
Abstract
The study was aimed to investigate the pathogens distribution and risk factors for PICC-related bloodstream infection in intensive care unit (ICU) patients. 402 patients placed with PICC in ICU were recruited in the study. The microbiological characteristics of PICC-related infection were investigated by Vitek 2 Compact automated microbial system. Antibiotics sensitivity was performed with disk diffusion and minimum inhibitory concentration (MIC) methods. Multivariate logistic and cox analyses were performed to identify the risk factors for PICC-related infection in ICU patients. 38 PICC-related infection cases were observed, and its morbidity was 9.45%. The morbidity was significantly higher in power PICC cases than that in common PICC cases. Gram-positive bacteria might be responsible for the major infection cases, followed by gram-negative bacteria, and fungi. Drug sensitivity analyses indicated that gram-negative bacteria showed low resistance to carbapenems antibiotics, and Cefperazone/sulbactam. The gram-positive bacterial exhibited sensitive to Teicoplanin and Vancomycin. The isolated fungi showed low resistance to the commonly used antifungal antibiotics. Multivariate analyses demonstrated that power PICC, high Charison scores, diabetes mellitus, double lumens triple lumens were risk factors for PICC-related infections among ICU patients. Power PICC, high Charison scores, diabetes mellitus, multi-lumens are risk factors for PICC-related bloodstream infection in ICU patients.
Similar content being viewed by others
Introduction
Central venous catheters (CVCs) are widely used in clinical setting due to their functional roles in intravenous treatments, laboratory testing, and hemodynamic monitoring1. Peripherally inserted central catheter (PICC), a specialized CVC, play an important role in treatment of hospitalized patients, especially intensive care unit (ICU) patients2. Compared with the traditional CVCs technique, PICC exerts various advantages, such as convenient placement without pleura-pulmonary damage, low cost, and long-term and stable vein access3,4. At present time, PICC has become widespread in clinical management for extended courses of chemotherapy, medication administration, and parenteral nutrition5, especially with the introduce of Power-injected PICC. Power PICC is made of ultra-resistant polyurethane which allows high flow injection using high pressure pump. Power PICC can meet the requirements for high flow rate of intravenous infusion, and multiple-lumen catheters which are common need among patients in ICU ward6. Thus, PICC is increasingly used in ICU setting.
Despite the various advantages of PICC for ICU patients, PICC shows some complications, including catheter-related thrombophlebitis, and bloodstream infection7. PICC-related bloodstream infection represents a severe complication that may lower the life of quality, increase cost, even contribute to mortality8. It is general considered that PICC shows low risk of bloodstream infection, compared with traditional CVCs9,10,11. However, PICC-related bloodstream infection is still a great challenge for ICU patients. To improve the management of PICC-related bloodstream infection, various researches were designed to identify the risk factors for infection among patients placed with PICC. For instance, Baxi et al. reported that multi-lumens and power PICC could increase the risk of PICC-related bloodstream infection12. A study based on cancer patients demonstrated that fixing method, indwelling season, catheter care, and tip position were significantly associated with incidence of PICC-related bloodstream infection13. Nevertheless, there was no consistent conclusion.
In this study, we aimed to investigate the basic characteristics of PICC-related bloodstream infections in ICU patients. Furthermore, multivariate analyses were applied to identify the risk factors for infections based on the study populations. In addition, antibiotics play pivotal roles in treatment of infection. In order to guide the empirical antibiotic application, the microbiological characteristics of PICC-related bloodstream infection was investigated, as well the drug sensitivity analysis.
Materials and Methods
Study population
The following methods were carried out in accordance with the approved guidelines. All authors reviewed the results and approved the final version of the manuscript. This study was approved by the Ethics Committee of the 306th Hospital of Chinese PLA.
All experimental protocols were approved by 306th Hospital of Chinese PLA, written informed consent was obtaining from every patient.
The patients in ICU who were placed PICC at 306th Hospital of Chinese PLA were collected in the study. The current investigation was based on adult group, and the expected survival time of the patients was longer than 14 days. In addition, the patients who were diagnosed with PICC placement contraindication, such as catheter allergy, suspicion of systemic infection, and so on, should be excluded from the research. Demographics information such as gender and age, and basic characteristics including Charlson scores, comorbidities, and antibiotic history were collected. In addition, the PICC characteristics such as indication for insertion, number of lumens, vein and arm of insertion, types of PICC were abstracted from the medical records. The related information of the patients were summarized in Table 1.
PICC setting
The operating procedure for PICC placement was according to the previous description14. All PICC insertion was done by the same vascular access team using sterile barriers and 2% chlorhexidine in alcohol site antisepsis. PICC placement was confirmed based on the portable ultrasonography and interventional radiology, and adjusted according to the finding of the chest radiograph or fluoroscopy. Routine surveillance was performed for all the patients by the same vascular access team. PICC was flushed with 10 mL normal saline daily according to the standard protocol. When PICC was removed or the patients presented a PICC-related bloodstream infection, the follow up investigation was finished. The days for PICC use was defined as the duration between the PICC insertion and removal. The time to infection was considered as the time from PICC insertion to the date of first positive culture isolated.
Definition of PICC-related bloodstream infections
PICC-related bloodstream infections were diagnosed based on the hospital diagnosis, nursing records, and microbiology data. The combined results were defined according to the National Healthcare Safety Network surveillance definition15. The blood specimens should be collected from the patients, when the patients presented with the infectious signs (fever > 38 °C, chills, rigor, hypotension) and without no other infectious sources. PICC-related bloodstream infection was defined as presence of bacteria or fungus in 1 or more blood cultures. The isolated organisms was identified by Vitek 2 Compact automated microbial system (BioMerieux Inc. ver04.02, France). The pathogen responsible for PICC-related bloodstream infection was defined as the organisms isolated from the positive blood culture. When more than one pathogens were isolated from the blood culture, the infection was considered as polymicrobial.
Drug sensitivity test
Antibiotics sensitivity analyses were performed with a disk diffusion method according to the standards of Clinical and Laboratory Standards Institute (CLSI) and the minimum inhibitory concentration (MIC) determined by BIOMIC system (Giles Scirntific, USA).
Statistical analysis
The rates of infection was calculated by percentage (%), moreover, we compared the percentages between Power PICC and common PICC. Demographic parameters and risk factors for PICC related bloodstream infection were summarized by descriptive statistics, and analyzed by chi-square test. Student’s t test was applied for categorical variables analysis. Logistic regression analysis was performed to identify the risk factors for PICC-related infection, and the results were expressed as odds ratios (ORs) and 95% CIs. In addition, Cox proportional hazards regression was also used to evaluate the potential risk factors for PICC-related bloodstream infection according to the time to infection. The statistical analysis were performed in SPSS 18.0 software (SPSS, Inc., Chicago, IL, USA). P value less than 0.05 was considered statistically significant.
Results
Basic characteristics of the study population
402 ICU patients including 199 men and 203 women were enrolled in the investigation. The average age of the patients were 55.99 ± 11.27 years. Among the patients, 167 (41.54%) of them were diagnosed with hypertension, 171 (42.54%) patients were combined with diabetes mellitus, and malignancy cases accounted for 43.03%. Furthermore, 214 (52.23%) cases were with antibiotics application history (Table 1).
The average PICC insertion time for the patients was 31.82 ± 23.17 days, and 215 (53.48) patients received power PICC. The major patients were placed single lumen (40.55%, n = 163) and double lumens (47.01%, n = 189), while only 12.44% (n = 50) patients were placed triple lumens. PICC was most commonly inserted in right arm (55.47%, n = 223) and basilic vein (67.91%, n = 273) (Table 1).
Occurrence rate of PICC-related bloodstream infections
Among the eligible patients, 38 patients (9.45%) presented PICC-related bloodstream infection. Moreover, the morbidity of infection was significantly higher in patients placed power PICC than those receiving common PICC (13.49% vs 4.81%, P = 0.003).
Microbiological characteristics of PICC-related infections
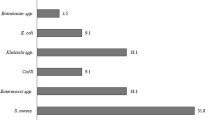
The distributions of pathogens were analyzed for the patients. Analysis results demonstrated that gram-positive bacteria was responsible for the major infection cases (60.53%, n = 23), followed by gram-negative bacteria (31.58%, n = 12). There were 3 (7.89%) infection episodes caused by fungi. The isolated gram-positive bacteria mainly included Staphylococcus aureus (n = 10), Enterococcus spp (n = 5), Staphylococcus haemolyticus (n = 3), Staphylococcus epidermidis (n = 3), and Staphylococcus huminis (n = 2). Furthermore, 2 methicillin-resistant Coagulase negative staphylococci and 5 methicillin-resistant Staphylococcus aureus were identified. Among the gram-negative bacteria, Escherichia coli accounted for 5 cases, Klebsiella pneumoniae accounted for 3 cases, and there were 2 Pseudomonas aeruginosa cases and 2 Acinetobacter baumanii episodes. The isolated fungi included Candida glabrata (n = 1), Candida albicans (n = 1), and Candida parapsilosis (n = 1) (Table 2).
Antibiotics sensitivity analysis for the isolated pathogens
We also investigated the sensitivity of the isolated pathogens to the commonly used antibiotics. The results indicated that gram-negative bacteria were sensitive to carbapenems antibiotics (resistant rate 8.33%), amikacin (8.33%), Cefperazone/sulbactam (25.00%) and Piperacillin/tazobactam (33.33%). The gram-positive bacterial exhibited sensitive to Teicoplanin (0.00%) and Vancomycin (4.35%). Additionally, the isolated fungi showed low resistance to the commonly used antifungal antibiotics (Table 3).
Risk factors for PICC-related bloodstream infections in ICU patients
We compared the medical parameters between infection cases and non-infection patients. As shown in Table 1, diabetes mellitus (P = 0.018), PICC type (P = 0.003), and number of PICC lumens (P = 0.001) were significantly different between the study groups.
In addition, the cumulative hazard curves of PICC-related bloodstream infection was constructed based on the types of PICC and number of lumens. As shown in Fig. 1, the morbidity of infection was significantly higher in patients placed power PICC than those receiving common PICC (log rank test, P = 0.002). The curves constructed according to the number of lumens demonstrated that single lumen would lower the risk of PICC-related infection in ICU patients (log rank test, P = 0.001) (Fig. 2).

The cumulative hazard curves for PICC-related bloodstream infection were plotted based on the types of PICC. The curves suggested that patients placed with power PICC had a significantly higher occurrence of infection than those receiving common PICC (log rank test, P = 0.002).

The cumulative hazard curves for PICC-related infection were constructed according to the number of lumens. Analysis results indicated that compared with double and triple lumens, single lumen would lower the risk of infection in ICU patients (log rank test, P = 0.001).
In order to identify the risk factors for PICC-related bloodstream infections, multivariate logistic and cox analyses were performed in the current study. Logistic analyses demonstrated that power PICC (OR = 4.239, 95%CI = 1.857–9.678, P = 0.001), high Charison scores (OR = 1.137, 95%CI = 1.004–1.287, P = 0.044), diabetes mellitus (OR = 2.663, 95%CI = 1.293–5.482, P = 0.008), double lumens (OR = 3.352, 95%CI = 1.343–8.368, P = 0.010) and triple lumens (OR = 8.018, 95%CI = 2.771–23.202, P = 0.000) were risk factors for infection among ICU patients placed PICC. The results of multivariate cox analysis suggested that power PICC (HR = 4.197, 95%CI = 1.932–9.119, P = 0.000), high Charison scores (HR = 1.120, 95%CI = 1.001–1.253, P = 0.048), diabetes mellitus (HR = 2.370, 95%CI = 1.224–4.588, P = 0.011), double lumens (HR = 2.939, 95%CI = 1.233–7.010, P = 0.015) and triple lumens (OR = 6.352, 95%CI = 2.533–16.580, P = 0.000) were independent risk factors for PICC-related infections (Table 4).
Discussion
At present time, the application of PICC is prevalent in ICU setting. PICC can provide long-term, stable vascular access for medications, parenteral nutrition, and hemodynamic monitoring16. Moreover, PICC can be placed by the specially trained nurses in outpatient department, causing low cost compared with the traditional CVCs17. However, the wide application of PICC may lead to several complications, such as catheter-related thrombophlebitis, and bloodstream infection18. PICC-related infection represents a severe complication that may contribute to prolonged hospital stay, increased medical cost, even mortality8,19. In this study, we investigated the basic and microbiological characteristics of PICC-related bloodstream infection, in order to prevent the incidence of infection and improve the management of PICC-related bloodstream infection.
In the present study, 402 eligible ICU patients were recruited, and 38 of them developed to PICC-related infection. The morbidity of PICC-related infection was 9.45%. Furthermore, we found that the occurrence rate of infection was significantly higher in patients receiving power PICC. Power PICC provide high flow rate of infusion, easy central venous pressure monitoring, and high-pressure injection of contrast media for radiodiagnostic procedures, and multi-lumens that is widely used in ICU as common practice20. Unfortunately, we found that the application of power PICC could increase the risk of PICC-related bloodstream infection, moreover, multivariate analyses proved that it was a risk factor for infection in ICU patients. Baxi et al. reported that power PICC was correlated with increased risk of PICC-related bloodstream infection12. Chopra et al. confirmed that power PICC was a risk factor for PICC-related bloodstream infection21. The two investigations were consistent with our study. However, some researches held opposing viewpoints. The study carried out by Pittiruti et al. demonstrated that the maintenance of power PICC exerted significant advantages in lowering the occurrence of infectious and non-infectious complications22. Thus, further researches were still needed to address the issue.
Compared with common PICC setting, power PICC can provide multi-lumens for simultaneous administration of potentially incompatible drugs6,22. However, growing evidences have indicated that multi-lumens was associated with increased risk of PICC-related complications. It was reported that multi-lumens application was correlated with unacceptable high venous thrombosis rates23,24. The influence of multi-lumens on incidence of PICC-related bloodstream infection was also reported in the previous studies. The related studies demonstrated that multi-lumens could increase the morbidity of infection among patients placed with PICC12,21. In this study, multivariate analyses demonstrated that double and triple lumens were significantly associated with extremely high occurrence of PICC-related bloodstream infection in ICU patients. Taken together, multi-lumens was a risk factor for PICC-complications, and serious monitoring should be taken when multi-lumens PICC was performed for ICU patients. In addition, there was an interesting finding in our research that diabetes mellitus was still a risk factor for PICC-related infection among ICU patients. The association between diabetes mellitus and PICC-related infection had been rarely reported in the previous investigation. The issue was needed to be addressed by further researches.
Timely and appropriate empirical antibiotic treatment is pivotal for outcomes of patients with bloodstream infection25,26. In order to improve the therapeutic effects of antibiotics, it is necessary to investigate the epidemiology of PICC-related bloodstream infection. In this study, we found that gram-positive bacterial such as Staphylococcus aureus, and Enterococcus spp, might be responsible for the major infection cases, followed by gram-negative bacteria including Escherichia coli and Klebsiella pneumoniae, and fungi. Drug sensitivity analyses demonstrated that gram-negative bacteria were sensitive to carbapenems antibiotics, amikacin, Cefperazone/sulbactam and Piperacillin/tazobactam. The gram-positive bacterial exhibited similarly high sensitive to Teicoplanin and Vancomycin. Additionally, the isolated fungi showed low resistance to the commonly used antifungal antibiotics. The antibiotics shown above might be used for empirical treatments for PICC-related infection among ICU patients in our hospital.
In conclusion, PICC-related bloodstream infection is a great challenge for ICU patients. Gram-positive and gram-negative bacteria may represent the major reasons for PICC-related infection. Power PICC, diabetes mellitus, high Charison scores, and multi-lumens may increase the risk of PICC-related infections among ICU patients.
References
Paras-Bravo, P. et al. Complications of Peripherally Inserted Central Venous Catheters: A Retrospective Cohort Study. PLoS One 11, e0162479 (2016).
Perin, D. C., Erdmann, A. L., Higashi, G. D. & Sasso, G. T. Evidence-based measures to prevent central line-associated bloodstream infections: a systematic review. Rev Lat Am Enfermagem 24, e2787 (2016).
Burns, T. & Lamberth, B. Facility wide benefits of radiology vascular access teams. Radiol Manage 32, 28-32; quiz 33-4 (2010).
Walker, G. & Todd, A. Nurse-led PICC insertion: is it cost effective? Br J Nurs 22, S9–15 (2013).
Peng, J. et al. A Novel Two-Step Technique for Retrieving Fractured Peripherally Inserted Central Catheter Segments Migrating into the Heart or the Pulmonary Artery. Biomed Res Int 2016, 7814529 (2016).
Di Giacomo, M. Comparison of three peripherally-inserted central catheters: pilot study. Br J Nurs 18, 8–16 (2009).
Moran, J. et al. Screening for novel risk factors related to peripherally inserted central catheter-associated complications. J Hosp Med 9, 481–9 (2014).
Chopra, V., O’Horo, J. C., Rogers, M. A., Maki, D. G. & Safdar, N. The risk of bloodstream infection associated with peripherally inserted central catheters compared with central venous catheters in adults: a systematic review and meta-analysis. Infect Control Hosp Epidemiol 34, 908–18 (2013).
Gunst, M. et al. Peripherally inserted central catheters may lower the incidence of catheter-related blood stream infections in patients in surgical intensive care units. Surg Infect (Larchmt) 12, 279–82 (2011).
Maki, D. G., Kluger, D. M. & Crnich, C. J. The risk of bloodstream infection in adults with different intravascular devices: a systematic review of 200 published prospective studies. Mayo Clin Proc 81, 1159–71 (2006).
Al Raiy, B. et al. Peripherally inserted central venous catheters in the acute care setting: A safe alternative to high-risk short-term central venous catheters. Am J Infect Control 38, 149–53 (2010).
Baxi, S. M. et al. Impact of postplacement adjustment of peripherally inserted central catheters on the risk of bloodstream infection and venous thrombus formation. Infect Control Hosp Epidemiol 34, 785–92 (2013).
Gao, Y. et al. The incidence and risk factors of peripherally inserted central catheter-related infection among cancer patients. Ther Clin Risk Manag 11, 863–71 (2015).
O’Grady, N. P. et al. Guidelines for the prevention of intravascular catheter-related infections. Am J Infect Control. 39(4 Suppl 1), S1–34 (2011).
O’Grady, N. P. et al. Guidelines for the prevention of intravascular catheter-related infections. Centers for Disease Control and Prevention. MMWR Recomm Rep 51, 1–29 (2002).
Bashir, R. A., Callejas, A. M., Osiovich, H. C. & Ting, J. Y. Percutaneously Inserted Central Catheter-Related Pleural Effusion in a Level III Neonatal Intensive Care Unit: A 5-Year Review (2008–2012). JPEN J Parenter Enteral Nutr (2016).
Johansson, E., Hammarskjold, F., Lundberg, D. & Arnlind, M. H. Advantages and disadvantages of peripherally inserted central venous catheters (PICC) compared to other central venous lines: a systematic review of the literature. Acta Oncol 52, 886–92 (2013).
Nolan, M. E., Yadav, H., Cawcutt, K. A. & Cartin-Ceba, R. Complication rates among peripherally inserted central venous catheters and centrally inserted central catheters in the medical intensive care unit. J Crit Care 31, 238–42 (2016).
Miller, D. L. & O’Grady, N. P. Guidelines for the prevention of intravascular catheter-related infections: recommendations relevant to interventional radiology for venous catheter placement and maintenance. J Vasc Interv Radiol 23, 997–1007 (2012).
Cotogni, P. & Pittiruti, M. Focus on peripherally inserted central catheters in critically ill patients. World J Crit Care Med 3, 80–94 (2014).
Chopra, V. et al. PICC-associated bloodstream infections: prevalence, patterns, and predictors. Am J Med 127, 319–28 (2014).
Pittiruti, M. et al. Clinical experience with power-injectable PICCs in intensive care patients. Crit Care 16, R21 (2012).
Trerotola, S. O. et al. Triple-lumen peripherally inserted central catheter in patients in the critical care unit: prospective evaluation. Radiology 256, 312–20 (2010).
Evans, R. S. et al. Risk of symptomatic DVT associated with peripherally inserted central catheters. Chest 138, 803–10 (2010).
Paul, M. et al. Systematic review and meta-analysis of the efficacy of appropriate empiric antibiotic therapy for sepsis. Antimicrob Agents Chemother 54, 4851–63 (2010).
Retamar, P. et al. Impact of inadequate empirical therapy on the mortality of patients with bloodstream infections: a propensity score-based analysis. Antimicrob Agents Chemother 56, 472–8 (2012).
Author information
Authors and Affiliations
Contributions
S.Z. conceived and designed the experiments; X.S. prepared figures. Y.L. wrote the main manuscript text. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhang, S., Sun, X. & Lei, Y. The microbiological characteristics and risk factors for PICC-related bloodstream infections in intensive care unit. Sci Rep 7, 15074 (2017). https://doi.org/10.1038/s41598-017-10037-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-10037-2
This article is cited by
-
Comparison of microbial colonization rates between central venous catheters and peripherally inserted central catheters
Antimicrobial Resistance & Infection Control (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
