
Abstract
Identifying the mechanisms behind socioeconomic inequalities in adiposity among youth is vital for efforts aimed at combating these inequalities. The study explored whether a broad range of behavioral and familial factors mediated the associations between parental education and indicators of adiposity among adolescents. Baseline data from a school-based intervention study conducted in 2007 among 11-year-old adolescents were used. Anthropometric outcomes, physical activity and sedentary time among adolescents were objectively measured. Other behavioral variables and parental waist circumference were self-reported. Mediation analyses were conducted. Among boys, maternal waist circumference (WC), paternal WC and TV viewing mediated 16%, 11.5% and 13% of the association between parental education and adolescent WC. The respective proportions when body fat percentage was used as the outcome variable were 22.5%, 16% and 21%. Among girls, maternal and paternal WC mediated 20% and 14% of the association between parental education and WC. The respective proportions when body fat percentage was used as the outcome variable were 14% and 10%. Other included variables did not play any mediating role. Parental WC was found to be a mediator of socioeconomic differences in adiposity in both genders; underlying mechanisms were however not investigated. Among boys, reducing TV time could contribute to the reduction of social inequalities in adiposity.
Similar content being viewed by others


Introduction
In 2016, it was estimated that 50 million girls and 74 million boys worldwide were obese1. The prevalence of overweight (OW)/obesity (OB) among Norwegian youth has similarly been found to be high, with around one in five children being OW or obese2,3,4,5. Some positive trends (i.e. stabilization and even decrease) in the prevalence of childhood OW and OB have been recently documented6. However, there is a need for more public health efforts to reverse the pattern of the OW/OB epidemics. Despite these positive trends, a widening of inequalities in OW and OB was found in around half of the studies included in a recent review6. Such findings are troubling as childhood OW/OB has several well-documented adverse impacts on health7,8,9,10,11; and can be moderately maintained into adulthood12. Inequalities in body weight in childhood can thus lead to or exacerbate inequalities in health in childhood as well as adulthood.
Body weight has multiple levels of influence ranging from individual to broader environmental factors, which often interact13. The most proximal determinants of body weight include energy balance-related behaviors as well as genetic predisposition. If these factors vary by socioeconomic position, they can potentially lead to (or mediate) socioeconomic inequalities in body weight. A mediator represents an intervening variable in the causal pathway between exposure and outcome14. The selection of potential mediators should thus be informed by their previously documented associations with socioeconomic position (exposure) and body weight (outcome). In this regard, sedentary time (ST) has been found to be positively related to OW and OB15,16, although associations have not always been consistent16. Inverse associations between physical activity (PA) and OW/OB among youth have been found17,18. Associations between different dietary behaviors and OW/OB have also been previously documented19,20,21,22. Socioeconomic differences in these energy balance-related behaviors have also been found in different contexts23,24,25. Parental adiposity is an important correlate of child adiposity, reflecting the role of genetic factors as well the shared obesogenic environment26,27,28. Children from a low socioeconomic background are more likely to have parents who are OW/OB than their counterparts with a higher socioeconomic position6,29,30.
Despite the well documented socioeconomic inequalities in body weight among youth6,29,30, in-depth knowledge about the specific factors contributing to these inequalities is however limited. The existing literature is marked by shortcomings including the limited use of formal tests of mediation and paucity of data needed to make firm conclusions (e.g. inclusion of a limited number of potential mediators)31.
Body mass index (BMI) has been the measure of adiposity most commonly used in studies assessing mediators of socioeconomic differences in adiposity among youth31. Existing research suggests that BMI might underestimate socioeconomic differences in childhood obesity compared to other indicators of adiposity32. Other measures such as waist circumference (WC) are found to be more important markers of cardio-metabolic disease risks33,34. However, WC and BMI might be clinically independent markers of cardio-metabolic risk35. Finally, only few previous studies focusing on mediators of socioeconomic inequalities in adiposity have assessed potential gender-related differences31.
In summary, there is a scarcity of studies including a broad range of mediators, using rigorous analytical methods, including measures of adiposity other than BMI and conducting gender-specific analyses. The present study aimed to address these gaps. The aims of the study were to explore whether selected dietary behaviors, objectively measured physical activity and sedentary time, screen-based sedentary behaviors and parental adiposity mediated the associations between parental education and measures of adiposity (WC and body fat percentage) among adolescents. Gender-specific analyses were conducted to explore potential differences between genders.
Methods
Design and sample
Baseline data from a school-based intervention study, the HEalth In Adolescents (HEIA) study were used36.
All schools from the third to fourth largest towns/municipalities in the seven counties surrounding the county of Oslo were invited to participate in the study if they met the study selection criteria (i.e. minimum of 40 enrolled 6th graders). A total of 177 schools were invited and 37 accepted the invitation. All 6th graders (n = 2165) in these 37 schools and their parents/legal guardians were invited to participate in the baseline study in September 2007. Informed consent from parents was obtained for 1589 of the adolescents and 1537 adolescents filled in the baseline questionnaire. Mothers and fathers were also invited to participate in the study; 1260 mothers and 1068 fathers participated.
Informed consent for participation was obtained from school administrators and from the parents of participating children. Adolescents provided assent. The research was carried out in accordance with relevant ethical guidelines and regulations. Ethical clearance was obtained from the Regional Committees for Medical Research in Norway and the Norwegian Social Science Data Service who approved the experimental protocol for the study.
Data collection and measures
The adolescents answered an internet-based questionnaire, assisted as necessary by research assistants. Anthropometric measurements were conducted by research group members. Parents filled in a paper questionnaire sent home via the adolescents.
Measures
Outcome variables: child anthropometrics
Adolescents’ WC was measured to the nearest 0.1 cm. The measuring tape was positioned midway between the lower rib and the iliac crest at the end of a normal expiration. Tanita scales (using bioelectrical impedance analysis) were used to measure body fat percentage (Tanita TBF-300, Tanita Corporation of America, Illinois, USA). The adolescents were measured in light clothing and barefoot.
Exposure variable: parental education
Parental education was gathered as part of the parental informed consent for the adolescent. Educational status of the parent with the longest education or else the one available was used in the analyses. Parental education was initially categorized into three: low (equal to or less than 12 years), medium (university/college (up to 4 years)) and high (university/college (more than 4 years)). However, there were no significant differences between the latter two categories in terms of the associations explored. Thus, these two categories were merged into a “high education” category.
Mediators
The mediators included in this study were: sedentary behaviors (TV/DVD use, computer/electronic game use), dietary behaviors (consumption of fruits, vegetables, unhealthy snacks and sugar-sweetened soft drinks), objectively measured PA and ST, maternal WC and paternal WC.
Four questions with pre-coded answer categories were asked to assess usual TV/DVD and computer/electronic game use: “How many hours do you usually watch TV and/or DVD on a normal weekday?” The same question was asked for a normal weekend day. The six answer categories ranged from half hour per day to five or more hours per day. The two questions on computer/electronic game use were formulated in the same way as for TV/DVD, but the six answer categories ranged from no use to four or more hours per day. Weekly scores for TV/DVD and computer/electronic games were calculated by summing hours reported for an average weekday (multiplied by five) and an average weekend day (multiplied by two).
Consumption of fruit and vegetables (raw and cooked) was assessed by three frequency questions with eight categories ranging from never/seldom to three times per day or more. The questions assessing the intake of fruits and vegetables were validated among 11-year-olds with a 7-day food record as the reference method. They were found to have a satisfactory ability to rank subjects according to their intake of fruits and vegetables37. Frequency of consumption of unhealthy snacks (candies, chocolate, sweet biscuits, buns/muffins and salty snacks (e.g. potato chips)) was assessed using questions with seven categories ranging from never/seldom to two times per day or more. Intake of sugar-sweetened soft drinks (sum of sugar-sweetened carbonated soft drinks and fruit drinks) during weekdays was assessed using two frequency questions with categories ranging from never/seldom to every weekday. Amount was assessed in glass (from one to four or more, with one glass = 1.67 deciliters). The adolescents were also asked the amount of sugar-sweetened soft drinks consumed in the weekends using two questions with categories ranging from never/seldom to 7 glasses or more. Weekday and weekend values were summed up to create a weekly intake variable. The questions assessing the intake of sugar-sweetened soft drinks have been validated among 9- and 13-year-olds using a 4-day pre-coded food diary as the reference method. Moderate correlation coefficients were obtained38.
Adequate test-retest correlation coefficients were obtained for the questions assessing dietary intake and screen-based sedentary behaviors in a separate test-retest study conducted 10–14 days apart among 111 6th graders prior to the main data collection36.
Objectively measured ST and PA were assessed using accelerometers (ActiGraph GT1M/model 7164, LLC, Pensacola, FL, USA). The adolescents were instructed to wear accelerometers for 5 consecutive days, during all waking hours, except when doing water activities (as monitors were not waterproof). ST was defined as activity at intensities less than 100 counts per minute (cpm), which equals the intensity of sitting or lying down (<1.5 MET). Moderate to vigorous physical activity (MVPA) was defined as all activity at intensities above 2000 cpm. This threshold is approximately equivalent to a walking pace of 4 km/h in youth. These cut-offs have been used in previous studies39,40. ST and MVPA were expressed as min/day of accelerometer activity measured. In addition, in order to account for variation in accelerometer wear time, these variables were divided by wear time of the accelerometer (min/day), yielding variables for percent time spent sedentary and percent time spent on MVPA. Details of the instructions provided to students and of the data handling and extraction procedures are available elsewhere41.
Parental WC was reported by parents. A flexible measuring tape was enclosed with the questionnaires sent to parents. Written guidelines (including an illustration) on how to do the measurement were also included.
Potential confounders
Family structure was divided into two categories: those living with two parents versus those with other living arrangements. Participants were divided into either ethnic Norwegian or ethnic minority. Ethnic minorities were defined as those having both parents born in a country other than Norway42.
The Pubertal Development Scale (PDS), based on the pubertal category scores defined by Carskadon and Acebo43, was used to assess pubertal status. The students self-reported this information on a separate paper questionnaire. PDS for boys included body hair growth, voice, and facial hair. For girls, PDS included body hair growth, breast development, and menarche. The categories were: pre-pubertal, early pubertal, mid-pubertal, late pubertal or post-pubertal. For the analyses, dichotomization into pre/early pubertal and mid/late/post-pubertal was made for girls and into pre-pubertal and early/mid/late/post-pubertal for boys. Such categorization was suggested by a study that compared PDS and the Sexual Maturation Scale44.
Statistical analyses
The study aims were first explored using descriptive statistics. Parental educational differences in anthropometric outcomes, potential mediators and potential confounders included were assessed using independent samples t-test for continuous variables and chi-squared test for categorical variables (Table 1). The associations between the potential mediators and the outcome variables (WC and body fat percentage) were explored using regression analyses (Table 2).
Mediation analyses
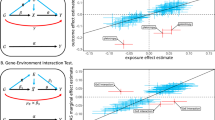
Figure 1 provides an outline of the hypothesized relationships between the exposure variable (parental education), potential mediators (sedentary behaviors, dietary behaviors, objectively measured PA and ST, maternal WC and paternal WC) and outcomes (adolescent WC and body fat percentage). Single mediation analyses were first conducted in which each mediator was separately entered in the analyses. In a single mediation analysis, the a paths represent the association between parental education and the mediator. The b paths represent the association between the mediator and the body weight parameter used as outcome, adjusted for parental education. The c’ path represents the association between parental education and the body weight parameter used as outcome, adjusted for the mediator. The c path represents the total association between parental education and the outcome variable. Since each mediator in the single-mediator models could be associated with omitted mediators (with unknown causal ordering) that might in turn be associated themselves with the outcome or exposure, these single-mediator models were not interpreted causally. Including the mediators jointly would obviate the need to delineate the causal ordering among these mediators under the strong assumption of no-uncontrolled-confounding (especially of the relationship between the mediator-set and the outcome in addition to those of the exposure-mediator set and the exposure-outcome relationships). Therefore, multiple mediation analyses using joint mediator models, in which all mediators were considered as a set in the effect decomposition, were conducted. In the multiple mediation analysis, the a paths represent the association between parental education and the mediators. The b paths represent the association between the mediators and the body weight parameter used as outcome (adjusted for parental education and other mediators). The c’ path represents the association between parental education and the body weight parameter used as outcome when adjusted for the mediators. The c path represents the total association between parental education and the outcome variable. The following potential confounders of the exposure-mediator set, the exposure-outcome, and the mediator-set-outcome relationships were entered as covariates in the model and controlled for in all paths: family structure, ethnicity and pubertal status. However, there was no substantive impact on the results, thus unadjusted models were presented. Bias-corrected and accelerated bootstrap confidence intervals (CI) were calculated for indirect effects (a * b). Bootstrapping (5000 samples) was conducted using the PROCESS macro for SPSS by Andrew Hayes45. The percentage mediated was reported. Assumptions of consistency, positivity, no-uncontrolled confounding and no other sources of bias were made. It was also assumed that there was no measurement error.

Multiple mediation model. ai paths: association between parental education (X) and the mediators (Mi), bi paths: association between the mediators (Mi) and the body weight parameter used as outcome (Y), adjusted for X, confounders (Z) and other mediators; c path: overall association between parental education (X) and outcome variable (Y), adjusted only for Z (total effect); c’ path: association between parental education X) and the outcome variable (Y) used as outcome when adjusted for Mi and Z (direct effect). *Maternal and paternal waist circumferences and TV viewing in boys; maternal and paternal waist circumferences in girls.
Due to missing data on some variables, namely objectively measured ST and PA (1119 adolescents had valid accelerometer data), parental adiposity measures (1260 mothers and 1068 fathers participated in the study), multiple imputation procedures were used. Sensitivity analyses were conducted to compare associations obtained using multiply imputed data and those obtained using complete data.
Results
The mean age of the participants was 11.2 years (SD = 0.3). The majority of adolescents was ethnic Norwegian and lived in two-parent families. Boys and girls with high parental education were more likely to live in two-parent families. Table 1 shows the characteristics of participants and the differences by parental education.
Association between parental education and body weight parameters (c path)
Parental education was inversely related to adolescents’ WC and body fat percentage in both genders (Table 1).
Association between parental education and potential correlates of body weight (a path)
Among girls, parental education was inversely related to the intake of sugar-sweetened soft drinks and unhealthy snacks. It was also inversely related to paternal and maternal WC. Among boys, parental education was inversely related to TV viewing, computer use, sugar-sweetened soft drink intake, unhealthy snack intake, maternal WC and paternal WC. There were no significant associations between the other potential mediators included and parental education (Table 1).
Association between potential correlates and body weight parameters (b path)
Table 2 shows the results of the linear regression analyses exploring the association between potential correlates and weight parameters (adjusted for parental education).
Among girls, daily sedentary time, percent time spent sedentary, maternal WC and paternal WC were positively related to WC and body fat percentage. MVPA (daily time and percent time) was inversely related to WC and body fat percentage.
Among boys, TV viewing, computer use, maternal WC and paternal WC were positively related to WC and body fat percentage. Percent time spent sedentary was also positively related to body fat percentage. Daily MVPA time and percent time spent on MVPA were inversely related to WC and body fat percentage.
Mediation analyses
Single mediation analyses (results not shown) found that the factors that mediated the association between parental education and both WC and body fat percentage were: paternal and maternal WC among girls, maternal WC, paternal WC and TV viewing among boys. The other factors were not found to be significant mediators in the single mediation analyses.
In the multiple mediation model among girls, maternal WC and paternal WC mediated 20% and 14% percent of the association between parental education and WC respectively. The respective proportions when body fat percentage was used as the outcome variable were 14% and 10%. Among boys, maternal WC, paternal WC and TV viewing mediated 16%, 11.5% and 13% of the association between parental education and WC. The respective proportions when body fat percentage was used as the outcome variable were 22.5%, 16% and 21% (Table 3).
Among girls, these mediators together mediated 33% of the association between parental education and WC; they mediated 24% of the association between parental education and body fat percentage. Among boys, the respective proportions were 40.5% and 59.5% (Table 3).
Missing data
Sensitivity analyses comparing associations obtained using imputed data and available data showed no substantive differences.
Discussion
In order to inform interventions aimed at reducing social inequalities in OW and OB among youth, it is vital to identify the mechanisms behind these inequalities. In the present study, parental WC was found to mediate parental educational differences in adolescent WC and body fat percentage in both genders. Parental BMI has previously been found to mediate inequalities in adiposity among youth31; this is in line with the findings for parental WC in the present study. These findings indicate the potential for a multigenerational “transmission” of socioeconomic differences in adiposity. The association between parental weight and child weight is itself multi-causal. It involves biological mechanisms as well as factors related to common environmental exposures, occurring in a complex gene-environment interaction context26,27,28. More studies are needed to shed light on the relative role of biological vs social/environmental factors in explaining the association between parental weight and child weight, as was also suggested in a recent review28. Dissociating the role of biological factors vs modifiable behavioral or environmental factors is vital for the planning as well as the timing of interventions.
TV viewing time was found to be a mediator of parental educational differences in WC and body fat percentage in boys but not in girls. Although the role of TV viewing as a mediator of socioeconomic differences in adiposity has previously been documented31, gender-specific differences in this regard have been less explored. TV viewing was not associated with WC and body fat percentage among girls in the present study. The association between TV viewing and body weight can be related to dietary behaviors, via mechanisms such as exposure to advertisement and passive overconsumption of foods46. Differences in dietary behaviors not included in this study that are related to TV viewing might thus at least partly explain the differences between genders. The findings suggest that efforts aimed at reducing screen time among boys could result in the reduction of socioeconomic differences in adiposity. Reducing screen time among youth can be a challenging task, in particular among those with low socioeconomic position (SEP). Increased screen time in this latter subgroup has been found to be related to factors such as parental time demands, concern about neighborhood safety or absence of alternative activities to TV viewing23. Carefully tailored interventions making use of existing knowledge about important determinants of TV viewing are thus needed.
The consumption of sugar-sweetened beverages has previously been found to mediate socioeconomic differences in adiposity31; this was not the case in the present study. The consumption of sugar-sweetened beverages was inversely related to parental education as also previously found in the literature47. However, it was not related to WC or body fat percentage. This might partly be due to differences in the type of sugar-sweetened beverages included in different studies. The reported intake of sugar-sweetened beverages in the current sample was also low. There has been an increasing awareness at the population level about the association between sugar-sweetened beverages and health. It is thus possible that there was some social desirability bias with underreporting of intake, in particular among those who were overweight/obese.
The intake of fruits and vegetables was not related to parental education; these findings are in line with those of a nationally representative survey among adolescents48. There was also no association between the intake of fruits and vegetables and WC as well as body fat percentage. A previous review found that there is indeterminate evidence for the mediating role of fruit and vegetable intake in the association between parental SEP and overweight/obesity31.
No mediating role of objectively measured PA and ST was found in this study, as these were not related to parental education. The present study contributes to the limited literature in this area which has often been based on self-reported measures of PA and SB31. In early adolescence, the main volume of PA is likely to be mainly non-structured/informal, as previously documented in the literature49. It may be that socioeconomic differences emerge later in adolescence when organized activities that might require more resources become more frequent. This hypothesis has previously also been used to explain the results of a systematic review which documented socioeconomic differences in PA levels among adolescents while such differences were not found among children (3–12 years of age)50. No parental educational differences in total ST were documented, although such differences were found for TV viewing and computer time. This suggests that it is the type of ST that varies by parental education and not the amount.
Higher proportions of the parental educational inequalities in adiposity were explained in boys than girls. In one of the few studies assessing gender-specific mediators of socioeconomic differences in adiposity among youth, similar findings were documented51. A substantial proportion of the parental educational differences in adiposity remain unexplained. This was particularly true for girls among whom only 24–33% of the association between parental education and indicators of adiposity was explained. Therefore, other mediators need to be assessed in future studies. These include factors such as a broader range of dietary behaviors, total energy intake, sleep patterns and meal patterns. Obesity is multi-causal and has multiple levels of influence; exploring the role of broader environmental factors including the availability and accessibility of opportunities for healthy lifestyle choices is warranted. Targeting such environmental factors can potentially lead to wide-reaching effects.
Strengths and Limitations
The strengths of the study include the broad range of potential mediators included, and the objective measurement of PA, ST and anthropometric outcomes. The use of indicators of adiposity other than BMI is also a strength of the study. Gender-specific analyses were conducted, contributing to the limited evidence in this regard. Formal tests of mediation were also conducted.
However, the study should be seen in light of the following weaknesses. The cross-sectional design limits inferences about causality. However, the association between parental education and child adiposity is likely to be unilateral among youth (i.e. parental SEP affects child adiposity and not vice versa). The measurement of body fat percentage in the present study did not follow recommended procedures as the students were not in a fasting state when measurements were made. The use of self-reported measures raises validity and reliability concerns, in particular among youth. However, measures used in this study are supported by evidence of adequate test-retest reliability. Assessing dietary intake using frequency measures only can be considered to be a limitation of this study. However, the measures (except the one assessing the intake of unhealthy snacks) have previously been validated using a 7 day food record or a pre-coded food diary. Results showed that increasing frequency of intake was related to increasing amount consumed37,38. Self-reported measures of weight circumference can lead to underestimation; subgroup differences in this underestimation might also exist52,53,54. Such errors can affect the documented associations. Some screen-based sedentary behaviors which are increasingly prevalent among youth (e.g. use of mobile devices) were not included in the present study. Future studies should include such measures. On the other hand, measures such as the use of DVDs, which was included in this study, are unlikely to be relevant for contemporary youth.
Parental education was the only indicator of SEP included in this study. Education has been found to be the indicator of SEP most commonly related to body weight among youth55. It is considered to be a good measure of SEP because it might reflect both resources and knowledge affecting behaviors and is stable over time. There are associations between education and other indicators of SEP such as income and occupation in Norway56. Although education, income and occupation are correlated, existing research suggests that the associations between these indicators of SEP and dietary behaviors among children might be specific/independent57. Therefore, future studies should include different indicators of SEP.
Finally, future studies should include other potential mediators in order to better shed light on the mechanisms explaining socioeconomic differences in adiposity among youth.
Conclusion
Parental WC was found to be a mediator of socioeconomic differences in adiposity in both genders. Identifying the underlying mechanisms behind this mediating role of parental adiposity is important from an intervention perspective. Dissecting the possible role of genetic factors as well as shared social and environmental factors in the association between parental weight and child weight is vital in this regard. Furthermore, reducing time spent watching TV, in particular among those with low parental education, could contribute to reducing social inequalities in adiposity among boys. The study, using objective measures, also found that PA and sedentary time do not play a role in explaining socioeconomic differences in adiposity in the study setting. A significant percentage of the association between parental education and adiposity among the adolescents remained unexplained. Thus, future studies including other potential mediators are warranted.
Data Availability
The datasets analysed during the current study are available from the corresponding author on reasonable request.
References
NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet. 390, 2627–2642 (2017).
Oellingrath, I. M. & Svendsen, M. V. BMI-specific associations between health-related behaviours and overweight - a longitudinal study among Norwegian adolescents. Public Health Nutr. 20, 481–491 (2017).
Júlíusson, P. B. et al. Overweight and obesity in Norwegian children: prevalence and socio-demographic risk factors. Acta Paediatr. 99, 900–5 (2010).
Hovengen, R. & Strand, B.H. Barns vekst i Norge - resultater 2010. [Children’s growth in Norway - Results from 2010. In Norwegian]. Nasjonalt folkehelseinstitutt (2011).
Helsedirektoratet. Fysisk aktivitet blant 6-, 9- og 15-åringer i Norge. Resultater fra en kartlegging i 2011. [Physical activity among 6 -, 9 - and 15-year-olds in Norway. Results from a survey in 2011. In Norwegian]. Oslo: Helsedirektoratet (2012).
Chung, A. et al. Trends in child and adolescent obesity prevalence in economically advanced countries according to socioeconomic position: a systematic review. Obes Rev. 17, 276–95 (2016).
Deckelbaum, R. J. & Williams, C. L. Childhood obesity: the health issue. Obes Res. 9(Suppl 4), 239S–243S (2001).
Daniels, S. R. et al. Overweight in children and adolescents: pathophysiology, consequences, prevention, and treatment. Circulation. 111, 1999–2012 (2005).
Lobstein, T. & Jackson-Leach, R. Estimated burden of paediatric obesity and co-morbidities in Europe. Part 2. Numbers of children with indicators of obesity-related disease. Int J Pediatr Obes. 1, 33–41 (2006).
Biro, F. M. & Wien, M. Childhood obesity and adult morbidities. Am J Clin Nutr. 91, 1499S–1505S (2010).
Reilly, J. J. & Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes (Lond). 35, 891–8 (2011).
Singh, A. S., Mulder, C., Twisk, J. W., van Mechelen, W. & Chinapaw, M. J. Tracking of childhood overweight into adulthood: a systematic review of the literature. Obes Rev. 9, 474–88 (2008).
Swinburn, B. A. et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet. 378, 804–14 (2011).
Pearl, J. Causality: Models, Reasoning and Inference. (Cambridge University Press, Cambridge, 2000).
Carson, V. et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: an update. Appl Physiol Nutr Metab. 4, S240–65 (2016).
Biddle, S. J., García Bengoechea, E. & Wiesner, G. Sedentary behaviour and adiposity in youth: a systematic review of reviews and analysis of causality. Int J Behav Nutr Phys Act. 14, 43 (2017).
Steinbeck, K. S. The importance of physical activity in the prevention of overweight and obesity in childhood: a review and an opinion. Obes Rev. 2, 117–30 (2001).
Janssen, I. & Leblanc, A. G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act. 7, 40 (2010).
Vartanian, L. R., Schwartz, M. B. & Brownell, K. D. Effects of soft drink consumption on nutrition and health: a systematic review and meta-analysis. Am J Public Health. 97, 667–75 (2007).
Must, A., Barish, E. E. & Bandini, L. G. Modifiable risk factors in relation to changes in BMI and fatness: what have we learned from prospective studies of school-aged children? Int J Obes. 33, 705–15 (2009).
Swinburn, B. A., Caterson, I., Seidell, J. C. & James, W. P. Diet, nutrition and the prevention of excess weight gain and obesity. Public Health Nutr. 7, 123–46 (2004).
Drewnowski, A., Almiron-Roig, E., Marmonier, C. & Lluch, A. Dietary energy density and body weight: is there a relationship? Nutr Rev. 62, 403–13 (2004).
Gebremariam, M. K. et al. Associations between socioeconomic position and correlates of sedentary behaviour among youth: a systematic review. Obes Rev. 16, 988–1000 (2015).
Zarnowiecki, D. M., Dollman, J. & Parletta, N. Associations between predictors of children’s dietary intake and socioeconomic position: a systematic review of the literature. Obes Rev. 15, 375–91 (2014).
Stalsberg, R. & Pedersen, A. V. Effects of socioeconomic status on the physical activity in adolescents: a systematic review of the evidence. Scand J Med Sci Sports. 20, 368–83 (2010).
Pate, R. R. et al. Factors associated with development of excessive fatness in children and adolescents: a review of prospective studies. Obes Rev. 14, 645–58 (2013).
Thompson, A. L. Intergenerational impact of maternal obesity and postnatal feeding practices on pediatric obesity. Nutr Rev. 71(Suppl 1), S55–61 (2013).
Wang, Y., Min, J., Khuri, J. & Li, M. A. Systematic Examination of the Association between Parental and Child Obesity across Countries. Adv Nutr. 8, 436–448 (2017).
Shrewsbury, V. & Wardle, J. Socioeconomic status and adiposity in childhood: a systematic review of cross-sectional studies 1990–2005. Obesity (Silver Spring). 16, 275–84 (2008).
Barriuso, L. et al. Socioeconomic position and childhood adolescent weight status in rich countries: a systematic review, 1990–2013. BMC Pediatrics 15, 129 (2015).
Gebremariam, M. K., Lien, N., Nianogo, R. A. & Arah, O. A. Mediators of socioeconomic differences in adiposity among youth: a systematic review. Obes Rev. 18, 880–898 (2017).
van den Berg, G., van Eijsden, M., Vrijkotte, T. G. & Gemke, R. J. BMI may underestimate the socioeconomic gradient in true obesity. Pediatr Obes. 8, e37–40 (2013).
McCarthy, H. D. Body fat measurements in children as predictors for the metabolic syndrome: focus on waist circumference. Proc Nutr Soc. 65, 385–92 (2006).
Savva, S. C. et al. Waist circumference and waist-to-height ratio are better predictors of cardiovascular disease risk factors in children than body mass index. Int J Obes Relat Metab Disord. 24, 1453–8 (2000).
Wicklow, B. A. et al. Comparison of anthropometric measurements in children to predict metabolic syndrome in adolescence: analysis of prospective cohort data. Int J Obes (Lond). 39, 1070–8 (2015).
Lien, N. et al. Design of a 20-month comprehensive, multicomponent school-based randomised trial to promote healthy weight development among 11-13 year olds: The HEalth In Adolescents study. Scand J Public Health. 38, 38–51 (2010).
Haraldsdóttir, J. et al. Validity and reproducibility of a precoded questionnaire to assess fruit and vegetable intake in European 11- to 12-year-old schoolchildren. Ann Nutr Metab. 49, 221–227 (2005).
Lillegaard, I. T., Overby, N. C. & Andersen, L. F. Evaluation of a short food frequency questionnaire used among Norwegian children. Food Nutr Res. 56 (2012).
Kolle, E., Steene-Johannessen, J., Andersen, L. B. & Anderssen, S. A. Objectively assessed physical activity and aerobic fitness in a population-based sample of Norwegian 9- and 15-year-olds. Scand J Med Sci Sports 20, 41–47 (2010).
Ekelund, U. et al. Associations between objectively assessed physical activity and indicators of body fatness in 9- to 10-y-old European children: a population-based study from 4 distinct regions in Europe (the European Youth Heart Study). Am J Clin Nutr 80, 584–590 (2004).
Bergh, I. H. et al. Personal and social-environmental correlates of objectively measured physical activity in Norwegian pre-adolescent children. Scand J Med Sci Sports. 21, e315–24 (2011).
Lie, B. Immigration and immigrants: Statistisk Sentralbyrå. Oslo: Statistics Norway (2002).
Carskadon, M. A. & Acebo, C. A self-administered rating scale for pubertal development. J Adolesc Health. 14, 190–5 (1993).
Bond, L. et al. A comparison of self-reported puberty using the Pubertal Development Scale and the Sexual Maturation Scale in a school-based epidemiologic survey. J Adolesc. 29, 709–20 (2006).
Preacher, K. J. & Hayes, A. F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 40, 879–91 (2008).
Hobbs, M., Pearson, N., Foster, P. J. & Biddle, S. J. Sedentary behaviour and diet across the lifespan: an updated systematic review. Br J Sports Med. 49, 1179–88 (2015).
Naska, A., Bountziouka, V. & Trichopoulou, A., DAFNE Participants. Soft drinks: time trends and correlates in twenty-four European countries. A cross-national study using the DAFNE (Data Food Networking) databank. Public Health Nutr. 13, 1346–55 (2010).
Hansen, L., Myhre, J. B., Johansen, A. M. W., Paulsen, M. M. & Andersen, L. F. UNGKOST 3 Landsomfattende kostholdsundersøkelse blant elever i 4. -og 8. klasse i Norge, 2015. Helsedirektoratet. Oslo: Folkehelseninstituttet (2015).
Mota, J. & Esculcas, C. Leisure-time physical activity behavior: structured and unstructured choices according to sex, age, and level of physical activity. Int J Behav Med. 9, 111–21 (2002).
Ferreira, I. et al. Environmental correlates of physical activity in youth - a review and update. Obes Rev. 8, 129–54 (2007).
Dollman, J., Ridley, K., Magarey, A., Martin, M. & Hemphill, E. Dietary intake, physical activity and TV viewing as mediators of the association of socioeconomic status with body composition: a cross-sectional analysis of Australian youth. Int J Obes (Lond). 31, 45–52 (2007).
Bigaard, J., Spanggaard, I., Thomsen, B. L., Overvad, K. & Tjonneland, A. Selfreported and technician-measured waist circumferences differ in middleaged men and women. J Nutr. 135, 2263–70 (2005).
Dekkers, J. C., van Wier, M. F., Hendriksen, I. J. & Twisk, J. W. & van Mechelen, W. Accuracy of self-reported body weight, height and waist circumference in a Dutch overweight working population. BMC Med Res Methodol. 8, 69 (2008).
Cullum, A. et al. Dietary restraint and the mis-reporting of anthropometric measures by middle-aged adults. Int J Obes Relat Metab Disord. 28, 426–33 (2004).
Barriuso, L. et al. Socioeconomic position and childhood-adolescent weight status in rich countries: a systematic review, 1990–2013. BMC Pediatr. 15, 129 (2015).
Råberg Kjøllesdal, M. K., Holmboe-Ottesen, G. & Wandel, M. Associations between food patterns, socioeconomic position and working situation among adult, working women and men in Oslo. Eur J Clin Nutr. 64, 1150–7 (2010).
Zarnowiecki, D., Ball, K., Parletta, N. & Dollman, J. Describing socioeconomic gradients in children’s diets - does the socioeconomic indicator used matter? Int J Behav Nutr Phys Act. 11, 44 (2014).
Acknowledgements
We would like to thank all the participants who took part in this study, the project staff, and the Principal Investigator, Professor Knut-Inge Klepp for planning and designing the overall HEIA study. The research leading to these results has received funding from the European Union Seventh Framework Programme (FP7-PEOPLE-2013-COFUND) under grant agreement no. 609020 - Scientia Fellows. The HEIA study was funded by the Norwegian Research Council with supplementary funds from the Throne Holst Nutrition Research Foundation, the University of Oslo and the Norwegian School of Sport Sciences.
Author information
Authors and Affiliations
Contributions
M.K.G., N.L. and O.A.A. conceived the study. M.K.G. conducted the statistical analyses and wrote the first draft of the manuscript. N.L., L.F.A., I.H.B., M.B., M.G. and Y.O. participated in the design, project planning and data collection of the HEIA study. T.H.T. participated in data preparation. All authors provided feedbacks on different versions of the manuscript and approved the final version submitted for publication.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gebremariam, M.K., Arah, O.A., Bergh, I.H. et al. Gender-specific mediators of the association between parental education and adiposity among adolescents: the HEIA study. Sci Rep 9, 7282 (2019). https://doi.org/10.1038/s41598-019-43604-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-43604-w
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
