
Abstract
A survey was performed to assess the current management of targeted temperature management (TTM) in patients following cardiac arrest (CA) and whether healthcare providers will change target temperature after publication of 2015 American Heart Association guidelines for resuscitation in China. 52 hospitals were selected from whole of China between August to November 2016. All healthcare providers in EMs and/or ICUs of selected hospitals participated in the study. 1952 respondents fulfilled the survey (86.8%). TTM in CA patients was declared by 14.5% of physicians and 6.7% of the nurses. Only 4 of 64 departments, 7.8% of physicians and 5.7% of the nurses had implemented TH for CA patients. Since the publication of 2015 AHA guidelines, 33.6% of respondents declared no modification of target temperature, whereas 51.5% declared a target temperature’s change in future practice. Respondents were more likely to choose 35∼36 °C-TTM (54.7%) after guidelines publication, as compared to that before guidelines publication they preferred 32∼34 °C-TTM (54.0%). TTM for CA patients was still in the early stage in China. Publication of 2015 resuscitation guidelines did have impact on choice of target temperature among healthcare providers. They preferred 35∼36 °C-TTM after guidelines publication.
Similar content being viewed by others

Introduction
There were more than 500 thousand cardiac arrests (CA) each year in China. Even in Beijing-the capital of China-where the medical technology was well developed, the survival to hospital discharge and the percentage of patients with good neurological outcome (usually defined as cerebral performance category 1 and 2) was only 1.3% and 1.0% following out-of-hospital CA1, the survival to hospital discharge and the percentage of patients with good neurological outcome was9.1% and 6.4% following in-hospital CA2.
Targeted temperature management (TTM) is one of few beneficial interventions to improve outcomes of CA patients, it has been recommended as a standard therapy for comatose patients after return of spontaneous circulation (ROSC)3,4. It has been already more than one decade since the two landmark studies of therapeutic hypothermia (TH) after CA have been published5,6. Since then, the widespread implementation of TH seemed to occur7,8,9. But in China it was not until 2012 that TH began to be used for CA patients.
TH was recommended that CA patients should be cooled to 32 °C to 34 °C for 12 to 24 hours in 2010 American Heart Association (AHA) Guidelines for cardiopulmonary resuscitation (CPR)10. But with the new evidence, they found that all TTM procedures (e.g. 36 °C-TTM and 33 °C-TTM) are similarly beneficial when compared with non-TTM regimen5,6,11,12,13. Especially the large well-conducted randomized TTM trial revealed that no main outcome differences were observed between the two evaluated levels of TTM: 33 °C versus 36 °C11. So selecting and maintaining a constant temperature between 32 °C and 36 °C during TTM was recommended in 2015 AHA guidelines3.
The awareness and application of TTM in CA patients and whether healthcare providers will change target temperature after publication of 2015 AHA guidelines has never been assessed in China. We conducted a nationwide survey to determine the current awareness and management of TTM for CA patients in emergency departments (EDs) and ICUs.
Methods
Study design and data collection
This was a cross-sectional multicenter study. Multistage convenience sampling was used. First of all 10 representative provinces were selected from the east, south, west, north and middle of China. The 10 provinces were well geographically distributed as shown in Fig. 1 (5 provinces were in the relatively developed east and south of China, 3 provinces were in the relatively underdeveloped west and north of China and 2 provinces were in middle of China). Then we chose at least one affiliated hospital of a well-known medical university (representing hospitals with relatively advanced medical technology)and hospitals with varying numbers in second- and third-tier cities (representing hospitals with relatively underdeveloped medical technology) in select province based on the number and level of the province’s hospitals. Among those hospitals, we were more likely to choose hospitals which have a good cooperative relationship with us in order to get a high response rate and high quality control. Finally 52 hospitals were included, of which 47 are Level III and 5 are Level II hospitals. Then we conducted a questionnaire survey for all healthcare providers in the EDs and/or ICUs of selected hospitals, in an attempt to target providers likely to care for cardiac arrest patients. Informed consent was obtained from all participants.

Geographic distribution of surveyed provinces http://echarts.baidu.com/ and the version URL is http://gallery.echartsjs.com/preview.html?c=xr1n8e1eO-.
The questionnaire was developed by a senior emergency physician experienced in CA and TTM and discussed 3 times by an emergency expert team working on rephrasing and improvement. Briefly, the questionnaire includes three parts: (1) Characteristics of the ICU or ED and the respondent; (2) General management of CA patients; (3) The awareness and practice of TTM in CA patients. The study group tested both test-retest reliability and split-half reliability of the questionnaire. Before the questionnaire was send to the respondents, test-retest reliability was analyzed. 105 healthcare providers, including 29 physicians and 76 nurses with reasonable distribution in different age and titles, were selected to fulfill the questionnaire two times in an interval of two weeks. There were no significant differences in the results of the repeated surveys and the Pearson correlation coefficient was 0.80 indicating a high quality in test-retest reliability. After data was collected from all respondents, split-half reliability was analyzed and the Guttman split-half coefficient of the questionnaire was 0.95 indicating a high quality in split-half reliability. The questionnaires were sent to the heads from August to November2016. Data collection ended in February 2017. All protocols were approved by Peking university third hospital. All methods were performed in accordance with the relevant guidelines and regulations.
Statistical methods
The data were analyzed by SPSS 20.0. Quantitative variables were expressed as mean (standard deviation) when following a Gaussian distribution or median (inter quartile range 25∼75%) otherwise. Qualitative variables were expressed as frequencies. Data was tested for normality using the Shapiro-Wilk Normality Test.
Results
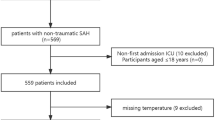
A total of 2250 questionnaires were sent, 1952 respondents of 64 EDs or ICUs fulfilled the survey (86.8%). General characteristics of respondents and departments are described in Table 1.Only 4 of 64 departments (6.3%) had implemented TH for CA patients.3 departments performed ≤5 cases per year and one departments performed 5∼10 cases per year. General management of CA patients was shown in Table 2.
The awareness of TTM in comatose adult patients with CA after ROSC
The awareness of TTM in comatose CA patients was described in Table 3. The ratio of respondents who did not know the concept of TTM recommended by guidelines was 77.1% in physicians and 86.2% in nurses, and that who did not know the concept of TH was 84.9% in physicians and 86.6% in nurses. 57.6% of physicians and 37.3% of nurses thought that intravascular cooling was better in temperature control and improvement of CA patients’ outcomes than that of surface cooling. But surface cooling was considered to be safer as reported by about 1/3 respondents. Considering the two target temperature levels of TTM (33 °C versus 36 °C), about 1/3 respondents believed that 33 °C-TTM was more beneficial in improving survival and neurologic outcomes of CA patients, but 44.0% of physicians and 31.8% of nurses thought that 36 °C-TTM had more advantages in security.
The practice of TTM in comatose adult patients with CA after ROSC
Temperature monitoring during TTM in CA patients was mainly performed using external measure as reported by 81.6% of respondents, and/or bladder probe by 21.4% of respondents (Fig. 2). TTM in CA patients was declared only by 14.5% of physicians and 6.7% of the nurses. The overall duration of TTM was mainly applied 12 h∼24 h by 36.8% of physicians, and 24 h∼48 h by 32.6%. Only 7.8% of physicians and 5.7% of the nurses had implemented TH for unconscious CA patients in practice. The top three reasons for nonuse of TH among physicians were technical difficulty of cooling (31.1%), lack of TH-related equipment (20.9%) and being afraid of potential TH-related adverse effect (20.4%) (Fig. 3).

Sites of temperature monitoring during TTM in CA patients (n = 201 respondents; 254 answers expressed as percentage of response). External measure: skin measurements; Intravascular devices: Swan-Ganz catheter or PICCO measurements. TTM: target temperature management; CA: Cardiac arrest.

Reasons why therapeutic hypothermia is not considered in unconscious cardiac arrest patients (Physicians: n = 614 respondents; 1119 answers expressed as percentage of responses; Nurses: n = 695 respondents; 1293 answers expressed as percentage of responses). CA: cardiac arrest.
Indications of TH implementation in CA patients are described in Table 4. TH was reported to be induced and/or maintained using cold intravenous fluid infusion and/or external water blanket more frequently, whereas external advanced surface cooling gel pads and intravascular cooling were rarely used. During the TH period, patients were reported to always receive sedatives only by 21.7% of respondents (midazolam 70.9% and/or propofol 54.7%), analgesics by 4.8% (morphine 54.3% and fentanyl 42.9%), and neuromuscular blockers by 15.8% (vecuronium 68.0% and rocuronium 16%).
Changes of TTM in the future practice after publication of 2015 AHA guidelines for CPR
Among respondents who were familiar with TTM and answered the question whether they would change target temperature in future practice in CA patients after 2015 guidelines publication, 31.6% (59/187) of physicians and 38.6% (49/127) of nurses declared no modification, whereas 57.2% (107/187) of physicians and 42.5% (54/127) of nurses declared that they would change target temperature in the future TTM practice. The temperature targets preferred by respondents before and after publication of 2015 guidelines were depicted in Fig. 4. Respondents were more likely to choose 35∼36 °C-TTM (54.7%) after guidelines publication, as compared to that before guidelines publication they preferred 32∼34 °C-TTM (54.0%).

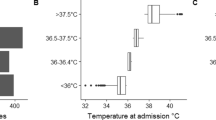
Distribution of target temperature before and after publication of 2015 AHA resuscitation guidelines (n = 298 respondents, expressed as percentage).
Discussion
Poor awareness and utilization of TTM
Our survey revealed that more than 4/5 healthcare providers of EDs or ICUs were not familiar with TTM in CA patients recommended by guidelines.TTM in CA patients was declared by 14.5% of physicians and 6.7% of the nurses. Only 4 of 64 departments, 7.8% of physicians and 5.7% of the nurses had implemented TH for CA patients in practice.
Since the two main studies published in 20025,6, TH began to be used for CA patients. In the early stage, the rates of TH implementation were relatively low ranging from 13 to 27% with variations according to countries7,14,15,16. Widespread TH implementation seemed to occur after publication of 2005 resuscitation guidelines17. Two consecutive surveys performed in Poland found that the number of ICUs using TH increased threefold in the5-year period of 2005–20107,8. Similarly, TH use increased from 28.4% to 85.6% between 2006 and 2010 in the United Kingdom18,19. Finally, Wils and coworkers reported up to 98.7% adherence to recommendations regarding TTM in Netherlands. Interestingly, 25% of ICUs had adapted their TTM protocol to a target temperature of 36 °C only several months after publication of TTM trial. It was a surprisingly rapid adoption of TTM practices compared to introduction of TH in the early 2000s20. Maybe TTM in CA patients would be more popular after 2015 resuscitation guidelines. But it was not until 2012 that TH was first used for CA patients in China. And to date only a few healthcare providers knew the concept of TTM and fewer of them had implemented it in practice. This was particularly prominent in nurses. It did reveal that healthcare providers in EDs or ICUs were failing to keep up with clinical developments and there was a huge gap between the TTM practice in China and that recommended by guidelines. In previous studies, providers have cited technical difficulties, a lack of financial or personnel resources to initiate TH14,21. Similarly in our study, one major impediment was that they felt too technically difficult to perform. The following two reasons for physicians were lack of TH-related equipment and being afraid of potential TH-related adverse effect. But nurses cited unknown field as the second reason for not cooling, reflecting the need for education to promote TTM awareness.
Cooling methods
Although more than 50% of the physicians believed that intravascular cooling was better in temperature control and improvement of outcomes in CA patients, external cooling was the most common method to induce and maintain TH in practice. Similarly, other surveys observed that surface cooling were mostly used in ICUs, usually reaching about 50–60%18,22. Mainly because surface cooling was easy to use and could be started immediately without invasive procedure23. The available data on safety and efficacy of different cooling technologies is limited. Most published studies were small, often retrospective and/or had evaluated only a single cooling device or method24. Until 2014 a prospective multicenter RCT found that compared to external cooling, intravascular methods provided a target temperature faster, smaller temperature fluctuations in the maintenance phase and reduced nursing workload25. Rosman and his colleagues had got the similar conclusions later26. But none had found statistically significant differences in patient outcomes between different cooling methods25,26,27.
TTM modifications after publication of 2015 AHA guidelines for CPR
Since the publication of 2015 AHA resuscitation guidelines3, 57.2% of physicians and 42.5% of nurses declared a target temperature’s change in future practice. Now the optimal target temperature was still unknown. A large RCT published in 2013 found no difference between strict temperature control at 33.0 °C compared to 36 °C28. Although the conclusions of this study have been criticized for problems such as potential selection bias, rapid rewarming, and other issues29. It did have an impact on guidelines and clinical practice. An international survey found that 37% of ICUs in 11 countries declared a practical target temperature change30. 19.2~40.4% of ICUs had adopted non 32~34 °C as new target temperature20,30,31. To the best of our knowledge, this is the first survey about TTM modifications after publication of 2015 guidelines.
The guidelines did have impact on attitude in choosing target temperature for TTM. The new target temperature 35 °C∼36 °C and 36 °C were preferred by 54.7% and 7.4% of the respondents respectively after guidelines publication, as compared to that 32 °C∼34 °C was preferred by 54.0% of respondents before publication. Similarly as observed in other surveys, clinicians who changed target temperature were more likely to choose a TTM set around 36°C30,32. But Bray and coworkers found that change from a post-arrest temperature target of 33 °C to 36 °C might lead to low compliance with target temperature and higher rates of fever which was associated with poorer patient outcomes32. Casamento et al. also reported high proportions of temperatures above target and fever (≥38 °C) across the first 24 h of ICU stay on the 36 °C protocol33. Mainly because shivering was usually more active at temperatures close to the normal range than at temperatures that are several degrees below normal23,34. Maybe it was more difficult to maintain a target temperature at 36 °C.
Improving utilization of TTM
In awareness level
Our study revealed that many healthcare professionals were not familiar with TTM. This lack of knowledge might lead to a negative attitude towards TTM implementation. Such barriers were also primarily identified by Toma et al.35. Education to the physicians and nurses in EDs and ICUs, especially the chief of departments, are crucial to increase the rates of TTM utilization which had been proven effective by Morrison et al.36.
In practice level
The major barrier to cooling was too technically difficult to perform as surveyed in our study. It was similarly reported in previous studies7,14,15,16,37. The solution may lie in publication of standardized cooling protocols and development of regional post cardiac-arrest care system. Although TH has been recommended by resuscitation guidelines3,10, few specific consensus protocols exist to detail how to best implement this complex therapy. The development and publication of standardized cooling protocols will likely help physicians to better utilize this challenging treatment. Furthermore we had established regional post cardiac-arrest TTM care system led by Peking University third hospital in Beijing. The system consisted of 7 level III hospitals. Providers at dedicated TTM centers are available for any protocol or equipment related questions. But the effect needs further evaluation. In addition promoting insurance cover of TTM costs may be another effective method to improve its use in China.
It was very difficult to conduct a randomized observational survey. Convenience sampling was used in our study in order to get a high response rate. Despite surveyed hospitals were geographically well distributed in this study, it did has disadvantages of convenience sampling. The survey may have been subject to bias ascertainment as level III hospitals were over-represented, making it likely that the degree of TTM awareness and use reflected in our survey is an optimistic perspective. The true proportion may be lower than that reported in this study.
Conclusions
TTM for CA patients had not been well understood by healthcare providers in EDs or ICUs and was still in the early stage in China. There was a huge gap between TTM practice in China and that recommended by guidelines. Interventions are needed to promote knowledge awareness and translations of guidelines into clinical practice. The publications of 2015 resuscitation guidelines did have impact on attitude in choosing target temperature for TTM. Healthcare providers were more likely to choose 35∼36 °C-TTM after guidelines publication, as compared to that before publication they preferred 32∼34 °C-TTM.
Availability of data and material
The datasets used for this study are available from the corresponding author on reasonable request.
References
Shao, F., Li, C. S., Liang, L. R., Li, D. & Ma, S. K. Outcome of out-of-hospital cardiac arrests in Beijing, China. Resuscitation 85(11), 1411–1417 (2014).
Shao, F. et al. Incidence and outcome of adult in-hospital cardiac arrest in Beijing, China. Resuscitation 102, 51–56 (2016).
Callaway, C. W. et al. Part 8: Post-Cardiac Arrest Care: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015;132(18Suppl 2):S465–S482.
Nolan, J. P. et al. EuropeanResuscitation Council and European Society of Intensive Care Medicine Guidelines for Post-resuscitation Care 2015: Section 5 of the European Resuscitation Council Guidelines for Resuscitation 2015. Resuscitation 95, 202–222 (2015).
Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med 346(8), 549–556 (2002).
Bernard, S. A. et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med 346(8), 557–563 (2002).
Laver, S. R., Padkin, A., Atalla, A. & Nolan, J. P. Therapeutic hypothermia after cardiac arrest: a survey of practice in intensive care units in the United Kingdom. Anaesthesia 61(9), 873–877 (2006).
Krawczyk, P., Fraczek, B. & Drab, E. Use of therapeutic hypothermia in Polish intensive care units. Resuscitation 79(2), 339 (2008).
Orban, J. C. et al. The practice of therapeutic hypothermia after cardiac arrest in France: a national survey. PLoS One 7(9), e45284 (2012).
Peberdy, M. A. et al. Part 9: post-cardiac arrest care: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 122(18Suppl 3), S768–S786 (2010).
Nielsen, N. et al. Targeted temperature management at 33 °C versus 36 °C after cardiac arrest. N Engl J Med 369(23), 2197–2206 (2013).
Rittenberger, J. C. & Callaway, C. W. Targeted temperature management after cardiac arrest. N Engl J Med 370(14), 1360–1361 (2014).
Kudenchuk, P. J. et al. Breakthrough in cardiac arrest: reports from the 4th Paris International Conference. Ann Intensive Care 5(1), 22 (2015).
Abella, B. S., Rhee, J. W., Huang, K. N., Vanden Hoek, T. L. & Becker, L. B. Induced hypothermia is underused after resuscitation from cardiac arrest: a current practice survey. Resuscitation 64(2), 181–186 (2005).
Merchant, R. M. et al. Therapeutic hypothermia utilization among physicians after resuscitation from cardiac arrest. Crit Care Med 34(7), 1935–1940 (2006).
Wolfrum, S. et al. Mild therapeutic hypothermia after cardiac arrest - a nationwide survey on the implementation of the ILCOR guidelines in German intensive care units. Resuscitation 72(2), 207–213 (2007).
ECC Committee, Subcommittees and Task Forces of the American Heart Association. 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2005;112(24 Suppl):V1-V203.
Krawczyk, P., Kolodziej, G., Szpyra, B. & Andres, J. Implementation of therapeutic hypothermia after cardiac arrest in intensive care units in Poland. Kardiol Pol 71(3), 270–274 (2013).
Binks, A. C. et al. Therapeutic hypothermia after cardiac arrest - implementation in UK intensive care units. Anaesthesia 65(3), 260–265 (2010).
Wils, E. J., van den Berg, T. & van Bommel, J. Current practice of target temperature management post-cardiac arrest in The Netherlands, a post-TTM trial survey. Resuscitation 97, e1–e2 (2015).
Nichol, G. et al. Does induction of hypothermia improve outcomes after in-hospital cardiac arrest? Resuscitation 84(5), 620–625 (2013).
Gasparetto, N. et al. Therapeutic hypothermia in Italian Intensive Care Units after 2010 resuscitation guidelines: still a lot to do. Resuscitation 85(3), 376–380 (2014).
Polderman KH. How to Stay Cool in the ICU? Endovascular vs. Surface Cooling. Circulation 2015.
Polderman, K. H. & Herold, I. Therapeutic hypothermia and controlled normothermia in the intensive care unit: practical considerations, side effects, and cooling methods. Crit Care Med 37(3), 1101–1120 (2009).
Deye, N. et al. Endovascular Versus External Targeted Temperature Management for Patients With Out-of-Hospital Cardiac Arrest: A Randomized, Controlled Study. Circulation 132(3), 182–193 (2015).
Rosman, J. et al. A comparison between intravascular and traditional cooling for inducing and maintaining temperature control in patients following cardiac arrest. Anaesth Crit Care Pain Med (2016).
Oh, S. H. et al. An observational study of surface versus endovascular cooling techniques in cardiac arrest patients: a propensity-matched analysis. Crit Care 19, 85 (2015).
BroJeppesen, John et al. Hemodynamics and Vasopressor Support During Targeted Temperature Management at 33 °C Versus 36 °C After Out-of-Hospital Cardiac Arrest: A Post Hoc Study of the Target Temperature Management Trial. Critical Care Medicine (2014).
Polderman, K. H. & Varon, J. Interpreting the results of the targeted temperature management trial in cardiac arrest. Ther Hypothermia Temp Manag 5(2), 73–76 (2015).
Deye, N. et al. Changes in cardiac arrest patients’ temperature management after the 2013 “TTM” trial: results from an international survey. Ann Intensive Care 6(1), 4 (2016).
Ford, A. et al. Management of cardiac arrest survivors in UK intensive care units: a survey of practice. Journal of the Intensive Care Society 17 (2015).
Bray, J. E. et al. Changing target temperature from 33 °C to 36 °C in the ICU management of out-of-hospital cardiac arrest: A before and after study. Resuscitation 113, 39–43 (2017).
Casamento, A. et al. A comparison of therapeutic hypothermia and strict therapeutic normothermia after cardiac arrest. Resuscitation 106, 83–88 (2016).
Silverman, M. G. & Scirica, B. M. Cardiac arrest and therapeutic hypothermia. Trends in Cardiovascular Medicine 26(4), 337 (2016).
Toma, A. et al. Perceived barriers to therapeutic hypothermia for patients resuscitated from cardiac arrest: a qualitative study of emergency department and critical care workers. Critical Care Medicine 38(2), 504 (2010).
Morrison, L. J. et al. Improving use of targeted temperature management after out-of-hospital cardiac arrest: a stepped wedge cluster randomized controlled trial. Crit Care Med 43(5), 954–964 (2015).
Kim, Y. M., Lee, S. J., Jo, S. J. & Park, K. N. Implementation of the guidelines for targeted temperature management after cardiac arrest: a longitudinal qualitative study of barriers and facilitators perceived by hospital resuscitation champions. BMJ Open 6(1), e9261 (2016).
Acknowledgements
We would like to thank all the clinical leads who gave their time to complete the survey and respondents who participated in this study. Status Monitoring of Therapeutic Hypothermia for Cardiac Arrest Patients after Resuscitation in Beijing (code: z13110700221314) and The Comparision of ECPR and CCPR in Youth cardiac arrest (code: BYSY2016005).
Author information
Authors and Affiliations
Contributions
Lanfang Du, Baolan Ge, Qingbian Ma have made contributions to the conception and design of the study, acquisition of data, analysis and interpretation of data, drafting the article and final approval of the version. Jianzhong Yang, Fengying Chen, Yuhong Mi, Huadong Zhu, Cong Wang, Yan Li, Hongbo Zhang, Rongjia Yang, Jian Guan, Xiongyi Zhang, Yungui Jin, Haiyan Zhu, Yan Xiong, Guoxing Wang, Zhengzhong Zhu, Haiyan Zhang, Yun Zhang, Jihong Zhu, Jie Li, Chao Lan, Hui Xiong have made important contributions to the conception and design of the study and acquisition of data.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Du, L., Ge, B., Ma, Q. et al. Changes in cardiac arrest patients’ temperature management after the publication of 2015 AHA guidelines for resuscitation in China. Sci Rep 7, 16087 (2017). https://doi.org/10.1038/s41598-017-16044-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-16044-7
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
