
Abstract
Altered mean platelet volume (MPV) is implicated in several malignancies. However, the clinicopathological significance and prognostic value of MPV in colorectal cancer (CRC) is still elusive. The purpose of this study was to elucidate the predictive significance of MPV in CRC. The retrospective study recruited 509 consecutive CRC patients between January 2009 and December 2009. The relationships between MPV and clinicopathological characteristics were analyzed. Kaplan-Meier method and Cox regression were used to evaluate the prognostic impact of MPV. Of the 509 CRC patients, high MPV levels were detected in 150 (29.5%) patients. Elevated MPV was associated with tumor differentiation (p < 0.001). Patients with increased MPV had poor overall survival compared with those with normal level (60.0% vs. 83.6%, log-rank test, p = 0.035). Cox regression analysis showed that MPV was an independent prognostic factor in CRC (HR = 1.452, 95% CI = 1.118–1.884, p = 0.005). In conclusion, MPV is easily available in routine blood test. Elevated MPV might act as a marker of prognosis and therapeutic target for CRC.
Similar content being viewed by others

Introduction
Colorectal cancer (CRC) is the third most commonly diagnosed cancer in males and the second in females. Although there are many established therapeutic strategies including surgery, chemotherapy and radiotherapy, the high rate of relapse and distant metastasis still threaten a large percentage of patients. Therefore, identification of appropriate markers for prognosis in CRC is of great importance.
Platelets play a pivotal role in cancer progression and metastasis. There is emerging evidence to suggest that platelets mediate tumor cell growth, angiogenesis, and dissemination1. Increased platelets are correlated with a decrease in overall survival and poorer prognosis in various types of cancer, including pancreatic cancer, gastric cancer, colorectal cancer, endometrial cancer, and ovarian cancer2,3,4,5,6. However, platelet count is determined by the balance between the rate of production and consumption of platelets. A normal platelet count could conceal the presence of highly hypercoagulative and pro-inflammatory cancer phenotypes in the presence of efficient compensatory mechanisms7.
Mean platelet volume (MPV), the most commonly used measure of platelet size, is a surrogate marker of platelet activation8. Altered MPV levels were found in gastric cancer, ovarian cancer, lung cancer, and breast cancer9,10,11,12. Our previous study demonstrated that MPV was elevated in CRC13. In a small-size sample study, MPV was found to be a prognostic indicator in metastatic colorectal cancer patients treated with bevacizumab-combined chemotherapy14.
In the present study, we investigated the effect of MPV levels on pathological parameters and clinical outcome.
Results
Between Jan, 2009 and Dec, 2009, a total of 509 CRC patients were enrolled in this study. Among the 509 patients, 239 (47.0) were women and 270 (53.0) were men, and the median age was 58.1 ± 9.9 years (range 30–87). The characteristics of the patients are reported in Table 1. In terms of the staging system, 243 cases were categorized as stage I and stage II, 266 as stage III and stage IV.
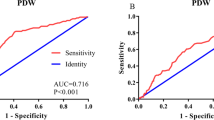
A ROC curve for OS prediction was plotted to verify the optimal cut-off value for MPV, which was 8.6 (Fig. 1). It demonstrated that MPV predicts cancer prognosis with a sensitivity of 33.8% and a specificity of 76.4% (AUC = 0.551, 95% CI: 0.507–0.551, p = 0.011). Then, patients were divided into 2 groups: patients with MPV ≤ 8.6 fL and patients with MPV > 8.6 fL. There were 359 (70.5%) patients with MPV ≤ 8.6 fL and 150 (29.5%) patients with MPV > 8.6 fL.

Optimized cut-off was determined for MPV using standard ROC curve analysis.
The relationships between MPV and clinical characteristics were shown in Table 1 and Table 2. Our study revealed that MPV was associated with tumor differentiation (p < 0.001). However, no significant differences were observed between the groups with regard to age, gender, NLR, PLR, tumor location, tumor size, T classification, lymph node metastasis, distant metastasis, and clinical stage.
With a median follow up of 60 months, 245 (48.1%) patients had death events. Patients with MPV ≤ 8.6 fL had a significantly better 5-year OS than patients with MPV > 8.6 fL (60.0% vs. 83.6%, p = 0.035). The Kaplan-Meier OS curves of the normal versus elevated MPV showed a significant separation (Fig. 2).

Kaplan–Meier analysis of overall survival in CRC patients.
In univariate analysis, age (categorical variable), MPV (categorical variable), WBC, hemoglobin, NLR, PLR, tumor location, differentiation, T classification, lymph node metastasis, distant metastasis, and TNM stage were significant predictors of OS (Table 3). Other parameters were not found to be in correlation with OS. Next, all the factors with a P value less than 0.10 in univariate analysis were included in multivariate analysis (Table 4). In multivariate analyses, we demonstrated that MPV was an independent prognostic factor in CRC patients. Patients with MPV > 8.6 fL had a hazard ratio (HR) of 1.452 [95% confidence interval (CI): 1.118–1.884, p = 0.005] for OS.
Discussion
This study found that MPV is correlated with patient’s survival and is an independent risk factor for prognosis. Our findings indicted the potential importance of assessing CRC prognosis by combining clinicopathological characteristics with platelet index.
Thrombocytosis is associated with reduced survival in several cancers, such as lung cancer, ovary cancer, endometrium cancer, rectum cancer, kidney cancer, gastric cancer, pancreas cancer, and breast cancer. Increased platelets facilitate cancer progression and metastasis by promoting angiogenesis and tumor cell establishment at distant sites15.
The explanation for the association between MPV and survival in CRC is not fully understood. Numerous studies have identified enhanced platelet activation occurred in CRC patients. Phospholipase A2 and platelet-activating factor (PAF) acetylhydrolase were two enzymes implicated in PAF production and degradation. Previous study reported that those two enzymatic activities were elevated in CRC patients16. Platelet-derived endothelial cell growth factor, an angiogenic factor, was found to undergo increased expression and to be an independent prognostic factor in CRC patients17, 18. Moreover, permanent inactivation of platelet COX-1 by low-dose aspirin might restore anti-tumor reactivity19. These data are also consistent with the current knowledge that anti-platelet is considered to be a part of cancer adjuvant therapy1. MPV is an early indicator of activated platelets and is available in any clinical practice. Platelets with elevated MPV contain more α-granules and release more prothrombotic substances, and these substances aggravate inflammation20. Recent studies confirmed higher levels of MPV in CRC patients13, 14. The current study further revealed the prognostic role of preoperative MPV in CRC patients. After curative treatment, 30% of patients with stage I-III and up to 65% of patients with stage IV CRC develop recurrent disease21. Our previous study showed the patients with colon cancer had higher MPV levels compared with normal controls, and MPV levels were reduced after surgery13. Therefore, MPV may be an easy approach for surveillance in post-operative CRC patients. In addition, MPV could be assessed in routine clinical practice without extra cost.
The potential limitations of the present study should be acknowledged. First, this was a single-center retrospective study and additional larger validation studies are needed to confirm our results. Second, we were unable to explore the exact mechanism of MPV in CRC. Third, the patients were composed of Chinese. The application to other ethnic groups still needs further investigation.
In conclusion, MPV is easily available with routine blood counts. Elevated MPV may serve as a marker of adverse prognosis in CRC. Further studies are warranted to clarify the exact role of MPV in CRC.
Patients and Methods
Study population
The records of 509 consecutive CRC cases who were admitted to Harbin Medical University Cancer Hospital, Harbin Medical University between January 2009 and December 2009 were retrospectively reviewed. All patients undergone surgical resection. The pathologic diagnoses of CRC were evaluated by two pathologists from biopsy reports. All cases were categorized according to the WHO classification. The pathologists reviewed all biopsy slides and scored the pathologic variables into 3 classes according to the WHO classification as follows: well differentiated (tubular appearance and mild/moderate atypia), moderately differentiated (lumen formation with moderate/severe atypia) and poorly differentiated (solid or medullary appearance, with severe dysplasia). None of the patients received preoperative chemotherapy or radiation therapy. After surgery, patients were treated with radiotherapy and/or chemotherapy or not. 71 patients who were at high risk of local recurrence and distant metastasis due to rejection, poor physical condition or side effects, did not receive adjuvant therapy. Patients were excluded if they had hematological disorders, coronary artery disease, hypertension, diabetes mellitus, and medical treatment with anticoagulant, statins, and acetylic salicylic acid.
Standard demographic and clinicopathological data were collected from the patients’ records in hospital. Survival data were obtained through follow-up. Overall survival (OS) was defined as the interval from the date of diagnosis to death or last follow-up. The median follow-up time was 60 months.
The Institutional Ethics Review Board of Harbin Medical University Cancer Hospital approved this study prior to commencement of data collection and waived the informed consent requirement because it was a retrospective study. All studies were conducted according to guidelines (Declaration of Helsinki) for biomedical research.
Biochemical measurements
Venous blood samples after an 10-hour overnight fasting were collected from the individuals within 1 week prior to surgery. White blood cell (WBC), haemoglobin, and platelet indices were measured by an autoanalyzer (Sysmex XE-2100, Kobe, Japan). The whole blood samples were collected in EDTA-containing tubes, and all samples were processed within 30 minutes after blood collection.
Statistical analysis
The descriptive statistics are presented as means ± SD or medians (interquartile range) for continuous variables and percentages of the number for categorical variables. Inter-group differences in categorical variables were assessed for significance using the Chi-square test; differences in continuous variables were assessed using the Mann-Whitney U test or t-test. The platelet-to-lymphocyte ratio (PLR) was calculated as the absolute platelet count measured in ×109/L divided by the absolute lymphocyte count measured in ×109/L. The neutrophil-to-lymphocyte ratio (NLR) was calculated as the absolute neutrophil count measured in ×109/L divided by the absolute lymphocyte count measured in ×109/L. Kaplan-Meier analysis was used to assess survival. Log-rank tests were used to compare survival of patients between subgroups. The Cox proportional hazards regression model was applied to evaluate multivariate analyses, and those statistically significant characteristics in univariate analysis (p value <0.1) were used to perform multivariate analysis. ROC analysis was conducted to select the optimum cut-off value of MPV dichotomize the patients into low and high groups. A value of p < 0.05 was regarded as a significant difference between groups. All statistical analyses were performed using SPSS Statistics version 22.0 (SPSS Inc., Chicago, IL, USA).
References
Mezouar, S. et al. Role of platelets in cancer and cancer-associated thrombosis: Experimental and clinical evidences. Thromb Res 139, 65–76 (2016).
Ekici, H. et al. Do Leukocyte and Platelet Counts Have Benefit for \Preoperative Evaluation of Endometrial Cancer. Asian Pac J Cancer Prev 16, 5305–5310 (2015).
Long, Y., Wang, T., Gao, Q. & Zhou, C. Prognostic significance of pretreatment elevated platelet count in patients with colorectal cancer: a meta-analysis. Oncotarget, (2016).
Pietrzyk, L., Plewa, Z., Denisow-Pietrzyk, M., Zebrowski, R. & Torres, K. Diagnostic Power of Blood Parameters as Screening Markers in Gastric Cancer Patients. Asian Pac J Cancer Prev 17, 4433–4437 (2016).
Qiu, J. et al. Preoperative plasma fibrinogen, platelet count and prognosis in epithelial ovarian cancer. J Obstet Gynaecol Res 38, 651–657 (2012).
Suzuki, K. et al. Platelets counts closely correlate with the disease-free survival interval of pancreatic cancer patients. Hepatogastroenterology 51, 847–853 (2004).
Seretis, C., Youssef, H. & Chapman, M. Hypercoagulation in colorectal cancer: what can platelet indices tell us. Platelets 26, 114–118 (2015).
Gasparyan, A. Y., Ayvazyan, L., Mikhailidis, D. P. & Kitas, G. D. Mean platelet volume: a link between thrombosis and inflammation. Curr Pharm Des 17, 47–58 (2011).
Kemal, Y., Demirağ, G., Ekiz, K. & Yücel, I. Mean platelet volume could be a useful biomarker for monitoring epithelial ovarian cancer. J Obstet Gynaecol 34, 515–518 (2014).
Kumagai, S. et al. Prognostic significance of preoperative mean platelet volume in resected non-small-cell lung cancer. Mol Clin Oncol 3, 197–201 (2015).
Shen, X. M. et al. Mean platelet volume provides beneficial diagnostic and prognostic information for patients with resectable gastric cancer. Oncol Lett 12, 2501–2506 (2016).
Tanriverdi, O. et al. The mean platelet volume may predict the development of isolated bone metastases in patients with breast cancer: a retrospective study of the Young Researchers Committee of the Turkish Oncology Group (TOG). J BUON 21, 840–850 (2016).
Li, J. Y., Li, Y., Jiang, Z., Wang, R. T. & Wang, X. S. Elevated mean platelet volume is associated with presence of colon cancer. Asian Pac J Cancer Prev 15, 10501–10504 (2014).
Tuncel, T. et al. Mean platelet volume as a prognostic marker in metastatic colorectal cancer patients treated with bevacizumab-combined chemotherapy. Asian Pac J Cancer Prev 15, 6421–6423 (2014).
Meikle, C. K. et al. Cancer and Thrombosis: The Platelet Perspective. Front Cell Dev Biol 4, 147 (2016).
Denizot, Y. et al. Elevated plasma phospholipase A2 and platelet-activating factor acetylhydrolase activity in colorectal cancer. Mediators Inflamm 13, 53–54 (2004).
Matsumura, M. et al. Platelet-derived endothelial cell growth factor/thymidine phosphorylase expression correlated with tumor angiogenesis and macrophage infiltration in colorectal cancer. Cancer Lett 128, 55–63 (1998).
Tsuji, T. et al. Platelet-derived endothelial cell growth factor expression is an independent prognostic factor in colorectal cancer patients after curative surgery. Eur J Surg Oncol 30, 296–302 (2004).
Sciulli, M. G. et al. Platelet activation in patients with colorectal cancer. Prostaglandins Leukot Essent Fatty Acids 72, 79–83 (2005).
Sansanayudh, N. et al. Prognostic effect of mean platelet volume in patients with coronary artery disease. A systematic review and meta-analysis. Thromb Haemost 114, 1299–1309 (2015).
van der Stok, E. P. MCW, S., Grünhagen, D.J., Verhoef, C. & Kuipers, E.J. Surveillance after curative treatment for colorectal cancer. Nat Rev Clin Oncol 14, 297–315 (2017).
Acknowledgements
This work was supported by Science Foundation of Heilongjiang Academy of Medical Science (Grant No. 201714) and Postdoctoral Scientific Research Development Fund (Grant No. LBH-Q16175).
Author information
Authors and Affiliations
Contributions
N.L., Z.W.Y. and X.Z. participated in manuscript preparation, data analysis and editing. T.M.L. and Y.X.S. participated in study design, and manuscript revision. R.T.W. and K.J.Y. participated in study design, data analysis, and manuscript preparation. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, N., Yu, Z., Zhang, X. et al. Elevated mean platelet volume predicts poor prognosis in colorectal cancer. Sci Rep 7, 10261 (2017). https://doi.org/10.1038/s41598-017-11053-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-11053-y
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
