
Abstract
Constipation is one of the most frequent non-motor symptoms of Parkinson disease (PD) and it may be ignored by PD patients, leading to this problem not to be reported in time. The relationships between constipation and demographic variables, motor symptoms and other non-motor symptoms of PD are still unknown. PD patients were evaluated by diagnostic criteria of functional constipation in Rome III and divided into PD with constipation (PD-C) and PD with no constipation (PD-NC) groups. PD patients were assessed by rating scales of motor symptoms and other non-motor symptoms, activity of daily living and quality of life. The frequency of constipation in PD patients was 61.4%, and 24.5% of PD patients had constipation before the onset of motor symptoms. PD-C group had older age and age of onset, longer disease duration, more advanced disease stage, and more severe motor symptoms and non-motor symptoms, including worse cognition and emotion, poorer sleep quality, severer autonomic symptoms, fatigue and apathy. Binary Logistic regression analysis showed that the age, H-Y stage, depression, anxiety and autonomic dysfunction increased the risk of constipation in PD patients. Constipation exerted serious impact on the activity of daily living and quality of life in PD patients.
Similar content being viewed by others

Introduction
Parkinson disease (PD) is a common neurodegenerative disorder characterized by the progressive loss of neuromelanin-containing dopaminergic neurons in substantia nigra pars compacta (SNpc) and depletion of dopamine (DA) in striatum. PD was previously thought to be characterized by motor symptoms, including resting tremor, bradykinesia, rigidity, and gait and postural abnormalities. However, PD pathological stage based on the location of α-synuclein-immunopositive Lewy bodies1 indicates the presence of various non-motor symptoms, including autonomic dysfunction2, neuropsychiatric disturbance3, abnormal sensation4 and sleep disorders5, etc. Constipation is one of the most frequent non-motor symptoms in autonomic system6,7 and gastrointestinal disturbance of PD8. About 509~80%10 PD patients suffer from constipation. It has been reported that constipation can precede motor symptoms by as much as 20 years6 and people with constipation may have a relatively high risk of developing PD11. Accordingly, constipation may predict the occurrence of PD. However, PD patients may not talk about their symptom of constipation actively, leading to this problem not to be reported in time12.
In previous studies, it was found that constipation was correlated with the duration and severity of PD13, and the frequency and severity of constipation were increased as PD progressed14. While constipation is one of the most studied prodromal symptoms of PD, how constipation is related to demographic variables, motor function and other non-motor symptoms of PD is still controversial so far.
In this study, we continuously recruited PD patients, evaluated clinical symptoms of PD and constipation by using a variety of related scales and analyzed the relationships among constipation, demographic variables, motor function, and non-motor symptoms in order to associate the clinical features and relevant factors of PD with constipation.
Methods
Ethics statement
The protocol was approved by the Institutional Review Board of Beijing Tiantan Hospital. All participants completed the written informed consents. This study met the guidelines of Capital Medical University, which abided by the Helsinki Declaration on ethical principles for medical research involving human subjects.
Participants
Patients were diagnosed with PD according to UK Parkinson’s Disease Society Brain Bank criteria15. Total 306 PD patients were consecutively recruited from the Departments of Geriatrics and Neurology, Beijing Tiantan Hospital, Capital Medical University, from 2012 to 2016. PD patients with severe systemic diseases, such as anemia, heart failure, pulmonary disorders, chronic liver/renal failure, gastrointestinal disorders, infectious disease and chronic inflammatory disease were excluded, and patients with a positive family history of PD were also excluded.
Demographic variables, including gender, age, age of onset, disease duration, education level, side of onset, clinical type and levodopa equivalent daily dose (LEDD) were recorded for all participants.
Patients were evaluated by the professionally trained and qualified neurologists in our team and they did not know whether an individual patient had constipation or not.
Constipation assessment
The Rome criterion is an internationally recognized objective definition of constipation and focuses on 6 symptoms, including straining, lumpy or hard stools, sensation of incomplete evacuation, sensation of anorectal obstruction or blockage, manual maneuvers to facilitate evacuation, and two or fewer bowel movements per week. It is associated with a diagnosis of constipation with 2 or more symptoms being present for at least 3 months16. According to the Rome criterion of constipation, patients in this study were divided into PD with constipation (PD-C) and PD with no constipation (PD-NC) groups. In PD-C group, we further asked about the frequency of daily bowel movement of each patient, additionally, the severity of constipation and the information on the use of laxatives were also collected.
Assessments of clinical features
Motor function
The severity of PD was assessed by Hoehn-Yahr (H-Y) stage.
Motor symptoms of PD patients were evaluated by Unified Parkinson Disease Rating Scale (UPDRS) III, in which items 20 and 21 were for tremor, item 22 was for rigidity and items 23–26 were for bradykinesia. According to the method for clinical phenotypes classification by Schrag17, participants were divided into tremor type, bradykinesia-rigidity type and mixed type of PD.
Motor complications include wearing-off, on and off phenomenon and dyskinesia. Wearing-Off Scale was used for evaluating wearing-off phenomenon and UPDRS IV for assessing on-off phenomenon and dyskinesia.
Non-motor symptoms
Non-motor symptoms were screened by Non-Motor Symptoms Quest (NMSQ). It is a widely used18 self-administered 30-item instrument for screening the presence of a series of non-motor symptoms and calculating the incidence of each non-motor symptom.
Cognitive impairment was screened by Mini-Mental State Examination (MMSE) scale19, which is the most widely used by frontline physicians. MMSE covers the cognitive domains, including orientation, memory, attention, naming, repetition, comprehension, writing, and construction. The score ranges from 0 to 30 point(s). Patients with illiteracy, primary education, and above junior education are identified to have cognitive impairment when the score of MMSE scale is below 17, 20 and 24 points, respectively.
Hamilton Depression (HAMD) Scale -24 items is a frequently utilized depression severity rating scale20, which contains 24 variables, including depressed mood, guilt, suicide, initial insomnia, middle insomnia, delayed insomnia, work and interests, retardation, agitation, psychic anxiety, somatic anxiety, gastrointestinal symptoms, general somatic symptoms, genital symptoms, hypochondriasis, loss of weight, insight, diurnal variation, depersonalization, paranoid symptoms, obsessional symptoms, helplessness, hopelessness, and worthlessness. Score of HAMD Scale -24 items less than 8 points, between 8 to 19 points, 20 to 34 points and more than 35 points suggests no, mild, moderate and severe depression, respectively.
Hamilton Anxiety (HAMA) Scale -14 items is a clinician-rated scale and used to assess and quantify severity of anxiety21. The scale assesses a series of cognitive, behavioral, and somatic symptoms, including anxious mood, tension, fears, insomnia, cognitive impairement, depressed mood, somatic anxiety for muscle, somatic anxiety for sensation, cardiovascular symptoms, respiratory symptoms, gastrointestinal symptoms, genito-urinary symptoms, autonomic symptoms and behavior at interview. Clinicians are required to rate the severity of anxiety symptoms, which are scored on a 5-point scale ranging from 0 (absent) to 4 (severe). HAMD Scale -14 items less than 7 points, between 7–14 points and more than 15 points indicates no anxiety, possible anxiety and definite anxiety, respectively.
Pittsburgh Sleep Quality Index (PSQI) is a generic, self-applied questionnaire designed to evaluate mainly the quality of nocturnal sleep and to examine sleep habits and disturbances22 in the previous month. PSQI consists of 19 self-rated questions that are combined to form 7 component scores: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication and excessive daytime somnolence, each of which can be scored from 0 to 3 point(s) (from no difficulty to severe difficulty). Maximum score is 21 points, representing the maximum difficulty in 7 domains. Score of PSQI ≥5 indicates clinically meaningful sleep disorders.
Epworth Sleepiness Scale (ESS) is a self-administered scale, focusing on daytime sleepiness23. It consists of 8 items referred to daily or frequent situations, including sitting and reading, watching TV, sitting inactive in a public place (e.g. a theater or a meeting), as a passenger in a car for an hour without a break, lying down to rest in the afternoon when circumstance permit, sitting and talking to someone, sitting quietly after a lunch without alcohol and in a car, while stopped for a few minutes in the traffic. The response to each item rates the chance of dozing or sleeping in such situation. Item score ranges from 0 (would never doze or sleep) to 3 (high chance of dozing or sleeping) point (s) and the total scale score ranges from 0 to 24 point (s). ESS score >6 points represents no dozing or sleeping.
Scale for Outcomes in PD for Autonomic Symptoms (SCOPA-AUT) is a specific instrument designed to assess autonomic function for PD patients24. It is composed of 25 items, targeting the regions of gastrointestinal (7 items), urinary (6 items), cardiovascular (3 items); thermoregulatory (4 items), pupillomotor (1 item) and sexual (2 items for men and 2 items for women). Currently, there is no definite cut-off value for this scale. Generally, the higher the total score of SCOPA-AUT, the more severe the autonomic symptoms.
Fatigue is screened by Fatigue Severity Scale (FSS)25. It is a self-administered 9-item fatigue rating scale that encompasses several aspects of fatigue and their impact on the daily functioning of patients. Patients are asked to rate how each item describes their fatigue from 1 (“strongly disagree”) to 7 point (s) (“strongly agree”). Total FSS score is obtained by dividing the sum of all item scores by 9. Score of FSS ≥4 indicates clinically meaningful fatigue.
Restless Legs Syndrome (RLS) Rating Scale (RLSRS) is used to evaluate RLS for PD patients. RLSRS consists of 10 questions, needs face to face interview, and is rated from 0 to 4 point (s)26. RLSRS scores of 0, 1–10, 11–20, 21–30 and 31–40 points represents asymptomatic, mild, moderate, severe and very severe, respectively. It shows excellent clinimetric properties and has been validated in cross-sectional studies and applied in clinical trials.
Modified Apathy Evaluation Scale (MAES) is recommended to rate apathy in PD patients by Movement Disorders Society27. It is a well-validated and 14-item self-report tool, for example: are you interested in learning new things? Are you interested in anything? Do you care about your health? and so on. The score of MAES ranges from 0 to 42 point (s), with higher score indicative of severer apathy28. Score of MAES ≥14 indicates clinically meaningful apathy.
Activity of daily living (ADL) and quality of life of PD patients
Activity of daily living is evaluated by ADL scale, which includes 20 items. The higher the score of the scale, the poorer the activity of daily living. Quality of life of PD patients was assessed by Parkinson Disease Quality of Life Questionnaire (PDQ) -39 items. The higher the score of the scale, the worse the quality of life.
Data analyses
Statistical analyses were performed with SPSS Statistics 20.0 (Chicago, IL, USA). P value was statistically significant when it was less than 0.05.
Demographic information, motor and non-motor symptoms were compared between PD-C and PD-NC groups.
Continuous variables, if normally distributed, were presented as means ± SDs and two groups were compared by 2-tailed t test. If not normally distributed, continuous variables were presented as median (quartile) and compared by nonparametric test. Discrete variables were compared by Chi square test.
Age, age of onset, disease duration, LEDD, H-Y stage, the scores of UPDRS III, UPDRS IV, MMSE, HAMD, HAMA, PSQI, SCOPA-AUT, FSS and MAES between PD-C and PD-NC groups were significantly different, thus, these variables were put into an established binary logistic regression equation and set as independent variables, whereas, with or without constipation in PD patients was set as a dependent variable. P value was significant when it was <0.05.
Results
The frequency and assessment of constipation in PD patients
In 306 PD patients, 188 cases (61.4%) were with constipation. Among 188 PD patients with constipation, 46 cases (24.5%) experienced constipation before the onset of motor symptoms. The evaluation of constipation in PD-C group was showed in Supplemental Table 1.
Demographic information of PD-C and PD-NC groups
Demographic variables of PD-C and PD-NC groups were compared in Table 1. The age and age of onset of PD-C group were significantly older than that of PD-NC group (P < 0.01). The disease duration of PD-C group was dramatically longer than that of PD-NC group (P < 0.05). The LEDD of PD-C group was significantly higher than that of PD-NC group (P < 0.05). There were no significant differences in gender, educational level, side of onset and clinical type between PD-C and PD-NC groups (P > 0.05).
Motor symptoms and motor complications of PD-C and PD-NC groups
Motor symptoms of PD-C and PD-NC groups were compared in Table 2. H-Y stage and UPDRS III score in PD-C group were remarkably increased when comparing with PD-NC group (P < 0.01), indicating that PD-C group had more advanced stage of PD and more severe motor symptoms.
Motor complications of PD-C and PD-NC groups were compared in Table 2. UPDRS IV score in PD-C group was significantly increased when comparing with PD-NC group (P < 0.01), implying that PD-C group had severer motor complications.
Non-motor symptoms of PD-C and PD-NC groups
The numbers of non-motor symptoms of PD-C and PD-NC groups were compared in Supplemental Table 1. The total number of non-motor symptoms, the number of non-motor symptoms before and after motor symptoms in PD-C group were all significantly more than that of PD-NC group (P < 0.01).
The frequency of each non-motor symptom evaluated by NMSQ in PD-C and PD-NC groups was compared in Supplemental Table 2. The frequencies of dribbling, loss of taste/smell, swallowing/choking difficulties, constipation, bowel emptying incompletion, urine urgency, nocturia, apathy, hallucinations, sexual dysfunction, falls, insomnia, intense dreaming, rapid eye movement sleep behavior disorder, restless legs and diplopia, were all significantly increased in PD-C group compared with PD-NC group (P < 0.05).
The performance of each following non-motor symptom assessed by related rating scales in PD-C and PD-NC groups was compared in Table 3. Compared with PD-NC group, PD-C group scored conspicuously lower on MMSE scale and scored remarkably higher on the scales of HAMD, HAMA, PQSI, SCOPA-AUT, FSS and AS, suggesting that individuals in PD-C group had evidently worsened cognitive impairment, mood disturbances, sleep quality, autonomic symptoms, fatigue and apathy (P < 0.05).
Further comparison of detailed symptoms of autonomic dysfunctions by SCOPA-AUT scale in PD-C and PD-NC groups was performed in Supplemental Table 3. Compared with PD-NC group, PD-C group scored significantly higher on the gastrointestinal symptoms, urinary dysfunction, cardiovascular disturbance, and thermoregulatory dysfunction, demonstrating that PD-C group had severe gastrointestinal, urinary, cardiovascular, and thermoregulatory symptoms (P < 0.05).
There were no distinct differences in the scores of ESS and RLSRS between PD-C and PD-NC groups (P > 0.05).
Activity of daily living and quality of life in PD-C and PD-NC groups
We conducted the comparisons of activity of daily living and quality of life in PD-C and PD-NC groups in Supplemental Table 4. Comparing with PD-NC group, the score of ADL scale in PD-C group was significantly increased (P < 0.01), demonstrating that PD-C group had obviously compromised activity of daily living.
The score of PDQ-39 score in PD-C group was markedly decreased compared with PD-NC group, implying that PD-C group had severely disturbed quality of life (P < 0.01).
Risk factors of PD-C
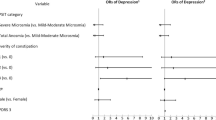
Logistic regression analysis was performed to figure out the risk factors of PD-C in Table 4. Eventually, it was found that only SCOPA-AUT score was the risk factor of constipation in PD patients (OR = 1.091; P < 0.01).
Discussion
In this study, 61.4% PD patients had constipation, in accordance with previous studies reporting 50% to 80% of constipation in PD patients9,10, thus, constipation is a common non-motor symptom of PD.
Here, it was found that 46 out of 188 patients (24.5%) in PD-C group experienced constipation before the onset of motor symptoms, illustrating that constipation is one of prodromal symptoms of PD. A previous study observed α-synuclein in colon tissue prior to onset of PD29, which might explicate constipation prior to motor symptoms.
Increasing evidence revealed that aging was an independent risk factor for the development and progression of PD30. In this study, it was observed that PD-C group had older age (Table 1). Additionally, PD-C group had older age of onset (Table 1), consistent with a study showing that constipation was more likely to occur in PD patients with disease onset at old-age31. Above data suggested that aging was involved in the constipation of PD. It could be speculated that in PD patients with older age and age of onset, less amount of activity and more weakened gastrointestinal motility evidently delayed colonic transport and thus caused constipation.
According to Braak stage of PD, Lewy bodies in the enteric nervous system and dorsal nucleus of vagus are associated with constipation of PD. In this study, PD-C group had longer disease duration (Table 1), more advanced disease stage and severer motor symptoms (Table 2). It was reported that constipation was positively correlated with disease duration and severity of PD13, and more severe with PD progression14. Thus, it might be that with PD duration and H-Y stage increased, dopamine level was markedly depleted and motor symptoms were remarkably aggravated as substantia nigra was largely impaired by Lewy bodies, which further precipitated gastrointestinal dysfunction and constipation deterioration.
Levodopa remains the mainstay of treatment for PD over 40 years after its introduction. Previous studies investigated the impact of dopaminergic treatment on autonomic symptoms, such as constipation, in PD patients32,33. In this study, PD-C group had significantly higher LEDD than PD-NC group (Table 1), this is in line with earlier studies reporting that changes in autonomic symptoms were related to dopaminergic treatment. In addition, the PD-C group had a longer disease duration and more advanced stages, thus might require more medications to alleviate symptoms.
Motor complications of PD are caused by the disease progression and long-time use of dopaminergic drugs with short half-life. In this study, PD-C group had more severe motor complications (Table 2), which might be explained by the findings that PD-C group had longer disease duration, more advanced H-Y stage, more severe motor symptoms, and larger dose of dopaminergic drugs.
In this study, PD-C group had more non-motor symptoms (Supplemental Table 5), among which constipation, ranked the top followed by taste/smell, dribbling, swallowing/choking difficulties, and nocturia, It was hypothesized that Lewy bodies, in addition to the deposition in the brain areas associated with constipation, were also extensively occurred in the brain regions associated with other non-motor symptoms.
Cognitive impairment was a very common non-motor symptom of PD34. In Braak stage V and VI, Lewy bodies occur in the brain regions related to cognitive impairment, such as limbic system and neocortex; meanwhile, Lewy bodies deposit more extensively in the areas associated with constipation, therefore, PD-C patients might suffered from significantly impaired cognitive function (Table 3).
Depression, a type of mood disturbance, might precede the development of motor symptoms and was considered as a prodromal symptom before the diagnosis of PD35,36. Anxiety is another common mood disturbance with high prevalence in PD patients despite that it was received attention in recent years37. In this study, depression and anxiety in PD-C group were significantly severer than that in PD-NC group (Table 3). It was reported that mood disturbances appeared to approximately double an individual’s risk of subsequent PD in a meta-analysis36. It is well known that 5-hydroxytryptamine (5-HT) is pivotal for the maintenance of normal mood, which depletion is one of the mechanism underlying depression and anxiety. Meanwhile, 5-HT exerted the action of enhancing gastrointestinal motility38, and 5-HT4 receptor agonists, mosapride39 and tegaserod40, alleviated the symptom of constipation. Accordingly, constipation and mood disturbances might share common mechanism relating 5-HT dysfunction in PD population.
Sleep disorders are the frequent non-motor symptoms in PD subjects41, and considered as an important independent determinant for impaired activity of daily living and quality of life42. In the current investigation, PSQI score in PD-C group was significantly higher than that in PD-NC group (Table 3), illustrating that the sleep quality was dramatically impaired in PD patients with constipation. Particularly, evaluations by using NMSQ showed that the incidences of insomnia, intense dreaming and rapid eye movement sleep behavior disorder in PD-C group were all significantly higher than that in PD-NC group (Supplemental Table 2), It was speculated that PD-C patients more easily suffered from above symptoms of sleep disorders, which might be due to discomfort in the abdomen caused by constipation.
PD patients with autonomic dysfunction presented numerous symptoms which compromised activities of daily living and quality of life43,44. The occurrence of autonomic symptoms is related to the deposition of Lewy bodies in the relevant brain regions. In this study, gastrointestinal, urinary, cardiovascular and thermoregulatory dysfunctions in PD-C group were significantly severer than that in PD-NC group (Supplemental Table 3) and high SCOPA-AUT score was the risk factor of constipation in PD patients (Table 4).
In gastrointestinal dysfunction, this study displayed remarkably higher incidence of dribbling, swallowing and bowel emptying incompletion in PD-C group than PD-NC group (Supplemental Table 2). Dribbling is not only caused by the increased secretion of salivary, but also by the reduced automatic swallowing due to dysphagia, resulting in a large amount of saliva fill in and outflow the mouth45. Dysphagia is related to the glossopharyngeum movement disorders, esophagectasis or slowdown of the esophageal peristalsis, and the decline of gastric motor function was frequently seen in advanced PD patients, which prolonged meal time and even leads to severe aspiration pneumonia and asphyxia46. Bowel emptying incomplete is diagnosed as constipation according to the Rome functional constipation diagnostic criterion, so the incidence of bowel emptying incompletion in PD-C group was significantly higher than that in PD-NC group.
The most striking feature of urinary dysfunction is the filling phase disorder, which includes urgency, nocturia and urinary incontinence47. Here, it was observed that the PD-C group had markedly higher incidences of urgency and nocturia than PD-NC group (Supplemental Table 2). Urgency and nocturia in PD patients might be attributed to detrusor hyperreflexia when the related brain region were affected by Lewy bodies.
The decreased cardiac uptake of 123I meta-iodobenzylguanidine (MIBG) on myocardial scintigraphy suggested that the degeneration of the cardiac sympathetic nerve began in the early stage of PD, even before neuronal loss in the dorsal vagal nucleus48. Data from this study implied that cardiovascular dysfunction in PD-C group was severer than that in PD-NC group (Supplemental Table 3), therefore, it was hypothesized that there was a common mechanism linking constipation and cardiovascular dysfunction in PD patients.
There was a paucity of literature about disruptions to thermoregulation in PD patients49. Firstly, PD patients are elderly population, which sensitivity to thermoreceptor is drastically decreased, accordingly, the process of heat production and heat radiation is drastically impaired when the outside temperature is changed. Secondly, sympathetic-adrenal system affected by Lewy bodies fails to control the process of heat production. Thirdly, severer motor symptoms, such as tremor and rigidity, cause skeletal muscle contraction and increase heat production. Above factors may contribute to the thermoregulatory dysfunction of PD patients. In this study, the results indicated that thermoregulatory dysfunction in PD-C group was severer than that in PD-NC group (Supplemental Table 3). Previous neuropathological studies found Lewy body deposition in the pons and medulla50, which might explain the thermoregulatory dysfunction and constipation observed in this study.
Fatigue was one of the most disabling non-motor symptoms51, however, how fatigue is related to constipation of PD is uncertain yet. Autonomic dysfunction was found to aggravate the subjective perception of fatigue52. The present study showed that PD-C group had severer fatigue than PD-NC group (Table 3), implying that constipation might aggravate fatigue of PD. When Lewy bodies deposited in raphe nuclei, locus coeruleus and magnocellular portions of the reticular formation, patients might manifest with autonomic dysfunction and fatigue, both of which might share similar pathological mechanism53.
Apathy, a lack of motivation characterized by diminished goal-oriented behaviors54, was one of the most common neuropsychiatric symptom of PD55. Here, apathy in PD-C group was dramatically severer compared with PD-NC group (Table 3), indicating that constipation might aggravate the symptom of apathy. A previous study found a negative correlation between apathy score and gray matter density in inferior frontal56 and premotor cortex, which were a part of autonomic system. Therefore, there might be a common structural basis for constipation and apathy for PD patients. Further investigation is needed to explore the underlying mechanism for their relationship.
Results from this study revealed that constipation dramatically decreased the activity of daily living and compromised the quality of life for PD patients. It was speculated that constipation together with more and severer motor and non-motor symptoms synergistically impact the activity of daily living and quality of life for PD patients.
In summary, this study systemically investigated the clinical characteristics and relevant factors of PD with constipation. The frequency of constipation in PD patients was 61.4%, and 24.5% of patients had constipation before the onset of motor symptoms. PD patients with constipation had older age and age of onset, longer disease duration, more advanced disease stage, and more severe motor and non-motor symptoms. Autonomic dysfunction increased the risk of constipation in PD patients. Constipation significantly compromised the activity of daily living and quality of life for PD patients.
References
Braak, H. et al. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiology of aging 24, 197–211 (2003).
Khoo, T. K. et al. The spectrum of nonmotor symptoms in early Parkinson disease. Neurology 80, 276–281, https://doi.org/10.1212/WNL.0b013e31827deb74 (2013).
Negre-Pages, L. et al. Anxious and depressive symptoms in Parkinson’s disease: the French cross-sectionnal DoPaMiP study. Movement disorders: official journal of the Movement Disorder Society 25, 157–166, https://doi.org/10.1002/mds.22760 (2010).
Degardin, A. et al. Deficient “sensory” beta synchronization in Parkinson’s disease. Clinical neurophysiology: official journal of the International Federation of Clinical Neurophysiology 120, 636–642, https://doi.org/10.1016/j.clinph.2009.01.001 (2009).
Schulte, E. C. & Winkelmann, J. When Parkinson’s disease patients go to sleep: specific sleep disturbances related to Parkinson’s disease. Journal of neurology 258, S328–335, https://doi.org/10.1007/s00415-011-5933-0 (2011).
Savica, R. et al. Medical records documentation of constipation preceding Parkinson disease: A case-control study. Neurology 73, 1752–1758, https://doi.org/10.1212/WNL.0b013e3181c34af5 (2009).
Gao, X., Chen, H., Schwarzschild, M. A. & Ascherio, A. A prospective study of bowel movement frequency and risk of Parkinson’s disease. American journal of epidemiology 174, 546–551, https://doi.org/10.1093/aje/kwr119 (2011).
Sakakibara, R. et al. Colonic transit time and rectoanal videomanometry in Parkinson’s disease. Journal of neurology, neurosurgery, and psychiatry 74, 268–272 (2003).
Ashraf, W., Pfeiffer, R. F., Park, F., Lof, J. & Quigley, E. M. Constipation in Parkinson’s disease: objective assessment and response to psyllium. Movement disorders: official journal of the Movement Disorder Society 12, 946–951, https://doi.org/10.1002/mds.870120617 (1997).
Verbaan, D. et al. Patient-reported autonomic symptoms in Parkinson disease. Neurology 69, 333–341, https://doi.org/10.1212/01.wnl.0000266593.50534.e8 (2007).
Lin, C. H., Lin, J. W., Liu, Y. C., Chang, C. H. & Wu, R. M. Risk of Parkinson’s disease following severe constipation: a nationwide population-based cohort study. Parkinsonism & related disorders 20, 1371–1375, https://doi.org/10.1016/j.parkreldis.2014.09.026 (2014).
Kaye, J., Gage, H., Kimber, A., Storey, L. & Trend, P. Excess burden of constipation in Parkinson’s disease: a pilot study. Movement disorders: official journal of the Movement Disorder Society 21, 1270–1273, https://doi.org/10.1002/mds.20942 (2006).
Krogh, K., Ostergaard, K., Sabroe, S. & Laurberg, S. Clinical aspects of bowel symptoms in Parkinson’s disease. Acta neurologica Scandinavica 117, 60–64, https://doi.org/10.1111/j.1600-0404.2007.00900.x (2008).
Edwards, L., Quigley, E. M., Hofman, R. & Pfeiffer, R. F. Gastrointestinal symptoms in Parkinson disease: 18-month follow-up study. Movement disorders: official journal of the Movement Disorder Society 8, 83–86, https://doi.org/10.1002/mds.870080115 (1993).
Hughes, A. J., Daniel, S. E., Kilford, L. & Lees, A. J. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. Journal of neurology, neurosurgery, and psychiatry 55, 181–184 (1992).
Thompson, W. G. et al. Functional bowel disorders and functional abdominal pain. Gut 45(Suppl 2), Ii43–47 (1999).
Schrag, A., Jahanshahi, M. & Quinn, N. What contributes to quality of life in patients with Parkinson’s disease? Journal of neurology, neurosurgery, and psychiatry 69, 308–312 (2000).
Lindqvist, D. et al. Non-motor symptoms in patients with Parkinson’s disease - correlations with inflammatory cytokines in serum. PloS one 7, e47387, https://doi.org/10.1371/journal.pone.0047387 (2012).
Folstein, M. F., Folstein, S. E. & McHugh, P. R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12, 189–198 (1975).
Williams, J. B. Standardizing the Hamilton Depression Rating Scale: past, present, and future. Eur Arch Psychiatry Clin Neurosci 251(Suppl 2), Ii6–12 (2001).
Hamilton, M. The assessment of anxiety states by rating. Br J Med Psychol 32, 50–55 (1959).
Buysse, D. J., Reynolds, C. F. 3rd, Monk, T. H., Berman, S. R. & Kupfer, D. J. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 28, 193–213 (1989).
Johns, M. W. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 14, 540–545 (1991).
Visser, M., Marinus, J., Stiggelbout, A. M. & Van Hilten, J. J. Assessment of autonomic dysfunction in Parkinson’s disease: the SCOPA-AUT. Movement disorders: official journal of the Movement Disorder Society 19, 1306–1312, https://doi.org/10.1002/mds.20153 (2004).
Friedman, J. H. et al. Fatigue rating scales critique and recommendations by the Movement Disorders Society task force on rating scales for Parkinson’s disease. Movement disorders: official journal of the Movement Disorder Society 25, 805–822, https://doi.org/10.1002/mds.22989 (2010).
Zea-Sevilla, M. A. & Martinez-Martin, P. Rating scales and questionnaires for assessment of sleep disorders in Parkinson’s disease: what they inform about? J Neural Transm (Vienna) 121(Suppl 1), S33–40, https://doi.org/10.1007/s00702-014-1217-z (2014).
Starkstein, S. E. Apathy in Parkinson’s disease: diagnostic and etiological dilemmas. Movement disorders: official journal of the Movement Disorder Society 27, 174–178, https://doi.org/10.1002/mds.24061 (2012).
Starkstein, S. E. et al. Reliability, validity, and clinical correlates of apathy in Parkinson’s disease. J Neuropsychiatry Clin Neurosci 4, 134–139, https://doi.org/10.1176/jnp.4.2.134 (1992).
Shannon, K. M., Keshavarzian, A., Dodiya, H. B., Jakate, S. & Kordower, J. H. Is alpha-synuclein in the colon a biomarker for premotor Parkinson’s disease? Evidence from 3 cases. Movement disorders: official journal of the Movement Disorder Society 27, 716–719, https://doi.org/10.1002/mds.25020 (2012).
Collier, T. J., Kanaan, N. M. & Kordower, J. H. Ageing as a primary risk factor for Parkinson’s disease: evidence from studies of non-human primates. Nature reviews. Neuroscience 12, 359–366, https://doi.org/10.1038/nrn3039 (2011).
Zhou, M. Z. et al. The association between non-motor symptoms in Parkinson’s disease and age at onset. Clinical neurology and neurosurgery 115, 2103–2107, https://doi.org/10.1016/j.clineuro.2013.07.027 (2013).
Muller, B. et al. Autonomic symptoms and dopaminergic treatment in de novo Parkinson’s disease. Acta neurologica Scandinavica 127, 290–294, https://doi.org/10.1111/ane.12010 (2013).
Kim, H. J. et al. Nonmotor symptoms in de novo Parkinson disease before and after dopaminergic treatment. Journal of the neurological sciences 287, 200–204, https://doi.org/10.1016/j.jns.2009.07.026 (2009).
Yu, S. Y. et al. Potential biomarkers relating pathological proteins, neuroinflammatory factors and free radicals in PD patients with cognitive impairment: a cross-sectional study. BMC neurology 14, 113, https://doi.org/10.1186/1471-2377-14-113 (2014).
Postuma, R. B. et al. Identifying prodromal Parkinson’s disease: pre-motor disorders in Parkinson’s disease. Movement disorders: official journal of the Movement Disorder Society 27, 617–626, https://doi.org/10.1002/mds.24996 (2012).
Noyce, A. J. et al. Meta-analysis of early nonmotor features and risk factors for Parkinson disease. Annals of neurology 72, 893–901, https://doi.org/10.1002/ana.23687 (2012).
Dissanayaka, N. N. et al. Anxiety disorders in Parkinson’s disease: prevalence and risk factors. Movement disorders: official journal of the Movement Disorder Society 25, 838–845, https://doi.org/10.1002/mds.22833 (2010).
Cellek, S. et al. 5-HT4 receptor agonists enhance both cholinergic and nitrergic activities in human isolated colon circular muscle. Neurogastroenterology and motility: the official journal of the European Gastrointestinal Motility Society 18, 853–861, https://doi.org/10.1111/j.1365-2982.2006.00810.x (2006).
Liu, Z. et al. Mosapride citrate, a novel 5-HT4 agonist and partial 5-HT3 antagonist, ameliorates constipation in parkinsonian patients. Movement disorders: official journal of the Movement Disorder Society 20, 680–686, https://doi.org/10.1002/mds.20387 (2005).
Sullivan, K. L., Staffetti, J. F., Hauser, R. A., Dunne, P. B. & Zesiewicz, T. A. Tegaserod (Zelnorm) for the treatment of constipation in Parkinson’s disease. Movement disorders: official journal of the Movement Disorder Society 21, 115–116, https://doi.org/10.1002/mds.20666 (2006).
Riedel, O. et al. Frequency of dementia, depression, and other neuropsychiatric symptoms in 1,449 outpatients with Parkinson’s disease. Journal of neurology 257, 1073–1082, https://doi.org/10.1007/s00415-010-5465-z (2010).
Scaravilli, T., Gasparoli, E., Rinaldi, F., Polesello, G. & Bracco, F. Health-related quality of life and sleep disorders in Parkinson’s disease. Neurological sciences: official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology 24, 209–210, https://doi.org/10.1007/s10072-003-0134-y (2003).
Berrios, G. E., Campbell, C. & Politynska, B. E. Autonomic failure, depression and anxiety in Parkinson’s disease. The British journal of psychiatry: the journal of mental science 166, 789–792 (1995).
Damiano, A. M., Snyder, C., Strausser, B. & Willian, M. K. A review of health-related quality-of-life concepts and measures for Parkinson’s disease. Quality of life research: an international journal of quality of life aspects of treatment, care and rehabilitation 8, 235–243 (1999).
Jost, W. H. Gastrointestinal dysfunction in Parkinson’s Disease. Journal of the neurological sciences 289, 69–73, https://doi.org/10.1016/j.jns.2009.08.020 (2010).
Troche, M. S. et al. Aspiration and swallowing in Parkinson disease and rehabilitation with EMST: a randomized trial. Neurology 75, 1912–1919, https://doi.org/10.1212/WNL.0b013e3181fef115 (2010).
Sakakibara, R. et al. Questionnaire-based assessment of pelvic organ dysfunction in Parkinson’s disease. Autonomic neuroscience: basic & clinical 92, 76–85, https://doi.org/10.1016/s1566-0702(01)00295-8 (2001).
Orimo, S. et al. Degeneration of cardiac sympathetic nerve begins in the early disease process of Parkinson’s disease. Brain pathology (Zurich, Switzerland) 17, 24–30, https://doi.org/10.1111/j.1750-3639.2006.00032.x (2007).
Pierangeli, G. et al. Nocturnal body core temperature falls in Parkinson’s disease but not in Multiple-System Atrophy. Movement disorders: official journal of the Movement Disorder Society 16, 226–232 (2001).
Braak, H. & Del Tredici, K. Neuroanatomy and pathology of sporadic Parkinson’s disease. Adv Anat Embryol Cell Biol 201, 1–119 (2009).
Abe, K., Takanashi, M. & Yanagihara, T. Fatigue in patients with Parkinson’s disease. Behavioural neurology 12, 103–106 (2000).
Friedman, J. H. et al. Fatigue in Parkinson’s disease: a review. Movement disorders: official journal of the Movement Disorder Society 22, 297–308, https://doi.org/10.1002/mds.21240 (2007).
Braak, H., Rub, U., Gai, W. P. & Del Tredici, K. Idiopathic Parkinson’s disease: possible routes by which vulnerable neuronal types may be subject to neuroinvasion by an unknown pathogen. Journal of neural transmission (Vienna, Austria: 1996) 110, 517–536, https://doi.org/10.1007/s00702-002-0808-2 (2003).
Marin, R. S. Apathy: a neuropsychiatric syndrome. The Journal of neuropsychiatry and clinical neurosciences 3, 243–254, https://doi.org/10.1176/jnp.3.3.243 (1991).
Pont-Sunyer, C. et al. The onset of nonmotor symptoms in Parkinson’s disease (the ONSET PD study). Movement disorders: official journal of the Movement Disorder Society 30, 229–237, https://doi.org/10.1002/mds.26077 (2015).
Reijnders, J. S. et al. Neuroanatomical correlates of apathy in Parkinson’s disease: A magnetic resonance imaging study using voxel-based morphometry. Movement disorders: official journal of the Movement Disorder Society 25, 2318–2325, https://doi.org/10.1002/mds.23268 (2010).
Acknowledgements
This work is supported by the National Key Research and Development Program of China (2016YFC1306000, 2016YFC1306300), the National Natural Science Foundation of China (81571229, 81071015, 30770745), the Key Project of Natural Science Foundation of Beijing, China (B) (kz201610025030), the Key Project of Natural Science Foundation of Beijing, China (4161004, kz200910025001), Natural Science Foundation of Beijing, China (7082032), National Key Basic Research Program of China (2011CB504100), Important National Science & Technology Specific Projects (2011ZX09102-003-01), National Key Technology Research and Development Program of the Ministry of Science and Technology of China (2013BAI09B03), Project of Beijing Institute for Brain Disorders (BIBD-PXM2013_014226_07_000084), High Level Technical Personnel Training Project of Beijing Health System, China (2009-3-26), Project of Construction of Innovative Teams and Teacher Career Development for Universities and Colleges Under Beijing Municipality (IDHT20140514), Capital Clinical Characteristic Application Research (Z12110700100000, Z121107001012161), Beijing Healthcare Research Project, China (JING-15-2, JING-15-3), Excellent Personnel Training Project of Beijing, China (20071D0300400076), Basic-Clinical Research Cooperation Funding of Capital Medical University, China (2015-JL-PT-X04, 10JL49, 14JL15), Youth Research Funding, Beijing Tiantan Hospital, Capital Medical University, China (2014-YQN-YS-18, 2015-YQN-15, 2015-YQN-05, 2015-YQN-14, 2015-YQN-17).
Author information
Authors and Affiliations
Contributions
Qiu-jin Yu: drafting/revising the manuscript, study concept or design, analysis or interpretation of data, accepts responsibility for conduct of research and will give final approval, acquisition of data, statistical analysis. Shu-Yang Yu: study concept or design, accepts responsibility for conduct of research and will give final approval, acquisition of data. Li-Jun Zuo: study concept or design, accepts responsibility for conduct of research and will give final approval, acquisition of data. Teng-Hong Lian: study concept or design, accepts responsibility for conduct of research and will give final approval, acquisition of data. Yang Hu: study concept or design, accepts responsibility for conduct of research and will give final approval, acquisition of data. Rui-Dan Wang: study concept or design, accepts responsibility for conduct of research and will give final approval, acquisition of data. Ying-Shan Piao: study concept or design, accepts responsibility for conduct of research and will give final approval, acquisition of data. Peng Guo: study concept or design, accepts responsibility for conduct of research and will give final approval, acquisition of data. Li Liu: study concept or design, accepts responsibility for conduct of research and will give final approval, acquisition of data. Zhao Jin: study concept or design, accepts responsibility for conduct of research and will give final approval, acquisition of data. Li-Xia Li: study concept or design, accepts responsibility for conduct of research and will give final approval, acquisition of data. Piu Chan: study concept or design, analysis or interpretation of data, accepts responsibility for conduct of research and will give final approval, statistical analysis, study supervision. Sheng-Di Chen: study concept or design, accepts responsibility for conduct of research and will give final approval, study supervision. Xiao-Min Wang: study concept or design, accepts responsibility for conduct of research and will give final approval, statistical analysis, study supervision. Wei Zhang: study concept or design, analysis or interpretation of data, accepts responsibility for conduct of research and will give final approval, acquisition of data, statistical analysis, study supervision.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yu, QJ., Yu, SY., Zuo, LJ. et al. Parkinson disease with constipation: clinical features and relevant factors. Sci Rep 8, 567 (2018). https://doi.org/10.1038/s41598-017-16790-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-16790-8
This article is cited by
-
Neuroimmune Connectomes in the Gut and Their Implications in Parkinson’s Disease
Molecular Neurobiology (2024)
-
REM sleep behavior disorder correlates with constipation in de novo Chinese Parkinson’s disease patients
Neurological Sciences (2023)
-
Mutant LRRK2 exacerbates immune response and neurodegeneration in a chronic model of experimental colitis
Acta Neuropathologica (2023)
-
An update on pathogenesis and clinical scenario for Parkinson’s disease: diagnosis and treatment
3 Biotech (2023)
-
Immunisation with UB-312 in the Thy1SNCA mouse prevents motor performance deficits and oligomeric α-synuclein accumulation in the brain and gut
Acta Neuropathologica (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
