
Abstract
The advent of coronary angiography in the 1960s allowed for the risk stratification of patients with stable angina. Patients with unprotected left main coronary artery disease have an increased risk of death related to the large amount of myocardium supplied by this vessel. Although coronary angiography remains the preferred imaging modality for the evaluation of left main coronary artery stenosis, this technique has important limitations. Angiograms of the left main coronary artery segment can be difficult to interpret, and almost one-third of patients can be misclassified when fractional flow reserve is used as the reference. In patients with clinically significant unprotected left main coronary artery disease, surgical revascularization was shown to improve survival compared with medical therapy and has been regarded as the treatment of choice for unprotected left main coronary artery disease. Two large-scale clinical trials published in 2016 support the usefulness of catheter-based revascularization in selected patients with unprotected left main coronary artery disease. In this Review, we describe the pathophysiology of unprotected left main coronary artery disease, discuss diagnostic approaches in light of new noninvasive and invasive imaging techniques, and detail risk stratification models to aid the Heart Team in the decision-making process for determining the best revascularization strategy for these patients.
Key points
Patients with unprotected left main coronary artery disease have an increased risk of death
Although coronary angiography remains the preferred diagnostic imaging modality for these patients, adjunctive anatomical and physiological methods are often required to assess the clinical significance of the lesion
In patients with unprotected left main coronary artery disease, surgical revascularization was shown to improve survival compared with medical therapy
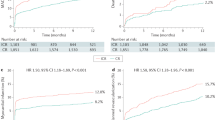
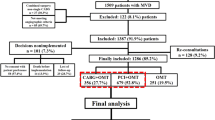
The EXCEL and NOBLE trials demonstrated the safety and efficacy of percutaneous coronary intervention compared with CABG surgery in selected patients with unprotected left main coronary artery disease
Long-term clinical follow-up is required to define the optimal clinical management of patients with unprotected left main coronary artery disease
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout





Similar content being viewed by others

Change history
21 February 2020
This article has been modified to correct the resolution of the arrows depicting shear stress in Figure 2. The figure has been updated in the HTML and PDF versions of the manuscript.
References
Braunwald, E. Treatment of left main coronary artery disease. N. Engl. J. Med. 375, 2284–2285 (2016).
Conley, M. J. et al. The prognostic spectrum of left main stenosis. Circulation 57, 947–952 (1978).
El-Menyar, A. A., Al Suwaidi, J. & Holmes, D. R. Jr. Left main coronary artery stenosis: state-of-the-art. Curr. Problems Cardiol 32, 103–193 (2007).
Hamilos, M. et al. Long-term clinical outcome after fractional flow reserve-guided treatment in patients with angiographically equivocal left main coronary artery stenosis. Circulation 120, 1505–1512 (2009).
Herrick, J. B. Landmark article (JAMA 1912). Clinical features of sudden obstruction of the coronary arteries. By James B. Herrick. JAMA 250, 1757–1765 (1983).
Favaloro, R. G. Saphenous vein autograft replacement of severe segmental coronary artery occlusion: operative technique. Ann. Thorac. Surg. 5, 334–339 (1968).
The Veterans Administration Coronary Artery Bypass Surgery Cooperative Study Group. Eleven-year survival in the Veterans Administration randomized trial of coronary bypass surgery for stable angina. N. Engl. J. Med. 311, 1333–1339 (1984).
CASS Principal Investigators and their Associates. Coronary artery surgery study (CASS): a randomized trial of coronary artery bypass surgery. Survival data. Circulation 68, (939–950 (1983).
European Coronary Surgery Study Group. Long-term results of prospective randomised study of coronary artery bypass surgery in stable angina pectoris. Lancet 2, 1173–1180 (1982).
Yusuf, S. et al. Effect of coronary artery bypass graft surgery on survival: overview of 10-year results from randomised trials by the Coronary Artery Bypass Graft Surgery Trialists Collaboration. Lancet 344, 563–570 (1994).
Gruentzig, A. Trnasluminal dilatation of coronary-artery stenosis. Lancet 311, 263 (1978).
Morice, M. C. et al. Outcomes in patients with de novo left main disease treated with either percutaneous coronary intervention using paclitaxel-eluting stents or coronary artery bypass graft treatment in the Synergy Between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery (SYNTAX) trial. Circulation 121, 2645–2653 (2010).
Stone, G. W. et al. Everolimus-eluting stents or bypass surgery for left main coronary artery disease. N. Engl. J. Med. 375, 2223–2235 (2016).
Makikallio, T. et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in treatment of unprotected left main stenosis (NOBLE): a prospective, randomised, open-label, non-inferiority trial. Lancet 388, 2743–2752 (2016).
Dodge, J. T. Jr., Brown, B. G., Bolson, E. L. & Dodge, H. T. Lumen diameter of normal human coronary arteries. Influence of age, sex, anatomic variation, and left ventricular hypertrophy or dilation. Circulation 86, 232–246 (1992).
Bergelson, B. A. & Tommaso, C. L. Left main coronary artery disease: assessment, diagnosis, and therapy. Am. Heart J. 129, 350–359 (1995).
Ofili, E. O. et al. Analysis of coronary blood flow velocity dynamics in angiographically normal and stenosed arteries before and after endolumen enlargement by angioplasty. J. Am. Coll. Cardiol. 21, 308–316 (1993).
Yasu, T., Yamagishi, M., Beppu, S., Nagata, S. & Miyatake, K. Left main coronary flow velocity associated with stenosis. Evaluation by transesophageal color-guided pulsed Doppler technique. Chest 104, 690–693 (1993).
Papafaklis, M. I. et al. Association of endothelial shear stress with plaque thickness in a real three-dimensional left main coronary artery bifurcation model. Int. J. Cardiol. 115, 276–278 (2007).
Chatzizisis, Y. S. et al. Role of endothelial shear stress in the natural history of coronary atherosclerosis and vascular remodeling: molecular, cellular, and vascular behavior. J. Am. Coll. Cardiol. 49, 2379–2393 (2007).
Slager, C. J. et al. The role of shear stress in the generation of rupture-prone vulnerable plaques. Nat. Clin. Pract. Cardiovasc. Med. 2, 401–407 (2005).
Oviedo, C. et al. Intravascular ultrasound classification of plaque distribution in left main coronary artery bifurcations: where is the plaque really located? Circ. Cardiovasc. Interv. 3, 105–112 (2010).
Maehara, A. et al. Intravascular ultrasound assessment of the stenoses location and morphology in the left main coronary artery in relation to anatomic left main length. Am. J. Cardiol. 88, 1–4 (2001).
Cohen, M. V., Cohn, P. F., Herman, M. V. & Gorlin, R. Diagnosis and prognosis of main left coronary artery obstruction. Circulation 45, I57–65 (1972).
McNeer, J. F. et al. The role of the exercise test in the evaluation of patients for ischemic heart disease. Circulation 57, 64–70 (1978).
Maddahi, J., Abdulla, A., Garcia, E. V., Swan, H. J. & Berman, D. S. Noninvasive identification of left main and triple vessel coronary artery disease: improved accuracy using quantitative analysis of regional myocardial stress distribution and washout of thallium-201. J. Am. Coll. Cardiol. 7, 53–60 (1986).
Chieffo, A. et al. Drug-eluting stent for left main coronary artery disease. The DELTA registry: a multicenter registry evaluating percutaneous coronary intervention versus coronary artery bypass grafting for left main treatment. JACC Cardiovasc. Interv. 5, 718–727 (2012).
Patel, N. et al. Outcomes after emergency percutaneous coronary intervention in patients with unprotected left main stem occlusion: the BCIS national audit of percutaneous coronary intervention 6-year experience. JACC Cardiovasc. Interv 7, 969–980 (2014).
Cameron, A. et al. Left main coronary artery stenosis: angiographic determination. Circulation 68, 484–489 (1983).
Arnett, E. N. et al. Coronary artery narrowing in coronary heart disease: comparison of cineangiographic and necropsy findings. Ann. Intern. Med. 91, 350–356 (1979).
Hermiller, J. B. et al. Unrecognized left main coronary artery disease in patients undergoing interventional procedures. Am. J. Cardiol. 71, 173–176 (1993).
Sano, K. et al. Assessing intermediate left main coronary lesions using intravascular ultrasound. Am. Heart J. 154, 983–988 (2007).
Abizaid, A. S. et al. One-year follow-up after intravascular ultrasound assessment of moderate left main coronary artery disease in patients with ambiguous angiograms. J. Am. Coll. Cardiol. 34, 707–715 (1999).
Porto, I. et al. Comparison of two- and three-dimensional quantitative coronary angiography to intravascular ultrasound in the assessment of intermediate left main stenosis. Am. J. Cardiol. 109, 1600–1607 (2012).
Girasis, C. et al. Impact of 3-dimensional bifurcation angle on 5-year outcome of patients after percutaneous coronary intervention for left main coronary artery disease: a substudy of the SYNTAX trial (synergy between percutaneous coronary intervention with taxus and cardiac surgery). JACC Cardiovasc. Interv. 6, 1250–1260 (2013).
Windecker, S. et al. 2014 ESC/EACTS guidelines on myocardial revascularization. EuroIntervention 10, 1024–1094 (2015).
de la Torre Hernandez, J. M. et al. Clinical impact of intravascular ultrasound guidance in drug-eluting stent implantation for unprotected left main coronary disease: pooled analysis at the patient-level of 4 registries. JACC Cardiovasc. Interv. 7, 244–254 (2014).
Kassimis, G. et al. Assessing the left main stem in the cardiac catheterization laboratory. What is “significant”? Function, imaging or both? Cardiovasc. Revasculariz. Med. 19, 51–56 (2017).
Okabe, T. et al. Five-year outcomes of moderate or ambiguous left main coronary artery disease and the intravascular ultrasound predictors of events. J. Invasive Cardiol. 20, 635–639 (2008).
Jasti, V., Ivan, E., Yalamanchili, V., Wongpraparut, N. & Leesar, M. A. Correlations between fractional flow reserve and intravascular ultrasound in patients with an ambiguous left main coronary artery stenosis. Circulation 110, 2831–2836 (2004).
Park, S. J. et al. Intravascular ultrasound-derived minimal lumen area criteria for functionally significant left main coronary artery stenosis. JACC Cardiovasc. Interv. 7, 868–874 (2014).
de la Torre Hernandez, J. M. et al. Prospective application of pre-defined intravascular ultrasound criteria for assessment of intermediate left main coronary artery lesions results from the multicenter LITRO study. J. Am. Coll. Cardiol. 58, 351–358 (2011).
De Bruyne, B. et al. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. N. Engl. J. Med. 367, 991–1001 (2012).
Pijls, N. H., van Son, J. A., Kirkeeide, R. L., De Bruyne, B. & Gould, K. L. Experimental basis of determining maximum coronary, myocardial, and collateral blood flow by pressure measurements for assessing functional stenosis severity before and after percutaneous transluminal coronary angioplasty. Circulation 87, 1354–1367 (1993).
Davies, J. E. et al. Use of the instantaneous wave-free ratio or fractional flow reserve in PCI. N. Engl. J. Med. 376, 1824–1834 (2017).
Gotberg, M. et al. Instantaneous wave-free ratio versus fractional flow reserve to guide PCI. N. Engl. J. Med. 376, 1813–1823 (2017).
Toth, G. et al. Evolving concepts of angiogram: fractional flow reserve discordances in 4000 coronary stenoses. Eur. Heart J. 35, 2831–2838 (2014).
Mallidi, J. et al. Long-term outcomes following fractional flow reserve-guided treatment of angiographically ambiguous left main coronary artery disease: a meta-analysis of prospective cohort studies. Catheter Cardiovasc. Interv. 86, 12–18 (2015).
Fearon, W. F. et al. The impact of downstream coronary stenosis on fractional flow reserve assessment of intermediate left main coronary artery disease: human validation. JACC Cardiovasc. Interv. 8, 398–403 (2015).
Yong, A. S. et al. Fractional flow reserve assessment of left main stenosis in the presence of downstream coronary stenoses. Circ. Cardiovasc. Interv. 6, 161–165 (2013).
Gould, K. L. Noninvasive assessment of coronary stenoses by myocardial perfusion imaging during pharmacologic coronary vasodilatation. I. Physiologic basis and experimental validation. Am. J. Cardiol. 41, 267–278 (1978).
Modi, B. N., van de Hoef, T. P., Piek, J. J. & Perera, D. Physiological assessment of left main coronary artery disease. EuroIntervention 13, 820–827 (2017).
Moss, A. J., Williams, M. C., Newby, D. E. & Nicol, E. D. The updated NICE guidelines: cardiac CT as the first-line test for coronary artery disease. Curr. Cardiovascular Imag. Rep. 10, 15 (2017).
Meijboom, W. B. et al. Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J. Am. Coll. Cardiol. 52, 2135–2144 (2008).
Edris, A., Patel, P. M. & Kern, M. J. Early recognition of catheter-induced left main coronary artery vasospasm: implications for revascularization. Catheter Cardiovasc. Interv. 76, 304–307 (2010).
Ishisone, T., Satoh, M., Okabayashi, H. & Nakamura, M. Usefulness of multidetector CT angiography for anomalous origin of coronary artery. BMJ Case Rep. https://doi.org/10.1136/bcr-2014-205180 (2014).
Xie, J. X. et al. Prognostic significance of nonobstructive left main coronary artery disease in women versus men: long-term outcomes from the CONFIRM (Coronary CT Angiography Evaluation For Clinical Outcomes: An International Multicenter) registry. Circul. Cardiovasc. Imag. 10, e006246 (2017).
Van Mieghem, C. A. et al. Multislice spiral computed tomography for the evaluation of stent patency after left main coronary artery stenting: a comparison with conventional coronary angiography and intravascular ultrasound. Circulation 114, 645–653 (2006).
Roura, G. et al. Multislice CT for assessing in-stent dimensions after left main coronary artery stenting: a comparison with three dimensional intravascular ultrasound. Heart 99, 1106–1112 (2013).
George, R. T. et al. Myocardial CT perfusion imaging and SPECT for the diagnosis of coronary artery disease: a head-to-head comparison from the CORE320 multicenter diagnostic performance study. Radiology 272, 407–416 (2014).
Guentzig, A. R., S, A. & Siegeuthaler, W. E. Non-operative dilatation of coronary artery stenosis. Percutaneous transluminal coronary angioplasty. N. Engl. J. Med. 301, 61–68 (1979).
Head, S. J., Milojevic, M., Taggart, D. P. & Puskas, J. D. Current practice of state-of-the-art surgical coronary revascularization. Circulation 136, 1331–1345 (2017).
Rab, T. et al. Current interventions for the left main bifurcation. JACC Cardiovasc. Interv. 10, 849–865 (2017).
Ye, Y., Yang, M., Zhang, S. & Zeng, Y. Percutaneous coronary intervention in left main coronary artery disease with or without intravascular ultrasound: a meta-analysis. PLoS ONE 12, e0179756 (2017).
Kang, S. J. et al. Comprehensive intravascular ultrasound assessment of stent area and its impact on restenosis and adverse cardiac events in 403 patients with unprotected left main disease. Circ. Cardiovasc. Interv. 4, 562–569 (2011).
Park, S. J. et al. Impact of intravascular ultrasound guidance on long-term mortality in stenting for unprotected left main coronary artery stenosis. Circ. Cardiovasc. Interv. 2, 167–177 (2009).
Maehara, A. et al. Impact of final minimal stent area by IVUS on 3-year outcome after PCI of left main coronary artery disease: the EXCEL trial. J. Am. Coll. Cardiol. 69, 963 (2017).
Capodanno, D. Risk stratification for percutaneous coronary intervention. Interv. Cardiol. Clin. 5, 249–257 (2016).
Sianos, G. et al. The SYNTAX Score: an angiographic tool grading the complexity of coronary artery disease. EuroIntervention 1, 219–227 (2005).
Farooq, V. et al. Anatomical and clinical characteristics to guide decision making between coronary artery bypass surgery and percutaneous coronary intervention for individual patients: development and validation of SYNTAX score II. Lancet 381, 639–650 (2013).
Serruys, P. W. et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N. Engl. J. Med. 360, 961–972 (2009).
Mohr, F. W. et al. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year follow-up of the randomised, clinical SYNTAX trial. Lancet 381, 629–638 (2013).
Park, S. J. et al. Randomized trial of stents versus bypass surgery for left main coronary artery disease. N. Engl. J. Med. 364, 1718–1727 (2011).
Morice, M. C. et al. Five-year outcomes in patients with left main disease treated with either percutaneous coronary intervention or coronary artery bypass grafting in the synergy between percutaneous coronary intervention with taxus and cardiac surgery trial. Circulation 129, 2388–2394 (2014).
Ahn, J. M. et al. Randomized trial of stents versus bypass surgery for left main coronary artery disease: 5-year outcomes of the PRECOMBAT study. J. Am. Coll. Cardiol. 65, 2198–2206 (2015).
Cavalcante, R. et al. Outcomes after percutaneous coronary intervention or bypass surgery in patients with unprotected left main disease. J. Am. Coll. Cardiol. 68, 999–1009 (2016).
Palmerini, T. et al. Clinical outcomes with percutaneous coronary revascularization versus coronary artery bypass grafting surgery in patients with unprotected left main coronary artery disease: a meta-analysis of 6 randomized trials and 4,686 patients. Am. Heart J. 190, 54–63 (2017).
Levine, G. N. et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention. a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J. Am. Coll. Cardiol. 58, e44–e122 (2011).
Zhang, J. J. & Chen, S. L. Classic crush and DK crush stenting techniques. EuroIntervention 11 (Suppl. V), V102–V105 (2015).
Buszman, P. E. et al. Early and long-term results of unprotected left main coronary artery stenting: the LE MANS (Left Main Coronary Artery Stenting) registry. J. Am. Coll. Cardiol. 54, 1500–1511 (2009).
Boudriot, E. et al. Randomized comparison of percutaneous coronary intervention with sirolimus-eluting stents versus coronary artery bypass grafting in unprotected left main stem stenosis. J. Am. Coll. Cardiol. 57, 538–545 (2011).
Reviewer information
Nature Reviews Cardiology thanks Y.-H. Kim, R. Waksman, W. Wijns, and the other anonymous reviewer(s) for their contribution to the peer review of this work.
Author information
Authors and Affiliations
Contributions
C.C. researched the data for the article. C.C. and P.W.S. discussed the content of the manuscript. C.C., D.C., G.W.S., and P.W.S. wrote the article. C.C., Y.O., A.B., G.W.S., D.P.T., and J.S. reviewed and/or edited the manuscript before submission.
Corresponding author
Ethics declarations
Competing interests
C.C. received research grants from Biosensors and HeartFlow. D.C. received speaker and consulting honoraria from Abbott Vascular, AstraZeneca, Bayer, Daiichi Sankyo, and Stentys. Y.O. is a member of the advisory board of Abbott Vascular. A.B. received lecture fees from Abbott Vascular, Boston Scientific, and Medtronic and grant support from Boston Scientific. G.W.S. received consulting fees from Ablative Solutions, Matrizyme, Medical Development Technologies, Miracor, Neovasc, TherOx, Reva, Toray, Vascular Dynamics, Velomedix, and V-Wave; served as a consultant on prasugrel patent litigation paid for by Lupin Pharmaceuticals; and holds equity, stock options, or both in the Aria, Biostar family of funds, Cagent, Caliber Therapeutics, Guided Delivery Systems, MedFocus family of funds, MiCardia, Qool Therapeutics, and Vascular Nanotransfer Technologies. Columbia University (G.W.S.) received royalties from Abbott Vascular for the sale of MitraClip. D.P.T. served as advisor and speaker for Abbott Laboratories, Medtronic, and Novadaq Technologies; and owns stock, stock option, or bonds from Novadaq Technologies. J.S. received fees for serving on advisory boards from Medtronic and the Sorin Group, training fees from Medtronic, and research funding from Abbott and Edwards Lifesciences. P.W.S. received consulting fees from Abbott, AstraZeneca, Biotronik, Cardialysis, GLG Research, Medtronic, SINO Medical Sciences Technology, St. Jude Medical, Stentys France, Svelte Medical Systems, and Volcano.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Glossary
- Right dominant coronary circulation
-
A circulation pattern in which the posterior descending artery, which supplies the myocardium of the inferior one-third of the interventricular septum, is a branch of the right coronary artery.
- Fractional flow reserve
-
The ratio of distal coronary pressure to aortic pressure during hyperaemia; linearly and strongly correlates to the ratio of stenotic-to-normal mean arterial Doppler-derived blood flow velocity.
- Heart Team
-
Multidisciplinary approach for revascularization; made up of an interventional cardiologist, a cardiac surgeon, and often the patient’s general cardiologist.
- Carina
-
Arterial region between the division of the main and side branch, where blood flow diverts and deflects.
- Shear stress
-
The tangential force derived from the friction of the flowing blood on the endothelial surface.
- Duke treadmill score
-
Weighted index combining treadmill exercise time using the standard Bruce protocol, maximum net ST-segment deviation (depression or elevation), and exercise-induced angina.
- Intravascular ultrasonography
-
Imaging methodology using a specially designed catheter with a miniaturized ultrasound probe attached to the distal end of the catheter to assess the coronary artery.
- Instantaneous wave-free ratio
-
Nonhyperaemic ratio of distal coronary pressure to aortic pressure during the diastolic wave-free period.
Rights and permissions
About this article

Cite this article
Collet, C., Capodanno, D., Onuma, Y. et al. Left main coronary artery disease: pathophysiology, diagnosis, and treatment. Nat Rev Cardiol 15, 321–331 (2018). https://doi.org/10.1038/s41569-018-0001-4
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41569-018-0001-4
This article is cited by
-
Left main coronary artery morphological phenotypes and its hemodynamic properties
BioMedical Engineering OnLine (2024)
-
Five-year outcomes in patients with multivessel coronary artery disease undergoing surgery or percutaneous intervention
Scientific Reports (2024)
-
Endothelin-1 is associated with mortality that can be attenuated with high intensity statin therapy in patients with stable coronary artery disease
Communications Medicine (2023)
-
Importance of optimal rewiring guided by 3-dimensional optical frequency domain imaging during double-kissing culotte stenting demonstrated through a novel bench model
Scientific Reports (2023)
-
Percutaneous coronary artery intervention in unprotected left main coronary artery disease: one-year outcome Egyptian registry
The Egyptian Heart Journal (2022)
