
Abstract
Anemia defined as reduced hemoglobin levels of red blood cells may carry less oxygen to skeletal muscle and impair physical performance. Previous studies have shown that exercise intolerance was related to moderate or severe anemia, however, the relationship to mild anemia was unknown. We investigated the cross-sectional association of mild anemia defined as a hemoglobin level of 10.0–13.9 g/dL with physical fitness in 3,666 military young males in Taiwan in 2014. Aerobic fitness was evaluated by 3000-meter run test, and anaerobic fitness was evaluated by 2-minute sit-ups and 2-minute push-ups, respectively. Multiple logistic regressions for the best 10% and the worst 10% performers were used to determine the relationship. There were 343 mild anemic males in whom 47.8% were microcytic anemia and 3,323 non-anemic males for the analysis. The multiple logistic regression shows that as compared with non-anemic males, mild anemic males were more likely to be the worst 10% performers in the 3000-meter run test (odds ratios (OR) and 95% confidence intervals: 1.47, 1.01–2.14) after adjusting for age, service specialty, body mass index, waist size, mean blood pressure, unhealthy behaviors, lipid profiles, and exercise frequency. On the contrary, mild anemic males had higher possibility to be the best 10% performers in the 2-minute push-ups test (OR: 1.48, 1.08–2.04). However, there was no association between mild anemia and 2-minute sit-ups. Our findings suggest that unspecified mild anemia might be associated with lower cardiorespiratory fitness but not with anaerobic fitness in physically active military males.
Similar content being viewed by others

Introduction
Anemia is characterized by a decrease in the hemoglobin levels or number of red blood cells, consequently leading to the oxygen-carrying capacity of red blood cells insufficient to meet the body’s physiologic needs. The global prevalence of anemia is high, affecting 1.93 billion people which corresponds to 27.0% of the population in 20131. Iron deficiency anemia is the dominant type accounting for more than 50% of the anemic cases1,2. Other important causes of anemia include thalassemia trait, hemoglobinopathies, infections, chronic kidney disease, folate or vitamin B12 deficiency, gastrointestinal and gynecological conditions3,4. Anemia patterns may vary by age and sex3,4,5. For instance, anemia in women is much influenced by their menstruation, and in the elderly, anemia is strongly related to chronic diseases.
People with anemia could have symptoms of weakness, fatigue, poor work productivity or difficulty concentrating. The mechanisms are mainly due to a decreased maximal oxygen uptake6 and diminished oxygen carrying capacity, which is the major cause of reduced exercise capacity as well7,8. Previous reports have revealed that iron deficiency anemia may impair aerobic exercise performance by a reduction in oxygen-transport capacity of blood cells and a decrease in maximal consumption of oxygen peripherally9,10. In addition, iron deficiency anemia could impair mitochondrial respiratory chain activity under certain conditions, thereby limiting exercise capacity11.
Most of the previous studies were carried out to confirm the unfavorable effects of moderate or severe anemia, which are respectively defined as a hemoglobin of 7.0–9.9 g/dL and <7.0 g/dL on cardiorespiratory system12,13. However, the impact of mild anemia, defined as hemoglobin with a lower limit of 10.0 g/dL in men on physical fitness has never been examined before. Therefore, we aimed to investigate the association between mild anemia and physical performance in a large military cohort of young males who are free of chronic diseases and used to receiving regular daily rigorous training.
Methods
Study population
The cardiorespiratory fitness and hospitalization events in armed forces study (CHIEF) includes a historical cohort enrolling 4,080 military men and women ages between 18 and 50 years in Eastern Taiwan in 201414,15,16. All military officers, noncommissioned officers and soldiers in Taiwan are obligated to undertake three exercise tests including 2-minute push-ups, 2-minute sit-ups, and 3000-meter run which are the same as the U.S. Army Physical Fitness Test annually17. All participants received the annual health surveys as well. Since moderate or severe anemia was an exclusion criterion to enlist in the Military, all of the participants had a hemoglobin level ≥10 g/dL14,15,16. Of these 4,080 participants, we excluded all 411 women in whom menstrual cycle affects the hemoglobin levels largely, and 3 men with an unexplained hemoglobin <10 g/dL, leaving a sample of 3,666 men for analysis.
The World Health Organization criteria for anemia in men and women are defined as a hemoglobin <13.0 g/dL and <12.0 g/dL, respectively18. Other criteria for anemia have been proposed the hemoglobin levels, ranging from 13.0 g/dL to 14.2 g/dL for men and 11.6 g/dL to 12.3 g/dL for women19. However, relevant criteria to clarify the value of anemia for young adults are lacking. In this study, mild anemia was defined using a relatively high upper limit of hemoglobin level of 13.9 g/dL to lower limit of a hemoglobin level of 10.0 g/dl for physically active young men and no anemia was defined as a hemoglobin level ≥14 g/dL18,19.
Measurements
All military participants’ annual health examinations were carried out in the Hualien Armed Forces General Hospital of Eastern Taiwan. Each participant self-reported a questionnaire to provide details of personal medical records, including habit of cigarette smoking, alcohol consumption, betel nut chewing (current versus former or never), weekly frequency of more than 30-minutes exercise in leisure time, and medication history in the past 6 months. The annual health examination included: anthropometric measurements of height, weight, and body mass index (BMI) (weight, kg divided by square of height, m2; assessed in a standing position); hemodynamic data of pulse rate and blood pressures measured over right upper arm in a sitting position after a rest for 15 minutes or longer, using the FT-201 automated blood pressure monitor (Parama-Tech Co Ltd, Fukuoka, Japan). Mean blood pressure was defined as a combination of one third of systolic blood pressure level and two thirds of diastolic blood pressure (mmHg); and biochemical data of serum total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, fasting plasma glucose, and triglycerides concentrations analyzed enzymatically on an Olympus AU640 auto analyzer (Olympus, Kobe, Japan). Hematological parameters including white, red, and platelet blood cell counts, and levels of hemoglobin, hematocrit, and mean corpuscular volume of red blood cells were determined by the Sysmex XT- 2000-I automated hematology analyzer. All blood samples were obtained at the same blood drawing station after an overnight 8-hour fast for the participants.
Basic physical fitness tests
The 2-minute push-up test was a measurement of anaerobic fitness superiority. The standardized 2-minute push-up test was performed on a sponge pad and recorded by a computerized monitor. The number of push-ups was scored only when the examinee’s body upward movement returned to the initial resting set level of a line of head, shoulder and buttock, as detected simultaneously by infrared sensors within 2 minutes. However, the push-ups test was aborted immediately upon either elbow or knee touching down on the sponge pad before the time ran out.
The 2-minute sit-up test was another evaluation of anaerobic fitness superiority. The 2-minute sit-up test was also performed in the similar circumstance. The examinee’s feet were fixed by the anchor on the floor with their hands close to the ears. It was scored only when the examinee’s upper body bended forward and elbows touched the electrical sensors on both thighs. If the participants violated the regulation such as the hands deviated to the ears temporarily, the test would be aborted immediately. As for the 3000-meter run, the participants ran on a flat rectangle playground at the Military Physical Training and Testing Center and did not carry any heavy object during the exercise. The test begun outdoor at 4 o’clock in the afternoon uniformly if the risk coefficient of heat stroke less than 40 (the product of outdoor temperature (°C) and relative humidity (%) × 0.1) and without heavy rainy days. All the entire test processes of each participant were recorded by video.
All eligible cases with outcome of interest were evaluated by the three exercise performances. The repetitive numbers of 2-minute push-ups mainly evaluated upper extremity muscle endurance, while the 2-minute sit-ups mainly for the endurance of abdominal muscles and hip flexors. Cardiorespiratory fitness and lower extremity muscle endurance of each participant were estimated by the time finishing a 3000-meter run. This retrospective study was approved by the Institutional Review Board of the Mennonite Christian Hospital (No. 16-05-008) in the Hualien City of Taiwan and written informed consent was obtained from all participants. We confirm that our study was performed in accordance with the 1964 Helsinki declaration and its later amendments.
Statistical analysis
The subject characteristics were presented as mean ± standard deviation (SD) for continuous data, and numbers and percentages for categorical data. The relationship of mild anemia and performance of each exercise (i.e., numbers of 2-minute push-ups, numbers of 2-minute sit-ups and duration of 3000-m non-weight bearing running) were estimated by using analysis of covariance (ANCOVA), and the results were presented as mean ± standard error (SE). The multiple stepwise linear regression of each exercise performance with mild anemia, in reference to no anemia, was also performed. In addition, multiple logistic regression was used to determine the odds ratio (OR) of the superior (highest 10th percentile) and the inferior (lowest 10th percentile) performance in each exercise with mild anemia, in reference to no anemia.
A two-tailed value of p-value < 0.05 was considered significant. In model 1, age and service specialty were adjusted. In model 2, body mass index and waist size were additionally adjusted. In model 3, mean blood pressure, serum total cholesterol, triglycerides, low-density lipoprotein, alcohol intake status, betel nut chewing status, cigarette smoking status, and weekly exercise frequency were further adjusted. These potential confounders were chosen for the models based on prior published associations with physical fitness16 and the presence of a significant difference between the mild anemic and non-anemic groups. Statistical analyses were performed with a standard program (Statistical Package for Social Sciences, SPSS, version 25.0).
Results
Subject characteristics
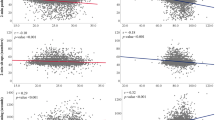
The subject characteristics of each group are shown in Table 1. The mild anemic males had greater red blood cell counts and platelet counts than the non-anemic males. Microcytic anemia (n = 164, 47.8%) accounted for nearly half of the unspecified mild anemia (Fig. 1). In addition, the mild anemic males had lower levels of BMI, waist circumference, mean blood pressure, lipid profiles, and lower prevalence of current cigarettes smoking.

Mean Corpuscular Volume against Hemoglobin Concentrations of 343 Mild Anemic Males.
Group means comparisons
Table 2 shows that there was a significant difference of the 3000-meter running time between the anemic males and the non-anemic males in model 3 (861.88 sec vs. 859.60 sec, p = 0.047). However, there were similar repetitive numbers of the 2-minute push-ups and 2-minute sit-ups between the anemic males and the non-anemic males in models 1–3.
Multiple linear regressions
The results of multiple linear regressions of each exercise performance, with mild anemia relative to no anemia, in models 1–3, shown in Table 3 are in line with the findings of group means comparisons. As compared with no anemia, mild anemia was positively correlated with 3000-meter running time (β = 7.88, p = 0.047) in model 3. However, mild anemia was not correlated with numbers of 2-minute push-ups and 2-minute sit-ups in models 1–3.
Multiple logistic regressions
The results of multiple logistic regressions of the best 10% and the worst 10% performances in each exercise, with mild anemia relative to no anemia, are shown in Table 4. The mild anemic males were more likely to be the best 10% performers in the 2-minute push-ups as compared to the non-anemic males in models 1–3 (OR = 1.68, 1.58, and 1.48, respectively). On the contrary, the mild anemic males had higher possibility of being the worst 10% performers in the 3000-meter run test in model 3 (OR = 1.47). However, mild anemia was not associated with the performances in 2-minute sit-ups in all models.
Discussion
On the basis of our findings, mild anemia might reduce the performance of short-to-medium distance running, a kind of aerobic exercise, but not affect the capacity of anaerobic exercises including short-time sit-ups and push-ups of the military males. In addition, mild anemic males had about 1.50-fold higher odds to be the best 10% performer in the 2-minute push-ups, but in contrast, to be the worst 10% performer in the 3000-meter run test. Our findings extend the concept that not only moderate or severe anemia but also mild anemia may impair the aerobic exercise capacity12,13.
Physiologically, the main function of red blood cells in exercise is to transport oxygen from the lungs to the peripheral tissues and deliver metabolically produced carbon dioxide to the lungs for expiration20. When the level of hemoglobin drops remarkably, the oxygenation of extremity skeletal muscles are reduced, possibly impairing the exercise performance in advance12,13. It has been reported that severe iron deficiency anemia is responsible for a decline in work capacity, particularly in aerobic endurance exercise21,22. Similarly as for anaerobic exercise, oxygen transport is a potent determinant of anaerobic threshold for iron deficiency anemia23. Therefore, anemia has been considered as a negative factor to physical fitness.
Our study shows an association between mild anemia and lower aerobic fitness. This finding confirms the concept that aerobic fitness is positively related to the overall capacity of hemoglobin in red blood cells carrying oxygen in circulation to cardiac and skeletal muscles. In addition, previous studies also reported that several physically active individuals may have anemia due to exercise-induced inflammatory cytokines production, plasma volume expansion, iron deficiency, and intravascular hemolysis from march hemoglobinuria24,25,26. As hemoglobin is consumed by the pathological reactions to overtraining, aerobic fitness could be accordingly reduced as well27,28,29.
On the contrary, mild anemia was not associated with lower anaerobic fitness. This finding could be explained by that the energy expenditure for 2-minute anaerobic exercises is oxygen free, using intramuscular adenosine triphosphate (ATP) and creatinine phosphate as the major fuel in the initial 30 seconds, and then lactate in the last 90 seconds30,31. Therefore, the effect of anemia on carrying oxygen would not be so critical for anaerobic fitness. In addition, the phenotype of elite long-distance runners has been found with muscle mass loss32, possibly reducing the intramuscular ATP and creatinine phosphate amount. In this case, the better aerobically trained individuals who had normal hemoglobin levels might have some impaired anaerobic profiles compared with the mild anemic individuals.
Our study had several strengths. First, all the exercise tests and laboratory examinations were performed in a strict manner and the procedures were standardized. Second, large numbers of military males were enrolled in this study which could provide sufficient power to detect the difference between those with and those without mild anemia. Third, only three male participants were removed from the analysis that the selection bias would be minimized. Fourth, since the daily life of military such as diet consumption and training was unified, many unmeasured confounders had been controlled at baseline. However, there were several limitations in our study. First, the study cohort included merely male subjects, making it difficult to apply the results to the female subjects. Second, the etiology of mild anemia was not fully clarified for the military members. We noticed that about half of the mild anemic males were normocytic and another 50% had a mean corpuscular volume < 80 fL suggesting a high likelihoods of iron deficiency anemia or thalassemia traits3,33. As occult gastrointestinal blood loss could be detected by the stool routine of the annual health examinations, iron deficiency anemia and thalassemia traits could be confirmed as the major types of mild anemia in our subjects. Third, although a number of covariates were adjusted, we could not avoid the existence of other potential confounders that may lead to a bias completely. For instance, the associations between mild anemia and physical fitness were measured merely based on a hemoglobin level from the primary dataset and no follow-up data of hemoglobin could be compared. Fourth, since the military members self-trained at their military bases, the measurement for each exercise performance was not available at baseline. However, these exercise tests are linked to the rank promotion and military award, the performance is regarded as the best physical fitness of each participant.
In conclusion, our findings suggest that unspecified mild anemia might be associated with lower cardiorespiratory fitness but not with anaerobic fitness in physically active military males. Whether the etiology of anemia may have different impacts on the exercise performances needs further investigations.
References
Kassebaum, N. J. & Collaborators, G. B. D. A. The Global Burden of Anemia. Hematol Oncol Clin North Am 30, 247–308 (2016).
Kassebaum, N. J. et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood. 123, 615–624 (2014).
Tefferi, A. Anemia in adults: a contemporary approach to diagnosis. Mayo Clin Proc. 78, 1274–1280 (2003).
Koch, C. G. et al. Hospital-acquired anemia: prevalence, outcomes, and healthcare implications. J Hosp Med. 8, 506–512 (2013).
Patel, K. V. Epidemiology of anemia in older adults. Semin Hematol. 45, 210–217 (2008).
Gledhill, N. The influence of altered blood volume and oxygen transport capacity on aerobic performance. Exerc Sport Sci Rev. 13, 75–93 (1985).
International Conference on Iron deficiency and Behavioral Development. Proceedings. Geneva, October 10-12, 1988. Am J Clin Nutr. 50, 565–705 (1989).
Bassett, D. R. Jr. & Howley, E. T. Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med Sci Sports Exerc. 32, 70–84 (2000).
Wolgemuth, J. C., Latham, M. C., Hall, A., Chesher, A. & Crompton, D. W. Worker productivity and the nutritional status of Kenyan road construction laborers. Am J Clin Nutr. 36, 68–78 (1982).
Willis, W. T., Brooks, G. A., Henderson, S. A. & Dallman, P. R. Effects of iron deficiency and training on mitochondrial enzymes in skeletal muscle. J Appl Physiol (1985). 62, 2442–2446 (1987).
Manios, Y. et al. The double burden of obesity and iron deficiency on children and adolescents in Greece: the Healthy Growth Study. J Hum Nutr Diet. 26, 470–478 (2013).
Weiskopf, R. B. et al. Human cardiovascular and metabolic response to acute, severe isovolemic anemia. JAMA. 279, 217–221 (1998).
Mani, A., Singh, T., Calton, R., Chacko, B. & Cherian, B. Cardiovascular response in anemia. Indian J Pediatr. 72, 297–300 (2005).
Lin, G. M. et al. Rationale and design of the cardiorespiratory fitness and hospitalization events in armed forces study in Eastern Taiwan. World J Cardiol. 8, 464–471 (2016).
Chen, Y. J. et al. Chronic hepatitis B, nonalcoholic steatohepatitis and physical fitness of military males: CHIEF study. World J Gastroenterol. 23, 4587–4594 (2017).
Tsai, K. Z. et al. Association of betel nut chewing with exercise performance in a military male cohort: the CHIEF study. J R Army Med Corps. 164, 399–404 (2018).
O’Connor, J. S., Bahrke, M. S. & Tetu, R. G. 1988 active Army physical fitness survey. Mil Med. 155, 579–585 (1990).
Nutritional anaemias. Report of a WHO scientific group. World Health Organ Tech Rep Ser. 405, 5–37 (1968).
Beutler, E. & Waalen, J. The definition of anemia: what is the lower limit of normal of the blood hemoglobin concentration? Blood. 107, 1747–1750 (2006).
Schumacker, P. T. & Samsel, R. W. Oxygen delivery and uptake by peripheral tissues: physiology and pathophysiology. Crit Care Clin. 5, 255–269 (1989).
Schumacher, Y. O., Schmid, A., Grathwohl, D., Bultermann, D. & Berg, A. Hematological indices and iron status in athletes of various sports and performances. Med Sci Sports Exerc. 34, 869–875 (2002).
Coates, A., Mountjoy, M. & Burr, J. Incidence of Iron Deficiency and Iron Deficient Anemia in Elite Runners and Triathletes. Clin J Sport Med. 27, 493–498 (2017).
Yonezawa, K. Effect of blood hemoglobin concentration on anaerobic threshold. Hokkaido Igaku Zasshi. 66, 458–467 (1991).
Selby, G. B. & Eichner, E. R. Endurance swimming, intravascular hemolysis, anemia, and iron depletion. New perspective on athlete’s anemia. Am J Med. 81, 791–794 (1986).
Sawka, M. N., Convertino, V. A., Eichner, E. R., Schnieder, S. M. & Young, A. J. Blood volume: importance and adaptations to exercise training, environmental stresses, and trauma/sickness. Med Sci Sports Exerc. 32, 332–348 (2000).
Peeling, P., Dawson, B., Goodman, C., Landers, G. & Trinder, D. Athletic induced iron deficiency: new insights into the role of inflammation, cytokines and hormones. Eur J Appl Physiol. 103, 381–391 (2008).
McClung, J. P. et al. Randomized, double-blind, placebo-controlled trial of iron supplementation in female soldiers during military training: effects on iron status, physical performance, and mood. Am J Clin Nutr. 90, 124–131 (2009).
Myhre, K. E. et al. Prevalence and Impact of Anemia on Basic Trainees in the US Air Force. Sports Med Open. 2, 23 (2015).
Epstein, D. et al. Prevalence of Iron Deficiency and Iron Deficiency Anemia in Strenuously Training Male Army Recruits. Acta Haematol. 139, 141–147 (2018).
Messonnier, L. A. Lactate kinetics at the lactate threshold in trained and untrained men. J Appl Physiol (1985). 114, 1593–1602 (2013).
Brooks, G. A. The Science and Translation of Lactate Shuttle Theory. Cell Metab. 27, 757–785 (2018).
Knechtle, B. & Nikolaidis, P. T. Physiology and Pathophysiology in Ultra-Marathon Running. Front Physiol. 9, 634 (2018).
DeLoughery, T. G. Microcytic anemia. N Engl J Med. 371, 1324–1331 (2014).
Acknowledgements
This study was funded by the Hualien Armed Forces General Hospital (grant number 805-C108-19).
Author information
Authors and Affiliations
Contributions
Kun-Zhe Tsai and Shiue-Wei Lai contributed equally to the study; Chin-Sheng Lin, Yen-Po Lin, Sung-Chiao Tsai, Pei-Shou Chung, Yu-Kai Lin, Tzu-Chiao Lin, Ching-Liang Ho, Chih-Lu Han, Younghoon Kwon, and Chung-Bao Hsieh made critical suggestions and revisions on the study; Kun-Zhe Tsai and Chia-Jung Hsieh collected and analyzed the data; Gen-Min Lin conceived, designed and corresponded to the study.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tsai, KZ., Lai, SW., Hsieh, CJ. et al. Association between mild anemia and physical fitness in a military male cohort: The CHIEF study. Sci Rep 9, 11165 (2019). https://doi.org/10.1038/s41598-019-47625-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-47625-3
This article is cited by
-
Co-infection of Plasmodium falciparum and Schistosoma mansoni is associated with anaemia
Malaria Journal (2023)
-
Three-week exercise and protein intake immediately after exercise increases the 6-min walking distance with simultaneously improved plasma volume in patients with chronic cerebrovascular disease: a preliminary prospective study
BMC Sports Science, Medicine and Rehabilitation (2022)
-
Erythrocyte indices and localized stage II/III periodontitis in military young men and women: CHIEF oral health study
BMC Oral Health (2022)
-
Metabolically healthy obesity and physical fitness in military males in the CHIEF study
Scientific Reports (2021)
-
Prevalence and characteristics of mitral valve prolapse in military young adults in Taiwan of the CHIEF Heart Study
Scientific Reports (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
