
Abstract
Natural disasters are often associated with forced residential relocation, thereby affected people experience a change of food environment that results in the increased body mass index. However, there are a few studies that examined whether a change in food environment caused risk of obesity after a natural disaster. To address this question, we leveraged a natural experiment of residential relocation in the aftermath of the 2011 Japan Earthquake and Tsunami. Our baseline data came from a nationwide cohort study of older community-dwelling adults conducted 7 months prior to the disaster. By chance, one of the field sites (Iwanuma City, Miyagi Prefecture) was directly in the line of the tsunami. Approximately 2.5 years after the disaster, we ascertained the residential addresses and health status of 3,594 survivors aged 65 years or older (82.1% follow-up rate). Fixed effects multinomial logistic regression showed that shortened distances to food outlets/bars increased the risks of transitioning from BMI in the normal range (18.5–22.9) to obesity (≥25.0) (Odds ratios: 1.46 for supermarkets; 1.43 for bars; 1.44 times for fast food outlets). Radically changed food access after a natural disaster may raise the risk of obesity among older survivors.
Similar content being viewed by others

Introduction
Natural disasters are increasing in frequency and severity worldwide1. Due to population aging, older individuals are increasingly and disproportionately affected by disasters. In the aftermath of the 2011 Great East Japan Earthquake and Tsunami, which occurred on March 11, 2011, 89% of the post-disaster related deaths were older residents who were 65 years old or older2.
Experiences of natural disasters may be associated with weight gain. For example, incident depressive symptoms following disaster-related trauma might lead stress-related over-eating as a coping response. A panel survey in affected three municipalities of the 2011 Great East Japan Earthquake and Tsunami showed that residential relocation due to housing destruction was associated with increased body weight3. Other studies have reported increased alcohol intake4 and lower vegetable/fruit intake5 among survivors of the 2011 earthquake. However, the weight gain was measured only after the disaster, i.e., the study lacked information on the pre-disaster body weight of survivors, so that it is not possible to draw a strong causal inference.
Natural disasters are often associated with property destruction and forced residential relocation, thereby affected people experience a change of food environment that is hypothesized to affect people’s nutritional habits and body mass index (BMI)6,7,8. However, there are a few studies for the association between change in food environment and changes in weight status before vs. after natural disasters. Asking about pre-disaster conditions after the disaster is obviously subject to recall bias.
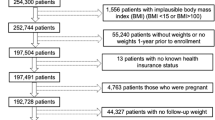
Here, we took advantage of a unique “natural experiment” stemming from the 2011 Great East Japan Earthquake and Tsunami, in which an estimated 18,500 people lost their lives9 and approximately 345,000 people were involuntarily displaced because of widespread sudden property destruction10. Our nationwide cohort study of aging, the Japan Gerontological Evaluation Study (JAGES), was established 7 months before the disaster to examine individual and community predictors of healthy aging. One of the field sites of the cohort was Iwanuma city in Miyagi Prefecture, located approximately 80-km west of the earthquake epicenter (Fig. 1). Approximately 2.5 years after the disaster, we recontacted 3,594 survivors to gather information about their disaster experiences and health status (82.1 percent follow-up rate) (Fig. 2).

Map of inundated area in Iwanuma city, Japan. Reproduced from Hikichi, H. et al. Social capital and cognitive decline in the aftermath of a natural disaster: a natural experiment from the 2011 Great East Japan Earthquake and Tsunami. The Lancet Planetary Health 1 (3), e105-e113, DOI: 10.1016/S2542–5196(17)30041-4 (2017) (CC BY-NC-ND 4.0 license).

Participants flow in this study.
Following the disaster, city officials directed the survivors who lost their homes to move into public prefabricated temporary housing villages [kasetsu jyutaku, resembling FEMA (Federal Emergency Management Agency)–style trailer housing communities in the United States] or to seek housing in the open rental market, both located in the central area of Iwanuma City. As a result (shown in Fig. 3), involuntarily relocated people experienced the greater convenience of access to local food establishments, including fast food outlets and bars. We hypothesized that shortened distances to food outlets/bar (supermarkets, fast food outlets, bars, and convenience stores) due to involuntary relocation would be associated with increased risk of weight gain.

Density of displaced respondents’ addresses and locations of food outlets/bars.
Methods
Study participants
The Japan Gerontological Evaluation Study (JAGES) is a nationwide cohort study established in 2010 to examine prospectively the predictors of healthy aging. One of the field sites of the JAGES cohort is based in the city of Iwanuma (total population 44,187 in 2010)11 in Miyagi Prefecture. We conducted a census of all residents aged 65 years or older in August 2010 (n = 8,576), using the official residential register. The survey inquired about personal characteristics as well as their health status. The response rate to our baseline survey was 59.0% (n = 5,058), which is comparable to other surveys of community-dwelling residents.
The earthquake and tsunami occurred on March 11, 2011, seven months after the baseline survey. Iwanuma city is a coastal municipality located approximately 80 kilometers west of the earthquake epicenter, so that it was in the direct line of the tsunami that killed 180 residents, damaged 5,542 houses and inundated 48% of the land area (Fig. 1)12.
Approximately 2.5 years after the disaster (starting in October 2013), we conducted a follow-up survey of all survivors. The survey gathered information about personal experiences of disaster as well as updating their health status. Informed consent was obtained at the time of survey collection.
The detailed flow-chart of the analytic sample is presented in Fig. 2. Of the 4,380 eligible participants from the baseline survey, we managed to re-contact 3,594 individuals (follow-up rate: 82.1%). Our analytic sample comprises 3,567 individuals, after excluding respondents (n = 27) who returned invalid informed consent forms (e.g., signed by the next of kin rather than the individual).
Outcome variable
Our primary outcome was BMI calculated from self-reported height and weight in both waves (2010 and 2013). The accuracy of self-reported BMI has been previously demonstrated in a Japanese older population, by comparing with physical measurements of BMI13. We categorized BMI into four categories, according to World Health Organization classification for Asian populations: <18.5 (underweight), 18.5–22.9 (normal weight), 23.0–24.9 (overweight), and ≥25.0 (obese)14.
Explanatory variables
Our primary exposure variable was a change in distance (in kilometers) from each respondent’s residential address to the nearest food outlet or bar during the follow-up period. Data of fast food outlets (hamburger, fried chicken, pizza, pancake, noodle, and beef bowl) and bars were obtained from the corporate telephone directories in April 2010 and 2013 provided by Nippon Software Knowledge Corporation. The list of supermarkets (except for small grocery stores) and convenience stores (e.g., Seven-Eleven) were obtained from the Zenrin Geo Intelligence Company Limited, which cover the months from September 2009 to December 2010 (representing the pre-disaster period) and from March 2013 to May 2014 (representing the post-disaster period). Using ArcGIS Desktop version 10.4 (Esri, Redlands, California, USA), we then calculated the road network distance of each resident to the nearest bar, fast food outlet, supermarket, or convenience store15 in Iwanuma as well as in Natori city which the closest neighboring city and geographically accessible from Iwanuma (Fig. 3).
Covariates
We selected time-varying demographic variables: age16, equivalized income17, spousal loss or divorce18, employment status19, and living alone20. Other time-invariant characteristics, such as sex and educational attainment, were omitted from our fixed effects regressions, because it was statistically differenced out in the model21. We also controlled for experiences of loss of relatives and/or friends during the disaster22.
We additionally examined a set of variables as potential risk factors for being obese. These variables included: current alcohol drinking23, current smoking24, the frequency of eating vegetables or fruits during the past one month25, the frequency of eating meat or fish during the past one month26, incident depressive symptoms27, and decreased daily walking time28, and neighborhood physical activity environment (within a 1 kilometer buffer zone from the residence)29. We asked respondents about the number of parks or sidewalks suitable for exercise or walking, the number of unwalkable places due to bumps or slopes, and the number of roads or intersections posing a high risk for traffic accidents.
Household income was equalized by the square root of the number of household members and grouped as 2 million Japanese yen or more versus under 2 million Japanese yen. Depressive symptoms were categorized into lower risk (4 points and lower) versus higher risk (5 points and higher)30.
Statistical analysis
In the present study, we used a fixed effects multinomial logistic regression approach to examine the associations between changes in closest distance to a food outlet/bar and changes in BMI categories over time. This analysis estimates within-person probabilities of transition from the normal range at baseline to another range (underweight, overweight, or obese) at follow-up. The fixed effects approach effectively differences out all observed and unobserved time-invariant confounding factors (e.g., sex, educational attainment, and genetic factors)31. The reference category for our multinomial regression was individuals whose baseline BMI was within the normal range (18.5–22.9 kg/m2).
As a sensitivity analysis, the fixed effects linear regression using BMI as a continuous outcome was also conducted to check the linearity of the association between changes in distances to nearest food outlets and changes in BMI for the overall analytic sample regardless of respondents’ baseline BMI.
Because food outlets tend to be spatially clustered, it is difficult to isolate the effect of any specific type of outlet over another. Hence, we conducted an additional robustness check to examine whether a change in the exposure to any outlet within a 1 km buffer zone was associated with change in BMI. We measured the number (i.e. density) of four types of food outlets/bar within a 1 km radius of each residential address8 at both surveys. Before the disaster, approximately half of displaced respondents lived in places where there was no any food shop/restaurant within a 1 km radius of their residences.
To address potential bias due to missing data, we used multiple imputation by Markov Chain Monte Carlo method assuming missingness at random for explanatory variables and covariates. We created fifty imputed data sets and combined each result of analysis using the Stata command “mi estimate”. All analyses were performed using STATA version 14.0 (STATA Corp LP., College Station, Texas, USA).
Ethics statement
The study was reviewed and approved by the Human Subjects Committee of the Harvard T. H. Chan School of Public Health, the Ethics Committee of the Tohoku University Graduate School of Medicine, the Research Ethics Committee of the Graduate School of Medicine, Chiba University, and the Research Ethics Committee involving Human Participants of the Nihon Fukushi University. Respondents signed on the informed consent form. We followed the STROBE Statement to report our observational study
Results
We compared our analytic sample with the local (pre-disaster) census data for older residents (Table S1). The proportion of women is comparable to the actual census of older residents in Iwanuma city in October 2010 (56.5% for our sample, 57.2% for census data)11. The age distribution of our sample is also close to that of the local census data except for the group aged 85 years and over (6.2% and 13.2%, respectively)11. Our respondents were also somewhat more likely to be married (72.8%) compared to the census (64.7%)32. However, the proportion of employed individuals in our study (17.8%) is quite close to the census data (17.2%)33.
We also compared the characteristics of our analytic sample to non-respondents at the follow-up survey (Table S1). The sex distribution was similar, although our analytic sample was somewhat older than the non-respondents. The proportion of married people in our analytic sample (72.8%) was higher than among non-respondents (64.9%). More respondents were likely to be employed at the time of the follow-up survey (17.8%) compared with the non-respondents (14.0%). This could have resulted in some attrition bias, but the differences were not large.
Table 1 presents the characteristics of displaced respondents (n = 208) and non-displaced respondents (n = 3,359) at baseline (prior to the disaster) and at follow-up 2.5 years later. Our primary outcome was BMI calculated from self-reported height and weight in both waves (2010 and 2013), which were categorized into four categories according to World Health Organization classification for Asian populations: <18.5 (underweight), 18.5–22.9 (normal weight), 23.0–24.9 (overweight), and ≥25.0 (obese)14. The prevalence of obesity (BMI ≥ 25.0) was sharply increased among displaced respondents (25.0% to 35.1%), whereas non-displaced respondents reported a slightly decreased prevalence of obesity (26.9% to 26.6%).
Table 1 also shows that displaced survivors moved closer to most types of food outlets as a result of residential relocation. We calculated the road network distance of each residential address to the nearest bar, fast food outlet, supermarket, and convenience store, using the geographic information system. For example, 83.7% of displaced residents lived more than 2.0 km from the nearest supermarket before the disaster, but the proportion was reduced to 5.8% after relocation. By contrast, 24.9% of non-displaced residents lived >2.0 km from the nearest supermarket (which proportion remained unchanged, because they did not move). The proportion of displaced respondents who reported losing relatives and/or friends in the disaster was approximately two times higher than non-displaced respondents (68.3% and 35.3%, respectively).
In the present study, we used a fixed effects multinomial logistic regression approach to examine the associations between changes in the closest distance to a food outlet/bar and changes in BMI categories over time. This analysis estimates within-person probabilities of transition from the normal range (BMI 18.5–22.9 kg/m2) at baseline to another range (underweight (BMI < 18.5), overweight (23.0–24.9), or obese (BMI ≥ 25)) at follow-up31. Table 2 present the results of fixed effects multinomial logistic regression models correlating the change in distance (in km) to the closest supermarket, bar, fast food outlet, and convenience store and the odds ratios of transitioning to obesity, overweight, and underweight. The results showed that moving 1.0 kilometer closer to a supermarket, bar, or fast food outlet increased the odds of transitioning from BMI in the normal range (18.5–22.9) to obesity (≥25.0) (Odds ratio [OR] 1.46, 95% confidence interval [CI] 1.15, 1.86; OR 1.43, 95% CI 1.11, 1.86; OR 1.44, 95% CI 1.12, 1.86; respectively). Among the potential risk factor for obesity, drinking alcohol was also significantly associated with transitioning from normal range to obesity (ORs 1.17 to 1.24 through models with each food outlet/bar). Loss of loved ones and incident depressive symptoms were not significant for the risk of being obese after the disaster.
The results of fixed linear regression using continuous BMI as the outcome similarly indicated significant associations between distances and BMI (Table 3). A decrease in distance to the closest supermarket by 1.0 km resulted in an increment in continuous BMI by 0.08 units (95% CI 0.02, 0.15). Similarly, each kilometer decrease in distance to the nearest bar was associated with an increase in continuous BMI (0.08 units, 95% CI 0.01, 0.15, for the closest bar).
As shown in Table S2, an increase in the exposure to any food outlet/bar from 0 to ≥1 after the disaster was associated with an increment in continuous BMI by 0.70 units (95% CI 0.30, 1.11).
Discussion
To our knowledge, this is the first study to demonstrate that involuntary relocation after a natural disaster is associated with a change in BMI among older survivors. The associations remained after statistically controlling for unobserved time-invariant variables as well as time-varying risk factors for change in BMI. Although shortened distance to the closest convenience store was not statistically significantly associated with risk of increasing BMI (Tables 2 and 3), the joint exposure to any type of food outlet/restaurants was statistically significant (Table S2). That is, improved food access may have caused an increase in BMI, regardless of the type of food outlet/restaurant.
There are several plausible mechanisms to explain weight gain among survivors of the disaster. For example, the stress and trauma experienced by survivors could lead to difficulties with sleep which is linked to increased BMI34. However, disaster-related trauma (i.e., loss of relatives and/or friends) and depressive symptoms were not significantly associated with increased BMI (Tables 2 and 3). Relocation to the trailer homes may have also resulted in diminished social interactions35, so that people had fewer opportunities to engage in physical activity, e.g. by walking every day to greet friends and neighbors. In our study, decreased daily walking time was also not significantly correlated with weight gain (Table 3). Thus, the remaining possible explanation for our findings is that improved access to restaurants, bars, and food retail outlets increased the opportunities for eating out and drinking, as changes in drinking habit are significantly associated with increased risk of becoming obese.
A major strength of this study is the availability of information pre-dating the disaster about BMI as well as other health conditions. Our design was, therefore, able to effectively address the problem of recall bias in most studies conducted in post-disaster settings.
A limitation is that selection bias might have arisen due to the 59% response rate to the baseline survey. However, this response rate is quite comparable to similar surveys involving community-dwelling residents36. In addition, we confirmed that the demographic profile of our participants is quite similar to the rest of Iwanuma residents aged 65 years or older (Table S1). Also, the response rate of our follow-up survey among survivors was quite high (82.1%). Owing to the compulsory residential registration system in Japan, only seventeen residents from the baseline sample could not be tracked (Fig. 2). Furthermore, BMI was self-reported and may include measurement error, although the accuracy of self-reports has been previously demonstrated in a Japanese older population13. Our findings may be still residually confounded by unobserved time-varying factors correlated with residential displacement. Our observations are also based on a relatively small sample of displaced survivors (n = 208), which may not be generalizable to displaced residents elsewhere. Nevertheless, our findings point to an important policy implication that planners should take into consideration access to services in making decisions about where to build temporary shelters in the aftermath of a disaster. In one sense, the local service access was “improved” for the disaster-affected residents in our study; but from the public health point of view, we also documented an unintended consequence, viz. dramatic weight gain.
Data Availability Statement
All data needed to evaluate the conclusions in the paper are present in the paper and/or the Supplementary Materials. The JAGES data used in this study will be made available upon request, as per NIH data access policies. The authors require the applicant to submit an analysis proposal to be reviewed by an internal JAGES committee to avoid duplication. Confidentiality concerns prevent us from depositing our data in a public repository. Authors requesting access to the Iwanuma data need to contact the principal investigator of the parent cohort (K.K.) and the Iwanuma sub-study principal investigator (I.K.) in writing. Proposals submitted by outside investigators will be discussed during the monthly investigators’ meeting to ensure that there is no overlap with ongoing analyses. If approval to access the data is granted, the JAGES researchers will request the outside investigator to help financially support our data manager’s time to prepare the data for outside use.
References
Center for Research on the Epidemiology of Disasters. EM-DAT the International Disaster Database, http://www.emdat.be/ (2017) Accessed April 25, 2017.
HelpAge International. Displacement and older people: The case of the Great East Japan Earthquake and Tsunami of 2011, http://www.helpage.org/silo/files/displacement-and-older-people-the-case-of-the-great-east-japan-earthquake-and-tsunami-of-2011.pdf Accessed December 3, 2016 (2013).
Takahashi, S. et al. Association between relocation and changes in cardiometabolic risk factors: a longitudinal study in tsunami survivors of the 2011 Great East Japan Earthquake. BMJ Open 6, e011291, https://doi.org/10.1136/bmjopen-2016-011291 (2016).
Kanehara, A. et al. Trends in psychological distress and alcoholism after The Great East Japan Earthquake of 2011. SSM - Population Health 2, 807–812, https://doi.org/10.1016/j.ssmph.2016.10.010 (2016).
Nishi, N. et al. Relationship of Living Conditions With Dietary Patterns Among Survivors of the Great East Japan Earthquake. Journal of Epidemiology 23, 376–381, https://doi.org/10.2188/jea.JE20130025 (2013).
Giskes, K., van Lenthe, F., Avendano-Pabon, M. & Brug, J. A systematic review of environmental factors and obesogenic dietary intakes among adults: are we getting closer to understanding obesogenic environments? Obesity Reviews 12, e95–e106, https://doi.org/10.1111/j.1467-789X.2010.00769.x (2011).
Holsten, J. E. Obesity and the community food environment: a systematic review. Public Health Nutrition 12, 397–405, https://doi.org/10.1017/S1368980008002267 (2009).
Cobb, L. K. et al. The relationship of the local food environment with obesity: A systematic review of methods, study quality and results. Obesity (Silver Spring, Md.) 23, 1331–1344, https://doi.org/10.1002/oby.21118 (2015).
National Police Agency. Damage overview and measures by the police in aftermath of Tohoku earthquake and tsunami, https://www.npa.go.jp/archive/keibi/biki/higaijokyo.pdf (2015) [Japanese]Accessed July 28, 2015.
Reconstruction Agency. The Number of Evacuees in aftermath of Tohoku earthquake and tsunami, http://www.reconstruction.go.jp/topics/main-cat2/sub-cat2-1/20150630_hinansha_suii.pdf (2015) [Japanese]Accessed July 28, 2015.
Iwanuma City. Change of Population by Age Group and Sex, https://www.city.iwanuma.miyagi.jp/shisei/tokei/joho/documents/4nenreikakusaijinkousuii.pdf Accessed May 7, 2017 (2010).
Miyagi Prefectural Government. Current situations of damage and evacuation, https://www.pref.miyagi.jp/uploaded/attachment/625724.pdf (2017) [Japanese]Accessed May 27, 2017.
Yong, V. & Saito, Y. How accurate are self-reported height, weight, and BMI among community-dwelling elderly Japanese?: Evidence from a national population-based study. Geriatrics & Gerontology International 12, 247–256, https://doi.org/10.1111/j.1447-0594.2011.00759.x (2012).
World Health Organization Regional Office for the Western Pacific, International Diabetes Institute, International Association for the Study of Obesity & International Obesity Task Force. The Asia-Pacific perspective: Redefining obesity and its treatment. (Health Communications Australia, 2000).
Charreire, H. et al. Measuring the food environment using geographical information systems: a methodological review. Public Health Nutrition 13, 1773–1785 (2010).
Dey, D. K., Rothenberg, E., Sundh, V., Bosaeus, I. & Steen, B. Height and body weight in the elderly. I. A 25-year longitudinal study of a population aged 70 to 95 years. European Journal of Clinical Nutrition 53, 905–914 (1999).
Murayama, H. et al. Socioeconomic Status and the Trajectory of Body Mass Index Among Older Japanese: A Nationwide Cohort Study of 1987–2006. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences 71, 378–388, https://doi.org/10.1093/geronb/gbu183 (2016).
Kamal, S. M. M., Hassan, C. H. & Alam, G. M. Dual Burden of Underweight and Overweight among Women in Bangladesh: Patterns, Prevalence, and Sociodemographic Correlates. Journal of Health, Population, and Nutrition 33, 92–105 (2015).
Kang, H.-T., Lee, H.-R., Lee, Y.-J., Linton, J. A. & Shim, J.-Y. Relationship between employment status and obesity in a Korean elderly population, based on the 2007–2009 Korean National Health and Nutrition Examination Survey (KNHANES). Archives of gerontology and geriatrics 57, 54–59, https://doi.org/10.1016/j.archger.2013.02.004 (2013).
Tani, Y. et al. Combined effects of eating alone and living alone on unhealthy dietary behaviors, obesity and underweight in older Japanese adults: Results of the JAGES. Appetite 95, 1–8, https://doi.org/10.1016/j.appet.2015.06.005 (2015).
Chang, H.-H. Functional food consumption and depression among the elderly — What can we learn from a longitudinal survey? Economic Modelling 33, 187–193, https://doi.org/10.1016/j.econmod.2013.04.023 (2013).
Husarewycz, M. N., El-Gabalawy, R., Logsetty, S. & Sareen, J. The association between number and type of traumatic life experiences and physical conditions in a nationally representative sample. General hospital psychiatry 36, 26–32, https://doi.org/10.1016/j.genhosppsych.2013.06.003 (2014).
Wakabayashi, I. Cross-Sectional Relationship between Alcohol Consumption and Prevalence of Metabolic Syndrome in Japanese Men and Women. Journal of Atherosclerosis and Thrombosis 17, 695–704, https://doi.org/10.5551/jat.3517 (2010).
Botoseneanu, A. & Liang, J. The Effect of Stability and Change in Health Behaviors on Trajectories of Body Mass Index in Older Americans: A 14-Year Longitudinal Study. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences 67, 1075–1084, https://doi.org/10.1093/gerona/gls073 (2012).
Sartorelli, D. S., Franco, L. J. & Cardoso, M. A. High intake of fruits and vegetables predicts weight loss in Brazilian overweight adults. Nutrition Research 28, 233–238, https://doi.org/10.1016/j.nutres.2008.02.004 (2008).
Kim, J. E., O’Connor, L. E., Sands, L. P., Slebodnik, M. B. & Campbell, W. W. Effects of dietary protein intake on body composition changes after weight loss in older adults: a systematic review and meta-analysis. Nutrition Reviews 74, 210–224 (2016).
de Wit, L. M., van Straten, A., van Herten, M., Penninx, B. W. J. H. & Cuijpers, P. Depression and body mass index, a u-shaped association. BMC Public Health 9, 14–14, https://doi.org/10.1186/1471-2458-9-14 (2009).
Sorkin, D. H., Biegler, K. A. & Billimek, J. Differences in Self-Reported Physical Activity and Body Mass Index Among Older Hispanic and Non-Hispanic White Men and Women: Findings from the 2009 California Health Interview Survey. Journal of the American Geriatrics Society 63, 2158–2163, https://doi.org/10.1111/jgs.13655 (2015).
Ding, D. et al. Neighborhood environment and physical activity among older adults: Do the relationships differ by driving status? Journal of aging and physical activity 22, 421–431, https://doi.org/10.1123/japa.2012-0332 (2014).
Weintraub, D., Oehlberg, K. A., Katz, I. R. & Stern, M. B. Test characteristics of the 15-item geriatric depression scale and Hamilton depression rating scale in Parkinson disease. Am J Geriatr Psychiatry 14, 169–175 (2006).
Pforr, K. femlogit-Implementation of the multinomial logit model with fixed effects. Stata Journal 14, 847–862 (2014).
Iwanuma C. Population 15 Years of Age and Over, by Marital Status (4 Groups), Age (Five-Year Groups), Sex, and Averaged Age, https://www.city.iwanuma.miyagi.jp/shisei/tokei/joho/documents/7haiguukankeidanjobetsujinkou.pdf (2010) [Japanese]Accessed May 6, 2017.
Iwanuma C. Population and Employed Persons 15 Years and Older, based on Place of Usual Residence and Place of Working or Schooling, by Age (Five-Year Groups) and Sex, https://www.city.iwanuma.miyagi.jp/shisei/tokei/joho/documents/23joujuuchimatahajuugyouchinojinnkou.pdf Accessed May 7, 2017 (2010).
Grandner, M. A., Schopfer, E. A., Sands-Lincoln, M., Jackson, N. & Malhotra, A. The Relationship between Sleep Duration and Body Mass Index Depends on Age. Obesity (Silver Spring, Md.) 23, 2491–2498, https://doi.org/10.1002/oby.21247 (2015).
Hikichi, H. et al. Residential relocation and change in social capital: A natural experiment from the 2011 Japan Earthquake and Tsunami. Science Advances 3, e1700426 (2017).
Santos-Eggimann, B., Cuénoud, P., Spagnoli, J. & Junod, J. Prevalence of Frailty in Middle-Aged and Older Community-Dwelling Europeans Living in 10 Countries. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences 64, 675–681, https://doi.org/10.1093/gerona/glp012 (2009).
Acknowledgements
We appreciate the support and cooperation of the Iwanuma Mayor’s office, and the staff of the Department of Health and Welfare of Iwanuma city government. This work was supported by a grant from the National Institutes of Health (R01 AG042463); Grants-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (KAKENHI 15H01972, KAKENHI 23243070, KAKENHI 22390400, KAKENHI 22592327 and KAKENHI 24390469); a Health Labour Sciences Research Grant from the Japanese Ministry of Health, Labour and Welfare (H22-Choju-Shitei-008, H24-Choju-Wakate-009 and H28-Chouju-Ippan-002); and a grant from the Strategic Research Foundation Grant-Aided Project for Private Universities from the Japanese Ministry of Education, Culture, Sports, Science and Technology (S0991035).
Author information
Authors and Affiliations
Contributions
H.H., J.A., K.K., T.T., I.K. conceived and designed the survey; H.H., J.A., K.K., T.T. performed the survey; H.H. analyzed the data; H.H. wrote the first draft of the manuscript; H.H., J.A., K.K., T.T., I.K. contributed to the writing of the manuscript. All authors agreed with manuscript results and conclusions.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hikichi, H., Aida, J., Kondo, K. et al. Residential relocation and obesity after a natural disaster: A natural experiment from the 2011 Japan Earthquake and Tsunami. Sci Rep 9, 374 (2019). https://doi.org/10.1038/s41598-018-36906-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-36906-y
This article is cited by
-
Association between sense of coherence and health and well-being among older survivors of a natural disaster: a prospective outcome-wide study
Scientific Reports (2023)
-
Post-Disaster Mental Health and Dietary Patterns among Older Survivors of an Earthquake and Tsunami
The Journal of nutrition, health and aging (2023)
-
Environmental risk factors of type 2 diabetes—an exposome approach
Diabetologia (2022)
-
Effect of temporary housing on incidence of diabetes mellitus in survivors of a tsunami-stricken area in 2011 Japan disaster: a serial cross-sectional RIAS study
Scientific Reports (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
