
Abstract
Magnetic resonance (MR) imaging is a powerful technique for non-invasive in-vivo imaging of the human brain. We employed a recently validated method for robust cross-sectional and longitudinal segmentation of MR brain images from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) cohort. Specifically, we segmented 5074 MR brain images into 138 anatomical regions and extracted time-point specific structural volumes and volume change during follow-up intervals of 12 or 24 months. We assessed the extracted biomarkers by determining their power to predict diagnostic classification and by comparing atrophy rates to published meta-studies. The approach enables comprehensive analysis of structural changes within the whole brain. The discriminative power of individual biomarkers (volumes/atrophy rates) is on par with results published by other groups. We publish all quality-checked brain masks, structural segmentations, and extracted biomarkers along with this article. We further share the methodology for brain extraction (pincram) and segmentation (MALPEM, MALPEM4D) as open source projects with the community. The identified biomarkers hold great potential for deeper analysis, and the validated methodology can readily be applied to other imaging cohorts.
Similar content being viewed by others

Introduction
Non-invasive magnetic resonance (MR) brain imaging can support the quantitative characterization of neurological conditions such as Alzheimer’s disease (AD). MR imaging can provide informative biomarkers even before clinical symptoms are apparent or irreversible neuronal damage has occurred1,2. The diagnostic potential of biomarkers based on structural imaging has been outlined by Frisoni et al.3 and Klöppel et al.4. Automatically extracted biomarkers can provide diagnostic decision support, increase objectivity in the disease assessment and improve differential diagnosis3,4,5,6. Another important avenue is the use of biomarkers for AD screening or for enrolling suitable participants for pharmaceutical trials4,7. Clinical trials can also benefit from MR biomarkers as they enable enrichment strategies8 or more rigorous inclusion criteria, leading to more homogeneous study groups1,2,3,4.
Subjects with mild cognitive impairment (MCI) do not fulfil the diagnostic criteria for AD9, but are at increased risk of developing AD10. Predicting conversion to AD is of particular importance to patients, clinicians and caregivers, but also for clinical trials4,9,10. An illustration of anatomical changes over a period of two years is shown in Fig. 1 for a healthy control (HC) subject, a progressive MCI (pMCI) subject converting to AD and a patient with AD. Modern neuroimaging can help to improve the accuracy of MCI diagnosis by adding positive predictive value when combined with other diagnostic criteria5,9,11,12. It is, however, uncertain whether information based on individual brain structures is sufficient to fully characterize the complex progression of AD or even to enable a differential dementia diagnosis7,13. Recent studies further suggest that structural MR imaging in combination with other diagnostic procedures, such as positron emission tomography (PET) or chemical analysis of cerebrospinal fluid (CSF), can detect pathological AD-related change years before the onset of AD dementia3,14. Many studies have shown that with progression of the disease, there is significant atrophy in structures of the medial temporal lobe (MTL) such as the hippocampus, amygdala, and entorhinal and parahippocampal cortices4,15,16,17. In the future, structural MR imaging will thus play an important role not only in the diagnosis of AD, but also in monitoring its treatment2,3,4. The development of automatic, robust, quantitative techniques to assess MR images of the brain is therefore an important factor to further increase the utility of structural imaging in the context of neurocognitive disorders.

Three examples of MR images (brain-extracted) of subjects from the ADNI1 cohort in coronal section. Top row: a healthy control subject (male, 84.8 years at baseline); middle row: MCI subject (female, 71.8 year at baseline) who converted to AD after three years; bottom row: an AD patient (male, 77.5 years at baseline). Left: baseline; middle: 2-year follow-up; right: baseline with overlaid difference image of rigidly aligned images (blue: volume loss/atrophy, red: positive volume change). The differences are visually subtle, but the increased atrophy in the medial temporal lobe and the enlarged ventricles are apparent in the difference image.
A vast number of studies have shown correlations between quantitative measures calculated from brain MR images with AD progression. Automatic methods perform similarly to trained radiologists when classifying MR images of patients with AD5. There is strong evidence that different anatomical brain structures are affected at different stages of the disease18, with early involvement of the hippocampus, amygdala and entorhinal cortex consistently shown in the literature9,15,17. Although sensitive to dementia, these markers may yet not be sufficiently specific to AD3,12. A uniform approach that considers pathological changes of multiple structures within the whole brain promises to increase specificity in dementia diagnosis and to support differential assessment of various types of dementia3,13. It is thus desirable to follow a holistic approach and to analyse a large number of structures of the whole brain rather than only a limited selection of brain structures. Due to its early involvement in dementia, the focus of many published methods lies on the segmentation of the hippocampus to quantify its volume or shape11,18,19,20,21,22,23,24,25,26,27,28,29. Grey matter (GM) tissue maps10,13 and cortical thickness have also been shown to be of high predictive value in the context of AD12,30. Other approaches are based on voxel-based morphometry (VBM)31, deformation-based morphometry (DBM)32, or tensor-based morphometry (TBM)33 to study group differences. In general, methods exploring the whole brain outperform those focusing on individual structures such as the hippocampus12,34.
Many studies have shown that biomarkers of morphometry, such as volume or shape, correlate with AD progression. However, intersubject variability can lead to substantial overlap with the healthy population and thus limit the discriminative power of these features21. Temporal change of the whole brain or individual structures tends to be more consistent between subjects. Atrophy rates are usually given as a percentage per year. Popular approaches rely on 3D + t optimization using graph cuts22, expectation maximization35, or the boundary shift integral21,23,36. The measurable increase in GM atrophy in patients with AD is a consequence of a substantially accelerated, regionally selective loss of neurons20,37. Most of the published studies can, however, only be compared qualitatively. In many cases, different features, a different methodology to extract the features and different classification techniques are used7. In addition, methods are applied to different cohorts or different subsets thereof. Most studies lack histopathologically confirmed ground truth diagnoses. Instead of seeing subjects as being either healthy or diseased, the diagnosis of AD is a dynamic process in which biomarkers gradually begin to change before current diagnosis criteria are met38,39,40,41,42,43,44. Advances in machine learning, e.g. Gaussian process modelling, have also introduced novel opportunities for personalized healthcare, shifting from “one-size-fits-all” population modeling towards personalized models45,46,47,48.
Of particular importance for routine use in clinical practice is the interpretability of biomarkers7. Many recently developed methods rely heavily on machine learning techniques, e.g. learned manifolds34,49, multiple instance learning50, or region grading51. Even though these methods are often highly accurate, the interpretation of their results can be difficult, and this impedes their adoption into clinical practice. Thus, it is desirable to calculate biomarkers that are easy to interpret, but at the same time as informative as features obtained through such sophisticated machine learning techniques. A further overview can be found in numerous surveys1,3,7,12,52.
In this manuscript we employ multi-atlas label propagation with expectation-maximisation based refinement (MALPEM)53, a state-of-the-art automatic segmentation method for robust segmentation of whole-brain MR images into 138 distinct anatomical structures. Johnson et al.54 recently validated a number of established segmentation methods (SPM31,55, ANTs Atropos56, MALP-EM53,57, FSL FAST58, FreeSurfer59) in the context of Huntington’s disease and found that “MALP-EM appeared to be the most visually accurate tool, […]”. In 2015, an entry based on MALPEM won a third prize in the CADDementia disease classification challenge held in conjunction with MICCAI52. We applied MALPEM to a set of 5074 images of the Alzheimer’s Disease Neuroimaging Initiative (ADNI) cohort with the goal to identify biomarkers that characterize the whole brain, specifically structural volumes and atrophy rates. Our main contributions are:
-
We confirm the accuracy and robustness of MALPEM/MALPEM4D in a cross-sectional/longitudinal study based on a large number of images from the ADNI database.
-
We assess the quality of extracted biomarkers with a clear clinical interpretation (volumes/atrophy rates) and show that their discriminative value is on par with published literature in the context of AD.
-
We share the employed methodology for brain extraction (pincram) and segmentation (MALPEM, MALPEM4D) as open source projects. The validated methodology can readily be applied to other imaging cohorts.
-
We share quality-checked brain masks, structural segmentations and extracted biomarkers for 5074 ADNI images with the community. This resource holds great potential for a deeper analysis and enables training of sophisticated model-based approaches by interested research groups.
Results
Cross-sectional analysis
In a cross-sectional analysis, we investigated the potential to discriminate AD disease stages based on the volumes of individual brain regions. An example segmentation result of a healthy control subject and a patient diagnosed with AD is shown in Fig. 2. The distribution of the measured s of six selected structures is shown in Fig. 3 for the four disease groups: HC, stable MCI (sMCI), pMCI and AD. The reduced GM volume of structures in the medial temporal lobe and the increased ventricular volume in patients with AD is apparent. All cross-sectional volumetric measurements were corrected for the nuisance variables subject age, gender, and intracranial. In the following, these corrected volumes will be employed to investigate their potential to classify relevant disease stages in AD.

Example cross-sectional segmentation results of a patient diagnosed with AD (ADNI_018_S_0286, male, 66 years of age) in axial (left), coronal (middle) and sagittal (right) view-plane.

Boxplots of structural volumes at baseline for six selected structures before correcting for nuisance factors for distinct disease groups. Structures were selected based on their performance in classifying the investigated disease groups (c.f. Table 1).
Disease classification using structural volumes
An overview of the results of the classification experiments is given in Table 1. The volume of the amygdala allows the strongest distinction between AD and HC with an effect size (Cohen’s d) of 1.56 and a balanced classification accuracy (bACC) of 80%, a sensitivity (SENS) of 76% and a specificity (SPEC) of 84%. Other structures in the MTL region such as the hippocampus (bACC: 78%) or the entorhinal area (bACC: 78%) were similarly discriminative (d > 1.5). Established findings that total brain volume, and cortical grey matter in particular, are smaller in patients with AD were confirmed in our experiments. Accuracy was further improved by combining all structural volumes as features in a support vector machine (SVM; bACC: 89%, SENS: 86%, SPEC: 92%) or random forest (RF; (bACC: 86%, SENS: 83%, SPEC: 90%). As indicated in Table 1, numerous structural differences were highly significant even after Bonferroni correction for multiple comparisons. The structural volumes of the amygdala (bACC: 65%, SENS: 63%, SPEC: 68%) and inferior lateral ventricle (bACC: 64%, SENS: 54%, SPEC: 74%) were most discriminative for the classification of pMCI vs. sMCI. Combining all extracted structural volumes into a single RF classifier further increased classification accuracies (bACC: 68%, SENS: 72%, SPEC: 64%). The classification results for all structures can be found in the supplementary material.
Longitudinal analysis
In a further longitudinal analysis we investigate the volume change of individual anatomical regions with respect to disease stage. Atrophy was measured for the month-12 (m12) or month-24 (m24) follow-up images with respect to their corresponding baseline (bl) images. In the following, we show atrophy rates with their corresponding sample sizes as well as discriminative power to distinguish between disease stages. Sections from an example segmentation obtained on a subject diagnosed with AD are shown in Fig. 4.

Example longitudinal segmentation results of baseline (left) and month 24 (middle) follow-up images of a patient diagnosed AD (ADNI_018_S_0286) in coronal section. Substantial hippocampal atrophy (measured: −7.81%) and ventricular enlargement (16.5%) are apparent in the difference image after affine registration (right).
Atrophy rates and sample sizes
Atrophy rates for selected structures can be found in Table 2 as well as in Table 3 for AD/HC and in Table 4 for pMCI/sMCI. The distribution of the volume change of six selected structures is shown in Fig. 5 for the four investigated clinical groups (HC, sMCI, pMCI and AD). In AD patients, GM structures such as the hippocampus (HC: −1.1%, AD: −4.8%) or the medial temporal gyrus (HC: −1.1%, AD: −3.8%) are subject to significant volume loss between baseline and m12. Concurrently, ventricles expand rapidly in AD patients (HC: 2.8%, AD: 7.2%). Overall, sMCI subjects show atrophy patterns similar to HC, while atrophy patterns in MCI subjects converting to AD are similar to those in AD patients. The amount of atrophy measured between the baseline and m24 are on the order of twice those measured between baseline and m12. The results indicate that the atrophy rate in the entorhinal region is slightly higher in pMCI subjects than in patients with AD. A volume change rate of −4.0% (±3.7) for pMCI subjects and −3.7% (±4.1) for AD patients was measured at m12. Respectively, a volume change rate of −7.4% (±4.7) for pMCI subjects and −7.0% (±5.5) for AD patients was measured at m24.

Based on the atrophy rates, sample sizes were calculated to detect a 25% change in atrophy rate with 80% power at a 5% significance level. The atrophy rates and sample sizes for selected structures are shown in Table 2. The smallest sample sizes (corrected for normal aging) were computed for the inferior lateral ventricles with 228 subjects for bl → m12 and 126 subjects for bl → m24. The measured atrophy rates of other structures such as the hippocampus or the medial temporal gyrus yielded sample sizes at a similar level. Atrophy rates for all investigated structures can be found in the supplementary material.
Disease classification using structural volume change
We further investigated the potential of structural atrophy rates to distinguish between the clinical groups AD vs. HC and pMCI vs. sMCI. P-values, effect sizes and classification accuracies were calculated to quantify group separation. The results are shown in Table 3 (AD vs. HC) and Table 4 (pMCI vs. sMCI).
The most discriminative structure to distinguish between AD and HC was the hippocampus (dm12 = 1.40, dm24 = 1.88). Based on m12 atrophy a bACCm12 of 78% (SENS: 67%, SPEC: 88%) was calculated, for m24 atrophy a balanced accuracy of 85% respectively. Combining all derived atrophy features in a RF classifier substantially increased classification results to bACCm12: 84%; bACCm24: 88%. Hippocampal atrophy was also a very good feature for classifying progressive versus stable MCI subjects: bACCm12: 67%; bACCm24: 74%. However, the highest individual classification accuracy was obtained at m12 for the medial temporal gyrus (bACCm12: 70%, SENS: 65%, SPEC: 75%) and the inferior lateral ventricles (bACCm12: 69%, SENS: 63%, SPEC: 75%). Over 24 months, atrophy in the fusiform gyrus was most informative for classifying MCI subjects (bACCm24: 76%). Exploiting all available longitudinal features in an RF classifier increased MCI classification accuracy to bACCm12: 73%; bACCm24: 78%. Ventricular enlargement is more discriminative than a reduction in brain tissue for both AD versus HC and pMCI versus sMCI classification. An overview over all considered features and their individual classification performance can be found in the supplementary material.
Discussion
In this study, sets of 1069 baseline, 802 m12, and 532 m24 follow-up images from the ADNI-1/-GO/-2 cohort were analyzed. Considering the size and heterogeneity of the database, we expect our findings to be applicable to other cohorts.
A selection of articles is listed in Table 5 to present our classification results in the context of those reported in the literature. When comparing results to other studies it must be noted that these did not use identical data subsets from the ADNI cohorts. A further potential confounding factor is the definition of the sMCI and pMCI disease groups. In our study, the stratification of MCI subjects in sMCI and pMCI is well-defined. However, this definition is not identical across published studies.
Our cross-sectional classification results are very similar to those presented in Wolz et al.34, which are based on the ADNI-1 cohort. Wolz et al.34 classified AD vs. HC (bACC: 89%, SENS: 93%, SPEC: 85%) and pMCI vs. sMCI (bACC: 68%, SENS: 67%, SPEC: 69%) based on a multitude of features, including more abstract criteria derived from TBM and manifold-learning based methods. Other studies report even higher classification results of up to bACC: 92.4% for AD vs. HC and bACC: 74.0% for pMCI vs. sMCI classification60. Unlike our study, most studies shown in Table 5 analyzed the 1.5 Tesla (T) images of ADNI-1 only. Also usually more complex features such as cortical features34,60,61,62, textural features63, manifold-based features34,61 or grading based features28 are employed. In summary, the results presented in this study are comparable to the state of the art. This is encouraging, as we analyzed a large and heterogeneous dataset acquired at both 1.5T and 3T using structural volumes only, which are features with clear biological interpretations. Furthermore, structures that were found to be most discriminative agree well with those highlighted in Fennema et al.2. Examples are the hippocampus, amygdala, entorhinal area, and regions within the temporal gyrus in general.
Based on hippocampal atrophy alone a bACCm12 of 78% and bACCm24 of 85% was calculated for classifying AD vs. HC. These results are similar to those obtained on a different ADNI subset with a method dedicated to hippocampal atrophy measurement22: bACCm12 of 82% (SENS: 81%, SPEC: 83%); bACCm24 of 86% (SENS: 85%, SPEC: 87%). The results for AD vs. HC classification using all longitudinal features are also on par with those using all structural volumes at baseline. However, classification accuracies substantially above 90% were not expected due to potential bias in the study data caused, for example, by diagnostic misclassification, variations in scanner type and field strength, as well as possible remnant differences between participating centres that even strict protocols such as ADNI’s cannot prevent. Using longitudinal information available at the month 24 follow-up visit increased accuracy for classifying sMCI vs. pMCI groups from 68% at baseline to 78%. This confirms the discriminative value of higher structural atrophy rates in MCI subjects who progress to AD. Unlike in patients with AD, atrophy in MCI subjects has not yet manifested itself in substantially reduced structural volumes at baseline.
In Barnes et al.64 the authors concluded in a large meta-analysis that the annualized hippocampal volume change of healthy elderly people is −1.4% compared with −4.6% for patients with AD. Our results are similar: −1.1% (±1.7) for HC and −4.8% (±3.7) for AD subjects. A mean change of −0.5% (±0.8) and −1.3% (±1.1) from bl to m12 was observed for HC and AD groups for brain tissue. These results are also in line with previously published annual brain volume change rates of around −0.6% for controls and −1.5% for AD patients65. This confirms that the employed methodology yields realistic atrophy measurements on individual structures, while providing a comprehensive overview of structural change throughout the whole brain.
For the four structures hippocampus, amygdala, inferior lateral ventricle, and lateral ventricle, their respective counterparts in the left/right brain hemisphere were analyzed separately. The results suggest that structural change in the left hippocampus is slightly more discriminative than change in the right hippocampus. There is no consistent trend for the other investigated structures. In general, features of left-right paired structures perform similarly for all investigated structures and combining them seems, in summary, beneficial.
The use of either SVM or RF classifiers provided substantial improvements over the results obtained using individual features only. Overall SVM and RF performed similarly, with slight advantages for one or the other in individual experiments.
Our experiments confirm that MALPEM is an accurate and sensitive approach for brain image analysis. One of MALPEM’s main advantages is that it delivers a full morphometric analysis of all of 138 structures, unlike specialized methods that only work on a small selected set of individual structures. Another important strength is that our methods allow both the accurate analysis of single images (MALPEM) as well as image series (MALPEM4D). Thus, the presented methodology has strong potential to support both cross-sectional and longitudinal studies that include MR imaging of the brain.
As part of this work, we created a morphometry database of unprecedented size and accuracy, which we share with the community. This database provides pincram brain extractions and MALPEM segmentations of 5074 MR images, as well as longitudinal features extracted from 1334 MR image series. In previous work, we shared a database built on images from ADNI-166. The present development differs from this past effort in important ways that reflect developments of ADNI (data from ADNI-2 and ADNI-GO became available in the meantime) as well as software improvements (MALPEM yields more accurate segmentations than the MAPER method67 used in the previous project). The previous database was substantially smaller and contained only cross-sectional data (996 baseline and screening images). Another difference is in the atlas database chosen: compared to the atlases used for the previous resource68,69, the NMM atlases offer more detailed cortical subdivisions.
We anticipate that our new morphometry database will be an immensely valuable resource for future research on classification and modeling approaches. It can further enable the optimization of training-data intense deep learning methodologies.
Methods
Materials
For this study a subset of T1-weighted (T1w) MR brain images was analyzed from all studies by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) for which data are currently available (ADNI-1/-GO/-2). The ADNI was launched in 2003 as a public-private partnership, led by Principal Investigator Michael W. Weiner, MD. ADNI enrols participants between the ages of 55 and 90 who are recruited at 57 sites in the United States and Canada. After obtaining informed consent, participants undergo a series of initial tests that are repeated at intervals over subsequent years, including a clinical evaluation, neuropsychological tests, genetic testing, lumbar puncture, and MRI and PET scans. Participants were studied under ADNI protocols that were approved by the Institutional Review Board (IRB) at each recruitment site. A listing of sites with named Site Investigators can be found online at https://adni.loni.usc.edu/wp-content/uploads/how_to_apply/ADNI_Acknowledgement_List.pdf (last accessed 30 June 2018). ADNI procedures manuals were developed as a resource for ADNI research sites. They are tailored to site Study Coordinator and support staff. The ADNI MRI Technical Procedures manuals are developed by the ADNI Imaging Core to direct MRI technicians in the scanning of ADNI subjects. For further details and up-to-date information please refer to the supplementary material and http://www.adni-info.org (last accessed 15 March 2018). All methods described in this study were performed in accordance with relevant guidelines and regulations. When the present study was started, we retrieved clinical information and corresponding MR images based on the ADNIMERGE package. Specifically, 5074 (1674 baseline, 3400 follow-up) images were processed with MALPEM. Subjects had been scanned up to 10 times, with the last follow-up image acquired 8 years after the baseline. For the present analysis, a subset of these 5074 processed images was selected based on clinical information. We applied the following criteria for inclusion/exclusion of individual subjects:
-
All subjects who reverted at any time point from a more severe to a less severe disease stage, i.e. AD → MCI or MCI → HC, were excluded from both the cross-sectional (N = 68) and the longitudinal analysis.
-
All subjects with baseline diagnosis early MCI (N = 277) or SMC (N = 76) were excluded from both the cross-sectional and the longitudinal analysis.
-
The sMCI group was defined as those subjects who were diagnosed as MCI (called ‘late MCI’ in ADNI-GO/-2) at baseline and remained at the MCI stage for at least two years and until the most recent diagnosis which was available. This means that subjects for whom this information was not available, e.g. because the repository did not contain a corresponding m24 or later visit, were excluded (N = 130).
-
The pMCI group was defined as those subjects who were diagnosed as MCI at baseline and converted within two years follow-up to a diagnosis of probable AD.
-
Subjects who were diagnosed as MCI at baseline but converted to probable AD more than two years later (N = 54) were excluded from the analyses and neither considered as sMCI nor pMCI.
-
The m12 image (I373205) of one subject (ADNI_007_S_4568) was reviewed after irregular volume measurements and excluded manually from the analysis due to poor image quality.
-
All subjects listed in Table 6 fulfil the above criteria. For the longitudinal analysis, however, all subjects that converted at any time of the study from HC to a symptomatic stage (e.g. to MCI or even to AD) were excluded (N = 52).
Table 6 gives an overview over the baseline images considered in the conducted analyses. Note that this is a well-defined subset of all 5074 images processed. Lists of the processed filenames that also include the unique image identifier are available online at https://doi.org/10.12751/g-node.aa605a70.
Preprocessing
As preprocessed versions of the images were downloaded from ADNI, no additional preprocessing was performed71. Brain masks were calculated for all available baseline images using pincram57. Brain masks were visually reviewed and some were recalculated with an updated pincram atlas database. Follow-up images were brain-extracted utilizing the corresponding baseline brain masks, which were transformed using rigid intrasubject registration.
Cross-sectional and longitudinal segmentation
All 5074 baseline and follow-up images were segmented individually using MALPEM as described in Ledig et al.53. As the atlas database, we used the manually annotated Neuromorphometrics (NMM) brain atlases (n = 30; provided by Neuromorphometrics, Inc. under academic subscription, http://Neuromorphometrics.com/, last accessed 15 March 2018). The atlas label sets contain expert delineations of 40 non-cortical and 98 cortical brain regions. A description of the individual structures is provided in the supplementary material. MALPEM was recently validated in an independent study led by Johnson et al.54 where the authors compared state-of-the-art segmentation methods in the context of Huntington’s disease. The refined, time-point specific probabilistic segmentation output and the intensity-normalized, brain-extracted images of MALPEM are then employed to perform the consistent longitudinal segmentation as described in Ledig et al.35 (MALPEM4D). MALPEM4D is an approach that employs spatially and temporally varying coupling weights between time points to obtain temporally consistent segmentation estimates. In this work, MALPEM4D incorporates symmetric affine intra-subject registration72,73 and corrects for differential bias between intra-subject acquisitions using unweighted differential bias correction74. MALPEM4D is run on pairs of images to separately estimate volume changes bl → m12 and bl → m24.
Features and classification
For the cross-sectional analysis at baseline, structural volumes were calculated with MALPEM and not MALPEM4D, as the latter exploits information of later scanning time points, which was not available at baseline. For the longitudinal analysis structural volumes were extracted based on the respective MALPEM4D segmentations.
As features, all available structural volumes were employed. For paired structures, the left and right volumes were merged (98/2 = 49 cortical plus 28/2 + 7 = 21 non-cortical features). Note that seven non-cortical structures are unpaired (3rd ventricle, 4th ventricle, brainstem, CSF, cerebellar vermal lobules I–V, cerebellar vermal lobules VI–VII, and cerebellar vermal lobules VIII–X). Exceptions were made for the amygdala, hippocampus, inferior lateral ventricles, and lateral ventricles. As it is expected that these structures are particularly informative, their left and right volumes were retained as separate features (8 features). This allowed us to investigate asymmetric involvement of these structures in the disease progression. Individual structures were further summarized as ventricles, cortical grey matter, deep grey matter, white matter, brain tissue and total brain volume (brain tissue including ventricles/CSF) (6 features). In total 86 features were considered, including age and gender.
For classification, a 6-fold cross-validation (CV) was performed using an linear discriminant analysis (LDA) classifier for individual features. When combining multiple features, both SVM and RF classifiers were employed. A classification framework was implemented using MATLAB (The MathWorks Inc, Natick, MA, USA) that relies on classify (LDA), TreeBagger (RF, 100 trees) and libSVM (linear SVM75). Features were normalized (rescaled) individually to a range from 0 to 1 for the SVM classification. In addition to the standard classification accuracy (ACC), we also quantified the balanced classification accuracy (bACC76) to account for imbalanced group sizes. The bACC is calculated as the arithmetic mean of SENS and SPEC.
Significance levels were quantified as p-values of two-sided, unpaired Student’s t-tests. We employed the conservative Bonferroni correction to correct for multiple comparisons. Further, effect sizes were calculated as Cohen’s d by dividing the differences of the sample means (absolute value) by their pooled standard deviation2,77,78. According to Cohen77 an effect size of d = 0.2 can be considered as small, of d = 0.5 as medium and of d = 0.8 as large. Reporting the effect size in addition to the p-value is important as it quantifies the magnitude of a group difference, while a low p-value by itself only confirms its existence79.
Correction for nuisance factors
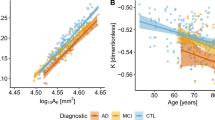
The volume of many individual brain structures diminishes during the course of normal, healthy aging. Also, strong correlations between structural volumes and overall head size are well established80. This is illustrated in Fig. 6, where linear regressors are fit to hippocampal volumes with respect to age, gender, and brain volume based on the processed HC subjects.

Top: Dependence of hippocampal volume on age (left), gender (middle) and brain volume (right). Bottom: Corresponding s corrected for nuisance factors age, gender and brain size. Overlaid regression lines for distinct disease groups with corresponding regression lines.
We followed a multiple linear regression approach as described in Koikkalainen et al.81 and investigated the nuisance factors age, gender and brain size. Specifically, a separate linear regressor was fit using the processed healthy control subjects for each individual structure and the abovementioned predictor variables. Each multivariate regressor is defined by the slope for each predictor cage, cgender and csize and an intercept b. Assuming M distinct features, feature m of subject n, denoted by \({{F}_{n}}^{m}\), is corrected as:
To correct for head size, the total brain size (sum of all structures) was used as an approximation of the intracranial volume. This is a commonly used approximation80.
The effect of correcting for the nuisance factors patient age, gender and head size is shown in Table 7. The correction substantially increased classification accuracies and effect sizes obtained on individual structures. The benefit of the correction for all investigated structures, including effect sizes, can be found in the supplementary material.
The observed benefit of correcting for these confounding factors is in agreement with the literature81. In the conducted experiment, correcting for brain size had the biggest effect and correcting for gender had a stronger impact than correcting for age. Correcting for all three nuisance factors (age, gender and brain size) was most beneficial in terms of both classification accuracy and effect size.
An illustration of the volumes before and after correction is provided in Fig. 6. Healthy control subjects have zero mean after correction, and the overall dependence on nuisance factors is clearly reduced.
The corrected volumes were used for the cross-sectional analysis. This means that feature values are no longer actual volumes, but rather volume differences with respect to a healthy population of matched age, gender and brain size. Note that the three independent variables patient age, gender, and head size were not corrected for.
Calculation of atrophy rates and sample sizes
For a volume \({v}_{{t}^{1}}\) at baseline and a volume \({v}_{{t}^{2}}\) at a follow-up time point we calculated atrophy rates using the logarithmic transform as \({{\rm{\Delta }}}_{v}({t}^{1},{t}^{2})={{\rm{\Delta }}}_{v}^{\mathrm{log}}({t}^{1},{t}^{2})=\)\(\mathrm{ln}({v}_{{t}^{2}}/{v}_{{t}^{1}})\cdot \mathrm{100 \% }\). Note that atrophy rate and volume change is used interchangeably, which means that a positive atrophy rate indicates an increase in volume.
For a power (1 − β) and significance level α the sample size can be calculated23 as:
Here Δ is the difference in atrophy rate that is to be shown between the clinical groups. In this study sample sizes were calculated to detect a 25% change in atrophy rate (Δ = 0.25 μg) with 80% power (z0.8 ≈ 0.84) at a 5% significance level (z1−0.05/2 ≈ 1.96). These parameter choices are commonly found in the literature22,23,72. It is important to relate atrophy rates in dementia to normal atrophy during aging, as in the uncorrected case it is assumed that 100% treatment effect would effectively reduce the structural atrophy to zero23. Sample sizes were thus corrected for normal ageing by evaluating Equation 2 with Δ = 0.25(μg−μhealthy) to reduce the maximal treatment effect to the level of normal ageing. In Equation 2 it is assumed that measurements of healthy atrophy have the same variance as measurements of diseased subjects (σg ≈ σhealthy)23. This usually leads to a more conservative estimate.
Data availability
The datasets generated during and/or analyzed in this study are available online (all resources last accessed 15 March 2018).
-
The source code of pincram57 and the MALPEM framework53 is available at https://github.com/ledigchr/MALPEM, the MIRTK source for the involved binaries is available at https://github.com/BioMedIA/MIRTK.
-
The binary brain masks (pincram) and structural segmentations (MALPEM) for 5074 images from the ADNI cohort are available for download at https://doi.org/10.12751/g-node.aa605a70.
-
All extracted features and selected clinical information (e.g. disease labels) are also available at https://doi.org/10.12751/g-node.aa605a70.
References
Scheltens, P., Fox, N. C., Barkhof, F. & De Carli, C. Structural magnetic resonance imaging in the practical assessment of dementia: beyond exclusion. The Lancet Neurology 1, 13–21 (2002).
Fennema-Notestine, C. et al. Structural MRI biomarkers for preclinical and mild Alzheimer’s disease. Human Brain Mapping 30, 3238–3253 (2009).
Frisoni, G. B., Fox, N. C., Jack, C. R., Scheltens, P. & Thompson, P. M. The clinical use of structural MRI in Alzheimer disease. Nature Reviews Neurology 6, 67–77 (2010).
Klöppel, S. et al. Diagnostic neuroimaging across diseases. NeuroImage 61, 457–463 (2012).
Klöppel, S. et al. Accuracy of dementia diagnosis–a direct comparison between radiologists and a computerized method. Brain 131, 2969–2974 (2008).
Heckemann, R. et al. Automatic try on MR brain images can support diagnostic decision making. BMC Medical Imaging 8, 9 (2008).
Falahati, F., Westman, E. & Simmon, A. Multivariate data analysis and machine learning in Alzheimer’s disease with a focus on structural magnetic resonance imaging. Journal of Alzheimer’s Disease 41, 685–708 (2014).
Sevigny, J. et al. Aducanumab (BIIB037), an anti-amyloid beta monoclonal antibody, in patients with prodromal or mild Alzheimer’s disease: interim results of a randomized, double-blind, placebo-controlled, phase 1b study. Alzheimer’s & Dementia 11, P277 (2015).
Dubois, B. et al. Research criteria for the diagnosis of Alzheimer’s disease: revising the NINCDS-ADRDA criteria. The Lancet Neurology 6, 734–746 (2007).
Davatzikos, C., Bhatt, P., Shaw, L. M., Batmanghelich, K. N. & Trojanowski, J. Q. Prediction of MCI to AD conversion, via MRI, CSF biomarkers, and pattern classification. Neurobiology of Aging 32, 2322.e19–2322.e27 (2011).
Colliot, O. et al. Discrimination between Alzheimer disease, mild cognitive impairment, and normal aging by using automated segmentation of the hippocampus. Radiology 248, 194–201 (2008).
Cuingnet, R. et al. Automatic classification of patients with Alzheimer’s disease from structural MRI: a comparison of ten methods using the ADNI database. NeuroImage 56, 766–781 (2011).
Klöppel, S. et al. Automatic classification of MR scans in Alzheimer’s disease. Brain 131, 681–689 (2008).
Sperling, R. A. et al. Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s & Dementia 7, 280–292 (2011).
Braak, H. & Braak, E. Neuropathological stageing of Alzheimer-related changes. Acta Neuropathologica 82, 239–259 (1991).
Jack, C. R. Jr. et al. Brain beta-amyloid measures and magnetic resonance imaging atrophy both predict time-to-progression from mild cognitive impairment to Alzheimer’s disease. Brain 133, 3336–3348 (2010).
Klein-Koerkamp, Y. et al. Amygdalar atrophy in early Alzheimer’s disease. Current Alzheimer Research 11, 239–252 (2014).
Dickerson, B. C. et al. MRI-derived entorhinal and hippocampal atrophy in incipient and very mild Alzheimer’s disease. Neurobiology of Aging 22, 747–754 (2001).
Fox, N. C. et al. Presymptomatic hippocampal atrophy in Alzheimer’s disease. Brain 119, 2001–2007 (1996).
Wang, L. et al. Changes in hippocampal volume and shape across time distinguish dementia of the Alzheimer type from healthy aging. NeuroImage 20, 667–682 (2003).
Barnes, J. et al. A comparison of methods for the automated calculation of s and atrophy rates in the hippocampus. NeuroImage 40, 1655–1671 (2008).
Wolz, R. et al. Measurement of hippocampal atrophy using 4D graph-cut segmentation: application to ADNI. NeuroImage 52, 109–118 (2010).
Leung, K. K. et al. Automated cross-sectional and longitudinal hippocampal volume measurement in mild cognitive impairment and Alzheimer’s disease. NeuroImage 51, 1345–1359 (2010).
Shen, D., Moffat, S., Resnick, S. M. & Davatzikos, C. Measuring size and shape of the hippocampus in MR images using a deformable shape model. NeuroImage 15, 422–434 (2002).
Chupin, M. et al. Fully automatic hippocampus segmentation and classification in Alzheimer’s disease and mild cognitive impairment applied on data from ADNI. Hippocampus 19, 579–587 (2009).
Lötjönen, J. M. et al. Fast and robust multi-atlas segmentation of brain magnetic resonance images. NeuroImage 49, 2352–2365 (2010).
Wolz, R., Aljabar, P., Hajnal, J. V., Hammers, A. & Rueckert, D. LEAP: learning embeddings for atlas propagation. NeuroImage 49, 1316–1325 (2010).
Coupé, P. et al. Scoring by nonlocal image patch estimator for early detection of Alzheimer’s disease. NeuroImage: Clinical 1, 141–152 (2012).
Tong, T., Wolz, R., Coupé, P., Hajnal, J. V. & Rueckert, D. Segmentation of MR images via discriminative dictionary learning and sparse coding: Application to hippocampus labeling. NeuroImage 76, 11–23 (2013).
Eskildsen, S. F. et al. Prediction of Alzheimer’s disease in subjects with mild cognitive impairment from the ADNI cohort using patterns of cortical thinning. NeuroImage 65, 511–521 (2013).
Ashburner, J. & Friston, K. J. Voxel-based morphometry - the methods. NeuroImage 11, 805–821 (2000).
Ashburner, J. & Friston, K. Nonlinear spatial normalization using basis functions. Human Brain Mapping 7, 254–266 (1999).
Koikkalainen, J. et al. Multi-template tensor-based morphometry: application to analysis of Alzheimer’s disease. NeuroImage 56, 1134–1144 (2011).
Wolz, R. et al. Multi-method analysis of MRI images in early diagnostics of Alzheimer’s disease. PLoS ONE 6, e25446 (2011).
Ledig, C. et al. Consistent and robust 4D whole-brain segmentation: application to traumatic brain injury. IEEE International Symposium on Biomedical Imaging: From Nano to Macro (ISBI) 673–676 (2014).
Freeborough, P. & Fox, N. C. The boundary shift integral: an accurate and robust measure of cerebral changes from registered repeat MRI. IEEE Transactions on Medical Imaging 16, 623–629 (1997).
Bobinski, M. et al. Neurofibrillary pathology - correlation with hippocampal formation atrophy in Alzheimer disease. Neurobiology of Aging 17, 909–919 (1996).
Schmidt-Richberg, A. et al. Multi-stage biomarker models for progression estimation in Alzheimer’s Disease. vol. 9123 of Lecture Notes in Computer Science, 387–398 (Springer International Publishing, 2015).
Schmidt-Richberg, A. et al. Learning biomarker models for progression estimation of Alzheimer’s disease. PloS one 11, e0153040 (2016).
Guerrero, R. et al. Instantiated mixed effects modeling of Alzheimer’s disease markers. NeuroImage 142, 113–125 (2016).
Ito, K. & Hutmacher, M. M. Predicting the time to clinically worsening in mild cognitive impairment patients and its utility in clinical trial design by modeling a longitudinal clinical dementia rating sum of boxes from the ADNI database. Journal of Alzheimer’s disease: JAD 40, 967–79 (2014).
Donohue, M. C. et al. Estimating long-term multivariate progression from short-term data. Alzheimer’s & dementia: the journal of the Alzheimer’s Association 10, S400–10 (2014).
Gavidia-Bovadilla, G. et al. Early prediction of Alzheimer’s disease using null longitudinal model-based classifiers. PloS one 12, e0168011 (2017).
Zhu, F. et al. Compass: A computational model to predict changes in mmse scores 24-months after initial assessment of Alzheimer’s disease. Scientific reports 6 (2016).
Ziegler, G. et al. Individualized gaussian process-based prediction and detection of local and global gray matter abnormalities in elderly subjects. Neuroimage 97, 333–348 (2014).
Lorenzi, M., Filippone, M., Frisoni, G. B., Alexander, D. C. & Ourselin, S. Probabilistic disease progression modeling to characterize diagnostic uncertainty: application to staging and prediction in Alzheimer’s disease. NeuroImage (2017).
Lorenzi, M. et al. Disentangling normal aging from Alzheimer’s disease in structural magnetic resonance images. Neurobiology of aging 36, S42–S52 (2015).
Hyun, J. W. et al. Stgp: Spatio-temporal gaussian process models for longitudinal neuroimaging data. Neuroimage 134, 550–562 (2016).
Guerrero, R., Wolz, R., Rao, A. W. & Rueckert, D. Manifold population modeling as a neuro-imaging biomarker: application to ADNI and ADNI-GO. NeuroImage 94, 275–286 (2014).
Tong, T. et al. Multiple instance learning for classification of dementia in brain MRI. Medical Image Analysis 18, 808–818 (2014).
Tong, T. et al. A novel grading biomarker for the prediction of conversion from mild cognitive impairment to Alzheimer’s disease. IEEE Transactions on Biomedical Engineering 64, 155–165 (2017).
Bron, E. E. et al. Standardized evaluation of algorithms for computer-aided diagnosis of dementia based on structural MRI: the CADDementia challenge. NeuroImage 111, 562–579 (2015).
Ledig, C. et al. Robust whole-brain segmentation: application to traumatic brain injury. Medical Image Analysis 21, 40–58 (2015).
Johnson, E. B. et al. Recommendations for the use of automated gray matter segmentation tools: Evidence from huntington’s disease. Frontiers in Neurology 8, 519 (2017).
Ashburner, J. & Friston, K. J. Unified segmentation. NeuroImage 26, 839–851 (2005).
Avants, B. B., Tustison, N. J., Wu, J., Cook, P. A. & Gee, J. C. An open source multivariate framework for n-tissue segmentation with evaluation on public data. Neuroinformatics 9, 381–400 (2011).
Heckemann, R. A. et al. Brain extraction using label propagation and group agreement: pincram. PLoS ONE 10, e0129211 (2015).
Zhang, Y., Brady, M. & Smith, S. Segmentation of brain MR images through a hidden Markov random field model and the expectation maximization algorithm. IEEE Transactions on Medical Imaging 20, 45–57 (2001).
Fischl, B. et al. Whole brain segmentation: automated labeling of neuroanatomical structures in the human brain. Neuron 33, 341–355 (2002).
Wee, C.-Y., Yap, P.-T. & Shen, D. Prediction of Alzheimer’s disease and mild cognitive impairment using cortical morphological patterns. Human Brain Mapping 34, 3411–3425 (2013).
Liu, X., Tosun, D., Weiner, M. W. & Schuff, N. Locally linear embedding (LLE) for MRI based Alzheimer’s disease classification. NeuroImage 83, 148–157 (2013).
Westman, E., Aguilar, C., Muehlboeck, J.-S. & Simmons, A. Regional magnetic resonance imaging measures for multivariate analysis in Alzheimer’s disease and mild cognitive impairment. Brain Topography 26, 9–23 (2013).
Chincarini, A. et al. Local MRI analysis approach in the diagnosis of early and prodromal Alzheimer’s disease. NeuroImage 58, 469–480 (2011).
Barnes, J. et al. A meta-analysis of hippocampal atrophy rates in Alzheimer’s disease. Neurobiology of Aging 30, 1711–1723 (2009).
Leung, K. K. et al. Robust atrophy rate measurement in Alzheimer’s disease using multi-site serial MRI: tissue-specific intensity normalization and parameter selection. NeuroImage 50, 516–523 (2010).
Heckemann, R. A. et al. Automatic morphometry in Alzheimer’s disease and mild cognitive impairment. NeuroImage 56, 2024–2037 (2011).
Heckemann, R. A. et al. Improving intersubject image registration using tissue-class information benefits robustness and accuracy of multi-atlas based anatomical segmentation. NeuroImage 51, 221–227 (2010).
Hammers, A. et al. Three-dimensional maximum probability atlas of the human brain, with particular reference to the temporal lobe. Human Brain Mapping 19, 224–247 (2003).
Gousias, I. S. et al. Automatic segmentation of brain MRIs of 2-year-olds into 83 regions of interest. NeuroImage 40, 672–684 (2008).
Ledig, C., Schuh, A., Guerrero, R., Heckemann, R. & Rueckert, D. Dataset - Structural brain imaging in Alzheimer’s disease and mild cognitive impairment: biomarker analysis and shared morphometry database. G-Node. http://doi.org/10.12751/g-node.aa605a (2018).
Tustison, N. et al. N4ITK: improved N3 Bias Correction. IEEE Transactions on Medical Imaging 29, 1310–1320 (2010).
Yushkevich, P. A. et al. Bias in estimation of hippocampal atrophy using deformation-based morphometry arises from asymmetric global normalization: An illustration in ADNI 3T MRI data. NeuroImage 50, 434–445 (2010).
Leung, K. K., Ridgway, G. R., Ourselin, S. & Fox, N. C. Consistent multi-time-point brain atrophy estimation from the boundary shift integral. NeuroImage 59, 3995–4005 (2012).
Lewis, E. B. & Fox, N. C. Correction of differential intensity inhomogeneity in longitudinal MR images. NeuroImage 58, 75–83 (2004).
Chang, C.-C. & Lin, C.-J. LIBSVM: A library for support vector machines. ACM Transactions on Intelligent Systems and Technology 2, 27:1–27:27 (2011).
Brodersen, K. H.,Ong, C. S., Stephan, K. E. & Buhmann, J. M. The balanced accuracy and its posterior distribution. In 20th International Conference on Pattern Recognition (ICPR), 3121–3124 (2010).
Cohen, J. Statistical power analysis for the behavioral sciences - second edition. (Lawrence Erlbaum Associates, Inc., Hillsdale, New Jersey, 1988).
Wang, H. et al. Multi-atlas segmentation with joint label fusion. IEEE Transactions on Pattern Analysis and Machine Intelligence 35, 611–623 (2013).
Sullivan, G. M. & Feinn, R. Using effect size-or why the p value is not enough. Journal of Graduate Medical Education 4, 279–282 (2012).
Barnes, J. et al. Head size, age and gender adjustment in MRI studies: a necessary nuisance? NeuroImage 53, 1244–1255 (2010).
Koikkalainen, H. et al. Improved classification of Alzheimer’s disease data via removal of nuisance variability. PLoS ONE 7, e31112 (2012).
Beheshti, I., Demirel, H. & Matsuda, H. Classification of Alzheimer’s disease and prediction of mild cognitive impairment-to-Alzheimer’s conversion from structural magnetic resource imaging using feature ranking and a genetic algorithm. Computers in Biology and Medicine 83, 109–119 (2017).
Hu, K., Wang, Y., Chen, K., Hou, L. & Zhang, X. Multi-scale features extraction from baseline structure MRI for MCI patient classification and AD early diagnosis. Neurocomputing 175, 132–145 (2016).
Zu, C. et al. Label-aligned multi-task feature learning for multimodal classification of Alzheimer’s disease and mild cognitive impairment. Brain Imaging and Behavior 10, 1148–1159 (2016).
Acknowledgements
This work was funded by the European Union’s Seventh Framework Programme under grant agreement no. 611005 (http://PredictND.eu). R.G. was funded by an Innovate UK (101685) (formerly UK Technology Strategy Board) grant. Data used in preparation of this article were obtained from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (adni.loni.usc.edu). As such, the investigators within the ADNI contributed to the design and implementation of ADNI and/or provided data but did not participate in analysis or writing of this report. A complete listing of ADNI investigators can be found at: http://adni.loni.usc.edu/wpcontent/uploads/how_to_apply/ADNI_Acknowledgement_List.pdf. Data collection and sharing for this project was funded by the ADNI (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (www.fnih.org). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
Author information
Authors and Affiliations
Contributions
C.L. performed the experiments and drafted the manuscript, C.L. and D.R. conceived the experiments, R.G., R.A.H. and D.R. supported the experiments, C.L. developed and implemented MALPEM, R.A.H. developed and implemented pincram and MAPER, A.S., R.A.H. and D.R. developed and implemented the registration methodology, A.S. and D.R. developed and implemented MIRTK. Alls reviewed and revised the manuscript.
Corresponding author
Ethics declarations
Competing Interests
C.L., A.S. and R.G. conducted this research while being employees of Imperial College London, U.K. (C.L., A.S., R.G.) and IXICO plc, U.K. (C.L., R.G.). D.R. is a co-founder and scientific advisor of IXICO plc, U.K., a provider of medical image analysis services. C.L. is currently employed by Imagen Technologies, Inc., N.Y., U.S.A. This does not alter thes’ adherence to Scientific Reports policies on sharing data and materials.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ledig, C., Schuh, A., Guerrero, R. et al. Structural brain imaging in Alzheimer’s disease and mild cognitive impairment: biomarker analysis and shared morphometry database. Sci Rep 8, 11258 (2018). https://doi.org/10.1038/s41598-018-29295-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-29295-9
This article is cited by
-
Hippocampal transcriptome-wide association study and pathway analysis of mitochondrial solute carriers in Alzheimer’s disease
Translational Psychiatry (2024)
-
Neuroimaging and machine learning for studying the pathways from mild cognitive impairment to alzheimer’s disease: a systematic review
BMC Neurology (2023)
-
The Mediating Role of Instrumental Activities of Daily Living in The Relation Between Cognitive Function and Life Satisfaction Among Malaysian Community-Dwelling Older Adults: Do Gender and Age Matter?
Applied Research in Quality of Life (2023)
-
Generalizable deep learning model for early Alzheimer’s disease detection from structural MRIs
Scientific Reports (2022)
-
A high-generalizability machine learning framework for predicting the progression of Alzheimer’s disease using limited data
npj Digital Medicine (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
