposition process of metal ions was related to numerous diseases1, free radicals and related active substances could affect health as a mediator of tissue damage and disease2, defects in pre-mRNA splicing were proven to be a common pathogenic mechanism3, etc. In recent years, with the expanding understanding of diseases, the role of vitamin D has also been extensively explored. Vitamin D not only affected the bone metabolism regulation and female reproductive and pregnancy outcomes4, but also had potential correlation to cancer5,6. Moreover, vitamin D was also considered to have potential beneficial effects on reducing inflammation and alleviating pain7,8. Therefore, exploring the role of vitamin D in common diseases is interesting and meaningful.
Previous studies suggested that most diseases might be associated with acute or chronic inflammation to some extent9,10,11. Insufficient inflammation could lead to persistent infection of pathogens, while excessive inflammation may contribute to chronic or systemic inflammatory diseases12. C-reactive protein (CRP) was considered as one of the best markers for measuring inflammation caused by bacterial infection or tissue damage, which was produced by stimulation of interleukin-1 (IL-1) and interleukin-6 (IL-6) in liver13,14. Therefore, it is meaningful to explore the role of vitamin D in common diseases via the associations of CRP with vitamin D.
A study of 923 patients in Netherlands found that vitamin D was negatively associated with CRP in both inflammatory and non-inflammatory diseases, and the liner associations were stronger in inflammatory diseases15. However, a randomized placebo-controlled trial of 413 patients in Australia showed that the associations of CRP with vitamin D were not significant16. There is still no consensus on the association between vitamin D and CRP, and further exploration is needed. Few studies focused on the nonlinear associations between vitamin D and CRP, and vitamin D was usually considered as a categorical variable classified as deficiency or not8,17. However, categorical variable cannot reflect the overall distribution of vitamin D, and cannot fully explore the associations of CRP with vitamin D.
It is a challenge to explore the associations of CRP with vitamin D by the overall distribution of vitamin D rather than by the average level of vitamin D through conventional methods (e.g., logistic regression). Fortunately, the generalized additive model (GAM) had great potential in addressing associations of continues variables. We therefore applied GAM to explore the associations of CRP with 25(OH)D in 24 specific diseases based on 9,809 participants who at least had one of diseases in the 2007~2010 in the U.S. National Health and Nutrition Examination Survey (NHANES).
Results
Descriptive characteristics of subjects with the 24 specific diseases
A total of 9,809 participants (4,703 males, 5,106 females) were involved in this study, and the characteristics of subjects with the 24 specific diseases were showed in Table 1, respectively.
Characteristics of the study population and distributions of CRP and 25(OH)D
Distributions of CRP were significantly different (P < 0.05) in gender, examination period and race, and distributions of 25(OH)D were statistically significant (P < 0.05) in examination period and race. Characteristics of the study population and distributions of CRP and 25(OH)D concentrations were shown in Table 2.
The relationship of CRP and 25(OH)D in 24 specific diseases
As shown in Fig. 1, CRP was negatively associated with 25(OH)D generally, and the associations were different by diseases-specific. And the associated curves were similar in diseases of each category.
-
i)
In general, in respiratory and gastrointestinal diseases (category “a”) and mental diseases (category “d”), CRP and 25(OH)D presented approximate linear associations, and the linear associations were stronger in mental diseases (category “d”);
-
ii)
In metabolic diseases (category “b”), non-linear associations were presented in CRP and 25(OH)D. As 25(OH)D increasing, the downward tendency of the curves was slowing down. Taking diabetes for example, the decreasing tendency of the associated curve gradually got slow, especially when 25(OH)D was higher than 30 μg/L. Other diseases in metabolic diseases group (category “b”) also showed similar trends. Furthermore, the cut-off value of 25(OH)D in cancer was higher than in other diseases;
-
iii)
In cardiovascular and cerebrovascular diseases (category “c”) and other diseases (category “e”), there was negative liner or non-liner associations between CRP and 25(OH)D generally.

Associations between CRP and 25(OH)D in 24 specific diseases using GAM models, adjusted by age, gender, examination period and race. The vertical axis represents the smoothness function value, where the numbers in brackets represent EDF, and the dotted line represents 95% confidence interval ((a) respiratory and gastrointestinal diseases; (b) metabolic diseases; (c) cardiovascular and cerebrovascular diseases; (d) mental diseases; (e) other diseases).
The parametric effects test of 25(OH)D in GAM
Table 3. showed the parametric effects test of 25(OH)D in GAM. Associations between CRP and 25(OH)D were statistically significant in majority diseases. Those minority diseases with nonsignificant associations may due to the small sample sizes of patients.
Discussion
Vitamin D was considered to have potential beneficial effects on reducing inflammation and alleviating pain7,8. Thus, our study aimed to explore the associations of CRP with 25(OH)D in 24 specific diseases among adults of NHANES using GAM. Firstly, we found that 25(OH)D was negatively associated with CRP in general. And the associations were disease-specific and disease category-specific: in respiratory, gastrointestinal and mental diseases, the associations tended to be approximately linear. While in metabolic diseases, the associations were nonlinear, and the slope of the non-linear curve decreased with 25(OH)D, especially when 25(OH)D was less than 30 μg/ L. Secondly, the cut-off value of 25(OH)D in cancer was higher than that in other diseases.
25(OH)D was negatively associated with CRP in almost all diseases, which was similar to previous studies15,18. One of the possible reasons is vitamin D could inhibit the progression of inflammation by reducing the secretion of inflammatory cytokines such as IL-6, which could indirectly decrease the CRP level19. Another reason may be that CD8+ T cells could directly destroy the damaged or infected host cells, thereby reducing the amount of pro-inflammatory cells. Meanwhile, CD8+ T cells carried higher levels of vitamin D receptor (VDR) expression, whose function was regulated by vitamin D20,21,22, which may also indirectly down-regulate the CRP level.
In this study, associations of CRP with 25(OH)D differed in different disease categories. Similar negative associations, which presented approximate linear, were found in respiratory, gastrointestinal diseases, mental diseases and arthritis. Previous studies based on large populations showed that there was a strong dose-response association between lower vitamin D levels and increased risk of upper respiratory infection23,24. The potential mechanism for this may be that vitamin D, by activating VDR, had immunomodulatory effects on structural cells in airways25, while these cells could trigger the pathogenesis of asthma through complex interactions with inflammatory lymphocytes26. Besides, the immune regulation effect of vitamin D in asthma could both reduce airway hyper-responsiveness and inflammation, and contribute to the airway remodeling27.
Previous studied reported that vitamin D status was associated with the composition and function of the intestinal microbiome. In addition, vitamin D and VDR regulate the innate immune response to the microbiome28,29. Moreover, previous evidence suggested that vitamin D may be beneficial for autoimmune and allergic pathologies30,31.
Vitamin D may also have influence on emotion and depression32,33. This could attribute to inflammation, a well-known hypothesis mechanism for depression34. 25(OH)D was negatively associated with CRP in mental diseases. It is reported that low levels of vitamin D and VDR were significantly associated with higher levels of inflammatory markers, which could be attenuated by vitamin D supplementation35.
Further, we found nonlinearly negative associations of 25(OH)D with CRP in metabolic diseases. Previous studies also indicated that vitamin D might associate with the pathogenesis of type 2 diabetes mellitus (T2DM)36 and dyslipidemia37. It was reported that the supplementation of vitamin D may reduce systemic inflammation, that is, vitamin D supplementation had beneficial effect on the CRP levels38,39. The main potential mechanism of progression of T2DM was β cell dysfunction due to inflammatory stress and insulin resistance, while VDR was the key regulator of inflammation and beta cell survival40. There was evidence that the associations between 25(OH)D level and hypertriglyceridemia may be mediated through inflammation, as these associations disappeared after CRP as a covariate41. It was also suggested that obesity-related inflammation could lead to abnormal function of fat cells, elevate circulating levels of free fatty acid and ectopic lipid accumulation42.
In addition, in metabolic diseases, we found that the nonlinear associations of CRP with 25(OH)D had a weakening tendency as 25(OH)D increasing, which is similar with several previous studies. They found that the negative association between 25(OH)D and CRP would gradually decrease when 25(OH)D level was close to or higher than 21 μg /L43,44. This result indicated that, when the 25(OH)D level was higher than 30 μg/L, no additional clinical benefit was obtained, which was consistent with our study. It was also noteworthy that the cut-off value of 25(OH)D above-mentioned in cancer was higher than common diseases. Moreover, it was reported that higher 25(OH)D concentrations had benefits effect on the breast cancer, lung cancer and colorectal cancer45,46,47. However, the optimal doses of 25(OH)D concentration has not been determined yet48,49.
Thus, vitamin D supplementation might be always beneficial in respiratory, gastrointestinal and mental diseases, which may not so significant in metabolic diseases. Although metabolic diseases were not considered as inflammatory diseases traditionally, inflammatory components apparent promoting the disease process were increasingly taken into investigation12. The negative associations of CRP with vitamin D might provide greater potential therapeutic prospects for common diseases. Moreover, the supplementation of vitamin D in cancer should be more than that in common diseases for greater benefit.
Some limitations should be noted in present study. Firstly, the study was cross-sectional, we cannot draw a causal conclusion on the associations of CRP with 25(OH)D. Secondly, several unexplained variables might influence the associations of CRP with 25(OH)D cannot be taken into account. Thirdly, the complex sampling analysis was not involved in this study.
Conclusion
In general, 25(OH)D was negatively associated with CRP, and the associations were disease-specific and disease category-specific. In respiratory, gastrointestinal and mental diseases, the associations tended to be approximately linear. While in metabolic diseases, the associations were nonlinear, and the slope of the nonlinear curve decreased with 25(OH)D, especially when 25(OH)D less than 30 μg/ L.
Methods
Sample
The NHANES, which were conducted by Centers for Disease Control and Prevention (CDC), aimed to assess the health status of the U.S. non-institutionalized civilian population. This survey utilized a complex probability sampling design, and collected information by standardized interviews, physical examinations and tests of biological samples50,51. A total of 20,686 subjects were enrolled in NHANES in 2007~2010. Our study focused on the relationship between CRP and 25(OH)D among adults in 24 specific diseases. For this purpose, the reluctant subjects who <18 years old (7,931 participants), unwilling to accept the measurement of 25(OH)D (1,925 participants) or CRP (4 participants) were excluded, and 1,017 participants who did not have any of 24 specific diseases were also excluded. As shown in Fig. 2, finally, a total of 9,809 participants who at least had one of diseases were involved in the study.
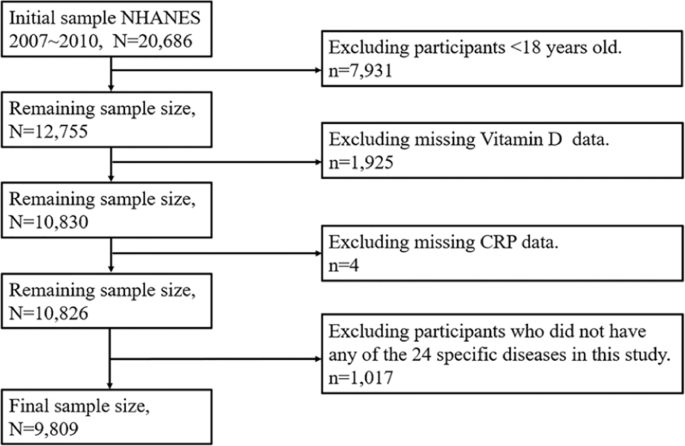
Flow chat for the study design and participants.
Data measurement
NHANES database sociodemographic information included age, gender, examination period and race. Examination period indicated the time that the participant measured the 25(OH)D, which was classified into either November 1st through April 30th or May 1st through October 31st. Because it was rather cold in the northern states in winter, the data were collected in the northern states in summer and southern states in winter52. Race was coded in 5 categories: Non-Hispanic Whites, Non-Hispanic Blacks, Mexican Americans, other Hispanics, and other non-Hispanic race including non-Hispanic multiracial.
During the NHANES physical examination, weight and height were measured in a standardized fashion. Height and weight values were automatically transmitted from stadiometers and scales to the Integrated Survey Information System database. This database was designed to reduce data errors and contained age- and sex-specific edit ranges for each body-size measure on the basis of previous NHANES data. If an entry was outside this range, the recorder was alerted that the value was unusual and required to verify the measurement53. Body mass index (BMI) was calculated by the weight divided by height squared (kg/m2). Blood specimens were processed, stored and shipped to University of Washington, Seattle, WA. CRP was quantified by latex-enhanced nephelometry using a Behring Nephelometer54. The CDC used a standardized liquid chromatography-tandem mass spectrometry (LC-MS/MS) method traceable to measure 25(OH)D3, 25(OH)D2 and C3 epimer of 25(OH)D3. Vitamin D (variable LBXVIDMS, for NHANES 2007~2010) was defined as the sum of 25(OH)D3 and 25(OH)D2 excluded the C3 epimer of 25(OH)D355.
Patients with the following diseases were defined as having been told by a doctor or other health professional: emphysema, diabetes, high cholesterol, thyroid problem, gout, kidney stone, failing kidney, anemia, heart attack, coronary heart disease (CHD), stroke, sleeping trouble, cancer, arthritis, prostate disease. Patients with asthma, chronic bronchitis and liver condition were defined as still having the disease at the time of the investigation. Patients with following diseases were defined as having these diseases started during those 30 days: cold/ chest cold, flu/ pneumonia/ ear infection, stomach or intestinal illness, anxious56. Patients with depression were defined as those whose Patient Health Questionnaire (PHQ-9) score ≥10, based on the participants’ symptoms over the past two weeks57,58. Obesity was defined those whose BMI ≥ 30 kg/m2 59. In addition, patients with cancer were defined that who had cancer or a malignancy of any kind.
In this study, 24 specific diseases were divided into 5 categories: a. respiratory and gastrointestinal diseases, including asthma, chronic bronchitis, cold/ chest cold, flu/ pneumonia/ ear infection, emphysema and stomach/intestinal illness; b. metabolic diseases, including diabetes, high cholesterol, thyroid problem, gout and obesity; c. cardiovascular and cerebrovascular diseases, including heart attack, CHD and stroke; d. mental diseases, including anxious, sleeping trouble and depression; e. other diseases, including cancer, arthritis, prostate disease, failing kidney, anemia, liver condition and kidney stone.
Statistical analysis
The x ± S and the M [P25, P75] were used to describe the distribution of continuous variables, and proportion was used to describe the distribution of categorical variables. Wilcoxon rank sum test was used to compare the continuous variables, and Rao-Scott-χ2 test was used to compare the categorical variables. CRP was log-transformed to obtain normal distributions for analysis, and back-transformed for representation in the tables. Age, gender, examination period and race were adjusted to examine the associations between log-CRP and 25(OH)D. GAM was also used to explore the associations of CRP with 25(OH)D. It was a generalization of the generalized additive model (GLM), which had great potential and flexibility in addressing non-linear relationships60. Two variables were linear associated when the estimated degrees of freedom (EDF) in GAM was equal to one. All statistical analyses were performed by R version 3.4.3, and the package “gam”61, “mgcv”62 and “glmnet”63 were used. Statistical significance was set at P < 0.05.
Ethics approval and consent to participate
All NHANES protocols were approved by the National Center for Health Statistics’ Research Ethics Review Board, all participants signed a consent form before their participations and all research was performed in accordance with relevant guidelines/regulations. The statement of informed consent is openly available in https://www.cdc.gov/nchs/nhanes/biospecimens/participants.htm.
Informed consent
Health information collected in the NHANES is kept in strictest confidence. During the informed consent process, survey participants are assured that data collected will be used only for stated purposes and will not be disclosed or released to others without the consent of the individual or the establishment in accordance with section 308(d) of the Public Health Service Act (42 U.S.C. 242 m). Only samples from participants who have consented for future research are stored in the NHANES Biospecimen Repository and are available to researchers.
Data availability
The data that support the findings of this study are openly available in https://www.cdc.gov/nchs/nhanes/. Information from NHANES is made available through an extensive series of publications and articles in scientific and technical journals. For data users and researchers throughout the world, survey data are available on the internet and on easy-to-use CD-ROMs.
References
Valko, M. & Jomova, K. Advances in metal-induced oxidative stress and human disease. Toxicology 283, 65–87 (2011).
Kehrer, J. P. & Klotz, L. O. Free radicals and related reactive species as mediators of tissue injury and disease: Implications for Health. Critical Reviews in Toxicology 45, 765–798 (2015).
Cooper, T. A., Wan, L. & Dreyfuss, G. RNA and Disease. Cell 136, 777–793 (2009).
Norman, A. W. From vitamin D to hormone D: Fundamentals of vitamin D endocrine system essential for good health. American journal of clinical nutrition 88, 491S–499S (2008).
Ma, Y., Johnson, C. S. & Trump, D. L. Mechanistic Insights of Vitamin D Anticancer Effects. Vitamins and Hormones 100, 395–431 (2016).
Grant, W. B. Roles of Solar UVB and Vitamin D in Reducing Cancer Risk and Increasing Survival. Anticancer research 36, 1357–70 (2016).
Ma, R. et al. Expressions of vitamin D metabolic components VDBP, CYP2R1, CYP27B1, CYP24A1, and VDR in placentas from normal and preeclamptic pregnancies. Am. J. Physiol. Metab. 303, E928–E935 (2012).
Rai, V., Dietz, N. E., Dilisio, M. F., Radwan, M. M. & Agrawal, D. K. Vitamin D attenuates inflammation, fatty infiltration, and cartilage loss in the knee of hyperlipidemic microswine. Arthritis Research and Therapy 18, 203 (2016).
Araki, A. & Ito, H. Diabetes mellitus and geriatric syndromes. Geriatr. Gerontol. Int. 9, 105–114 (2009).
Langhans, C. et al. Inflammation-induced acute phase response in skeletal muscle and critical illness myopathy. PloS one 9, e92048 (2014).
Wu, Y., Antony, S., Meitzler, J. L. & Doroshow, J. H. Molecular mechanisms underlying chronic inflammation-associated cancers. Cancer Letters 345, 164–173 (2014).
Guo, H., Callaway, J. B. & Ting, J. P. Inflammasomes: mechanism of action, role in disease, and therapeutics. Nature Medicine 21, 677–687 (2015).
Kao, P. C., Shiesh, S. C. & Wu, T. J. Serum C-reactive protein as a marker for wellness assessment. Ann. Clin. Lab. Sci. 36, 163–169 (2006).
Bolton, C. E. et al. The CRP genotype, serum levels and lung function in men: the Caerphilly Prospective Study. Clinical Science 120, 347–355 (2010).
Kruit, A. & Zanen, P. The association between vitamin D and C-reactive protein levels in patients with inflammatory and non-inflammatory diseases. Clinical Biochemistry 49, 534–537 (2016).
Zheng, S. et al. Vitamin D supplementation and inflammatory and metabolic biomarkers in patients with knee osteoarthritis: post hoc analysis of a randomised controlled trial - Corrigendum. Br. J. Nutr. 121, 118–119 (2019).
Bellia, A. et al. Serum 25-hydroxyvitamin D levels are inversely associated with systemic inflammation in severe obese subjects. Internal and Emergency Medicine 8, 33–40 (2013).
Ridker, P. M. High-sensitivity C-reactive protein and cardiovascular risk: rationale for screening and primary prevention. The American journal of cardiology 92, 17–22 (2003).
Khoo, A. L. et al. Translating the role of vitamin D3 in infectious diseases. Crit. Rev. Microbiol. 38, 122–135 (2012).
Bashir, M. et al. Effects of high doses of vitamin D3 on mucosa-associated gut microbiome vary between regions of the human gastrointestinal tract. European Journal of Nutrition 55, 1479–1489 (2016).
Veldman, C. M., Cantorna, M. T. & DeLuca, H. F. Expression of 1,25-dihydroxyvitamin D3 receptor in the immune system. Arch. Biochem. Biophys. 374, 334–338 (2000).
K., M. T cell-mediated cytotoxicity in: Janeway CA, Travers JP, Walport M, Shlomchik MJ, editors. New York Garl. Sci. (2011).
Belderbos, M. E. et al. Cord Blood Vitamin D Deficiency Is Associated With Respiratory Syncytial Virus Bronchiolitis. Pediatrics 127, e1513–e1520 (2011).
Ginde, A. A., Mansbach, J. M. & Camargo, C. A. Jr. Association between serum 25-hydroxyvitamin d level and upper respiratory tract infection in the third national health and nutrition examination survey. Archives of Internal Medicine 169, 384–390 (2009).
Hall, S. C., Fischer, K. D. & Agrawal, D. K. The impact of Vitamin D on asthmatic human airway smooth muscle. Expert Review of Respiratory Medicine 10, 127–135 (2016).
Pain, M. et al. Tissue remodelling in chronic bronchial diseases: From the epithelial to mesenchymal phenotype. European Respiratory Review 23, 118–130 (2014).
Hall, S. C. & Agrawal, D. K. Vitamin D and Bronchial Asthma: An Overview of Data From the Past 5 Years. Clinical Therapeutics 39, 917–929 (2017).
Weiss, S. T. & Litonjua, A. A. Vitamin D, the Gut Microbiome, and the Hygiene Hypothesis. How Does Asthma Begin? Am. J. Respir. Crit. Care Med. 191, 492–493 (2015).
Cantorna, M. T., McDaniel, K., Bora, S., Chen, J. & James, J. Vitamin D, immune regulation, the microbiota, and inflammatory bowel disease. Exp. Biol. Med. 239, 1524–1530 (2014).
Agmon-Levin, N., Theodor, E., Segal, R. M. & Shoenfeld, Y. Vitamin D in systemic and organ-specific autoimmune diseases. Clin. Rev. Allergy Immunol. 45, 256–266 (2013).
Muehleisen, B. & Gallo, R. L. Vitamin D in allergic disease: Shedding light on a complex problem. Journal of Allergy and Clinical Immunology 131, 324–329 (2013).
Giovannucci, E. Expanding roles of vitamin d. Journal of Clinical Endocrinology & Metabolism 94(2), 418 (2009).
Hoogendijk, W. et al. Depression is associated with decreased 25-hydroxyvitamin d and increased parathyroid hormone levels in older adults. Archives of General Psychiatry 65, 508–512 (2008).
Maes, M. Major depression and activation of the inflammatory response system. Ceska a Slovenska Psychiatrie 95, 233–243 (1999).
Timms, P. M. et al. Circulating MMP9, vitamin D and variation in the TIMP-1 response with VDR genotype: mechanisms for inflammatory damage in chronic disorders? QJM 95, 787–96 (2002).
Gagnon, C. et al. Serum 25-Hydroxyvitamin D, Calcium Intake, and Risk of Type 2 Diabetes After 5 Years. Diabetes Care 34, 1133–1138 (2011).
Karhapää, P. et al. Diverse associations of 25-hydroxyvitamin D and 1,25-dihydroxy-vitamin D with dyslipidaemias. J. Intern. Med. 268, 604–610 (2010).
Krasowska, K. et al. The Preoperative Supplementation With Vitamin D Attenuated Pain Intensity and Reduced the Level of Pro-inflammatory Markers in Patients After Posterior Lumbar Interbody Fusion. Front. Pharmacol. 10, 527 (2019).
Razzaghi, R. et al. The effects of vitamin D supplementation on wound healing and metabolic status in patients with diabetic foot ulcer: A randomized, double-blind, placebo-controlled trial. J. Diabetes Complications 31, 766–772 (2017).
Wei, Z. et al. Vitamin D Switches BAF Complexes to Protect β Cells. Cell 173, 1135–1149.e15 (2018).
Guasch, A. et al. Plasma vitamin D and parathormone are associated with obesity and atherogenic dyslipidemia: A cross-sectional study. Cardiovascular Diabetology 11 (2012).
Amer, M. & Qayyum, R. Relation between serum 25-hydroxyvitamin D and C-reactive protein in asymptomatic adults (from the continuous national health and nutrition examination survey 2001 to 2006). American Journal of Cardiology 109, 226–230 (2012).
García-Bailo, B. et al. Plasma Vitamin D and Biomarkers of Cardiometabolic Disease Risk in Adult Canadians, 2007–2009. Preventing Chronic Disease 10 (2013).
Kim, M., Na, W. & Sohn, C. Correlation between vitamin D and cardiovascular disease predictors in overweight and obese Koreans. Journal of Clinical Biochemistry and Nutrition 167–171, https://doi.org/10.3164/jcbn.12-81 (2013).
McDonnell, S. L. et al. Breast cancer risk markedly lower with serum 25-hydroxyvitamin D concentrations >/=60 vs <20 ng/ml (150 vs 50 nmol/L): Pooled analysis of two randomized trials and a prospective cohort. PLoS One 13, e0199265 (2018).
Feng, Q., Zhang, H., Dong, Z., Zhou, Y. & Ma, J. Circulating 25-hydroxyvitamin D and lung cancer risk and survival: A dose-response meta-analysis of prospective cohort studies. Medicine (Baltimore). 96, e8613 (2017).
Maalmi, H. et al. Association between Blood 25-Hydroxyvitamin D Levels and Survival in Colorectal Cancer Patients: An Updated Systematic Review and Meta-Analysis. Nutrients 10 (2018).
Mondul, A. M. et al. Vitamin D and cancer risk and mortality: State of the science, gaps, and challenges. Epidemiologic Reviews 39, 28–48 (2017).
Madden, J. M., Murphy, L., Zgaga, L. & Bennett, K. De novo vitamin D supplement use post-diagnosis is associated with breast cancer survival. Breast Cancer Research and Treatment 172, 179–190 (2018).
U.S. Census Bureau. Current Population Survey (CPS) - Definitions and Explanations (2008).
Services, U. S. D. of H. and H. Poverty guidelines, research, and measurement. US Dep. Heal. Hum. Serv. website. Available online, http//aspe. hhs. gov/POVERTY/index. shtml/(accessed 16 March 2012) (2010).
Freedman, D. M., Looker, A. C., Abnet, C. C., Linet, M. S. & Graubard, B. I. Serum 25-hydroxyvitamin D and cancer mortality in the NHANES III study (1988-2006). Cancer Res. 70, 8587–8597 (2010).
National Center for Health Statistics (NCHS) Anthropometry procedures manual. National Health and Nutrition Examination Survey (NHANES). Available at: http://www.cdc.gov/nchs/data/nhanes/nhanes_11_12/Anthropometry_Procedures (2011).
Huffman, F. G., Gomez, G. P. & Zarini, G. G. Metabolic syndrome and high-sensitivity C-reactive protein in Cubans. Ethnicity and Disease 19, 115–120 (2009).
Yetley, E. A. et al. NHANES Monitoring of Serum 25-Hydroxyvitamin D: A Roundtable Summary. J. Nutr. 140, 2030S–2045S (2010).
Centers for Disease Control. NHANES 2007-2008 Questionnaire Data. Available at: https://wwwn.cdc.gov/nchs/nhanes/search/datapage.aspx?Component=Questionnaire&CycleBeginYear=2007.
Manea, L., Gilbody, S. & McMillan, D. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): A meta-analysis. Cmaj 184 (2012).
Kroenke, K., Spitzer, R. L. & Williams, J. B. W. The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine 16, 606–613 (2001).
Buser, M. C., Murray, H. E. & Scinicariello, F. Age and sex differences in childhood and adulthood obesity association with phthalates: Analyses of NHANES 2007-2010. Int. J. Hyg. Environ. Health 217, 687–694 (2014).
Hastie, T. & Tibshirani, R. Generalized additive models for medical research. Stat. Methods Med. Res. 4, 187–196 (1995).
Hastie, T. J. & Pregibon, D. Generalized linear models. In Statistical Models in S 195–247, https://doi.org/10.1201/9780203738535 (2017).
Simon, N. et al. Fast stable restricted maximum likelihood and marginal likelihood estimation of semiparametric generalized linear models. Journal of the Royal Statistical Society: Series B (Statistical Methodology) 73, 3–36 (2011).
Simon, N., Friedman, J., Hastie, T. & Tibshirani, R. Regularization Paths for Cox’s Proportional Hazards Model via Coordinate Descent. Journal of Statistical Software 39 (2011).
Acknowledgements
This work was supported by the Natural Science Foundation of Science and Technology Department of Jilin Province, China (grant number: 20180101129JC), Outstanding Youth Foundation of Science and Technology Department of Jilin Province, China (grant number: 20170520049JH), the National Natural Science Foundation of China (grant number: 11301213 and 11571068), the National Key Research and Development Program of China (grant number: 2016YFC1303800).
Author information
Authors and Affiliations
Contributions
F.Y., M.Z.S., L.N.J. and Y.Y. had the original idea for the study, and with all co-authors, carried out the design. Y.Y. provided valuable insight regarding the methodological approach and organization of the manuscript. M.Z.S. and C.S. carried out the statistical analysis and reviewed the consistency of data included in the paper. F.Y. and M.Z.S. wrote the first draft of the manuscript. M.Z.S., J.G.L., X.N.Y., C.L.B., M.W. and L.Y.P. performed the interpretation of the results and wrote the final version of article in collaboration with Y.Y. and L.N.J. F.Y., M.Z.S., J.M.W., C.X.W., M.Z.X., Y.Y. and L.N.J. revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yang, F., Sun, M., Sun, C. et al. Associations of C-reactive Protein with 25-hydroxyvitamin D in 24 Specific Diseases: A Cross-sectional Study from NHANES. Sci Rep 10, 5883 (2020). https://doi.org/10.1038/s41598-020-62754-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-62754-w
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
