
Abstract
We assessed whether visceral adipose tissue (VAT) compared with subcutaneous adipose tissue (SAT) has modifying effects on the cross-sectional association between ambient air pollution and hypertension in Korean men. This study included 1,417 adult men who visited a health checkup center. Abdominal fat depots were measured by computed tomography, and we used the annual average concentrations of ambient air pollutants such as particulate matter with an aerodynamic diameter of ≤10 μm (PM10), nitrogen dioxide, sulfur dioxide, and carbon monoxide (CO). The annual mean concentrations of PM10 (odds ratio [OR] = 1.30; 95% confidence interval [CI] = 1.12–1.52) and CO (OR = 1.20; 95% CI = 1.03–1.39) showed a positive association with hypertension. In particular, modifying effects on hypertension were found between PM10 and VAT-related traits such as VAT and visceral-to-subcutaneous fat ratio (VSR). The association between PM10 and hypertension was much stronger in the high-VAT (OR = 1.74; 95% CI = 1.12–2.71) and high-VSR groups (OR = 1.53; 95% CI = 1.23–1.91). However, the strength of association across levels of SAT was not observed (Pint = 0.4615). In conclusion, we found that association between PM10 exposure and hypertension is different by abdominal fat distribution.
Similar content being viewed by others


Introduction
Ambient air pollution, including particulate matter (PM), is a serious health burden worldwide and has recently emerged as the biggest social issue in the Korean society1. The number of deaths from air pollution is estimated at approximately 3 million worldwide each year2. A recent report from the Organization for Economic Cooperation and Development (OECD) documented that Korea will have the most significant increase in the number of premature deaths caused by outdoor air pollution among the OECD countries by 20603. The majority of air pollution-related premature deaths are associated with cardiovascular events, such as myocardial infarction, stroke, and heart attack, and hypertension is regarded as a crucial risk factor in the development of such cardiovascular disease4,5. In recent years, a growing number of epidemiological studies have identified the deleterious effects of ambient air pollution on hypertension6,7,8.
More recent evidence has suggested the importance of obesity in association between long-term air pollution exposure and blood pressure (BP) increments9,10,11. Although the biological pathways underlying this connection have not been completely elucidated, several plausible hypotheses, such as inflammatory and oxidative stress, have been proposed. However, given that central adiposity is a stronger marker for major cardiovascular diseases compared with simple obesity markers, such as body mass index (BMI), and given that its regional distribution, such as subcutaneous and visceral adiposity, plays different roles in the development of such diseases, the depot-specific characteristics of visceral and subcutaneous fat in obesity need to be distinguished to understand these mechanisms. Excessive accumulation of visceral adipose tissue (VAT) has been shown to contribute to the development of cardiovascular diseases via the activation of inflammatory molecules or systemic oxidative damage, even in people with a normal BMI12,13,14. VAT produces more proinflammatory cytokines, such as interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), and visfatin, than subcutaneous adipose tissue (SAT), and this triggers the overproduction of reactive oxygen species (ROS)15,16. In contrast, the subcutaneous fat compartments might even play a protective role in health outcomes16. Within this context, the modification effect of obesity on the association between air pollution and hypertension may be differentiated by adiposity traits; therefore, studies using the accurate measurement of fat mass measured by computed tomography (CT) are needed. However, to the best our knowledge, no studies have been conducted to evaluate such a hypothesis regarding regional fat distributions.
This study aimed to investigate the cross-sectional association between ambient air pollution and hypertension in Korean men and to identify whether these relations are modified by abdominal fat distribution, especially visceral fat.
Materials and Methods
Participants
The subjects in this study were recruited from a health checkup center managed by Seoul National University Hospital from 2006 to 201417,18. Briefly, In South Korea, adults in the general population usually receive regular comprehensive health screenings for the prevention or early detection of the disease. For this reason, large hospitals in South Korea operate comprehensive health check-up center for them. Abdominal fat distribution is very different by sex, and Korean men are known to have a larger distribution of visceral fat than women. In fact, when we classified into three groups by adiposity level using the identical cut-off points in men and women, the sample size of high VAT (n = 26) or visceral-to-subcutaneous fat ratio (VSR) (n = 48) group in women was a very small for statistical analysis (Data not shown). Thus, only male subjects were considered for the study. A total of 1,759 adult men were enrolled during this period, and 342 subjects without abdominal CT data were excluded from this study. Therefore, a total of 1,417 subjects were included in the final statistical analysis. Considering the purpose of this study to investigate the relationship between air pollution and hypertension is modified by abdominal fat, it was inevitable to exclude subjects without abdominal CT information. There was no big difference between the included (n = 1,417) and excluded (n = 342) samples in BP traits and hypertension. In addition, the distributions of BMI and anthropometric data including height and weight were similar between included and excluded samples. In case of age, the distribution between the included and excluded samples was also similar. However, there were a little difference between the two samples in lifestyle such as smoking status, drinking, and physical activity (Data not shown). The protocol for this study was approved by the institutional review board of the Seoul National University Hospital Biomedical Research Institute (IRB no.: 1708-017-873), and all participants provided informed written consent before the initiation of the study. All methods were performed in accordance with the relevant guidelines and regulations.
Assessment of hypertension
All the evaluation including anthropometric, BP, and laboratory measurement were done in 12 hours overnight fasting state. In case of BP measurement, each subject was requested to sit quietly in a chair with back supported at least for 5 minutes before measurement is taken. All the BP measurements were done using the same validated automatic BP device (EASY-X800 model from JAWON Medical). Two separate measurements with minimum 1 minute interval were taken. The average value of two readings was taken as each subject’s final systolic blood pressure (SBP) and diastolic blood pressure (DBP) data. We also checked whether each individual was taking antihypertensive medications or not. Hypertension was defined as a SBP of ≥140 mmHg, a DBP of ≥90 mmHg, or taking antihypertensive medications. In addition, for subjects who were taking antihypertensive medications, we added 10 mmHg and 5 mmHg to the measured SBP and DBP values, respectively, before analysis for continuous outcomes such as SBP and DBP19.
Assessment of obesity/abdominal adiposity
Based on the Asia-Pacific obesity classification of adult Asians20, the subjects were classified into three groups: underweight or normal (BMI <23 kg/m2), overweight (23 kg/m2 ≤ BMI <25 kg/m2), and obese (BMI ≥25 kg/m2). In addition, abdominal adiposity was measured using the Somatom Sensation 16 CT scanner (Siemens AG, Erlangen, Germany). We estimated the cross-sectional area of abdominal fat compartments using Rapidia 2.8 software (from −250 to −50 Hounsfield units] (INFINITT, Seoul, Korea). The VAT area was defined by delineating intra-abdominal fat bound by parietal peritoneum or transversalis fascia, excluding the vertebra and spinal muscles. SAT area was defined as fat tissue located between inside of dermis and outside of back and abdominal muscles. The VSR was also calculated. We considered the first cut-off value for VAT at 100 cm2, which has been reported as a reasonable criterion for screening for obesity-related cardiovascular disorders21,22. In addition, to define the high visceral obesity group, the second cut-off point for VAT was applied at 200 cm2, twice the screening cut-off level (VAT = 100 cm2)23. Therefore, we classified into three groups according to VAT level: low-VAT group (VAT ≤ 100 cm2), intermediate VAT group (100 cm2 < VAT ≤ 200 cm2), and high-VAT group (VAT > 200 cm2). Subjects were also categorized into three subgroups according SAT level using the same criteria as VAT, because of the absence of optimal cut-off criterion in an Asian population for SAT: low-SAT group (SAT ≤ 100 cm2), intermediate SAT group (100 cm2 < SAT ≤ 200 cm2), and high-SAT group (SAT >200 cm2). In addition, we divided into three groups according to VSR level: low-VSR group (VSR ≤ 0.8), intermediate VSR group (0.8 < VSR ≤ 1.0), and high-VSR group (VSR > 1.0).
Covariate variables
To control the effects of potential confounding variables, we examined the health-related behaviors such as smoking status and alcohol drinking. These items were investigated using a structured questionnaire and were categorized as follows: smoking status (never, former, or current smoker) and alcohol drinking (never, former, or current drinker). Physical activity was defined as moderate- or vigorous-intensity physical activities engagement of more than 10 min at a time at least one day per week. This variable was coded as a binary variable (“yes” or “no”). To identify the potential covariate variable for hypertension, a univariate analysis was performed (Table S1). First, the variables such as age, BMI, and smoking status, which are related to hypertension, were considered as covariates. Second, we also adjusted the physical activity and alcohol consumption, which is essentially considered as covariate variables for hypertension studies, based on previous literature6,8,9, even though their associations were not observed in our data (Table S1).
Assessment of air pollution exposure
We used atmospheric monitoring data for 24-h concentrations of ambient air pollutants from the Ministry of the Environment of Korea (https://www.airkorea.or.kr). The data included concentrations of air pollutants, such as PM with an aerodynamic diameter of ≤10 μm (PM10), nitrogen dioxide (NO2), sulfur dioxide (SO2), and carbon monoxide (CO), measured in approximately 300 national monitoring stations from January 1, 2006 to December 31, 2014. In addition, each subject’s residential zip code information was obtained from the hospital information system database. Using this zip code information, we identified the nearest monitoring station to each subject’s home. To assess the exposure concentrations to air pollutants, we calculated the annual average concentrations corresponding to the health checkup year at the closest monitoring station from each subject’s residence. All four air pollutants are interrelated, with correlation ranging from 0.21 to 0.61 (Table S2). To perform the subgroup analysis stratified by PM10 levels, the quantitative PM10 exposure was classified into four levels using quartiles: quartile 1 (PM10 ≤ 43.8 mg/m3), quartile 2 (43.8 mg/m3 < PM10 ≤ 48.7 mg/m3), quartile 3 (48.7 mg/m3 < PM10 ≤ 55.0 mg/m3), and quartile 4 (PM10 > 55.0 mg/m3). For the final analysis, we divided the subjects into three PM10 exposure groups using these quartiles: low exposure (quartile 1), intermediate exposure (quartiles 2–3), and high exposure (quartile 4).
Statistical analysis
The associations between adiposity trait or ambient air pollution and hypertension were determined by multiple logistic regression analysis. The odds ratios (ORs) and 95% confidence intervals (CIs) of adiposity trait or air pollution for hypertension were estimated in unadjusted and adjusted models for covariates such as age, smoking status, alcohol consumption, and physical activity. In addition, we performed multiple linear regression analysis to identify associations between adiposity trait or ambient air pollution and quantitative BP trait (i.e. SBP or DBP). The beta coefficients (β) and standard errors (SE) of adiposity trait or air pollution for BP traits were estimated in unadjusted and adjusted models for covariates such as age, smoking status, alcohol consumption, and physical activity. The estimates in adiposity traits (i.e. VAT and SAT) and air pollutants were converted by scale to the 100-cm2 area and interquartile range (IQR) for each air pollutant (11.2 μg/m3 for PM10, 15.6 ppb for NO2, 1.9 ppb for SO2, and 2.0 ppm for CO) (Table S2). We also performed a stratified analysis for groups with three different levels of abdominal adiposity trait such as BMI, VAT, SAT, and VSR. In addition, we applied the multiple regression approach with interaction term to test the modifying effect of adiposity level. The modifications on BP traits and hypertension were identified by performing multiple linear regression analysis [Y = β0 + β1age + β2smoking status + β3alcohol consumption + β4physical activity + β5adiposity level + β6air pollution exposure + β7(adiposity level × air pollution exposure) + e] and multiple logistic regression analysis [logit(P) = β0 + β1age + β2smoking status + β3alcohol consumption + β4physical activity + β5adiposity level + β6air pollution exposure + β7(adiposity level × air pollution exposure) + e], respectively. Using the same method as stratification analysis by the adiposity level, we also have performed the subgroup analysis stratified by PM10 levels. All analyses were performed using SAS 9.3 version (SAS Institute, Cary, NC, USA).
Results
The characteristics of the study subjects
Table 1 shows the detailed characteristics of our study subjects. A total of 1,417 men were included in the final association analyses. All subjects were men, and their mean age was 55.9 years. The percentage of current smokers and current drinkers were 31.3% (n = 444) and 66.5% (n = 942), respectively. The mean BMI value was 24.6 kg/m2. With regard to adiposity trait, the mean value of VAT (133.0 cm2) was similar to that of SAT (136.4 cm2), and the mean VSR value was 1.0. Mean SBP and DBP values were 127.6 mmHg and 77.5 mmHg, respectively, and about 27% of the subjects were taking antihypertensive medications. Ultimately, 41.9% of the subjects were classified as hypertensive patients (n = 593).
The association between adiposity-related traits or air pollutants and hypertension
We investigated the association between BP traits and risk factors (i.e. adiposity-related traits and air pollutants) before evaluating hypertension (Table S3). All adiposity-related traits were positively associated with both SBP and DBP. In the case of air pollution, only PM10 in the adjustment model showed a positive association with both SBP (β = 2.13; SE = 0.58) and DBP (β = 1.33; SE = 0.41). In addition, IQRs increases in NO2 (β = 1.16; SE = 0.55) and CO (β = 1.26; SE = 0.60) concentrations in adjusted model were related to increase of SBP. Logistic regression analysis results of the association between adiposity-related traits or air pollutants and hypertension are shown in Table 2. In both unadjusted and adjusted models, all adiposity-related traits, including BMI, VAT, SAT, and VSR, were positively associated with hypertension. The OR of VAT area per 100 cm2 increase (adjusted model: OR = 1.98; 95% CI = 1.63–2.41) was slightly higher than that of the SAT area per 100 cm2 increase (adjusted model: OR = 1.84; 95% CI = 1.49–2.27). With regard to the association between air pollution and hypertension, an IQR (11.2 μg/m3) increase in PM10 concentrations was positively associated with hypertension (adjusted model: OR = 1.30; 95% CI = 1.12–1.52). An IQR (0.2 ppm) increase in CO concentrations also showed a positive association with hypertension (adjusted model: OR = 1.20; 95% CI = 1.03–1.39). However, NO2 (adjusted model: OR = 1.07; 95% CI = 0.93–1.24) and SO2 (adjusted model: OR = 1.01; 95% CI = 0.89–1.15) did not show an association with hypertension.
The subgroup results by classifying the BMI, VAT, SAT, and VSR into three levels
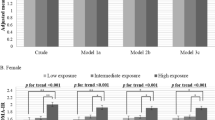
To investigate the association of air pollutants with hypertension based on the degree of each adiposity-related trait, a subgroup analysis was performed by classifying the BMI, VAT, SAT, and VSR into three levels (Table 3 and Fig. 1). In a stratified analysis of BMI, compared with the normal (BMI < 23 kg/m2) or overweight group (23 kg/m2 ≤ BMI < 25 kg/m2), the obese group (BMI ≥ 25 kg/m2) showed a positive association between IQR (11.2 μg/m3) increase in PM10 and hypertension (OR = 1.49; 95% CI = 1.19–1.88). However, the effect of the BMI modification on PM10 and hypertension was not observed (Pint = 0.1315). Modification effects were observed between ambient PM10 and visceral fat-related traits. With regard to VAT, the low adiposity group (VAT ≤ 100 cm2) showed no association between PM10 and hypertension (OR = 1.11; 95% CI = 0.82–1.51), whereas the groups with adiposity traits above the intermediate level were positively associated with increased odds of hypertension. In particular, IQR (11.2 μg/m3) increase in PM10 concentrations in the high-VAT group (VAT > 200 cm2) showed the strongest association with hypertension (OR = 1.74; 95% CI = 1.12–2.71), and the effect of VAT modification was found (Pint = 0.0197). Likewise, with regard to VSR, the association of PM10 with hypertension was the strongest in the high-VSR group (OR = 1.53; 95% CI = 1.23–1.91), and a modifying effect was also identified (Pint = 0.0083). However, the effect of SAT modification on PM10 and hypertension was not observed (Pint = 0.4615). We also identified patterns of PM10 exposure effects on hypertension by fat distribution, including VAT, SAT, and VSR (Fig. 1). Notably, in the case of VAT and VSR, the association of PM10 with hypertension gradually increased with increasing adiposity levels, but there was no difference in the association of PM10 and hypertension according to the SAT level. In addition to hypertension, in subgroup results for quantitative BP traits, the association between PM10 and SBP or DBP was also differential by adiposity level (Tables S4 and S5). However, unlike hypertension, the association between PM10 and increased BP was modified by both VAT and SAT regardless of abdominal fat distribution (all Pint < 0.05).

The associations of PM10 exposures with hypertension according to VAT, VSR, and SAT categories.
The subgroup results stratified by exposure level to PM10
In addition, we performed the subgroup analysis stratified by PM10 levels (Table 4). As shown in Table 4, interestingly, the associations between adiposity and hypertension were also differential by PM10 exposure levels. Similar to the results of subgroup analysis stratified by adiposity levels, association between VAT and hypertension was stronger in the high exposure group (OR = 3.58; 95% CI = 2.32–5.51) than the low exposure group (OR = 1.06; 95% CI = 0.70–1.61). The pattern of result for VSR was similar to that of VAT. Their modifying effects were also observed (both Pint < 0.05). In the case of the SAT, the modifying effect was not found (Pint = 0.1673), although the association with the HTN was greater in the high exposure group (OR = 2.52; 95% CI = 1.60–3.97) than in the low exposure group (OR = 1.63; 95% CI = 1.05–2.53). Besides, we indicate the PM10 concentration-response (i.e. percentage of hypertension) curves according to the VAT or VSR levels (Fig. 2). As the PM10 concentration gradually increased, the proportion of hypertension in the high VAT (Fig. 2a) or VSR (Fig. 2b) group also increased.

The hypertension (%) according to PM10 concentration levels and (a) VAT or (b) VSR levels.
Discussion
We investigated the associations of ambient air pollution and hypertension in adult Korean men and whether these associations were differently modified by each fat depot, including VAT and SAT. In the subgroup analysis classified according to the level of visceral abdominal fat, we observed that the associations between PM10 concentration and hypertension were much stronger in the high-VAT group than in the low-VAT group. Its modification effect was also identified. Besides, the results of the subgroup analysis for VSR showed a pattern similar to that for VAT. In contrast, there was no big difference in the associations between PM10 concentration and hypertension in the subgroup of SAT levels. Our findings suggest that the positive association of PM10 exposure with hypertension is more apparent in people with greater visceral fat rather than in people with subcutaneous fat.
Visceral adiposity has been associated with the occurrence of metabolic and cardiovascular diseases24,25. With regard to hypertension, such relations are especially prominent in the Asian population. Hayashi et al. found a significant association between visceral adiposity and hypertension in Japanese Americans26,27. In 2011, Koh et al. also reported a similar association, indicating that visceral adiposity, rather than subcutaneous fat, is closely related to high BP in Japanese men28. On the contrary, an epidemiological study conducted in a group of African Americans and Hispanic Americans observed no significant relationship between visceral adiposity and hypertension among men29. The effect of visceral fat on hypertension in Asian populations may be more important, as Asians have a greater deposition of visceral fat compared with other ethnic populations. Our results showed that VAT had the highest risk ratio for hypertension, and VSR also showed a significant association with hypertension. These results support the importance of visceral fat in the Asian population.
Recent epidemiological studies have identified the modification effects of obesity defined by BMI on increased BP and ambient air pollution. In 2013, Zhao et al. investigated whether the association between airborne pollutants and increased BP or hypertension is modified by obesity status in a Chinese population9. They reported that the risks for high BP and hypertension by ambient air pollution were greater in overweight/obese adult men. Similarly, more recent study conducted in Chinese children identified significant interaction effects of obesity and long-term air pollution exposure on BP and hypertension10. Our results also showed that the association of PM10 with hypertension is stronger in the obese group than in the non-obese (normal or overweight) group, even though its modification effect was not considered significant. Rather, the modification effect was more pronounced in the abdominal visceral fat-related traits measured directly by CT, than in the BMI, an indirect measure of body fat. These findings highlight the importance of using accurate fat distribution indicators measured directly by CT to better understand the epidemiological or biological association between air pollution, hypertension, and obesity.
The physiological mechanism for the difference in the association between PM10 exposure and hypertension by visceral fat levels is not clear. However, several plausible hypotheses associated with adipocyte have been proposed. The most likely mechanism is inflammation. Prolonged exposure to PM causes hypertension-related vascular endothelial dysfunction via local vascular inflammation or systemic inflammation30,31,32,33. Such endothelial dysfunction may be involved in an increased systemic vascular resistance, thereby leading to the development of hypertension34. Similarly, excess visceral fat accelerates systemic inflammation by releasing inflammatory adipokines, such as TNF-α, IL-6, C-reactive protein, resistin, and macrophage chemoattractant protein-1, in obese humans35,36. Besides, the level of adiponectin associated with anti-inflammatory function is inversely correlated with visceral adiposity. Both PM and visceral fat accumulation are closely associated with increased inflammation response, and the strong association of PM10 and hypertension in the high-visceral adiposity group may be explained by the combined effects of visceral fat and ambient air pollution on vascular and/or systemic inflammation. Another hypothesis is an increase in oxidative stress. Oxidative stress response is one of the major mechanisms underlying hypertension37. Particles in air pollutants alter the vasomotor balance by inducing the production of ROS in the vascular endothelium. Similarly, obesity is involved in systemic oxidative stress responses, and ROS is known to be more associated with visceral fat accumulation than subcutaneous fat accumulation38. In addition, both PM and visceral fat contribute to the imbalance in the autonomic nervous system function30,39, which can lead to the development of hypertension40.
We used four components (i.e. PM10, NO2, SO2, and CO) of ambient air pollution with partially different characteristics. Contrary to the PM10, the gaseous pollutants, such as NO2, SO2, and CO, were not associated with hypertension in our data. Similarly, several previous studies have shown that PM compared to gaseous substances has a strong negative effect on health outcomes4,41,42. PM is a complex mixture of different particles (solid and liquid particles) with physical, chemical and toxicological properties, unlike gaseous pollutants derived from a specific gas43. Such PM in comparison with gaseous pollutants is responsible for a large portion of the pathogenic effects, leading to the development of systemic pro-inflammation via activation of innate immunity as well as enhancement of free radical reactions in cells and tissues43,44. The larger association of PM10 than gaseous pollutants may be explained by the different nature of the air pollutants.
In this study, we measured VAT and SAT using CT to determine the accurate quantitative measurement of fat mass. To our knowledge, we found for the first time that the relationship between PM10 and prevalence of hypertension was more strongly associated with abdominal visceral fat accumulation than subcutaneous fat accumulation. However, several limitations need to be discussed. First, our study had a cross-sectional design, which cannot be used to determine the causal relationship between ambient air pollution, adiposity traits, and hypertension. Second, this study did not include women, due to the large differences in abdominal fat distribution by sex. Air pollution- or adiposity-induced health outcome may differ by gender due to activity patterns, sex hormones, occupational exposure, and lifestyle, in addition to differences in fat distribution. Therefore, our main results, including only adult men, can be difficult to generalize in women. Third, we could not consider socio-economic status information as a confounding factor, due to the absence of relevant data. Therefore, the results may be likely to be affected by residual bias. In addition, it was difficult to estimate a longer period of exposure concentration, because we do not have any information regarding the residential history of the subjects. Therefore, we finally used only the annual average air pollutant concentrations of the year of participant’s medical checkup. Lastly, to estimate air pollution exposure concentrations, we used the community-level exposure assessment which can reduce variations in exposure using a zip code instead of an individual’s exact exposure estimate because of lack of relevant data. This way does not reflect various factors such as indoor or occupational exposure level, diversity of mobility among individuals, residence history, and proximity to major roads. Thus, this may have the potential for exposure misclassification.
In conclusion, we identified that association between PM10 and hypertension in Asian men is different by abdominal fat, especially visceral fat levels. However, more work studying in women or other populations is needed to understand the association between obesity, air pollution exposure, and hypertension.
References
KIHASA. Study of Social Problem and Social Cohesion in Korea with Policy Recommendations. (2017).
van der Wall, E. E. Air pollution: 6.6 million premature deaths in 2050! Netherlands heart journal: monthly journal of the Netherlands Society of Cardiology and the Netherlands Heart Foundation 23, 557–558, https://doi.org/10.1007/s12471-015-0763-9 (2015).
OECD. The Economic Consequences of Outdoor Air Pollution. (2016).
Newby, D. E. et al. Expert position paper on air pollution and cardiovascular disease. European heart journal 36, 83–93b, https://doi.org/10.1093/eurheartj/ehu458 (2015).
Lee, B. J., Kim, B. & Lee, K. Air pollution exposure and cardiovascular disease. Toxicological research 30, 71–75, https://doi.org/10.5487/TR.2014.30.2.071 (2014).
Fuks, K. et al. Long-term urban particulate air pollution, traffic noise, and arterial blood pressure. Environmental health perspectives 119, 1706–1711, https://doi.org/10.1289/ehp.1103564 (2011).
Dong, G. H. et al. Association between long-term air pollution and increased blood pressure and hypertension in China. Hypertension 61, 578–584, https://doi.org/10.1161/HYPERTENSIONAHA.111.00003 (2013).
Basile, J. N. & Bloch, M. J. Exposure to air pollution increases the incidence of hypertension and diabetes in black women living in Los Angeles. Journal of clinical hypertension 14, 819–820, https://doi.org/10.1111/jch.12000 (2012).
Zhao, Y. et al. Does obesity amplify the association between ambient air pollution and increased blood pressure and hypertension in adults? Findings from the 33 Communities Chinese Health Study. International journal of cardiology 168, e148–150, https://doi.org/10.1016/j.ijcard.2013.08.071 (2013).
Dong, G. H. et al. Interactions Between Air Pollution and Obesity on Blood Pressure and Hypertension in Chinese Children. Epidemiology 26, 740–747, https://doi.org/10.1097/EDE.0000000000000336 (2015).
Weichenthal, S., Hoppin, J. A. & Reeves, F. Obesity and the cardiovascular health effects of fine particulate air pollution. Obesity 22, 1580–1589, https://doi.org/10.1002/oby.20748 (2014).
Lam, Y. Y. et al. Role of the gut in visceral fat inflammation and metabolic disorders. Obesity 19, 2113–2120, https://doi.org/10.1038/oby.2011.68 (2011).
Qiang, G. et al. The obesity-induced transcriptional regulator TRIP-Br2 mediates visceral fat endoplasmic reticulum stress-induced inflammation. Nature communications 7, 11378, https://doi.org/10.1038/ncomms11378 (2016).
Wisse, B. E. The inflammatory syndrome: the role of adipose tissue cytokines in metabolic disorders linked to obesity. Journal of the American Society of Nephrology: JASN 15, 2792–2800, https://doi.org/10.1097/01.ASN.0000141966.69934.21 (2004).
Marseglia, L. et al. Oxidative stress in obesity: a critical component in human diseases. International journal of molecular sciences 16, 378–400, https://doi.org/10.3390/ijms16010378 (2014).
Porter, S. A. et al. Abdominal subcutaneous adipose tissue: a protective fat depot? Diabetes care 32, 1068–1075, https://doi.org/10.2337/dc08-2280 (2009).
Nam, K. W. et al. High neutrophil to lymphocyte ratios predict intracranial atherosclerosis in a healthy population. Atherosclerosis 269, 117–121, https://doi.org/10.1016/j.atherosclerosis.2017.12.035 (2018).
Nam, K. W. et al. Cerebral white matter hyperintensity is associated with intracranial atherosclerosis in a healthy population. Atherosclerosis 265, 179–183, https://doi.org/10.1016/j.atherosclerosis.2017.09.010 (2017).
Cui, J. S., Hopper, J. L. & Harrap, S. B. Antihypertensive treatments obscure familial contributions to blood pressure variation. Hypertension 41, 207–210 (2003).
AsiaPacificPerspective. Redefining Obesity and Its Treatment. WorldHealth Organization/international Association for the Study ofObesity/international Obesity Task Force, Geneva, Switzerland, pp. 2000. (2000).
Japan, E. C. o. C. f. O. D. i. New criteria for ‘obesity disease’ in Japan. Circulation Journal 66, 987–992 (2002).
Okauchi, Y. et al. Absolute value of bioelectrical impedance analysis-measured visceral fat area with obesity-related cardiovascular risk factors in Japanese workers. J Atheroscler Thromb 17, 1237–1245 (2010).
Kim, H. J. et al. Abdominal adiposity intensifies the negative effects of ambient air pollution on lung function in Korean men. International journal of obesity 41, 1218–1223, https://doi.org/10.1038/ijo.2017.97 (2017).
Chiba, Y. et al. Relationship between visceral fat and cardiovascular disease risk factors: the Tanno and Sobetsu study. Hypertension research: official journal of the Japanese Society of Hypertension 30, 229–236, https://doi.org/10.1291/hypres.30.229 (2007).
Fox, C. S. et al. Abdominal visceral and subcutaneous adipose tissue compartments: association with metabolic risk factors in the Framingham Heart Study. Circulation 116, 39–48, https://doi.org/10.1161/CIRCULATIONAHA.106.675355 (2007).
Hayashi, T. et al. Visceral adiposity and the prevalence of hypertension in Japanese Americans. Circulation 108, 1718–1723, https://doi.org/10.1161/01.CIR.0000087597.59169.8D (2003).
Hayashi, T. et al. Visceral adiposity is an independent predictor of incident hypertension in Japanese Americans. Annals of internal medicine 140, 992–1000 (2004).
Koh, H. et al. Visceral adiposity, not abdominal subcutaneous fat area, is associated with high blood pressure in Japanese men: the Ohtori study. Hypertension research: official journal of the Japanese Society of Hypertension 34, 565–572, https://doi.org/10.1038/hr.2010.271 (2011).
Foy, C. G. et al. Visceral fat and prevalence of hypertension among African Americans and Hispanic Americans: findings from the IRAS family study. American journal of hypertension 21, 910–916, https://doi.org/10.1038/ajh.2008.213 (2008).
Brook, R. D. & Rajagopalan, S. Particulate matter, air pollution, and blood pressure. Journal of the American Society of Hypertension: JASH 3, 332–350, https://doi.org/10.1016/j.jash.2009.08.005 (2009).
Dharmashankar, K. & Widlansky, M. E. Vascular endothelial function and hypertension: insights and directions. Current hypertension reports 12, 448–455, https://doi.org/10.1007/s11906-010-0150-2 (2010).
Savoia, C. et al. Vascular inflammation and endothelial dysfunction in experimental hypertension. International journal of hypertension 2011, 281240, https://doi.org/10.4061/2011/281240 (2011).
Tamagawa, E. et al. Particulate matter exposure induces persistent lung inflammation and endothelial dysfunction. American journal of physiology. Lung cellular and molecular physiology 295, L79–85, https://doi.org/10.1152/ajplung.00048.2007 (2008).
Dinh, Q. N., Drummond, G. R., Sobey, C. G. & Chrissobolis, S. Roles of inflammation, oxidative stress, and vascular dysfunction in hypertension. BioMed research international 2014, 406960, https://doi.org/10.1155/2014/406960 (2014).
Fontana, L., Eagon, J. C., Trujillo, M. E., Scherer, P. E. & Klein, S. Visceral fat adipokine secretion is associated with systemic inflammation in obese humans. Diabetes 56, 1010–1013, https://doi.org/10.2337/db06-1656 (2007).
Monteiro, R. & Azevedo, I. Chronic inflammation in obesity and the metabolic syndrome. Mediators of inflammation 2010, https://doi.org/10.1155/2010/289645 (2010).
Ceriello, A. Possible role of oxidative stress in the pathogenesis of hypertension. Diabetes care 31(Suppl 2), S181–184, https://doi.org/10.2337/dc08-s245 (2008).
Fujita, K., Nishizawa, H., Funahashi, T., Shimomura, I. & Shimabukuro, M. Systemic oxidative stress is associated with visceral fat accumulation and the metabolic syndrome. Circulation journal: official journal of the Japanese Circulation Society 70, 1437–1442 (2006).
Fidan-Yaylali, G. et al. The Association between Central Adiposity and Autonomic Dysfunction in Obesity. Medical principles and practice: international journal of the Kuwait University, Health Science Centre 25, 442–448, https://doi.org/10.1159/000446915 (2016).
Mancia, G. & Grassi, G. The autonomic nervous system and hypertension. Circulation research 114, 1804–1814, https://doi.org/10.1161/CIRCRESAHA.114.302524 (2014).
Eze, I. C. et al. Long-term air pollution exposure and diabetes in a population-based Swiss cohort. Environ Int 70, 95–105, https://doi.org/10.1016/j.envint.2014.05.014 (2014).
Fuks, K. B. et al. Long-term exposure to ambient air pollution and traffic noise and incident hypertension in seven cohorts of the European study of cohorts for air pollution effects (ESCAPE). European heart journal 38, 983–990, https://doi.org/10.1093/eurheartj/ehw413 (2017).
Eze, I. C. et al. Long-Term Exposure to Ambient Air Pollution and Metabolic Syndrome in Adults. PLoS One 10, e0130337, https://doi.org/10.1371/journal.pone.0130337 (2015).
Araujo, J. A. Particulate air pollution, systemic oxidative stress, inflammation, and atherosclerosis. Air Qual Atmos Health 4, 79–93, https://doi.org/10.1007/s11869-010-0101-8 (2010).
Acknowledgements
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education, Science and Technology (grant number, 2015R1D1A1A01057619 and 2018R1D1A1A09083190). This study was supported in part by a research grant from Hanmi Pharmaceutical Co., Ltd, Republic of Korea.
Author information
Authors and Affiliations
Contributions
H.-J.K. and H.K. planned this study, and J.-H.P. managed this study. H.K., S.-M.J., S.H.E. and J.-H.P. contributed to the acquisition and quality control of data for the work, and H.-J.K. analyzed data. H.-J.K. wrote the manuscript, and J.-H.P. finally reviewed the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kim, HJ., Kwon, H., Jeong, SM. et al. Effects of abdominal visceral fat compared with those of subcutaneous fat on the association between PM10 and hypertension in Korean men: A cross-sectional study. Sci Rep 9, 5951 (2019). https://doi.org/10.1038/s41598-019-42398-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-42398-1
This article is cited by
-
Effects of the abdominal fat distribution on the relationship between exposure to air pollutants and thyroid hormones among Korean adult males
European Journal of Medical Research (2023)
-
A genome-wide by PM10 exposure interaction study for blood pressure in Korean adults
Scientific Reports (2023)
-
Genome-wide identification and characterization of long non-coding RNAs during differentiation of visceral preadipocytes in rabbit
Functional & Integrative Genomics (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
