
Abstract
This study aims to investigate the efficacy of bevacizumab-combined chemotherapy (BCC) in Chinese stage IV colorectal cancer (CRC), and analyze the relationship between clinicopathological features with survival. Patients with stage IV CRC treated with BCC were analyzed retrospectively. 217 metastatic CRC (mCRC) patients were collected, out of which79 were right-sided CRCs and 138 were left-sided ones. Patients with Eastern Cooperative Oncology Group (ECOG) performance status ≤2, single agent chemotherapy, poor/mucous/signet ring cell component, second-and further-line of bevacizumab administration, multiple metastasis sites had comparatively worse survival. Among 141 patients with known KRAS status, 55 patients harbored KRAS mutation and 86 had wild type KRAS. The ORR and DCR were 41.9% and 78.9%, respectively, in patients with wild type KRAS, while ORR and DCR was 38.7% and 77.9%, respectively, in patients with KRAS mutation. The median PFS of patients with wild type and mutant KRAS were 8.38, and9.59 months, respectively; whereas the OS was 23.00 and 21.26 months, respectively for mCRC patients with wild-type and mutant KRAS. Cumulatively, our study indicated that BCC was effective and beneficial for Chinese stage IV CRC patients. KRAS mutation status and tumor location were not a prognostic factor for survival.
Similar content being viewed by others

Introduction
Colorectal cancer (CRC) is one of the most common malignancies globally and is the third major cause of cancer morbidity and mortality1. In China, stage IV constitutes more than 10% of the total CRC patients. In stage IV CRC patients, multiple treatment modalities including surgical resection, chemotherapy and radiotherapy are the current methods of choice. In recent years, with the development of our understanding the signaling pathway and mechanism of tumorigenesis, targeted therapy pervaded in anti-cancer regimens and demonstrated further clinical benefits in combination with systemic chemotherapy. Bevacizumab is one of the most successful biologic agents in treating stage IV CRC2.
Neoangiogenesis is one of the hallmarks of cancer3. One of the important regulators of neoangiogenesis is vascular endothelial growth factor (VEGF)4. VEGF expression is highly induced in tumor tissue and is associated with tumor cell proliferation, invasion and metastasis. By downregulating VEGF expression, tumor growth can be inhibited5. Bevacizumab, a recombinant humanized monoclonal IgG antibody, selectively combines with VEGF-A inhibiting its binding the VEGF receptors, thus avoiding VEGF-mediated angiogenesis6,7. The AVF2107g clinical trial demonstrated that bevacizumab combined with chemotherapy prolonged the survival of patients with stage IV CRC8. Based on results from this study, bevacizumab was first approved by the United States Food and Drug Administration (FDA) for stage IV CRC in combination with other cytotoxic agents. Based on numerous clinical trials9,10,11,12,13,14, in the National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology (NCCN Guidelines) for colon and rectal cancer, bevacizumab is recommended as first-, second- and even cross line treatment after first disease progression for stage IV CRC.
While the benefits of treatment with bevacizumab are well studied in American and European patients with stage IV CRC, the effect and safety of treatment with bevacizumab combined chemotherapy in Chinese patients, and whether the KRAS mutation status and primary tumor site could affect the prognosis of Chinese stage IV CRC have not been demonstrated clearly. This retrospective study aimed at investigating the efficacy and safety profile of combination treatment with bevacizumab in Chinese stage IV CRC patients and analyzing prognostic factors for predicting patients’ survival.
Methods
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study protocol was approved by the Institutional Review Board of Chinese PLA General Hospital.
Study population
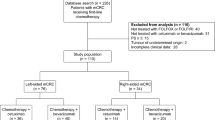
This retrospective study included 217 patients with stage IV CRC who had been treated with bevacizumab-containing chemotherapy between May 1, 2011 and August 1, 2015 in Chinese PLA General Hospital. Patients who met the following criterions were included in this study: (1) histologically confirmed colorectal adenocarcinoma with clinical and/or histological evidences of distant metastasis cancer; (2) ECOG performance status (PS) ≤2; (3) life expectancy >3 months; (4) measurable disease consistent with the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, (5) adequate organ function, including liver and kidney (total bilirubin ≤1.5-times the institutional upper normal limit, aspartate aminotransferase and alanine aminotransferase ≤2.5-times the institutional upper normal limit, and serum creatinine ≤institutional upper normal limit or creatinine clearance (CCr, calculated using the Cockcroft-Gault formula) ≥50 ml/min); adequate bone marrow function (leucocyte count ≥3000/mm3,neutrophil count ≥1500/mm3, platelet count ≥100,000/mm3, and haemoglobin ≥9.0 g/dl); and, (6) provided signed informed consent. The key exclusion criteria were as follows: no pathological diagnosis; history of malignancy other than CRC; less than 4 cycles of bevacizumab-containing chemotherapy, thus the tumor response could be evaluated at least once; the presence of clinically significant cardiovascular disease; uncontrolled hypertension; bleeding diathesis or coagulopathy; central nervous system metastasis; use of full-dose anticoagulants or thrombolytics; pregnancy or lactation; non-healing wounds; inability to take therapy on time. Patients with no completed clinicopathological and survival data were also excluded.
Treatment
All of the 217 patients included were treated intravenously with 5 mg/kg bevacizumab (Avastin; Genentech, San Francisco, CA, USA) every 2 weeks or 7.5 mg/kg every 3 weeks according to different chemotherapy regimens, prior to the chemotherapy. Bevacizumab was administered initially over 90 minutes, and if the first infusion was well tolerated, the second was delivered no less than 60 minutes, and if well tolerated, the subsequent administration was over 30 minutes. Bevacizumab was temporarily or permanently reduced or forbidden in case of serious bevacizumab-related toxicity. Among the 217 patients included in this retrospective study, 75 patients received bevacizumab combined with XELOX chemotherapy, 41 patients received FOLFOX chemotherapy, 67 patients received FOLFIRI chemotherapy; 10 patients received oxaliplatin only; 8 patients received irinotecan alone; 10 received raltitrexed chemotherapy; 6 patients received 5-fluoropyrimidine or capecitabine chemotherapy. The chemotherapy regimens are detailed in Table 1.
Clinical Outcome Assessments
The long-term effectiveness measures included PFS, which is defined as the duration from the start of the initial bevacizumab-containing therapy to the first recorded occurrence of disease progression or death; overall survival (OS), which is calculated as the duration from the initiation of the bevacizumab-containing therapy to death or censoring. Patients without an event who still remained in follow-up were censored on the last follow-up date, July 31, 2016. Short-term effective objectives included overall response rate (ORR) and disease-control rate (DCR). Baseline tumor statuses of targeted lesions were evaluated using computer tomography (CT) scan of the chest, abdominal and pelvis. Tumor responses were evaluated at the completion of each 6-week cycle according to RECIST.
Statistical analyses
For survival analyses, the Kaplan–Meier method was used to estimate the correlation between PFS, OS rates and clinicopathological variables, at 95% CI. The log-rank test was used to compare survival curves. All the statistical analysis was conducted by SPSS 19.0 software package and a P < 0.05 was considered as statistically significant.
Results
Patient characteristics
217 stage IV CRC patients (120 men, 97 women, median age 58 years old) treated with bevacizumab-containing chemotherapy between May 1, 2011 and August 1, 2015 in Chinese PLA General Hospital were collected and retrospectively analyzed. Baseline demographics and clinical characteristics are summarized in Table 1. 169 patients had an ECOG PS scored 0–1 and 48 patients scored 2 at the initial bevacizumab administration. The number of metastasis in no more than 2 organs was discovered in 156 patients till the last follow-up date. The most common metastatic organ was liver (158 patients), 106 of whom suffered from synchronous liver metastases. One hundred fifty three patients received primary tumor surgery.
Short-term effect
Among 217 patients, 193 patients had progressive disease, out of whom 118 patients expired by the last follow-up date. The total ORR was 38.3% and DCR was 87.1%. The ORR and DCR were 51.5% and 96.2% when bevacizumab was administered in first-line therapy and 25.5% and 78.2% when administered in second-line therapy. However, ORR and DCR were 10.0% and 53.3% when bevacizumab was given just in third- and forth-line, respectively (Table 2).
Long-term effect
With the median follow-up duration of 27.30 months (range, 11.99–62.52 months), the median PFS and OS were 10.05 and 20.67 months, respectively (Fig. 1, Table 1). Stage IV CRC patients with ECOG 2 had worse PFS and OS than patients with ECOG 0–1 (P < 0.05) (Fig. 2A,B; Table 1).

Progression-free survival (PFS) (A) and overall survival (OS) (B) of 217 stage IV CRC treated with bevacizumab-containing chemotherapy. For details of chemotherapeutic regimen please refer to Table 1. With the median follow-up duration of 27.30 months (range, 11.99–62.52 months), the median PFS and OS were 10.05 and 20.67 months, respectively.

OS (A,C) and PFS (B,D) of stage IV CRC patients with different ECOG (A,B) and under different chemotherapeutic treatment regimens (C,D). Stage IV CRC patients with ECOG = 2 had significantly worse OS and PFS than patients with ECOG 0–1 (P < 0.05) (A,B). The differences of PFS and OS between oxaliplatin-based combined chemotherapies and irinotecan-based ones were not significant (P > 0.05) (C,D).
As for chemotherapy regimens, single agent such as oxaliplatin, irinotecan, 5-fluoropyrimidine, capecitabine and raltitrexed did not prolong the patients’ survival compared with combinatorial chemotherapeutic regimens. There was no statistically significant difference of PFS and OS between oxaliplatin-based combined chemotherapies and irinotecan-based ones (Fig. 2C,D; Table 1).
Poor/mucous/signet ring cell component had different effort on PFS and OS. Poor differentiation, resembling advanced metastatic stage, significantly shortened the OS (P < 0.05) (Fig. 3A) instead of PFS (P > 0.05) (Fig. 3B; Table 1). Similar observations were made for number of metastatic sites with patients with more than 2 sites having a significantly lower OS and PFS (P < 0.05 in each case) (Fig. 3C,D; Table 1).

Effect of bevacizumab on OS and progression-free survival of stage IV CRC patients with different differentiation states (A,B), number of metastatic sites (metastatic sites ≥3 VS 1–2; (C,D)), and based on line of therapy (first line VS ≥ 2 line; (E,F)).
We divided time of bevacizumab regimen to two groups – first line and ≥2 (Table 1). The PFS and OS were directly dependent on how quickly bevacizumab was administered (P < 0.05 in each case) (Fig. 3E,F; Table 1). The other clinicopathological features did not present differential long-term effect.
Primary tumor location and KRAS mutation status
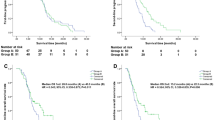
Current evidence suggest that right-sided and left-sided CRC are different diseases15,16,17, and referring to stage IV CRC, right-sided ones had significantly worse survival than left-sided ones15. We were interested in the effect of primary tumor location on bevacizumab-related survival. Among 217 enrolled patients, 79 were right-sided CRCs and 138 were left-sided ones. Left- and right-sided CRC had no difference in overall survival following treatment with bevacizumab-containing chemotherapy (Fig. 4A,B; Tables 2,3). Furthermore we analyzed the differences of survival of right- and left-sided CRC in every line of bevacizumab, and there were still no significant differences (data not shown).

Tumor location and KRAS mutation status had no significant effect on PFS and OS of stage IV CRC receiving bevacizumab chemotherapy. OS (A,C) and PFS (B,D) of stage IV CRC patients with right- or left-sided disease (A,B) and wild type or mutant of KRAS (C,D) (P > 0.05 in each case).
The other commonly used monoclonal antibody in mCRC is cetuximab, which is an anti-EGFR monoclonal antibody18. However, KRAS mutation is a negative predictive marker for anti-EGFR treatment. For this reason, only mCRC with wild type KRAS could be treated with cetuximab19. We wondered if KRAS mutation status would affect bevacizumab efficacy, so patients who had the KRAS status information (n = 141) were divided in to KRAS mutation group (n = 55) and wild type group (n = 86). The ORR and DCR were 41.9% and 87.2% in patients with wild type KRAS, while 38.2% and 85.5% in patients with mutant KRAS. The median PFS and OS of KRAS wild type and mutation type were 8.44 vs 9.43 months and 24.61 vs 19.09 months, but the differences were not significant (P > 0.5) (Fig. 4C,D; Tables 1,2).
Discussion
After bevacizumab was initially approved by the FDA for stage IV colorectal cancer in 2004 based on the results of the AVF2107g RCT, it became one of the standards for first-line, second-line and cross-line therapeutic regimen20. The addition of bevacizumab to chemotherapy had been shown to prolong stage IV CRC patients’ survival in multiple randomized controlled clinical trial (RCT) from European and North American countries, where people were mostly Caucasian. A multiple-centered phase III RCT launched in the United States of America in 2004 containing 402 mCRC patients to receive irinotecan, bolus fluorouracil, and leucovorin (IFL) plus bevacizumab and 411 to receive IFL and placebo. The median OS and PFS of combination group were 20.3 and 10.6 months, the ORR was 44.8%. While in IFL group, OS and PFS were 15.6 and 6.2 month, with an ORR of 34.8%8. Follow-up clinical trials were conducted to explore the effect of bevacizumab administration during every phase of therapy (important phase III ones are summarized in Table 4).
The BEAT study established the combination chemotherapy plus bevacizumab other than monotherapy as the standard therapy for mCRC first-line treatment11. However, all RCTs did not get equivalent results. In the N016966 study, even though bevacizumab administration resulted in longer PFS, it did not have the same effect on OS12. The CARIO3 and MACRO phase III studies proved the benefit bevacizumab when used only as maintenance therapy21,22. The E3200 study, where mCRC patients treated with FOLFIRI were enrolled, revealed that the addition of bevacizumab significantly improved survival after first progression13. The ML18147 and BEBYP studies revealed the benefits of continuation of bevacizumab even after initial chemotherapeutic resistance14,23.
In China where people are mostly of Mongoloid decent, the evidence of RCT study in bevacizumab was not as sufficient as described above. The ARTIST study, a phase III RCT study, demonstrated that in Chinese population bevacizumab could increase mCRC survival significantly24. Oncologists in China mostly decide therapeutic regimens following international guidelines and additional experiences of bevacizumab administration are required. In the present study, we obtained similar results as RCT studies discussed above. The subtle differences in duration of survival and response rate may due to the different regimens and population.
The poor survival and the prognostic impact of KRAS mutation in the CRC have been previously reported25. It was shown that KRAS mutation status did not have a significant effect on the PFS in first-line treatment of mCRC26. Hurwitz et al. (2009) reported that the clinical benefit of bevacizumab in mCRC was independent of KRAS mutation status; bevacizumab provided significant clinical benefit in patients with mCRC expressing either mutant or wild-type KRAS 27. We explored the efficacy of bevacizumab-contained chemotherapy for stage IV CRC patients according to different KRAS mutation status. Our result revealed that patients with KRAS mutation had a shorter survival than patients with wild type KRAS wild type; however, the difference was not statistically significant.
Current evidence indicates that right- and left-sided CRC respond differently to treatment. Proximal and distal colon show different pathways to develop and tumorigenesis. The proximal colon originating from the embryonic midgut is perfused by the superior mesenteric artery, however the distal colon deriving from the hindgut is supplied by the inferior mesenteric artery28. KRAS mutations were more frequently found in the right than left Dukes’ C colon cancer29. The patients with right-sided CRC were older female, poorly differentiated and suffered from poorer survival30. The more active EGFR signaling in distal CRC meant that left-sided cancers benefited significantly more from cetuximab31,32. In addition, it was shown using data obtained from PROVETTA, AVF2107g and NO16966 trials, that even though efficacy of bevacizumab was independent of tumor location, patients with left-sided tumors had significantly better outcomes33.
In the current study, we analyzed the short and long term efficacy in different anatomic sites of mCRC treated with bevacizumab. We divided mCRC into right- and left-sided groups and found that tumor location was not a prognostic factor for survival. Although the median PFS, OS and response rate of right-sided mCRC were all worse than left-sided cancers, none of the differences achieved statistical significance, which is contradictory with two previous reports33,34. The difference is perhaps because of the different population and line of bevacizumab administration. This highlights the importance of similar studies in the context of different population and analytic setting.
Statement of Ethics
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
References
Siegel, R. L., Miller, K. D. & Jemal, A. Cancer statistics, 2015. CA: a cancer journal for clinicians (2015).
Cidon, E. U., Alonso, P. & Masters, B. Markers of Response to Antiangiogenic Therapies in Colorectal Cancer: Where Are We Now and What Should Be Next? Clinical Medicine Insights Oncology. 10(Suppl 1), 41–55 (2016).
Hanahan, D. & Weinberg, R. A. Hallmarks of cancer: the next generation. Cell. 144(5), 646–674 (2011).
Kajdaniuk, D., Marek, B., Foltyn, W. & Kos-Kudla, B. Vascular endothelial growth factor (VEGF) -part 2: in endocrinology and oncology. Endokrynol Pol. 62(5), 456–464 (2011).
Pavlidis, E. T. & Pavlidis, T. E. Role of bevacizumab in colorectal cancer growth and its adverse effects: a review. World J Gastroentero. 19(31), 5051–5060 (2013).
Kramer, I. & Lipp, H. P. Bevacizumab, a humanized anti-angiogenic monoclonal antibody for the treatment of colorectal cancer. J Clin Pharm Ther. 32(1), 1–14 (2007).
Jain, R. K. Normalizing tumor vasculature with anti-angiogenic therapy: a new paradigm for combination therapy. Nat Med. 7(9), 987–989 (2001).
Hurwitz, H. et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. New Engl J Med. 350(23), 2335–2242 (2004).
Kozloff, M. et al. Clinical outcomes associated with bevacizumab-containing treatment of metastatic colorectal cancer: the BRiTE observational cohort study. Oncologist. 14(9), 862–870 (2009).
Bendell, J. C. et al. Treatment patterns and clinical outcomes in patients with metastatic colorectal cancer initially treated with FOLFOX-bevacizumab or FOLFIRI-bevacizumab: results from ARIES, a bevacizumab observational cohort study. Oncologist. 17(12), 1486–1495 (2012).
Van Cutsem, E. et al. Safety and efficacy of first-line bevacizumab with FOLFOX, XELOX, FOLFIRI and fluoropyrimidines in metastatic colorectal cancer: the BEAT study. Ann Oncol. 20(11), 1842–1847 (2009).
Saltz, L. B. et al. Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: a randomized phase III study. J Clin Oncol. 26(12), 2013–2019 (2008).
Giantonio, B. J. et al. Bevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previously treated metastatic colorectal cancer: results from the Eastern Cooperative Oncology Group Study E3200. J Clin Oncol. 25(12), 1539–1544 (2007).
Bennouna, J. et al. Continuation of bevacizumab after first progression in metastatic colorectal cancer (ML18147): a randomised phase 3 trial. Lancet Oncol. 14(1), 29–37 (2013).
Meguid, R. A., Slidell, M. B., Wolfgang, C. L., Chang, D. C. & Ahuja, N. Is there a difference in survival between right- versus left-sided colon cancers? Ann Surg Oncol. 15(9), 2388–2394 (2008).
Gervaz, P., Buhler, L., Scheiwiller, A. & Morel, P. A tale of two colons and two cancers. Distinct carcinogenesis and clinical outcome according to location proximal or distal to the splenic flexure. Swiss surgery = Schweizer Chirurgie = Chirurgie suisse = Chirurgia svizzera. 9(1), 3–7 (2003).
Benedix, F. et al. Comparison of 17,641 patients with right- and left-sided colon cancer: differences in epidemiology, perioperative course, histology, and survival. Dis Colon Rectum. 53(1), 57–64 (2010).
Ciardiello, F. et al. Antiangiogenic and antitumor activity of anti-epidermal growth factor receptor C225 monoclonal antibody in combination with vascular endothelial growth factor antisense oligonucleotide in human GEO colon cancer cells. Clin Cancer Res. 6(9), 3739–3747 (2000).
De Roock, W. et al. Effects of KRAS, BRAF, NRAS, and PIK3CA mutations on the efficacy of cetuximab plus chemotherapy in chemotherapy-refractory metastatic colorectal cancer: a retrospective consortium analysis. Lancet Oncol. 11(8), 753–7 62 (2010).
Wu, Q., Shi, Y., Chen, L., Xiao, X. & Dai, G. Effect and safety of bevacizumab-containing chemotherapy treatment in Chinese patients with metastatic colorectal cancer. Oncotargets Ther. 6, 485–490 (2013).
Simkens, L. H. et al. Maintenance treatment with capecitabine and bevacizumab in metastatic colorectal cancer (CAIRO3): a phase 3 randomised controlled trial of the Dutch Colorectal Cancer Group. Lancet. 385(9980), 1843–1852 (2015).
Diaz-Rubio, E. et al. First-line XELOX plus bevacizumab followed by XELOX plus bevacizumab or single-agent bevacizumab as maintenance therapy in patients with metastatic colorectal cancer: the phase III MACRO TTD study. oncologist. 17(1), 15–25 (2012).
Masi, G. et al. Continuation or reintroduction of bevacizumab beyond progression to first-line therapy in metastatic colorectal cancer: final results of the randomized BEBYP trial. Ann Oncol. 26(4), 724–730 (2015).
Guan, Z. Z. et al. Efficacy and safety of bevacizumab plus chemotherapy in Chinese patients with metastatic colorectal cancer: a randomized phase III ARTIST trial. Chin J Cancer. 30(10), 682–689 (2011).
Sinicrope, F. A. et al. Prognostic impact of deficient DNA mismatch repair in patients with stage III colon cancer from a randomized trial of FOLFOX-based adjuvant chemotherapy. J Clin Oncol. 31(29), 3664–3672 (2013).
Cabart, M. et al. KRAS mutation does not influence oxaliplatin or irinotecan efficacy, in association with bevacizumab, in first line treatment of metastatic colorectal cancer. B Cancer. 103(6), 541–551 (2016).
Hurwitz, H. I. et al. The clinical benefit of bevacizumab in metastatic colorectal cancer is independent of K-ras mutation status: analysis of a phase III study of bevacizumab with chemotherapy in previously untreated metastatic colorectal cancer. 14(1), 22–28 (2009).
Iacopetta, B. Are there two sides to colorectal cancer? Int J Cancer. 101(5), 403–8 (2002).
Bleeker, W. A. et al. Impact of KRAS and TP53 mutations on survival in patients with left- and right-sided Dukes’ C colon cancer. Am J Gastroenterol. 95(10), 2953–7 (2000).
Benedix, F., Meyer, F., Kube, R., Gastinger, I. & Lippert, H. Right- and left-sided colonic cancer - different tumour entities. zbl Chir. 135(4), 312–317 (2010).
Missiaglia, E. et al. Distal and proximal colon cancers differ in terms of molecular, pathological, and clinical features. Ann Oncol. 25(10), 1995–2001 (2014).
Sunakawa Y, et al. Prognostic Impact of Primary Tumor Location on Clinical Outcomes of Metastatic Colorectal Cancer Treated With Cetuximab Plus Oxaliplatin-Based Chemotherapy: A Subgroup Analysis of the JACCRO CC-05/06Trials. Clin Colorectal Can. (2016).
Loupakis, F. et al. Primary tumor location as a prognostic factor in metastatic colorectal cancer. J Natl Cancer Inst. 107(3), pii.dju427 (2015).
Wong, H. L. et al. Impact of Primary Tumor Site on Bevacizumab Efficacy in Metastatic Colorectal Cancer. Clin Colorectal Can. 15(2), e9–e15 (2016).
Acknowledgements
This study was supported by the Chinese PLA General Hospital.
Author information
Authors and Affiliations
Contributions
D.C.S. and Y.S. participated in the design of the study, Y.R.W. and Y.L. performed data analysis. H.Y. helped to revise the manuscript. H.M. carried out data collection, Z.K.W. and Z.Y.W. helped to draft the manuscript. W.W.S. and G.H.D. performed statistical analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sun, Dc., Shi, Y., Wang, Yr. et al. KRAS mutation and primary tumor location do not affect efficacy of bevacizumab-containing chemotherapy in stagae IV colorectal cancer patients. Sci Rep 7, 14368 (2017). https://doi.org/10.1038/s41598-017-14669-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-14669-2
This article is cited by
-
Targeted therapy for metastatic colorectal cancer: what do we currently have in clinical practice?
Drugs & Therapy Perspectives (2022)
-
Extracellular vesicle-miRNAs as liquid biopsy biomarkers for disease identification and prognosis in metastatic colorectal cancer patients
Scientific Reports (2020)
-
The influence of PD-L1 genetic variation on the prognosis of R0 resection colorectal cancer patients received capecitabine-based adjuvant chemotherapy: a long-term follow-up, real-world retrospective study
Cancer Chemotherapy and Pharmacology (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
