
Abstract
Little is known about the mechanical properties of pelvic floor structures and their role in the course and treatment of pelvic organ prolapse (POP). We hypothesize that in vivo mechanical properties of the vaginal wall are related to the appearance of POP and pre-and post-operative states. We used a suction device for intravaginal application, the aspiration device, to evaluate two in vivo mechanical parameters of the anterior vaginal wall, the load dependent tissue displacement and the initial displacement, by image analysis in pre- and post-menopausal women with (POP) and without (control) cystocele (POP: pre-menopausal: N = 6, post-menopausal: N = 19, control: pre-menopausal: N = 17, post-menopausal: N = 6). Mechanical parameters in women with and without cystocele and pre- and post-operative parameters were compared. Statistically significant differences were observed between the two mechanical parameters in pre- and post-operative states (P = 0.04, P = 0.03), but not between the parameters for women with and without cystocele (P = 0.92, P = 0.75). The mechanical behavior of pelvic floor structures is influenced by factors such as POP, age or estrogenization that are apparent at different length scales, which cannot be separated by the aspiration based biomechanical measurements. When comparing pre- and post-operative states of the same patient, a firmer tissue response was observed after intervention.
Similar content being viewed by others


Introduction
A woman’s lifetime risk of undergoing an operation for pelvic organ prolapse (POP) or urinary incontinence is 11.1%1. Still, little is known about the mechanical properties of pelvic floor structures and tissues which play a major role in the pathogenesis and course of POP2,3,4. In fact, corresponding findings seem to support different conclusions.
Ex vivo mechanical tests have been conducted using tissue strips of prolapsed and non-prolapsed vaginal wall excised during surgery or excised from female cadavers2,3,5,6,7,8,9,10,11,12. In uniaxial tension, prolapsed vaginal wall tissue is stiffer than control tissue6,11. And prolapsed vaginal wall tissue is stiffer in shear deformation compared to control tissue12.
Alternatively, in vivo methods using tactile and suction devices have been presented aiming at an intravaginal evaluation of the mechanical properties of the vaginal wall13,14,15. In contrast to ex vivo findings, in vivo stiffness of the vaginal wall is reported to be inversely correlated to the stage of POP13,15. Moreover, all devices have been able to discriminate between the mechanical properties in pre- versus post-operative states. The post-operative vaginal wall was reported to be stiffer than the pre-operative in patients treated by different surgical techniques, i.e. before and after mesh application, native prolapse repair or sacrocolpopexy16,17,18.
Our study intended to shed light onto the apparently contradictory in vivo and ex vivo findings with respect to the relationship between vaginal wall stiffness and POP. We used a novel suction device we have called “the aspiration device” to evaluate in vivo mechanical parameters of the anterior vaginal wall in pre- and post-menopausal patients with and without cystocele under optical guidance by means of a video camera. For women undergoing traditional surgical cystocele repair, mechanical parameters were compared pre- and post-operatively. It is hypothesized that the assessed mechanical parameters allow discrimination between the mechanical properties of the anterior vaginal wall of women (i) with and without cystocele and (ii) in pre- and postoperatively.
Materials and Methods
Study design
In this prospective, non-randomised, controlled, non-blind, interventional study in collaboration between the Department of Gynecology of the University Hospital Zurich (USZ), the Institute of Anatomy of the University of Zurich and the Center of Mechanics of ETH Zurich, pre- and post-menopausal women with cystocele (POP group) and without cystocele (control group) who were hospitalized at USZ for gynecological intervention were invited to participate (written informed consent required). In the POP group, POP repair was performed by means of native repair without implanting a mesh, such as anterior colporrhaphy, posterior colporrhaphy, or sacrospinal ligament fixation as appropriate. The control group consisted of patients without POP who underwent hysterectomy for benign gynecological condition. Exclusion criteria were age below 18 years, pregnant, breastfeeding, malignancies in the pelvis or local infections, or previous POP surgery.
Clinical examination
The patients were examined the evening before surgery in semirecumbent position with an empty urinary bladder. To avoid artificial lubrication by examination or ultrasound gel, the aspiration measurement was taken first. Afterwards, the stage of prolapse was quantified in accordance with the POP-Q standard19. Clinical parameters, such as age, body mass index (BMI), parity and menopausal state were recorded. During post-operative follow-up of the POP group at 6 to 12 weeks, clinical examination and POP-Q assessment were performed, and in patients who had undergone anterior colporrhaphy the aspiration measurement was repeated.
Aspiration device
The applied aspiration technique is based on the pipette aspiration principle20. The tissue of interest is elevated by a defined vacuum pressure and the resulting tissue displacement is evaluated thus providing a metric proportional to tissue compliance. The aspiration device has been used in several clinical applications21,22,23. No complications have been reported, and no risks and no harm were to be expected for the participants.
We used a probe design specifically developed for vaginal application. The aspiration setup consisted of the measurement probe, a pressure unit, and a personal computer with the appropriate software (Fig. 1a and b). The aspiration probe (AP) (Fiberoptic P & P AG, Spreitenbach, Switzerland) was a slender tube with a modular tip, serving as a vacuum cavity (Fig. 1a). A camera and a pressure sensor (p2) were mounted within the cavity. At its distal end, the tip had a lateral aperture shaped as a long-hole (13.5 mm × 8.5 mm). For in vivo measurements, the probe was applied intravaginally such that the aperture was placed on the anterior vaginal wall (Fig. 1b). The vacuum within the aspiration cavity, i.e. the load applied to the tissue, was provided by the pressure unit. In addition to electronic components, the pressure unit also included a vacuum container, a diaphragm gas pump (Type: NMP 830 KNDC, KNF Neuberger AG, Balterswil, Switzerland), two valves (Type: VDW21-5G-3-01F-Q, SMC Pneumatik AG, Weisslingen, Switzerland), an internal pressure sensor (Type: XFGMC-3025KPGSRH, Pewatron AG, Zurich, Switzerland), and a tubing system. The vacuum container had a capacity of 0.01 m3 evacuated by the pump to a controlled constant vacuum pressure. Controlled by the valves, the aspiration cavity was either connected to the vacuum container or to the environment, subjecting the tissue to the vacuum pressure or releasing it, respectively. The actuators, the pump and the two valves were computer-controlled, realizing a defined load history of the air pressure (that is suction) p(t) [N/mm2] acting on the tissue. The respective software was programmed with LabVIEW (National Instruments, Austin, Texas, USA). The integrated camera recorded a side view image sequence of the current tissue configuration at a frame rate of 20 images/s and allowed a continuous visual control (Fig. 2a). The measurement output consisted of a continuous pressure signal and a corresponding image sequence, which needed further processing, in order to quantify the tissue displacement. The camera images were further used to quantify the visual appearance of the vaginal wall through the nature of rugae. For this purpose, we defined index taking values of 1–3, 1 indicating that no rugae were visible on the anterior vaginal wall, 2 corresponding to intermediate, and 3 to distinct rugae.

The Aspiration Device. (a) Aspiration probe, top: modular tip with the aspiration opening and a scale, bottom: probe with the unmounted tip, exposing the aspiration pipe, the optical fiber providing light, the camera objective and the pressure sensor (p2). (b) Transvaginal application (schematic view): The lateral opening is attached to the vaginal wall. The tip cavity is evacuated through the aspiration pipe. The current vacuum pressure is observed by the internal pressure sensor (p2) and controlled by the pressure unit. The camera records side view images of the intruding tissue at rest (dashed line) and at load (full line). The tissue elevation describes the difference between these two configurations.

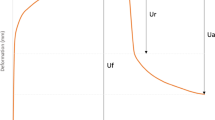
Mechanical parameters. (a) The area enclosed by the contour of the tissue displacement is a quantitative measure of the tissue configuration. The area enclosed by the undeformed configuration is called the reference configuration A0 (i). The load dependent difference of each current tissue configuration A(p(t)) with respect to the reference configuration A0 is called the tissue elevation ΔA(p(t)), which is indicative of tissue displacement (ii). (b) Evaluation of the mechanical parameters based on the history of the load dependent tissue configuration A(p(t)). Only cycles 5–10 were considered. The cyclic tissue displacement ΔAi = Ai,max − Ai,0 was defined as the maximum tissue elevation in each cycle. The initial displacement was defined as the initial unloaded tissue configuration in cycle 5.
Aspiration protocol
Aspiration measurements were performed on the anterior vaginal wall, 5 cm proximal to the hymen in the region close to the bladder neck. This location was chosen as the bladder neck is directly affected by an anterior vaginal wall prolapse and as the vaginal wall is less wrinkled (rugae) leading to more reproducible measurements. All measurements were done by the same experienced gynecologist. The vacuum container was evacuated to −25 mbar (relative to the atmospheric pressure), a pressure level which was, on the one hand harmless for the patient, and on the other hand high enough to obtain a visible tissue deformation. The tissue was loaded (−25 mbar) and released (0 mbar) cyclically by holding each level for 10 s. One measurement was performed per patient and consisted of ten such cycles, lasting for a total of 200 s. With respect to measurement failure, we differentiated between technical failure such as malfunction of technical components and procedural failure such as insufficient vacuum or the the vaginal wall touching the inner surface of the aspiration cavity.
Data processing
Programs for data analysis were written with Matlab (The Mathworks Inc., Natick, Massachusetts, USA). The image sequence recorded by the camera documented the current, deformed tissue configuration dependent on the defined pressure history p(t). The tissue displacement was determined from the load dependent change of the tissue configuration. The current tissue configuration at time-point t [s] subject to the current pressure p(t) was quantified by the two-dimensional projected area A(p(t)) [mm2] enclosed by the contour of the tissue displacement (Fig. 2a).
Mechanical parameters
The mechanical response measured with the aspiration experiment is influenced by the mechanical properties of tissue below the surface, down to 1–2 times the radius of the aspiration device opening24. In the present case, this reaches the full vaginal wall thickness including (to some extent) the influence of fascial tissue. In accordance with the literature, an intact integration of the vaginal wall within the pelvic floor and an intact microstructure were assumed to be associated with a compact, dense unloaded configuration and a stiff mechanical response13,15. Moreover, scar tissue formation and a change in anatomical boundary conditions, which are present after a surgical intervention were expected to increase the structural stiffness of the vaginal wall. A stiffness-like mechanical parameter was evaluated based on the history of the current tissue configuration A(p(t)). The difference between any current tissue configuration A(p(t)) and a defined reference configuration A0 was called tissue elevation ΔA(p(t)) = A(p(t)) − A0 (Fig. 2a). The cyclic tissue displacement was defined as the maximum tissue elevation per cycle ΔAi = Ai,max − Ai,0 as shown in Fig. 2b, where the indices i, max and 0 denote the cycle number, the cyclic maximum and the cyclic initial tissue intrusion. It was observed, that the cyclic tissue displacement during the initial cycles was weakly reproducible, comparable to preconditioning effects, known for biological tissues25. Thus, cycles 1–4 were not considered for parameter evaluation. The median cyclic tissue displacement of cycles 5–10 was called tissue displacement ΔA 5–10 , a parameter representing the local structural and material stiffness of the vaginal wall. A representative unloaded state of the vaginal wall was defined by the initial tissue configuration in cycle 5, called initial displacement A 5,0 (Fig. 2b). Tissue displacement and initial displacement were analyzed for differences between POP and control, pre- and post-menopausal state, and pre- and post-operative measurements.
Grouping of participants
The participants were subdivided into a pre- and post-menopausal group. Postmenopause was defined as absence of menstruation for a minimum of 12 months. Perimenopausal women were considered as premenopausal. Cystoceles stage 0 and I (POP-Q) were considered as control, and stage >I as POP. Systemic or local hormone treatment was also recorded but not considered for the present study as this would have led to even smaller group sizes.
Statistics
Statistical evaluation was carried out using Matlab. The data was treated anonymously. Descriptive statistical data was presented as mean, standard deviation (SD), and range (minimum – maximum). The mechanical parameters in the POP and control group were compared using the Mann-Whitney U test. Changes due to a surgical intervention were analysed using the Wilcoxon signed rank test. P values < 0.05 indicated statistical significance (two-sided). Due to the lack of preliminary data for the aspiration technique of the anterior vaginal wall with our device, no sample size calculation was feasible.
This trial was performed in accordance with the approved protocol obtained from the local Cantonal ethics committee of Zurich (StV 11/2009). This study is registered with ClinicalTrials.gov, number NCT01042470 (date of registration: January 4, 2010).
Results
Basic characteristics
Between November 2010 and February 2012, 48 women were recruited (Table 1), with all having a pre-operative assessment with the aspiration technique. Mean age was 58.2 years (SD 13.4, range 38.2–83.7), mean BMI 25.9 (SD 4.0, range 18.1–35.3), and mean parity 1.6 (SD 1.3, range 0–5). In 14 women, both pre- and post-operative measurements were performed. In the pre-menopausal subgroup, patients with POP had statistically significantly a higher parity than patients in the control group (1.3 ± 1.4 vs. 3.0 ± 1.3, P = 0.03). In the post-menopausal subgroup, patients with POP were with 71.2 ± 8.4 years statistically significantly older than patients in the control group (61.0 ± 8.8, P = 0.03).
Aspiration measurement: Pre- versus post-operative
Statistically significant differences were observed between mechanical parameters for pre- and post-operative measurements: both tissue displacement and initial displacement were smaller after POP surgery (ΔA5–10 P = 0.04, A5,0 P = 0.03) as presented in Table 2.
Aspiration measurement: POP versus control
No statistically significant differences between the mechanical parameters tissue displacement (ΔA5–10) and initial displacement (A5,0) could be assessed for women with (POP) and without (control) cystocele, neither for pre-menopausal (ΔA5–10, P = 0.92; A5,0, P = 0.75) nor for post-menopausal (ΔA5–10, P = 0.63; A5,0, P = 0.15) women (Table 3).
No measurements had to be excluded due to procedural failure (procedural failure rate 0%). Technical failure was due to computer-related problems saving the image sequence. The technical failure rate was <10%.
Discussion
The aim of this study was to detect in vivo differences in the biomechanical properties of the anterior vaginal wall in patients with and without cystocele and before and after anterior colporrhaphy. Using a novel and innovative technique, the aspiration device, our present aspiration protocol allows detection of such differences between the pre-operative and post-operative situation, but not between women with and without cystocele.
Our results are in accordance with the findings of Werbrouck et al. who reported no significant differences in the mechanical properties of the vaginal wall in women with and without POP14,16. Conversely, Epstein et al. reported correlations between the mechanical properties of the vaginal wall and the stage of prolapse15. In contrast to our study, Epstein et al. and Werbrouck et al. applied high levels of suction pressure up to −300 mbar (compared to −25 mbar in our study) resulting in a high level of applied forces of up to 1.57 N (compared to 0.25 N in our study). Due to the nonlinear stress strain relationship which is characteristic for most soft biological tissues, a reason for their need of such supraphysiological forces could be the implied prestrain on the vaginal wall caused by a high contact force and the use of a speculum. In our study, a vacuum pressure of −25 mbar was seen to represent an upper bound to reliably avoid the tissue touching the inner wall of the cavity of the aspiration probe. With respect to the tissue reference configuration and according boundary conditions, we aimed at an unloaded configuration closely reproducing the physiological in vivo conditions. The inhomogeneous, wrinkled structure of the vaginal wall with the typical rugae and the lubrication represented major sources of uncertainty influencing the reproducibility of the measured data. In contrast, Epstein et al. defined a standard protocol to set up an altered, but more reproducible reference configuration15. They inserted a speculum, pre-stretching the vagina, and flattening the rugae. The measurement position was chosen as 2 cm proximal to the hymen, and thus more distal as compared to our protocol and closer to the speculum. The measurement site was cleaned and dried with a swab, removing the lubricating film and thus normalizing the friction behavior. Hence, in particular, mesostructural influences such as rugae and lubrication were reduced. The application of uncontrolled, unphysiological boundary conditions might induce systematic bias in the determination of the biomechanical properties. This approach was therefore avoided in our protocol. Recently, Parkinson et al. demonstrated another approach to measure the vaginal pressure profile, using an optical-fiber-based instrumented speculum for distributed real-time pressure measurement of the vaginal pressure profile in sheep26. They found higher pressure profiles for nulliparous than for parous sheep and observed an increased tissue laxity in the upper anterior vagina for parous sheep.
How do we interpret the findings from a biomechanical point of view? The structure of the vagina can be sub-divided into different length scales. At the macroscale, the vagina is embedded within the pelvic floor, determining its global boundary conditions (anatomy). At the mesoscale, the surface of the vaginal wall has a wrinkled and layered structure consisting of rugae. The microscale is mainly characterized by the fibrous constituents of the extracellular matrix, i.e. collagen and elastin. Among other factors, POP, estrogenization, and age influence the vaginal wall at all these length scales. POP is a macroscale change of the pelvic floor anatomy, related to vaginal wall laxity and decreased vaginal wall integrity19,27. Moreover, POP is associated with alterations of the microstructure, i.e. of the collagen metabolism and the content of normal elastin27,28,29. The meso- and microstructure are influenced by estrogen and age. They determine the appearance of the rugae, the collagen maturation and the content of elastin27,30. The relative contribution of each factor to the actually measured mechanical parameter depends on the sensitivity of the aspiration measurement to phenomena at the different length scales. The current procedure is not sensitive to changes at one single length scale. However, significant changes influencing all length scales, such as surgical cystocele repair, can be addressed with the present protocol.
In contrast to in vivo measurements, ex vivo tests exclude anatomic influences (macrostructure), such as the level of vaginal wall integrity. Testing after cadaver dissections can provide excellent detail on structural morphology, but biomechanical properties can be distorted by post-mortem or embalming processes. In vivo, the prolapsed, less integrated and slack vaginal wall leads to a decreased structural stiffness compared to the intact, well integrated vaginal wall13,15. Ex vivo, all slackness is removed, leading to a stiffened material response6,11,12. These differences in the tissue reference configuration are probably responsible for the divergent findings in the current literature.
When comparing in vivo and ex vivo techniques, major limitations of ex vivo studies are the restricted availability of non-prolapsed human vaginal wall tissue and the minor relevance particularly of uniaxial tensile tests, due to non-physiological loading and boundary conditions5,31. In contrast, non-invasive in vivo measurement techniques represent promising tools for POP diagnosis and prevention15,18. Based on the mechanical properties of pelvic tissues, the risk for a recurrent prolapse will be reduced through case specific treatment (native tissue or prosthetic mesh repair) or a more conscious selection of prosthetic materials3,5,31. Moreover, follow-up observations of mechanical parameters should help to evaluate the long-term surgical outcome17,18.
The strength of our study with the aspiration device is that its vaginal application caused no discomfort, no pain, and no complications. Compared to procedural failure rates of approximately 20% and >50% in other studies14,15, our aspiration protocol demonstrated an outstanding reliability (procedural failure rate of 0%). A significant and very important value was seen in the use of a camera, which is a unique characteristic of the present suction device. The camera provided visual feedback which enabled us to guarantee safety and to exclude procedural measurement failure. Furthermore, visual analysis of the tissue configuration allowed the challenges related to the influence of rugae and the selection of a reference configuration to be identified.
The unbalanced groups are one limitation of this study. On the one hand, pre-menopausal women with cystocele were quite rare and on the other hand, post-menopausal controls were less frequently hospitalized in the USZ, leading to a selection bias.
We believe that a characterization of the pelvic floor mechanics related to POP needs to address processes at different length scales and at the same time needs to be able to differentiate between them, - a challenging requirement that has not yet been reached by any of the currently applied techniques. In this context, the present study might contribute to a further improvement of currently available, together with the development of alternative, in vivo techniques which are still the subject of fundamental research. In particular, the combination of aspiration experiments with high resolution tissue imaging might provide direct insight on the level of deformation of each tissue structure contributing to the mechanical properties of vaginal wall.
Conclusions
Our novel aspiration device gives a visually monitored insight into the biomechanical behavior of the anterior vaginal wall. So far, the aspiration technique has enabled the detection of differences in the mechanical properties of the vagina in patients before and after cystocele repair. For future research, there is a need to gain more insight into the relationship between biomechanical properties of pelvic floor structures and POP. Moreover, it would be of interest to classify findings according to demographic parameters like specific age groups, parity status, ethnic group, hormonal status and/or other varying pelvic floor conditions. Further research of the biomechanical properties of the vaginal wall and the pelvic floor are important, in particular with regard to recurrences after native repair for POP surgery and the actual debate on alloplastic meshes for POP repair.
References
Olsen, A. L., Smith, V. J., Bergstrom, J. O., Colling, J. C. & Clark, A. L. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol 89, 501–506, https://doi.org/10.1016/S0029-7844(97)00058-6 (1997).
Fu, X., Siltberg, H., Johnson, P. & Ulmsten, U. Viscoelastic properties and muscular function of the human anterior vaginal wall. Int Urogynecol J 6, 229–234, https://doi.org/10.1007/BF01894267 (1995).
Rubod, C. et al. Biomechanical properties of vaginal tissue: preliminary results. Int Urogynecol J 19, 811–816, https://doi.org/10.1007/s00192-007-0533-3 (2008).
Gilchrist, A. S., Gupta, A., Eberhart, R. C. & Zimmern, P. E. Do Biomechanical Properties of Anterior Vaginal Wall Prolapse Tissue Predict Outcome of Surgical Repair? J Urology 183, 1069–1073, https://doi.org/10.1016/j.juro.2009.11.025 (2010).
Pena, E. et al. Experimental study and constitutive modeling of the viscoelastic mechanical properties of the human prolapsed vaginal tissue. Biomech Model Mechan 9, 35–44, https://doi.org/10.1007/s10237-009-0157-2 (2010).
Lei, L. L., Song, Y. F. & Chen, R. Q. Biomechanical properties of prolapsed vaginal tissue in pre- and postmenopausal women. Int Urogynecol J 18, 603–607, https://doi.org/10.1007/s00192-006-0214-7 (2007).
Goh, J. T. W. Biomechanical properties of prolapsed vaginal tissue in pre- and postmenopausal women. Int Urogynecol J Pel 13, 76–79, https://doi.org/10.1007/s001920200019 (2002).
Ettema, G. J. C., Goh, J. T. W. & Forwood, M. R. A new method to measure elastic properties of plastic-viscoelastic connective tissue. Med Eng Phys 20, 308–314, https://doi.org/10.1016/S1350-4533(98)00026-5 (1998).
Gilchrist, A., Zimmern, P., Bhat, A., Gupta, A. & Eberhart, R. Do biomechanical properties of anterior prolapsed vaginal tissue predict surgical outcome repair? Neurourol Urodynam 27, 149–150 (2008).
Zimmern, P. E., Eberhart, R. C. & Bhatt, A. Methodology for Biomechanical Testing of Fresh Anterior Wall Vaginal Samples From Postmenopausal Women Undergoing Cystocele Repair. Neurourol Urodynam 28, 325–329, https://doi.org/10.1002/Nau.20657 (2009).
Jean-Charles, C. et al. Biomechanical properties of prolapsed or non-prolapsed vaginal tissue: impact on genital prolapse surgery. Int Urogynecol J 21, 1535–1538, https://doi.org/10.1007/s00192-010-1208-z (2010).
Feola, A., Duerr, R., Moalli, P. A. & Abramowitch, S. D. Changes in the rheological behavior of the vagina in women with pelvic organ prolapse. Int Urogynecol J, https://doi.org/10.1007/s00192-012-2002-x (2012).
Egorov, V., van Raalte, H. & Lucente, V. Quantifying vaginal tissue elasticity under normal and prolapse conditions by tactile imaging. Int Urogynecol J 23, 459–466, https://doi.org/10.1007/s00192-011-1592-z (2012).
Werbrouck, E. et al. In ICS/IUGA.
Epstein, L. B., Graham, C. A. & Heit, M. H. Systemic and vaginal biomechanical properties of women with normal vaginal support and pelvic organ prolapse. Am J Obstet Gynecol 197, 165.e161–165.e166, https://doi.org/10.1016/j.ajog.2007.03.040 (2007).
Werbrouck, E. et al. Correlation of in vivo biomechanical properties of the vaginal wall and clinical severity scores in patients with and without previous prolapse surgery. Non-Discussion Poster in ICS-IUGA annual scientific meeting (2010).
Epstein, L. B., Graham, C. A. & Heit, M. H. Impact of sacral colpopexy on in vivo vaginal biomechanical properties. Am J Obstet Gynecol 199, 664.e661–664.e666, https://doi.org/10.1016/J.Ajog.2008.07.056 (2008).
Egorov, V., van Raalte, H. & Sarvazyan, A. P. Vaginal Tactile Imaging. Ieee T Bio-Med Eng 57, 1736–1744, https://doi.org/10.1109/Tbme.2010.2045757 (2010).
Bump, R. C. et al. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am J Obstet Gynecol 175, 10–17, https://doi.org/10.1016/S0002-9378(96)70243-0 (1996).
Aoki, T., Ohashi, T., Matsumoto, T. & Sato, M. The pipette aspiration applied to the local stiffness measurement of soft tissues. Ann Biomed Eng 25, 581–587, https://doi.org/10.1007/Bf02684197 (1997).
Bauer, M. et al. Assessment of the in vivo biomechanical properties of the human uterine cervix in pregnancy using the aspiration test A feasibility study. Eur J Obstet Gyn R B 144, S77–S81, https://doi.org/10.1016/j.ejogrb.2009.02.025 (2009).
Mazza, E. et al. Mechanical properties of the human uterine cervix: An in vivo study. Med Image Anal 10, 125–136, https://doi.org/10.1016/j.media.2005.06.001 (2006).
Nava, A., Mazza, E., Furrer, M., Villiger, P. & Reinhart, W. H. In vivo mechanical characterization of human liver. Med Image Anal 12, 203–216, https://doi.org/10.1016/j.media.2007.10.001 (2008).
Nava, A., Mazza, E., Kleinermann, F., Avis, N. J. & McClure, J. Determination of the mechanical properties of soft human tissues through aspiration experiments. Lect Notes Comput Sc 2878, 222–229 (2003).
Fung, F. C. Biomechanics: Mechanical Properties of Living Tissue (Springer-Verlag, 1993).
Parkinson, L. A. et al. Real-time measurement of the vaginal pressure profile using an optical-fiber-based instrumented speculum. J Biomed Opt 21, 127008, https://doi.org/10.1117/1.JBO.21.12.127008 (2016).
Drutz, H. P., Herschorn, S. & Diamant, N. E. Female pelvic medicine and reconstructive pelvic surgery. (Springer-Verlag 2003).
Connell, K. A. Elastogenesis in the vaginal wall and pelvic-organ prolapse. The New England Journal of Medicine 364, 2356–2358, https://doi.org/10.1056/NEJMcibr1104976 (2011).
Budhata, M. et al. Extracellular matrix proteases contribute to progression of pelvic organ prolapse in mice. J Clin Invest 121, 2048–2059, https://doi.org/10.1172/Jci45636 (2011).
Kerkhof, M. H., Hendriks, L. & Brolmann, H. A. M. Changes in connective tissue in patients with pelvic organ prolapse-a review of the current literature. Int Urogynecol J 20, 461–474, https://doi.org/10.1007/s00192-008-0737-1 (2009).
Cosson, M. et al. A biomechanical study of the strength of vaginal tissues - Results on 16 post-menopausal patients presenting with genital prolapse. European Journal of Obstetrics Gynecology and Reproductive Biology 112, 201–205, https://doi.org/10.1016/S0301-2115(03)00333-6 (2004).
Acknowledgements
The authors would like to thank Rico Muff (EMPA Materials Science and Technology, Dübendorf, Switzerland) for developing and implementing the control software for the aspiration device. We would also like to thank Johnson & Johnson for unconditional financial support. The authors had collaborations with and were supported by unconditional funding from Johnson & Johnson Medical (Norderstedt, Germany), for this project (administration number 41-3605.4/03618). The company did not interfere with the planning, execution or reporting of this experimental study nor does it own the results.
Author information
Authors and Affiliations
Contributions
E.M., B.R., and D.S. designed and developed the protocol and the project, collected and managed the data, performed the data and statistical analysis, and drafted and revised the article critically for important intellectual content. In addition, D.S. performed the clinical examination. C.B., D.P., M.B., C.M., and D.F. contributed to conception and design (project development, revising the article critically for important intellectual content), and in addition, D.F. and E.M. gave their final approval.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Röhrnbauer, B., Betschart, C., Perucchini, D. et al. Measuring tissue displacement of the anterior vaginal wall using the novel aspiration technique in vivo. Sci Rep 7, 16141 (2017). https://doi.org/10.1038/s41598-017-16083-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-16083-0
This article is cited by
-
Non-invasive biomechanical assessment of the prolapsed vaginal wall: an explorative pilot study on cutometry and indentometry
Scientific Reports (2023)
-
Bilayer Stiffness Identification of Soft Tissues by Suction
Experimental Mechanics (2023)
-
Anisotropy of the Passive and Active Rat Vagina Under Biaxial Loading
Annals of Biomedical Engineering (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
