
Abstract
Assessing movement over 24 hours increases our understanding of the total physical activity level and its patterns. In the FinHealth 2017 Survey, a population-based health examination study, 940 participants between 25 and 93 years were instructed to wear an accelerometer (Actigraph GT9X Link) on their non-dominant wrist for 24 hours on 7 consecutive days. Physical activity information was extracted from 100-Hz triaxial 60-second epoch data as average vector magnitude counts per minute (VM cpm). Results were analyzed by gender, 10-year age-groups, employment status, and education. Hourly means were plotted and compared. Analyses included 915 participants (44% men) who wore the device at least 10 hours on 4 or more days, with mean wear time being 149.5 hours (standard deviation of 615.2 minutes).Women had higher average VM cpm than men (p < 0.001), with significant gender differences in all age-groups until 65 years and older. Total physical activity was lower with age, unemployment, and retirement, where the hourly patterns mirrored the findings. Our findings agree with previous large-scale wrist-accelerometry data, but extend current knowledge by providing data on gender and socioeconomic variation in physical activity across 24 hours in a population-based adult sample representing a broad age range.
Similar content being viewed by others

Introduction
Physical activity can be considered as the accumulation of movement throughout the day, independent of type, location or purpose1. Technical development of accelerometers has facilitated an assessment of people’s 24 hour movement pattern and physical activity level during everyday life, also in large-scale population cohorts. Wrist-worn accelerometers have become increasingly popular for assessment of physical activity over 24 hours since they have shown good wear compliance2,3. Wrist-accelerometry has long been used within sleep research to estimate sleep duration, sleep efficiency, and the circadian rest-activity rhythm, often in clinical samples4. Many large-scale studies with adult populations have now incorporated wrist-accelerometry in their protocols, such as for example the UK Biobank2, the Whitehall II Study5, the NHANES 2011-20123, the Rotterdam Study6, and Pelotas birth cohorts7.
Only few studies have yet described the 24-hour physical activity levels in a general adult population. Results from the UK Biobank study2 are among the most extensive so far; showing hourly, daily and seasonal variation of activity among adults (aged 45 to 79 years). In Finland, Husu et al.8 examined daytime physical activity and the times spent in different intensities of physical activity among adults (aged 18 to 85 years) using hip-worn accelerometers. According to the results, men were more sedentary than women, and younger adults had more moderate-to-high intensity physical activity compared to older ones8. Wrist-worn accelerometers produce substantially higher output as compared to hip-worn or waist-worn accelerometers9,10,11. To date, there is yet no consensus on the best method or criteria for detecting the type or the intensity of physical activity from the wrist-worn accelerometer data10,12. Hip-worn and wrist-worn accelerometer outputs correlate positively, and wrist-worn accelerometers have proven feasible in assessing total physical activity level9,11,13. In general, very simple summary measures such as total, median or mean activity counts or activity related acceleration per day, can be used to describe the overall physical activity level2,10,14,15. Furthermore, describing the accumulation of physical activity and the daily physical activity pattern over 24 hours enable visualization of data and better understanding of the amount of activity performed by more sedentary subgroups; minimizing a potential loss of information related with cut-points16.
To contribute to the current gap of knowledge to describe and define 24-hour physical activity and wrist-accelerometry at the general adult population, our aim is to examine the total physical activity levels and hourly activity patterns assessed by wrist-worn accelerometers among adults in Finland. We aim to study the variation by gender, age, employment and education.
Material and Methods
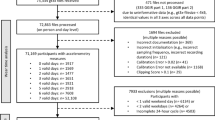
Data comprise the FinHealth 2017 Survey, a population-based health examination study conducted in 2017. The FinHealth 2017 Survey protocol is described in detail elsewhere17. Briefly, 10000 adults over 18-years of age living in Finland were invited to participate by two-stage cluster sampling from the population register. The study included questionnaires and a health examination where measurements on body composition, blood pressure, functional capacity and blood sampling were undertaken. Out of the initial cohort, 2000 persons aged 25 or more were randomized into a “Physical activity and sleep” sub-study. Totally 1140 subjects (57%) of the sub-study participated in the health-examination where accelerometers were offered to participants as a part of the measurements. The participation into the device-based measurements of physical activity is described in a flow chart below (Fig. 1). The FinHealth 2017 Survey was approved by the Coordinating Ethics Committee for the Helsinki-Uusimaa hospital district. A written informed consent was obtained from all participants. All methods were performed in accordance with the relevant guidelines and regulations.

Flow chart of participation in the accelerometer sub-study.
Accelerometer measurements
At the health examination site, participants belonging to the “Physical activity and sleep” sub-study were given a triaxial wrist-worn accelerometer (Actigraph GT9X Link, Actigraphcorp, Pensacola, USA) and advised on the use of it by trained nurses. Accelerometers were initialized to collect acceleration data on three axes at 100 Hz sampling rate. The accelerometers were worn on the non-dominant wrist for 7 days, beginning from the visit at the health examination. Accelerometers were instructed to be removed only if entering sauna or swimming. Participants were asked to keep a diary to mark their bedtimes and possible non-wear periods. On the 7th morning of measurements subjects could take the accelerometer off and they were told to return the device and the diary to the National Institute for Health and Welfare by prepaid mail.
Subjects who visited the health examination but for whom there were no accelerometers available at site (n = 257), were contacted afterwards by phone and offered an accelerometer. Those who agreed to take a device were mailed an accelerometer and a diary, together with written instructions for the measurements. These subjects were instructed to start wearing the device when receiving it and to end the measurements at the 7th morning and return the device and the diary to the National Institute for Health and Welfare by prepaid mail.
Totally 776 persons were given an accelerometer in person at the health examination site and 164 persons received an accelerometer together with written instructions by mail (Fig. 1). Out of 940 initialized accelerometer measurements, 933 devices were returned. The diary was returned by 918 participants.
Accelerometer data processing
Accelerometer data processing was done using the Actilife software version 6.13.3 (Actigraphcorp, Pensacola, USA) using vector magnitude (VM) counts in 60 second epoch data, i.e., counts per minute (cpm). The VM is calculated as the square root of the sum of the squared counts in three (x, y, z) axis.
As a first step, the Cole-Kripke algorithm was applied to score every 60 s epoch as asleep or awake, and the modified Tudor-Locke algorithm was applied to identify sleep periods18,19,20. Briefly, the Tudor-Locke algorithm makes use of the result by the Cole-Kripke algorithm and it determines the in-bedtime where first 5 consecutive minutes asleep are identified. Thereafter the algorithm identifies wake time as the time point where 10 consecutive minutes of awake are observed in the data following a bedtime. The minimum time between bedtime and wake time must be at least 160 minutes and the maximum length of the sleep period cannot exceed 1440 minutes.
After automatic identification of sleep periods the data were checked against the diary information for the number of sleep periods. If data included more sleep periods as compared to the diary and if the sleep periods were separated by less than 4 hours, the periods were either united or the extra sleep periods were removed depending on the notes in the diary. Furthermore, sleep data were also checked against self-reported non-wear times for potential overlapping in case of which the false sleep-period was removed. Sleep times per se were not altered.
After the detection of sleep periods the data were analyzed for non-wear by applying the Choi et al. algorithm to the VM data21,22. The algorithm checks the data for 90 consecutive minutes of zero VM counts, allowing for up to 2 minutes of non-zero counts, using a floating 30 minute window. For this non-wear checking process sleep-periods were marked as wear-time to avoid misclassification as non-wear. Finally, the 60 s epoch data files without non-wear periods were exported as VM cpm into csv-format for further analyses in external statistical software. Participants with minimum of 4 days including 10 hours of wear time from midnight-to-midnight were included in current analyses (n = 915).
Sociodemographic factors
Information about employment status and education were assessed on a health questionnaire. Employment status was grouped into working (full-time or part-time), unemployed, retired, student, and other (including family leave and stay-at-home mothers/fathers). Education was defined as low, mid or high, according to completed educational years standardized by birth cohort. To explore levels and hourly patterns of physical activity the participants were divided into strata by gender and 10-year age-groups (25–34; 35– 44; 45–54; 55–64; 65–74; and 75+). Hourly patterns were also studied by weekday.
Statistical methods
Differences in basic characteristics and the average VM cpm between genders were studied by t-test and between age-, employment- and education groups by analysis of variance (ANOVA). The employment- and education group comparisons were adjusted for age and gender. The average VM cpm were plotted by hour over 24-hours and the means between two consecutive hours by gender and age-group were compared by Wilcoxon signed-rank test for related samples with Bonferroni correction for multiple tests. All statistical analyses were conducted using SAS 9.3 (SAS Institute Inc, Cary, NC).
Results
Those who returned the accelerometer (n = 933) were more often women (56% vs. 47%) and not as often aged 25–34 (13% vs. 18%) or above 85-years (3% vs. 10%), compared to the rest of the sub-study sample (n = 1067, including those who did not attend the health examination, those who did not receive an accelerometer and those who did not return the device). Descriptive characteristics, the mean wear time in minutes and number of valid days for included participants are shown by gender in Table 1. Women accumulated higher average VM cpm than men (Table 1). No statistically significant differences between genders in wear time or number of valid days was observed.
Gender differences in average VM cpm were significant in all age-groups except the oldest two (Table 2). Within both genders there were significant differences between age-groups in the average VM cpm, with lower values in the older age-groups of 65 −74 and 75+ years than in the three youngest age-groups.
In Fig. 2 the variation in physical activity over 24 hours by gender and age-groups is presented. In general, a low activity level at night (between 1 a.m. and 4 a.m.), a considerable rise in activity level during morning hours (around 5 and 6 a.m.) (Supplementary Table S1), a higher activity level during daytime hours and a more or less pronounced drop in activity level towards evening hours (around 8 p.m.) were observed (Fig. 2).

Hourly pattern of physical activity by age-group and gender. Upper figure men, lower figure women.
Differences in average daily VM cpm by age-groups are mirrored in the different hourly patterns between age groups. In the oldest participants the VM cpm level of two consecutive hours showed few significant differences while in younger men and women several consecutive hours in the morning and in the evening differed between each other (Supplementary Table S1). In youngest women and two oldest groups in both genders, changes in activity level from one hour to another were significant from the 5th and 6th hour until the 8th hour. In women aged 35-44 and men and women 45-64 years the rise in activity level was significant between consecutive hours from the 5th and 6th hour until the 9th or 10th hour (Supplementary Table S1). In men, the youngest age group reached their highest activity levels in the later afternoon hours (after 16th hour) whereas the peak levels in other age groups occurred earlier in the day, particularly for the oldest two age-groups Also in women, the youngest reached their highest activity levels in late afternoon hours (Fig. 2 and Supplementary Table S1), whereas in the two oldest age-groups the hours with highest average VM cpm were observed before noon. In women, all ages had a peak in activity in the morning hours and in the youngest three age-groups a second peak was observed around 6 p.m. in late afternoon.
The hourly patterns of activity were different between weekdays (Fig. 3). In both genders the weekend days (Saturday and Sunday) showed a different hourly pattern as compared to the other weekdays (Monday through Friday) which all were very similar to each other. In men, there was a clearly higher peak in activity level during Saturdays than on any other weekdays. Also in women, higher activity levels were observed on Saturdays, but also on Sundays. The comparisons of VM cpm between consecutive hours showed that the change in activity level from one hour to the next were mostly significant only in early morning and late evening hours on all days of the week. For both genders, the activity level on weekend mornings before 9 a.m. was clearly lower as compared to the rest of the weekdays (Fig. 3 and Supplementary Table S2).

Hourly pattern of physical activity by weekday. Upper figure men, lower figure women.
Significant differences in physical activity levels were also observed for employment status, but not educational level (Table 3). Students and the retired had the lowest average VM cpm, when adjusted for age and gender. The group of others showed the highest average VM cpm of all employment groups. The retired and the unemployed showed one clear peak in activity level in the morning hours, followed by a tapering towards evening hours (Fig. 4). The employed sustained their activity level throughout daytime whereas students had the slowest rise in activity level during morning hours with the peak in activity occurring in the early evening.

Hourly patterns of physical activity by employment status (upper figure) and education (lower figure).
Discussion
We observed that women had higher average VM cpm than men in all except the oldest two age-groups. An inverse association between age and average VM cpm was observed within genders. The hourly patterns of activity were different between age-groups and weekdays, as well as employment status. The oldest had the lowest level of activity throughout the day and the hourly pattern in students was opposite to other employment groups with activity level rising towards evening hours. Furthermore, in both men and women, the hourly activity patterns on Saturday and Sunday were different from the other weekdays.
Even if only few results regarding physical activity based on 24-hour accelerometer-based data are available from large population-based cohorts, the gender differences in activity level have already been observed by others as well. In one of the largest studies applying wrist-accelerometry, the UK Biobank study, women had higher mean acceleration values as compared to men, except in those aged 45 to 54-years2. Men had lower physical activity level that tended to decline more by age, as compared to women. In three different Brazilian birth cohorts, women gender and low socioeconomic status where associated with higher physical activity as measured by wrist-worn accelerometers7. However, similar to our finding, there are some other studies that have applied wrist-worn devices in adults aged 60 years or older and not observed any differences between genders5,23.
Based on questionnaire data, women engage more in household activities than men24, which could be a reason for differences in the observed wrist-accelerometer output between genders. According to Shiroma et al.10 the hip-worn and the wrist-worn monitors may be engaged in somewhat different behaviors during the course of the day. Where the hip-worn devices may assess the whole-body movements, the wrist-worn devices measure most of the whole-body movements in addition to the movements being specific to wrist- or upper body. Furthermore, a wrist-worn accelerometer reaches 25% of total daily activity earlier than a hip-worn device, but a hip-worn device reaches 75% faster than the wrist10. This indicates that towards evening hours the movement type might become different and include less ambulatory, whole-body movements resulting in less movement to be captured for a hip-worn accelerometer10. More exact reasons for the differences in the accelerometer output between genders for different wear locations remain to be studied further, in order to improve the understanding of gender differences in physical activity.
Our result also shows that older adults had significantly lower VM cpm than younger ones. Other large-scale studies have consistently shown a decline in device-based total physical activity with increasing age2,7,15,16,25,26. Doherty et al.2 reported total physical activity level over 24-hours to differ strongly between age-groups in both genders, with approximately 7.5% lower mean physical activity level per decade of age. Also in Brazilian children, adolescents and young adults, an inverse linear association was observed between age and overall physical activity7 and in Dutch adults older age was associated with a more stable hourly pattern between days, when examined by wrist-accelerometry6.
We present the hourly patterns of activity in adults of a broad range of ages. We only compared the activity level for every two consecutive hours, but it was observed that the youngest participants aged 25- to 34 years, reached their highest average VM cpm in late afternoon or evening hours. Further, particularly for women in the mid-age, the rise in activity level continued significant until later hours in the morning. In the oldest men and women there were only few significant differences in activity level between consecutive hours, which to some extent confirms that there was less variation in activity level during 24 hours in the oldest participants. Our observations are supported by some previous studies that have shown the activity level in older persons to peak early in the day (around 10 a.m.) and a prolonged taper throughout the rest of the day10,27. The differences in physical activity between age-groups have also been most prominent in the afternoon hours2, older participants showing a decline in activity level after a peak in the morning, whereas younger subjects sustain their activity level until later hours in the afternoon16.
One important underlying factor for the hourly patterning of activity is chronotype. The chronotype of adolescents28 and young adults29 is more often evening type, and chronotype may change with ageing towards more of morning type30. However, it may be that the morning types become more frequent among older age-groups due to an increase in premature deaths among the evening types30,31. Age-related differences in the hourly pattern of physical activity can also be a result of household or family size, where especially the presence of younger children in the household could result in a more active afternoon and evening time as compared to a person living as single.
As expected, the hourly patterns of activity differed between weekdays and there was a higher, albeit later peak in activity level on weekend days, especially Saturdays, in both genders. It is known that physical activity during weekend days may be different from other weekdays, but also that Saturdays and Sundays may differ2,32. Especially women may show slightly higher physical activity levels on Saturdays compared to the average weekday33. Older persons show a more stable pattern between weekdays6 and younger persons have more activity during weekend days2,34. Furthermore, in the current study the activity levels on weekend mornings were lower than on other weekdays and this also support the findings that people may alter their sleep times, particularly their wake-up time during free days as compared to working days29. Even if our result does not permit to conclude on what type of activity the peak during Saturdays include, together with previous findings the observation supports the importance of weekend days as contributors to the weekly physical activity amount in adults.
The unemployed differed in activity level and pattern from the working aged in general, indicating that not having a work to attend decrease the activity level throughout the day. Employment, but not type of employment, is associated with more activity as measured by waist-worn accelerometer, with strongest effect size in younger subjects16. Employed and highly educated persons seem to concentrate their physical activity on weekend days34. Interestingly, we observed students to have the lowest average VM cpm and the most different hourly activity pattern with a slow rise in activity level and the latest timing of peak in activity. This indicates that students may engage in more stationary activities and follow a different diurnal rhythm compared to other employment groups. However, the number of students in the sample is small and is limited to those aged 25 and older, thus limiting broad generalization of the result.
Limitations
The potential impact of non-wear and sleeping time on the activity output needs to be acknowledged35. In the current study, once sleep periods were determined, they were set as wear-time in the non-wear analysis, to avoid the misclassification of sleep periods as non-wear. The separation of non-wear from actual sleep in such 24 hour data is important in order not to exclude true zeros, i.e., zero VM cpm that can occur in sleep from the analyses. In protocols for hip-worn accelerometers false non-wear identification most likely affect estimates of sedentary time. We did not assess reasons for non-wear, but due to the 24-hour protocol it is likely that longer non-wear periods occur for example due to jobs where a wrist-worn device cannot be worn (such as surgeon, nurse, chef, etc.). Thus it can be speculated that long non-wear periods in this dataset rather include activity than sedentary time, which in turn would increase rather than decrease the activity level of some sub-groups.
We decided, as many before us, to report counts, not raw acceleration. Reporting physical activity by accelerometers “counts” is popular36, yet their use is criticized. Counts constitute a summary measure based on the frequency and intensity of post-filtered acceleration values from the accelerometer (Actigraph LLC). Counts also can vary between accelerometer brands which makes comparability between studies difficult. Our goal was to report the total volume and hourly patterning of overall physical activity, and in this matter we believe that both counts and raw acceleration provide the same story. This is also supported by comparisons between hip-worn and wrist-worn devices that include both counts and raw acceleration9,10,11 as well as by the similarity of our findings to studies that have reported the average raw acceleration2.
To classify physical activity into different intensity categories, a variety of different cut points are available, but mainly when the accelerometer is worn on the waist or hip13. The use of cut-points to determine physical activity intensities is questionable, since cut-points are sensitive to the population and wear-site for which they were created3. Furthermore, for 24 hour measurements it is important to notice that a lot of the activity is also happening from non-ambulatory activities, but that many calibration studies have only used ambulatory activities when developing their prediction models37. Implementing machine learning techniques taught on free-living data show promising results also for wrist-worn devices to identify between activity intensities and types38. Once better consensus on the processing of wrist-accelerometer data are achieved it will without doubt be interesting to deepen the findings also from the current study by more specific information about intensity and type of activity throughout the 24 hours.
There is some selection in the participation to the current measurements, as typically for health examination studies where women and older persons are more likely to participate39. Subjects who returned the accelerometer were more likely women and in mid-age as compared to the initial sub-study sample, limiting generalizability of the result to some extent.
Strengths of this study include a fairly large, population-based and randomly selected cohort of adults representing a broad range of ages. The wrist-worn accelerometer resulted in excellent compliance and provides valuable information about the full 24 hour movement continuum. There is great value in activity pattern analyses as they provide a means to examine differences in activity volume between different subgroups of people that would not necessarily be identified using time in intensity level approaches10. Furthermore, the accelerometer that was used in the FinHealth 2017 Survey is one of the most widely used research monitor devices and thus enables future comparison with many existing and forthcoming studies nationally and internationally.
Conclusions
This study is the first to report on device-based physical activity levels and hourly patterns across 24 hours in the general adult population in Finland. Findings indicate higher total physical activity in women than men in age-groups younger than 65 years. However, further work is required for the underlying sources of the gender and age differences observed by wrist-accelerometry to be better understood and specific activity types to be identified more accurately. Even if the wrist-accelerometer may capture also other than whole-body movements, the hourly patterns of physical activity highlight the differences in level and timing of activity between age and socioeconomic groups, as well as between weekdays in the population. The information is useful to consider for more targeted physical activity promotion with respect to different population groups.
Data Availability
Access to FinHealth data is normally granted for researchers who are affiliated with a known institution, to study topics in line with the given ethical guidelines and Finnish legislation. The Executive Board of the FinHealth Survey approves the data access based on written requests and study plans, after which a signed data use contract between the receiving institute and the Finnish National Institute for Health and Welfare is required.
References
2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report. Washington, DC: U.S. Department of Health and Human Services, (2018).
Doherty, A. et al. Large Scale Population Assessment of Physical Activity Using Wrist Worn Accelerometers: The UK Biobank Study. PLoS One 12, e0169649 (2017).
Troiano, R. P., McClain, J. J., Brychta, R. J. & Chen, K. Y. Evolution of accelerometer methods for physical activity research. Br. J. Sports Med. 48, 1019–1023 (2014).
Ancoli-Israel, S. et al. The role of actigraphy in the study of sleep and circadian rhythms. Sleep 26, 342–392 (2003).
Sabia, S. et al. Physical activity and adiposity markers at older ages: accelerometer vs questionnaire data. J. Am. Med. Dir. Assoc. 16, 438e7–438e13 (2015).
Luik, A. I. et al. Stability and Fragmentation of the Activity Rhythm Across the Sleep-Wake Cycle: The Importance of Age, Lifestyle, and Mental Health. Chronobiol. Int. 30, 1223–1230 (2013).
da Silva, I. C. et al. Physical activity levels in three Brazilian birth cohorts as assessed with raw triaxial wrist accelerometry. Int. J. Epidemiol 43, 1959–1968 (2014).
Husu, P. et al. Objectively measured sedentary behavior and physical activity in a sample of Finnish adults: a cross-sectional study. BMC Public Health 16, 920 (2016).
Kamada, M., Shiroma, E. J., Harris, T. B. & Lee, I. M. Comparison of physical activity assessed using hip- and wrist-worn accelerometers. Gait Posture 44, 23–28 (2016).
Shiroma, E. J. et al. Daily physical activity patterns from hip- and wrist-worn accelerometers. Physiol. Meas. 37, 1852–1861 (2016).
Hildebrand, M., VAN Hees, V. T., Hansen, B. H. & Ekelund, U. Age group comparability of raw accelerometer output from wrist- and hip-worn monitors. Med. Sci. Sports Exerc. 46, 1816–1824 (2014).
de, A. M. et al. Calibration of raw accelerometer data to measure physical activity: A systematic review. Gait Posture 61, 98–110 (2018).
Migueles, J. H. et al. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Med 47, 1821–1845 (2017).
Bassett, D. R., Troiano, R. P., McClain, J. J. & Wolff, D. L. Accelerometer-based physical activity: total volume per day and standardized measures. Med. Sci. Sports Exerc. 47, 833–838 (2015).
Wolff-Hughes, D. L., Fitzhugh, E. C., Bassett, D. R. & Churilla, J. R. Waist-Worn Actigraphy: Population-Referenced Percentiles for Total Activity Counts in U.S. Adults. J. Phys. Act. Health 12, 447–453 (2015).
Schrack, J. A. et al. Assessing the “physical cliff”: detailed quantification of age-related differences in daily patterns of physical activity. J. Gerontol. A Biol. Sci. Med. Sci 69, 973–979 (2014).
Koponen, P. et al. Health, functional capacity and welfare in Finland - FinHealth 2017 study. National Institute for Health and Welfare. Helsinki, Finland (2018).
Cole, R. J., Kripke, D. F., Gruen, W., Mullaney, D. J. & Gillin, J. C. Automatic sleep/wake identification from wrist activity. Sleep 15, 461–469 (1992).
Tudor-Locke, C., Barreira, T. V., Schuna, J. M., Mire, E. F. & Katzmarzyk, P. T. Fully automated waist-worn accelerometer algorithm for detecting children’s sleep-period time separate from 24-h physical activity or sedentary behaviors. Appl. Physiol. Nutr. Metab. 39, 53–57 (2014).
Actigraphcorp. What does the “Detect Sleep Periods” button do and how does it work? https://actigraphcorp.com/ (2018).
Choi, L., Ward, S. C., Schnelle, J. F. & Buchowski, M. S. Assessment of wear/nonwear time classification algorithms for triaxial accelerometer. Med. Sci. Sports Exerc. 44, 2009–2016 (2012).
Choi, L., Liu, Z., Matthews, C. E. & Buchowski, M. S. Validation of accelerometer wear and nonwear time classification algorithm. Med. Sci. Sports Exerc. 43, 357–364 (2011).
Ramires, V. V. et al. Physical activity levels objectively measured among older adults: a population-based study in a Southern city of Brazil. Int. J. Behav. Nutr. Phys. Act. 14, 3 (2017).
Picavet, H. S., Wendel-vos, G. C., Vreeken, H. L., Schuit, A. J. & Verschuren, W. M. How stable are physical activity habits among adults? The Doetinchem Cohort Study. Med. Sci. Sports Exerc. 43, 74–79 (2011).
Dyrstad, S. M., Hansen, B. H., Holme, I. M. & Anderssen, S. A. Comparison of self-reported versus accelerometer-measured physical activity. Med. Sci. Sports Exerc. 46, 99–106 (2014).
Hagstromer, M., Troiano, R. P., Sjostrom, M. & Berrigan, D. Levels and patterns of objectively assessed physical activity–a comparison between Sweden and the United States. Am. J. Epidemiol. 171, 1055–1064 (2010).
Sartini, C. et al. Diurnal patterns of objectively measured physical activity and sedentary behaviour in older men. BMC Public Health 4, 609 (2015).
Randler, C., Fassl, C. & Kalb, N. From Lark to Owl: developmental changes in morningness-eveningness from new-borns to early adulthood. Sci. Rep 7, 45874 (2017).
Roenneberg, T. et al. Epidemiology of the human circadian clock. Sleep Med. Rev. 11, 429–438 (2007).
Broms, U. et al. Long-term consistency of diurnal-type preferences among men. Chronobiol. Int. 31, 182–188 (2014).
Knutson, K. L. & von Schantz, M. Associations between chronotype, morbidity and mortality in the UK Biobank cohort. Chronobiol. Int. 35, 1045–1053 (2018).
Jaeschke, L., Steinbrecher, A., Jeran, S., Konigorski, S. & Pischon, T. Variability and reliability study of overall physical activity and activity intensity levels using 24 h-accelerometry-assessed data. BMC Public Health 18, 8 (2018).
Matthews, C. E., Ainsworth, B. E., Thompson, R. W. & Bassett, D. R. Sources of variance in daily physical activity levels as measured by an accelerometer. Med. Sci. Sports Exerc. 34, 1376–1381 (2002).
Gubelmann, C., Vollenweider, P. & Marques-Vidal, P. Of weekend warriors and couch potatoes: Socio-economic determinants of physical activity in Swiss middle-aged adults. Prev. Med. 105, 350–355 (2017).
Tudor-Locke, C., Johnson, W. D. & Katzmarzyk, P. T. U.S. population profile of time-stamped accelerometer outputs: impact of wear time. J. Phys. Act. Health 8, 693–698 (2011).
Plasqui, G., Bonomi, A. G. & Westerterp, K. R. Daily physical activity assessment with accelerometers: new insights and validation studies. Obes. Rev. 14, 451–462 (2013).
Matthews, C. E. et al. Influence of Accelerometer Calibration Approach on Moderate-Vigorous Physical Activity Estimates for Adults. Med. Sci. Sports Exerc. 50, 2285–2291 (2018).
Willetts, M., Hollowell, S., Aslett, L., Holmes, C. & Doherty, A. Statistical machine learning of sleep and physical activity phenotypes from sensor data in 96,220 UK Biobank participants. Sci. Rep 8, 1 (2018).
Mindell, J. S. et al. Sample selection, recruitment and participation rates in health examination surveys in Europe–experience from seven national surveys. BMC Med. Res. Methodol. 15, 4 (2015).
Author information
Authors and Affiliations
Contributions
H.W., K.B., A.P. and H.R. took part in data collection and were responsible for processing and analyzing data. All authors contributed to planning, drafting and finalizing the paper.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wennman, H., Pietilä, A., Rissanen, H. et al. Gender, age and socioeconomic variation in 24-hour physical activity by wrist-worn accelerometers: the FinHealth 2017 Survey. Sci Rep 9, 6534 (2019). https://doi.org/10.1038/s41598-019-43007-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-43007-x
This article is cited by
-
The middle-aged and older Chinese adults’ health using actigraphy in Taiwan (MOCHA-T): protocol for a multidimensional dataset of health and lifestyle
BMC Public Health (2024)
-
Defining and reporting activity patterns: a modified Delphi study
International Journal of Behavioral Nutrition and Physical Activity (2023)
-
Wearable-based accelerometer activity profile as digital biomarker of inflammation, biological age, and mortality using hierarchical clustering analysis in NHANES 2011–2014
Scientific Reports (2023)
-
Rest-activity profiles among U.S. adults in a nationally representative sample: a functional principal component analysis
International Journal of Behavioral Nutrition and Physical Activity (2022)
-
Objectively-measured sleep patterns and cardiometabolic health in a rural South African setting: a cross sectional analysis
Sleep Science and Practice (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
