
Abstract
Using for-presentation and for-processing digital mammograms, the presence of microcalcifications has been shown to be associated with short-term risk of breast cancer. In a previous article we developed an algorithm for microcalcification cluster detection from for-presentation digital mammograms. Here, we focus on digitised mammograms and use a three-step algorithm. In total, 253 incident invasive breast cancer cases (with a negative mammogram between three months and two years before diagnosis, from which we measured microcalcifications) and 728 controls (also with prior mammograms) were included in a short-term risk study. After adjusting for potential confounding variables, we found evidence of an association between the number of microcalcification clusters and short-term (within 3–24 months) invasive breast cancer risk (per cluster OR = 1.30, 95% CI = (1.11, 1.53)). Using the 728 postmenopausal healthy controls, we also examined association of microcalcification clusters with reproductive factors and other established breast cancer risk factors. Age was positively associated with the presence of microcalcification clusters (p = 4 × 10−04). Of ten other risk factors that we studied, life time breastfeeding duration had the strongest evidence of association with the presence of microcalcifications (positively associated, unadjusted p = 0.001). Developing algorithms, such as ours, which can be applied on both digitised and digital mammograms (in particular for presentation images), is important because large epidemiological studies, for deriving markers of (clinical) risk prediction of breast cancer and prognosis, can be based on images from these different formats.
Similar content being viewed by others

Introduction
Microcalcifications are deposits of calcium oxalate and calcium phosphate within the breast tissue that appear as white specks on a mammogram. The mechanisms by which microcalcifications occur are not clearly understood, although many factors are suspected to play a role, such as age, hormonal unbalance, pregnancy, breastfeeding and diet change. Active cellular processes, or effects of cellular degeneration may be involved1. Calcification deposits are found within the ductal system, the breast acini, stroma and vessels2. Microcalcifications are present in approximately 55% of nonpalpable breast malignancies and are responsible for the detection of 85–95% of cases of ductal carcinoma in situ (DCIS) by screening mammography3, and they can also be present in invasive cancers4. The role of microcalcifications in the detection of breast cancer has been widely studied and some research groups have even investigated the role of microcalcifications in terms of risk and progression of breast cancer.
Previous studies have shown that women with false-positive results at screening have, on average, higher risks of breast cancer being detected at subsequent mammographic examinations than women with negative screening results5,6,7, in particular, when the false positive results are due to microcalcifications at mammography8. Detected abnormalities, although noncancerous, may therefore be useful as imaging features for breast cancer risk prediction. Microcalcifications represent a challenge in both perception and interpretation; between 12.7% and 41.2% of women are recalled with calcifications as the main mammographic feature/finding in screening programs. Although the value of using the computer aided detection (CAD) in breast screening is questioned9, in a study in the U.S., where CAD is used routinely in screening, it has been shown that false positive recall is associated with short-term risk of breast cancer10. It has also been demonstrated that CAD generated false positive detection, which includes the assessment of the presence of suspicious microcalcifications, can be used as a quantitative imaging marker of short-term breast cancer risk11. Further, it has been shown in a population where CAD is not routinely used, that the presence of clustered microcalcifications detected by a CAD algorithm, is important for short-term risk prediction12, even of invasive breast cancer.
Although almost all mammograms, nowadays, are acquired with full-field digital mammography systems (and are available in either for-processing or for-presentation formats, or both), some valuable databases contain predominantly traditional screen-film mammographic images. In the current paper, we adapt a method that we recently developed for detecting microcalcification clusters in for-presentation digital images13, for use on digitised images. Developing such algorithms as ours, which can be applied on both digitised and for-presentation digital mammograms, is important because large epidemiological studies, for deriving markers of (clinical) risk prediction of breast cancer and for studying prognosis, may have to be based on banks of images from different formats. We evaluate our algorithm in an epidemiological study of the short term risk of breast cancer using a case-control study design.
Our algorithms are specifically intended to be used in studies aimed at improving understanding of the importance/potential of microcalcifications for short-term risk prediction. Unlike in the development of CAD algorithms for suspicious microcalcification detection, in our context there is no gold-standard that can be derived and trained against. The underlying logic of our approach is that even if no detectable tumor is currently present, there may be characteristics in a woman’s mammographic image, picked up by our algorithm, that are indicative of an increased risk of breast cancer in the near future (the coming few years). It would of course be possible to use existing CAD algorithms, e.g. based on deep learning in short-term risk prediction models (see Mordang et al.14 for a deep learning approach to microcalcification detection, trained against radiologists annotations, in for-processing digital images, and see Wang & Yang15 for a deep learning approach to distinguish between benign and malignant calcifications), but they may not be optimal for our purpose. CAD algorithms are designed specifically for cancer detection and are focused on malignant calcifications. However, even non-malignant calcifications may be indicative of a future risk.
To shed some light on the processes generating the microcalcification clusters that are picked up by our algorithm and to further demonstrate the algorithm’s validity, we also study association with classical breast cancer risk factors.
In summary, the purposes of our study are (1) to describe the adaptation of our algorithm (described previously for for-presentation digital images) for potential microcalcification cluster assessment on digitised mammograms and to investigate the association of these clusters with the short-term risk of developing invasive breast cancer, and (2) to investigate the associations of established breast cancer (mainly reproductive history) risk factors with the presence of microcalcification clusters on mammograms.
Methods
Materials
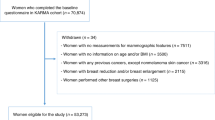
Our analysis is based on CAHRES (Cancer and Hormone Replacement Study), a population-based post-menopausal breast cancer case-control study of Swedish residents born in Sweden and aged 50 to 74 years, between October 1993 and 31 March 1995. The CAHRES study base, from which we selected a subset of cases and controls, includes approximately 6000 women (approximately 3000 cases and 3000 age group matched controls). Details on data collection in CAHRES have been described elsewhere16. All cases had primary invasive breast cancer. CAHRES was able to collect (via screening and radiology units) mammograms for approximately 75% of its cases17. After making a number of exclusions (see Eriksson et al.17) e.g. for having implants in the breast, a measure of percent density was able to be calculated for 1747 cancer patients, on mammograms close to diagnosis (the median time before diagnosis for these mammograms was 50 days). Area-based percent density (PD) has been measured for these women using Cumulus18, a computer-assisted thresholding technique, using the mammogram contralateral to the tumor. We were able to trace negative screens prior to diagnosis for 1338 of these cancer patients, but only 662 had a negative screening within 3−24 months before diagnosis. Of these, 325 had mediolateral oblique (MLO) mammograms from both left and right breasts. In the current study we used mammograms from 253 of these cases for which complete data on age, BMI, hormone replacement therapy (HRT) status, parity, smoking status, diabetes status, and age at menopause were available. We used a similar procedure, to that used for the cancer patients (cases), for selecting controls from the original CAHRES study base, by searching for images within 3−24 months before questionnaire date, and found 728 women that had both left and right mammograms as well as complete data for the covariates. In controls, PD had been measured from a single mammogram, with side chosen at random. We note that we could use fewer cases (253) than controls (728) because we needed the exact diagnostic date for cases, which was sometimes missing.
For both cases and controls, body mass index (BMI) was recorded at entrance to the study, whereas age, in this study, was defined as age at mammography. Mammograms were digitised with an Array 2905 HD Laser Film Digitizer (Array Corporation, Tokyo, Japan), which cover a range of 0−4.7 optical density. The size of the images was 4770 × 3580 pixels with 0.05 mm per pixel. Informed consent was obtained from all individual participants included in the study, and the study had the approval of the ethics review board at Karolinska Institutet, Stockholm, Sweden.
Additional information (with some missing values) on breast feeding, life time breast feeding duration, and age at first birth for parous women was included in an additional analysis of association with case-control status and also in our analysis of association of microcalcifications with breast cancer risk factors.
Microcalcification cluster detection
Our proposed approach for microcalcification cluster detection, which is described in details in our earlier paper13, can be divided into the following steps: (a) image preprocessing, consisting mainly of denoising, quality improvement and enhancement of small objects, (b) identification of microcalcifications, (c) filtering out noise and grouping microcalcifications into clusters; see Fig. 1. The main differences between digital for-presentation and traditional screen-film mammograms are in terms of image contrast, post-acquisition enhancement steps and the amount of noise. It is therefore mainly the preprocessing step of our algorithm for for-presentation digital images13 that needs to be adapted for use on screen-film mammograms.

A schematic overview of the proposed method. (a) Shows the original digitised image before preprocessing and (b) shows the image after breast profile segmentation and denoising, (c) Shows the output of each step of microcalcification detection on three different patches. The preprocessing step includes the intensity transformation and the DOG filtering. The detection of candidates includes the HOG filtering and the thresholding. The final step includes removing noise and clustering of potential microcalcifications. Microcalcifications in magenta were retained whilst those in green were discarded in the cleaning step (clusters are in circles).
Preprocessing of screen-film mammograms
The main aim of the preprocessing step is to separate the breast from other objects in the mammogram (i.e. labels, tags and screening artefacts, see Fig. 1(a)) with a minimum loss of breast tissue. To segment the breast profile, the contrast of the image first needed to be enhanced to brighten the low-intensity pixels close to the skin line. This was achieved using a logarithmic transformation of the image. The image was then segmented into three classes according to Otsu’s multithresholding method. The two brightest classes were kept since they corresponded to the breast region and the other objects in the mammogram, whilst the darkest corresponded to the background. The breast mask was finally extracted as the largest group of connected components and smoothed using morphological filtering.
In digitised mammograms, intrinsic noise can occur during the scanning, due to dust and artefacts present on the film or in the scanner. To reduce this noise, we fist applied morphological opening using a disk structuring element of one pixel radius and we then used the Anscombe transformation where noise was removed in the Anscombe domain through an adaptive Wiener filter19. From this step on, we used the same procedures as were used with for-presentation digital images13.
The microcalcifications are among the brightest objects in the image, so we spread out the upper gray levels (and contract the lower gray levels) by applying intensity transformations using the cosine function. We finally applied the Difference of Gaussian filter (DoG), a band-pass filter in which both cut-off frequencies were parametrised to be associated with microcalcification candidate sizes.
Microcalcification detection and grouping
The segmentation of microcalcifications in mammographic images is challenging due to several reasons. Due to their physical properties, they are arbitrarily shaped spots of a limited range of sizes and there are often strong variations in the background, which can introduce structures which are similar to those of microcalcifications. Also, a noisy background in an image can sometimes exceed the signal of interest. We tackled these problems by applying a selective detector (Hessian of Gaussian (HOG)), targeting both blob-like and line-like structures20, that can enhance the brightness of microcalcifications and, at the same time, give more homogeneous linear structures. After applying thresholding operations to obtain the microcalcification candidate, all objects with shapes, sizes and appearances similar to microcalcifications were then filtered to reduce the noise. The last step involved microcalcification grouping using a Density-Based Spatial Clustering of Applications with Noise (DBSCAN) algorithm21. The same parameters that were defined for for-presentation images13 were used here.
Statistical analysis
We evaluated the association between the presence of microcalcification clusters and case-control status by fitting a logistic regression model treating case-control status as the dependent variable. We treated the total number of microcalcification clusters in the left and right breasts as an independent variable. The variable used in our study of for-presentation images was defined in the same way. We first fitted logistic regression using all cases (253) and controls (728) by including the covariates age (continuous), BMI (continuous), PD (continuous), HRT (categorical), parity (continuous), smoking status (categorical), diabetes status (categorical) and age at menopause (continuous), as adjustment variables. In an additional logistic regression analysis we also added breastfeeding and age at first birth as adjustment variables. Because these variables are defined only for non-parous women, we combined the variables parity, breastfeeding and age at first birth into a single categorical variable with 9 categories. We also calculated and compared AUCs for two models, with and without the total number of microcalcification clusters variable entered as a covariate. In both cases all other covariates, except breastfeeding and age at first birth were included (i.e. we used the first model). To avoid over-fitting, we calculated “honest” values (of the AUCs) using the bootstrap procedure described by Harrell et al.22. We note that the AUCs will be partially age-adjusted23 (i.e. will partly remove the effect of age), due to the fact that the study base, CAHRES, matched cases and controls within five year age groups.
To assess, at a population level, the association between a selection of established breast cancer risk factors (one at a time) with the presence of microcalcification clusters, using only breast cancer-free controls, we fitted a number of age-adjusted logistic regression models. We chose to study microcalcification clusters as a binary variable here (0 vs. 1+ microcalcification clusters). The data was too sparse to use multinomial logistic regression. Use of logistic regression is also consistent with a previous study of factors of vascular calcifications24. The risk factors were age, BMI, PD, parity, age at first birth, breastfeeding duration, breastfeeding, HRT use, smoking status, diabetes status and age at menopause, and these were treated in the same way as in the risk analysis. In the results section we report parameter estimates from the models as odds ratios (OR) (with 95% confidence intervals (CI)). All analyses were performed in accordance with relevant institutional and national guidelines and regulations.
Consent for publication
All authors approved the manuscript and consented for publication.
Results
We illustrate the results of applying our algorithm for detecting microcalcifications, for an example of digitised image; see Fig. 1. First, we segment the breast profile to remove tags and background noise. We denoise the image to improve its quality and we enhance the contrast of small objects. We show the output of each step on three different patches in Fig. 1(c): a group of microcalcifications in the first two rows, and a false detection caused by linear structures in the third row. After the identification of microcalcifications, we filter out noise and group microcalcifications into clusters since isolated calcifications are not clinically significant.
Key characteristics of cases and controls included in our association analyses are described in Table 1. There was strong evidence that both PD and HRT use are (positively) associated with case-control status.
After adjusting for potential confounding variables (BMI, PD, HRT, parity, smoking status, diabetes status and age at menopause), we found evidence of an association between the total number of microcalcification clusters and short-term invasive breast cancer risk (per cluster OR = 1.306, 95% CI = (1.112–1.534), p = 1 × 10−03), see Table 2. The association for PD was OR = 1.022, 95% CI = (1.012–1.034), p = 1 × 10−04; this corresponds, for example, to an OR of 5.1 when comparing women with a difference in PD of 75%. In a second logistic regression where we adjusted for all potential confounding variables (210 cases and 605 controls), we found similar evidence of association with the number of microcalcification clusters (OR = 1.278, 95% CI = (1.069–1.529), p = 7 × 10−03). In this model the OR for PD was 1.025, 95% CI = (1.012–1.038), p = 1 × 10−04). Using a bootstrapping procedure (based on 1000 bootstrap samples), we obtained honest estimates of 0.656 and 0.645 for the AUCs for the full model, with and without the total number of potential microcalcification clusters, respectively (the corresponding apparent AUCs were 0.680 and 0.667).
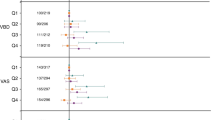
Among the 728 postmenopausal healthy women, 27% had microcalcification clusters at mammography. Age was positively associated with the presence of microcalcification clusters (Table 3). Results from the association analysis of the other risk factors with microcalcification clusters, based on fitting age-adjusted models are presented in Table 3. Analyses were carried out on subsets of individuals with complete data on the risk factors (one-at-a-time). Life time duration of breastfeeding was positively and significantly associated with the presence of microcalcification clusters (unadjusted p-value = 0.001). We found a suggestion of positive association with diabetes status (unadjusted p-value = 0.019) and of negative associations with smoking status, and age at first birth (unadjusted p-values of 0.006 and 0.044, respectively), but none of these associations withstood the (admittedly conservative) Bonferroni correction for multiple testing. No significant association was found between HRT use, PD, BMI, or age at menopause and the presence of microcalcification clusters.
Discussion
We have adapted an algorithm for detecting microcalcifications which was originally developed for for-presentation digital images, for use on digitised film mammograms and, in a case-control study of postmenopausal invasive breast cancer, using negative screening images taken prior to diagnosis, have shown that our measure of microcalcification clusters is significantly associated with short-term risk of invasive breast cancer. In this study, we provide further evidence that microcalcifications can predict the future risk of invasive breast cancer.
Many factors that increase the long-term risk of breast cancer are now known, such as a high percent density, a family history of breast cancer, a late age of first birth, an early onset of first menstruation, a late age at menopause. A large number of genetic markers of susceptibility to the disease, both rare and common have also been identified25. Whilst factors such as those listed above may be useful for long-term individualised screening26, there is also a need to find factors associated with short-term breast cancer risk, for which there would be an immediate clinical relevance (recalling women to screening earlier if they have a high short-term risk). As we, and others, have shown, incorporating potential microcalcification clusters on mammography can be helpful for short-term breast cancer risk prediction.
The association of the presence of microcalcification clusters and age can be due to involution27 or to noncancerous lumps shrinking and calcifying with menopause and aging. To our knowledge, ours is the first study to describe an association between breast feeding and the presence of microcalcification clusters. Several cases of postlactational microcalcifications have been reported in the literature28,29. This might be a result of a combination of programmed cell death (apoptosis) and stasis of secretions29, since upon cessation of lactation the breast decreases in size as the glandular elements regress and atrophy.
The mechanisms by which these factors are associated with microcalcifications is still not clear and it is possible that these factors are associated differently across subtypes of microcalcification clusters.
In the current study, we considered all type of microcalcifications. For example, the output of our algorithm will include breast arterial calcifications (BAC), which are small calcium deposits in the vessel walls of the arteries; see Fig. 2(b). These are in fact one of the most common false positives detected by CAD systems. We note that these calcifications are a risk factor for cardiovascular disease and that studies have shown that increasing age, diabetes, parity and earlier age at first birth are associated with higher BAC prevalence24,30, whereas smoking is associated with lower BAC prevalence30.

Examples of calcification: (a) shows microcalcifications, and (b) shows breast arterial calcifications.
The confidence intervals for the effect size of microcalcification clusters in this study (OR = 1.306; 95% CI: (1.112,1.534)) and in our previous study13 (OR = 1.510; 95% CI: (1.317,1.733)), which was based on for-presentation mammograms, largely overlap. We suspect, however, that the “true” effect size based on digitised images may be smaller due to the quality of the images, since digital mammograms offer improved image contrast, and no digitisation noise, as well as access to information about the exact pixel resolution of the images. We would also point out that the women considered in this study are older than in our previous study, which means that there is a higher rate of detected microcalcification clusters due to age. There are limitations to any detection process, regardless of image format; it is not possible to account for random artifacts and noise that occur during the acquisition/digitisation step. In addition, studies have shown that microcalcification detection is sensitive to image quality and the radiation doses that are used31,32.
We reiterate that it is important to develop algorithms for novel image-based markers that can be derived from both digital and digitised mammograms in order to open the door for research based on large collections of mammograms. We are, for example, currently working on a study of mammographic features for the early prediction of invasive breast cancer subtypes which is based on combining digital and digitised mammograms. Another interesting line of research would be to investigate the association of features describing microcalcification clusters, such as cluster locations in the breast, morphology and density, with cancer risk. It would even be interesting to study the relationships of these features with cancer risk factors. In a future study, we would like to test for association between microcalcification clusters and breastfeeding duration based on digital images.
Conclusion
We have presented a method for microcalcification detection using digitised images. Our results confirm the association between the number of microcalcification clusters and the short-term risk of being diagnosed with invasive breast cancer. We have also reported associations between the presence of microcalcification clusters and a selection of breast cancer risk factors. Lifetime breast feeding duration was found to be positively associated with the presence of microcalcifications.
References
Wilkinson, L., Thomas, V. & Sharma, N. Microcalcification on mammography: approaches to interpretation and biopsy. The British journal of radiology 90(1069), 20160594 (2017).
Henrot, P., Leroux, A., Barlier, C. & Génin, P. Breast microcalcifications: The lesions in anatomical pathology. Diagnostic and Interventional Imaging 95(2), 141–152, https://doi.org/10.1016/j.diii.2013.12.011, http://www.sciencedirect.com/science/article/pii/S2211568413003884, Radio-histological correlations in breast imaging (2014).
Bent, C. K., Bassett, L. W., D’Orsi, C. J. & Sayre, J. W. The positive predictive value of bi-rads microcalcification descriptors and final assessment categories. American Journal of Roentgenology 194(5), 1378–1383 (2010).
Stomper, P. C., Geradts, J., Edge, S. B. & Levine, E. G. Mammographic predictors of the presence and size of invasive carcinomas associated with malignant microcalcification lesions without a mass. American Journal of Roentgenology 181(6), 1679–1684 (2003).
Goossens, M. C. et al. Breast cancer risk is increased in the years following false-positive breast cancer screening. European Journal of Cancer Prevention 26(5), 396 (2017).
McCann, J., Stockton, D. & Godward, S. Impact of false-positive mammography on subsequent screening attendance and risk of cancer. Breast Cancer Research 4(5), R11 (2002).
Román, M., Castells, X., Hofvind, S. & von Euler-Chelpin, M. Risk of breast cancer after false-positive results in mammographic screening. Cancer medicine 5(6), 1298–1306 (2016).
Castells, X. et al. Risk of breast cancer in women with false-positive results according to mammographic features. Radiology 280(2), 379–386 (2016).
Lehman, C. D. et al. Diagnostic accuracy of digital screening mammography with and without computer-aided detection. JAMA internal medicine 175(11), 1828–1837 (2015).
Henderson, L. M., Hubbard, R. A., Sprague, B. L., Zhu, W. & Kerlikowske, K. Increased risk of developing breast cancer after a false-positive screening mammogram. Cancer Epidemiology and Prevention. Biomarkers 24(12), 1882–1889 (2015).
Mirniaharikandehei, S., et al. Applying a cad-generated imaging marker to assess short-term breast cancer risk. In: Medical Imaging 2018: Computer-Aided Diagnosis, vol. 10575, p. 105753F. International Society for Optics and Photonics (2018)
Eriksson, M. et al. A clinical model for identifying the short-term risk of breast cancer. Breast Cancer Research 19(1), 29, https://doi.org/10.1186/s13058-017-0820-y (2017).
Alsheh Ali, M., Eriksson, M., Czene, K., Hall, P. & Humphreys, K. Detection of potential microcalcification clusters using multi vendor for-presentation digital mammograms and associations with short-term breast cancer risk. Medical physics 46(4), 1938–1946 (2019).
Mordang, J.-J. et al. Automatic microcalcification detection in multi-vendor mammography using convolutional neural networks. In International Workshop on Digital Mammography, Springer, 35–42 (2016).
Wang, J. & Yung, Y. A context-sensitive deep learning approach for microcalcification detection in mammograms. Pattern recognition 78, 12–22 (2018).
Magnusson, C. et al. Breast-cancer risk following long-term oestrogen-and oestrogen-progestin-replacement therapy. International Journal of Cancer 81(3), 339–344 (1999).
Eriksson, L., Czene, K., Rosenberg, L., Humphreys, K. & Hall, P. The influence of mammographic density on breast tumor characteristics. Breast cancer research and treatment 134(2), 859–866 (2012).
Byng, J. W., Boyd, N., Fishell, E., Jong, R. & Yaffe, M. J. The quantitative analysis of mammographic densities. Physics in Medicine & Biology 39(10), 1629 (1994).
Vieira, M.A., Bakic, P.R., Maidment, A.D., Schiabel, H. & Mascarenhas, N.D. Filtering of poisson noise in digital mammography using local statistics and adaptive wiener filter. In: International Workshop on Digital Mammography, pp. 268–275. Springer (2012).
Jerman, T., Pernuš, F., Likar, B. & Špiclin, Ž. Enhancement of vascular structures in 3d and 2d angiographic images. IEEE transactions on medical imaging 35(9), 2107–2118 (2016).
Ester, M., et al. A density-based algorithm for discovering clusters in large spatial databases with noise. In: Kdd, vol. 96, pp. 226–231 (1996).
Harrell, F. E., Lee, K. L. & Mark, D. B. Multivariable prognostic models: issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Statistics in medicine 15(4), 361–387 (1996).
Pepe, M. S., Fan, J. & Seymour, C. W. Estimating the receiver operating characteristic curve in studies that match controls to cases on covariates. Academic radiology 20(7), 863–873 (2013).
Bielak, L. F., Whaley, D. H., Sheedy, P. F. & Peyser, P. A. Breast arterial calcification is associated with reproductive factors in asymptomatic postmenopausal women. Journal of Women’s Health 19(9), 1721–1726 (2010).
Michailidou, K. et al. Genome-wide association analysis of more than 120,000 individuals identifies 15 new susceptibility loci for breast cancer. Nature genetics 47(4), 373 (2015).
Hall, P. & Easton, D. Breast cancer screening: time to target women at risk. British Journal of Cancer 108, 2202–2204 (2013).
Preto, A., et al. Mammographic calcifications revisited. pp. C–127. European Society of Radiology, https://doi.org/10.1594/ecr2008/C-127 (2008)
Giron, G. L., Boolbol, S. K., Gross, J., Cohen, J. M. & Feldman, S. Postlactational microcalcifications. The breast journal 10(3), 247–252 (2004).
Stucker, D. T. et al. New bilateral microcalcifications at mammography in a postlactational woman: case report. Radiology 217(1), 247–250 (2000).
Hendriks, E. J. et al. Breast arterial calcifications: a systematic review and meta-analysis of their determinants and their association with cardiovascular events. Atherosclerosis 239(1), 11–20 (2015).
Warren, L. et al. Dependence of detectability of microcalcification clusters on quality of mammography images. Breast Cancer Research 13(1), P23 (2011).
Zanca, F. et al. Evaluation of clinical image processing algorithms used in digital mammography. Medical physics 36(3), 765–775 (2009).
Acknowledgements
This work was supported by the Swedish Research Council [grant number 2016-01245], the Swedish Cancer Society [grant number CAN 2017/287], the Swedish e-Science Research Centre, and the Cancer Health Risk Prediction Centre (CRISP; www.crispcenter.org), a Linneus Centre (contractID 70867902) financed by the Swedish Research Council. Open access funding provided by Karolinska Institute.
Author information
Authors and Affiliations
Contributions
M.A.A. and K.H. were involved in the development and application of the methodology, were responsible for interpreting the results, and drafting and revising the manuscript. K.C. and P.H. helped in collection and assembly of data and in revising the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alsheh Ali, M., Czene, K., Hall, P. et al. Association of Microcalcification Clusters with Short-term Invasive Breast Cancer Risk and Breast Cancer Risk Factors. Sci Rep 9, 14604 (2019). https://doi.org/10.1038/s41598-019-51186-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-51186-w
This article is cited by
-
MRFE-CNN: multi-route feature extraction model for breast tumor segmentation in Mammograms using a convolutional neural network
Annals of Operations Research (2023)
-
Is loss of p53 a driver of ductal carcinoma in situ progression?
British Journal of Cancer (2022)
-
Mammographic microcalcifications and risk of breast cancer
British Journal of Cancer (2021)
-
DNA methylation landscape of triple-negative ductal carcinoma in situ (DCIS) progressing to the invasive stage in canine breast cancer
Scientific Reports (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
