
Abstract
The public health problems caused by schizophrenia are becoming increasingly prominent and can place a huge economic burden on society. This study takes Gansu Province as an example to analyze the level and changing trend of the economic burden of schizophrenia inpatients in economically underdeveloped areas of China. Using a multi-stage stratified cluster sampling method, 39,054 schizophrenics from 197 medical and health institutions in Gansu Province were selected as the research objects, and their medical expenses and related medical records were obtained from the medical information system. The rank sum test and Spearman rank correlation were used for univariate analysis. Quantile regression and random forest were used to analyze the influencing factors. The results show that the average length of stay of schizophrenics in Gansu Province of China was 52.01 days, and the average hospitalization cost was USD1653.96 from 2014 to 2019. During the six years, the average hospitalization costs per time decreased from USD2136.85 to USD1401.33. The average out-of-pocket costs per time decreased from USD1238.78 to USD267.68. And the average daily hospitalization costs increased from USD38.18 to USD41.25. The main factors influencing hospitalization costs are length of stay, proportion of medications, and schizophrenic subtype. The hospitalization costs per time of schizophrenics in Gansu Province have decreased but remain at a high level compared to some other chronic non-communicable diseases. In the future, attention should be paid to improving the efficiency of medical institutions, enhancing community management, and promoting the transformation of the management model of schizophrenia.
Similar content being viewed by others

Introduction
Schizophrenia is a complex psychiatric disorder, often accompanied by obstacles in perception, thinking, emotion, and behavior1. And it remains one of the most expensive mental illnesses in human society2. The disease occurs in late adolescence and early adulthood, and has a poor prognosis3. The mortality rate is 3.12 times higher in the patient population than in the general population4. It is reported that the number of schizophrenics worldwide increased from 13.1 million in 1990 to 20.9 million in 20163. The global age-standardized prevalence of schizophrenia is 287.4 per 100,000 in 20195. And the lifetime prevalence in China is 0.6%6. The public health problems caused by schizophrenia have become increasingly prominent because of the concentration of the disease in young adults, the high unemployment rate of patients7, the susceptibility to co-morbidity with other somatic diseases8, and the high incidence of aggression and violence9. And they also bring huge economic burden to schizophrenic families and the society.
The economic burden of illness is measured and analyzed in terms of the economic costs or losses incurred by the population due to the disease, including the costs of treatment and care for the patients, as well as the loss of productivity due to injury, disability, caregiver assistance or the patient’s violent behavior10. It mainly includes direct economic burden, indirect economic burden, and intangible economic burden. The direct economic burden reflects the medical resources used in the course of disease treatment11, and the hospitalization expense is the largest contributor to the total direct medical costs of schizophrenia12. The existing research shows that the social costs due to schizophrenia vary widely globally13. The global lifetime social cost of schizophrenia per capita ranges from USD5818 in Thailand to USD94,587 in Norway14. The level of economic development and medical care varies greatly among different regions in China, therefore the level of the economic burden of this disease may also vary greatly. However, only small sample data or medical insurance data have been reported in China to analyze the economic burden of the illness15,16,17, and they are mostly concentrated in more economically developed regions. Few relevant studies using large sample treatment data in less economically developed regions have been seen.
Gansu Province is located in an economically underdeveloped region in northwestern China, with a resident population of 26.47 million at the end of 2019. The GDP of the province this year was 871.83 billion Chinese yuan, with 12 prefecture level cities and 2 autonomous prefectures under its jurisdiction18. At present, there is a shortage of full-time prevention and control personnel of mental health in the province. In 2018, the standardized management rate of registered patients with severe mental disorders was 71.78%, of which the regular medication-taking rate of schizophrenia was only 27.49%19. Therefore, this study using Gansu Province as an example has more research significance in analyzing the level of economic burden of schizophrenia in economically underdeveloped regions of China. This study used the treatment data of schizophrenia inpatients to analyze the composition and changing trend of hospitalization costs in Gansu Province of China from 2014 to 2019. At the same time, it explored the factors influencing the average hospitalization cost per time and the average daily hospitalization cost of schizophrenics and their significance. Thus, it provides a theoretical basis for policy-makers to formulate relevant health policies and reduce the economic burden of schizophrenia.
Results
Patient characteristics and univariate analysis
A total of 39,054 inpatients with schizophrenia were enrolled in this study from 2014 to 2019, including 21,272 males (54.47%) and 17,782 females (45.53%). The average age was 37.28 ± 12.32 years old. The average length of stay was 52.01 ± 41.87 days. And the percentage of patients using the medical insurance reimbursement payment method was 59.17%. In terms of institutional level (graded by administrative subordination), 98.25% of patients were treated in provincial or municipal medical and health institutions. In terms of the type of institution, 94.32% of the patients were seen in specialized hospitals. Among schizophrenia inpatients with defined subtypes, paranoid schizophrenia had the highest percentage of 34.06%.
The results of the univariate analysis showed statistically significant differences in the average costs of hospitalization per time between patients with different gender, ages, payment methods, hospital nature, hospital levels, hospital types, number of comorbidities, length of stay, proportion of medications, and schizophrenic subtypes (P < 0.05). See Table 1.
Component of hospitalization costs for schizophrenics
From 2014 to 2019, the average hospitalization expenses of schizophrenics per visit in Gansu Province were CNY11,409.83 (USD1653.96). Among them, the treatment expenses were CNY4,568.64 (USD662.27, 42.25%), which accounted for the highest percentage. This was followed by bed and nursing fees of CNY1938.65 (USD281.02, 17.93%), medication costs of CNY1521.65 (USD220.58, 14.07%), and examination costs of CNY1301.55 (USD188.67, 12.04%). The proportion of consultation costs accounted for the lowest, at CNY286.00 (USD41.46, 2.64%). See Fig. 1.

Composition of hospitalization costs of schizophrenia patients in Gansu Province, China, from 2014 to 2018.
The trend of hospitalization costs for schizophrenics
From 2014 to 2019, the average hospitalization costs of schizophrenics per time in Gansu Province showed an overall downward trend, from CNY14,741.08 (USD2136.85) to CNY9667.07(USD1401.33; rs = −0.161, P < 0.001). The average growth rate over the 6 years was −8.09%. Average inpatient out-of-pocket costs have also been decreasing from CNY8545.74 (USD1238.78) in 2014 to CNY1846.56 (USD267.68) in 2019 (rs = −0.294, P < 0.001). The average growth rate was −26.39%. However, during the same period, the average daily hospitalization costs for patients showed an overall increasing trend from CNY263.41 (USD38.18) to CNY284.56 (USD41.25), with an average growth rate of 1.56%. See Table 2.
Quantile regression analysis of hospitalization costs
Natural log-transformed hospitalization costs per time and average daily hospitalization costs of schizophrenia patients were used as dependent variables. Variables that were statistically significant for univariate analysis, such as gender, age, payment method, hospital nature, hospital level, hospital type, number of comorbidities, length of stay, proportion of medications, schizophrenic subtype, and year of hospitalization, were used as independent variables. Incorporating each of the above variables into the quantile regression model simultaneously. The Pseudo R2 of the model in the 10th, 50th, and 90th percentile points of hospitalization costs were 0.479, 0.529, and 0.542 respectively, with the best fit at the 90th percentile. The Pseudo R2 at the three percentile points of average daily hospitalization costs were 0.637, 0.287, and 0.156 respectively, with the best fit at the 10th percentile. The results showed that the effects of age, payment method, hospital nature, hospital level, length of stay, and proportion of medications were significant at all three percentile levels of hospitalization costs and average daily hospitalization costs (all P < 0.05).
Age, hospital level, and proportion of medications had a significant negative effect (P < 0.05) on all three quantile points of hospitalization costs per time, and the intensity of the effect was higher at the lower quantile point than at the higher point. Length of stay was positively associated with hospitalization costs, with the strength of its effect being slightly higher at the higher quartile point than at the lower. Among payment methods, full out-of-pocket patients had lower hospitalization costs at the 10th percentile and higher at the remaining two quartiles than medical insurance reimbursement patients (all P < 0.05). For the number of comorbidities, patients with one, two, and three or more comorbidities had higher hospitalization costs at the 50th and 90th percentiles than patients without comorbidities (all P < 0.05).
Hospital nature, length of stay, and proportion of medications had a significant negative effect at all three quartiles of average daily hospitalization costs (all P < 0.05). In contrast, payment method and hospital level had a significant positive impact on the three quantiles (all P < 0.05). For the number of comorbidities, patients with one, two, and three or more comorbidities had higher average daily hospitalization costs at the 50th and 90th percentiles than patients without comorbidities (all P < 0.05). See Table 3.
Analysis of the importance of factors influencing hospitalization costs
Natural log-transformed hospitalization costs per time and average daily hospitalization costs of schizophrenia patients were used as dependent variables. Factors from the quantile regression analysis that had a significant effect on hospitalization costs were used as independent variables. Incorporating them jointly into the random forest regression tree model. The training set and testing set sample cases are randomly assigned in the ratio of 3:1. Set the number of random seed to 666, the number of trees to grow (ntree) to 500, and the number of variables randomly sampled as candidates at each split (mtry) to 3. At this point, the standardized mean squared error (RMSE) of the random forest regression tree model for hospitalization costs per time was 0.266 with R2 = 0.898, and the RMSE for average daily hospitalization costs was 0.257 with R2 = 0.857. The model generalization ability is strong and the fit is excellent.
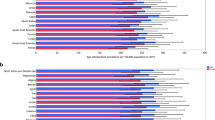
Finally, the importance of the influencing factors was analyzed according to the mean decrease accuracy (%IncMSE). That is, the larger the %IncMSE, the higher the importance. The results showed that the top five influencing factors for hospitalization costs per time were length of stay, proportion of medications, schizophrenic subtype, number of comorbidities, and year of hospitalization, respectively. The top five factors influencing average daily hospitalization costs were proportion of medications, length of stay, schizophrenic subtype, hospital type, and age. See Fig. 2.

a Ranking the importance of factors on the hospitalization costs per time of patients with schizophrenia. b Ranking the importance of factors on the average daily hospitalization costs of patients with schizophrenia.
Discussion
This study analyzed the hospitalization costs of schizophrenia patients in economically underdeveloped areas of China, using a large sample of consecutive 6 years of treatment data in Gansu Province. The results showed that the average age of schizophrenia inpatients in Gansu Province from 2014 to 2019 was 37.28 ± 12.32 years, and the average length of stay was 52.01 ± 41.87 days. Previous studies have shown that the average length of stay for patients with schizophrenia in Central and Eastern Europe (CEE) and the United States was 25.3 and 9.08 days, respectively10,20. The median length of stay for schizophrenia inpatients in Portugal was 18.0 days, and the mean age of the patients was 41.68 ± 12.93 years21. In comparison, Chinese patients with schizophrenia were hospitalized at a younger age and for a longer length of stay. This may be because countries such as the United States have implemented integrated community-based rehabilitation interventions, which have shifted from an inpatient model to a community-based model for schizophrenia services, thereby the length of stay has been significantly reduced22. Medical resources are scarce in underdeveloped areas in northwest China. And there are few full-time mental health prevention and control personnel in grassroots institutions. It is difficult for patients to obtain high-quality community nursing services after discharge. The above together lead to the longer length of stay for schizophrenia in China. The average hospitalization costs per visit of schizophrenia patients in Gansu Province from 2014 to 2019 was CNY 11,409.83 (USD 1653.96). A higher percentage of these are for treatment costs, bed and nursing fees, and medication costs, with the three accounting for more than 80% of the total costs. The average hospitalization costs per time for schizophrenia is lower than that of gastric cancer (CNY12,514.98 in 2017)23, but much higher than some other chronic non-communicable diseases such as diabetes (CNY 5131.34 in 2018) and coronary heart disease (CNY 6791.38 in 2015)24,25. Unlike the medication-based cost model for non-psychiatric disorders, treatment costs, which measure the value of the medical workforce, account for the highest proportion of schizophrenia hospitalization costs. This is consistent with the findings of other similar schizophrenia studies15.
The results showed that the average hospitalization costs and out-of-pocket costs per time of schizophrenia patients in Gansu Province showed a decreasing trend from 2014 to 2019, with an average growth rate of −8.09% and −26.39% respectively. The decrease in hospitalization costs may be related to the promotion of graded treatment in the region and the improvement of service capacity of primary medical and health institutions. The region has implemented the service model of “treating schizophrenia in the hospital and managing rehabilitation in the community”. For patients in the acute stage and unstable condition, the primary institutions promptly refer them to professional mental institutions for standardized treatment. After stabilization, they return to the community to receive maintenance treatment with basic psychiatric medicines26. Average out-of-pocket costs per time declined obviously faster than hospitalization costs. This may be related to the comprehensive promotion of rescue and treatment assistance for severe mental disorders and the gradual improvement of medical coverage level for the patients in the region. The average daily hospitalization costs showed an overall increasing trend over the 6-year period, with an average rate of increase of 1.56%. This was driven primarily by the decrease in length of stay.
Random forest is an integrated learning algorithm based on decision trees, which has better tolerance for outliers and noise and is less prone to overfitting27,28. This study used random forest regression tree model to obtain the importance ranking of independent variables on the degree of impact of hospitalization costs. The results showed that length of stay, medication proportion, and schizophrenic subtype are the main factors influencing the hospitalization costs. Combined with the quantile regression results, the average hospitalization cost per time was negatively correlated with age and medication proportion, and positively correlated with length of stay and number of comorbidities. A previous Chinese study showed that the optimal length of stay for functional recovery in schizophrenics was between 20 and 50 days29. Therefore, the length of stay for schizophrenia patients should be reasonably reduced and other physical illnesses of the patients should be actively prevented. The efficiency of treatment in medical institutions should also be continuously improving. This will, on the one hand, help to increase bed turnover and bring more economic benefits to medical institutions, and on the other hand, help to reduce the patient’s medical costs. The average cost of a hospital stay at district and county level is lower than at provincial and municipal level. And the cost of specialized hospitals is higher than that of general hospitals. The number of inpatients with schizophrenia attending provincial and municipal level medical institutions is much higher than that of district and county level. This may be due to the fact that higher-grading institutions are better equipped and have a higher level of diagnosis and treatment. Therefore, patients are more likely to visit such facilities, and the costs are correspondingly higher. The hospitalization costs for full out-of-pocket patients are higher than for medical insurance reimbursement patients. This suggests that medical insurance has had a cost-controlling effect on schizophrenia inpatients. It has reduced unnecessary expenditure in medical costs, thus having a positive effect on reducing the economic burden of the disease.
This study also has some limitations. Firstly, the data for the study were obtained from the billing and settlement systems of healthcare institutions. Hence the variables included were somewhat limited and could not include other variables such as disease severity that may affect hospitalization costs. Second, for reasons such as the poor implementation of schizophrenia typing in Chinese clinical practice, some of the available statistics do not contain detailed information on disease subtypes. This may limit the further mining of data information.
In conclusion, the average costs per time and the length of stay of schizophrenia inpatients in Gansu Province, China, decreased from 2014 to 2019, but currently remain at a high level. Therefore, in order to further reduce the level of the patient’s economic burden, the length of stay should be reasonably reduced. At the same time, the treatment efficiency of medical institutions should be improved, and the capacity of primary medical and health institutions for prevention and control of mental illness should be strengthened. Thus, the community management level of schizophrenia can be further improved and the rational distribution of medical resources can be continuously promoted.
Methods
Data source
In this study, a multi-stage stratified cluster sampling method was used. In stage 1, among the provincial institutions, half of the number of general hospitals and Traditional Chinese Medicine hospitals (TCM hospitals) and one of each different type of specialized hospitals were selected as sample institutions using simple random sampling method. In stage 2, based on the economic level, geographical condition, and population size of the 14 cities and prefectures in Gansu Province, five cities, namely Pingliang, Dingxi, Zhangye, Wuwei, and Tianshui, were finally selected as sample cities. The cities follow the same sampling principle as the provincial medical and health institutions for municipal institutions. In stage 3, according to the geographical location and the urban and rural characteristics, one district and two counties were selected in each sample city, totaling 15 counties (districts). And then according to the provincial institutions sampling principle, the county (district) level medical and health institutions shall be selected. In stage 4, among the selected counties (districts), 5–8 township health centers or community health service centers were selected by simple random sampling method. Eventually, a total of 197 medical and health institutions were acquired.
According to the code F20 of the International Classification of Diseases 10th Revision (ICD-10) issued by WHO, the medical records of inpatients with a primary diagnosis of schizophrenia were collected in each sample institution from 2014 to 2019. Among them, the ICD-10 code F20.0 refers to paranoid schizophrenia. F20.1 refers to hebephrenic schizophrenia. F20.2 refers to catatonic schizophrenia. F20.3 refers to unidentified schizophrenia. F20.4 refers to post-schizophrenic depression. F20.5 refers to residual schizophrenia. F20.6 refers to simple schizophrenia. F20.8 refers to other schizophrenia. F20.9 refers to schizophrenia, unspecified. We obtain the patient’s case information, including general demographic information (age, gender, disease diagnosis, date of discharge, length of stay, and information about the medical institution, etc.) and hospitalization cost information (treatment costs, medication costs, examination costs, consultation costs, bed and nursing fees, and other costs). Finally, a database of hospitalization costs of schizophrenia patients was formed.
Data pre-processing
Hospitalization costs are the costs incurred by the patient for the diagnosis and treatment of the disease during hospitalization. Among them, medication costs include TCM costs and western medicine costs. Examination costs include check fees, test fees, and radiate fees. Bed and nursing fees include bed fees and nursing fees. Other costs include all expenses except treatment costs, medication costs, examination costs, consultation costs, and bed and nursing fees. Proportion of medications refers to the proportion of medication costs to the total hospitalization costs.
After data entry, the integrity and authenticity of the data were verified and the logical error correction was performed promptly. Subsequently, the information with incorrect ICD-10 coding should be corrected. Reject the unqualified data, including: (1) Primary diagnosis of non-schizophrenia. (2) Missing and poorly documented major items. (3) Logical relationships between costs that were clearly incorrect and could not be logically corrected. (4) The presence of outlier data. A total of 39,054 hospitalization data for patients with schizophrenia were eventually collected in this study. To ensure comparability between cost data across years, the costs were converted comparably using the GDP deflator for 2019 as the base year. The relevant calculation formula is shown below Eqs. (1) (2). The nominal GDP values and GDP indices for each year are obtained from the official data of the National Bureau of Statistics of the People’s Republic of China. According to data from the People’s Bank of China, the annual exchange rate between the U.S. dollar and the Chinese yuan for 2019 is USD1.0 = CNY6.8985.
Statistical analysis
Excel 2016 was used to standardize the data obtained from the field survey. Stata 14.0 and R 4.1.3 software were used to build the database and perform data cleaning and statistical analysis. And GraphPad Prism 8.3.0 and R 4.1.3 software were used to make graphs. Qualitative data were expressed as number of cases (composition ratio) [n(q%)], and measurement data were expressed as mean ± standard deviation [mean(SE)]. Since hospitalization costs are positively skewed, the median and quartiles [M(P25, P75)] were used to describe their distribution. Univariate analysis of average hospitalization costs per time of each classification of patients using Mann–Whitney U test and Kruskal–Wallis H test. Spearman’s rank correlation was used to analyze the correlation between non-normally distributed hospitalization costs and age, length of stay, proportion of medications, and year. Transforming the hospitalization costs into a natural logarithm so that it follows an approximately normal distribution. The factors influencing the hospitalization costs and their importance were analyzed using quantile regression model and random forest regression tree model. In this study, based on the experience of previous similar studies30, the 10th, 50th, and 90th percentiles of hospitalization costs were selected for fitting in the quantile regression model. This provides a comprehensive picture of the effect of independent variables on low, medium, and high levels of hospitalization costs. Variable assignment is shown in Table 4. The two-sided test level α = 0.05.
Data availability
The data are not publicly available at present. However, it can be obtained from the corresponding author according to reasonable requirements.
References
Lehman, A. F. et al. Practice guideline for the treatment of patients with schizophrenia, second edition. Am. J. Psychiatry 161, 1–56 (2004).
Os, V. J. & Kapur, S. Schizophrenia. Lancet 374, 635–645 (2009).
Charlson, F. J. et al. Global epidemiology and burden of schizophrenia: findings from the Global Burden of Disease Study 2016. Schizophr. Bull. 44, 1195–1203 (2018).
Gatov, E., Rosella, L., Chiu, M. & Kurdyak, P. A. Trends in standardized mortality among individuals with schizophrenia, 1993–2012: a population-based, repeated cross-sectional study. CMAJ 189, E1177–E1187 (2017).
Ferrari, A. J. et al. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 9, 137–150 (2022).
Huang, Y., Wang, Y. & Wang, H. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry 6, E11–E11 (2019).
Marwaha, S. & Johnson, S. Schizophrenia and employment - a review. Soc. Psychiatry Psychiatr. Epidemiol. 39, 337–349 (2004).
Lambert, T. J. R., Velakoulis, D. & Pantelis, C. Medical comorbidity in schizophrenia. Med. J. Aust. 178, S67–S70 (2003).
Hodgins, S. & Klein, S. New clinically relevant findings about violence by people with schizophrenia. Can. J. Psychiatry 62, 86–93 (2017).
Szkultecka-Debek, M. et al. Schizophrenia causes significant burden to patients’ and caregivers’ lives. Psychiatr. Danub. 28, 104–110 (2016).
Jemal, A. et al. Cancer burden in Africa and opportunities for prevention. Cancer 118, 4372–4384 (2012).
Laidi, C. et al. Factors associated with direct health care costs in schizophrenia: results from the FACE-SZ French dataset. Eur. Neuropsychopharmacol. 28, 24–36 (2018).
Kovács, G. et al. Direct healthcare cost of schizophrenia - European overview. Eur. Psychiatry 48, 79–92 (2018).
Jin, H. & Mosweu, I. The societal cost of schizophrenia: a systematic review. Pharmacoeconomics 35, 25–42 (2017).
Zhang, H., Sun, Y., Zhang, D., Zhang, C. & Chen, G. Direct medical costs for patients with schizophrenia: a 4-year cohort study from health insurance claims data in Guangzhou city, Southern China. Int. J. Ment. Health Syst. 12, 72 (2018).
Wu, J. et al. Health care resource use and direct medical costs for patients with schizophrenia in Tianjin, People’s Republic of China. Neuropsychiatr. Dis. Treat. 11, 983–990 (2015).
Zhai, J., Guo, X., Chen, M., Zhao, J. & Su, Z. An investigation of economic costs of schizophrenia in two areas of China. Int. J. Ment. Health Syst. 7, 26 (2013).
Gansu Province Bureau of Statistics. Gansu Development Yearbook. http://tjj.gansu.gov.cn/tjj/tjnj/2020/zk/indexch.htm (2020).
Xu, F. F., Jiang, X., Pan, W. M., Xue, L. & Li, K. Distribution features and status of severe mental disorder in Gansu province. Bull. Dis. Control Prev. 34, 15-17+55 (2019).
Chen, E. et al. Schizophrenia hospitalization in the US 2005–2014: examination of trends in demographics, length of stay, and cost. Medicine (Baltimore) 100, e25206 (2021).
Goncalves-Pinho, M., Ribeiro, J. P. & Freitas, A. Schizophrenia related hospitalizations - a big data analysis of a national hospitalization database. Psychiatr. Q. 92, 239–248 (2021).
Chilvers, R., Macdonald, G. M., Hayes, A. A. Supported housing for people with severe mental disorders. Cochrane Database Syst. Rev. CD000453. https://doi.org/10.1002/14651858.CD000453.pub2 (2006).
Yao, A. et al. Characteristics and implications of insurance-reimbursed inpatient care for gastric and oesophageal cancers in Anhui, China. Int. Health 13, 446–455 (2021).
Quan, P. Q., Hu, X. B., Wang, C., Che, X. Y. & Li, Q. E. The trend of hospitalization expenditure and its influencing factors of patients with type 2 diabetes mellitus in Gansu Province from 2014 to 2018. Chin. J. Prev. Contr. Chron. Dis. 30, 8–13 (2022).
Ding, J. M., Zhang, X. Z., Hu, X. J., Chen, H. L. & Yu, M. Analysis of hospitalization expenditures and influencing factors for inpatients with coronary heart disease in a tier-3 hospital in Xi’an, China: a retrospective study. Medicine (Baltimore) 96, e9341 (2017).
Health Commission of Gansu Province. Gansu Province implements the National Mental Health Work Plan (2015–2020). http://wsjk.gansu.gov.cn/wsjk/c113467/201707/1264473.shtml (2017).
Mazumdar, M. et al. Comparison of statistical and machine learning models for healthcare cost data: a simulation study motivated by Oncology Care Model (OCM) data. BMC Health Serv. Res. 20, 350 (2020).
Breiman, L. Random forests. Mach. Learn. 45, 5–32 (2001).
Bian, Y. et al. The optimal length of hospitalization for functional recovery of schizophrenia patients, a real-world study in Chinese people. Psychiatr. Q. 90, 661–670 (2019).
Olsen, M. A. et al. Use of quantile regression to determine the impact on total health care costs of surgical site infections following common ambulatory procedures. Ann. Surg 265, 331–339 (2017).
Acknowledgements
This work was supported by Special Research on Lanzhou University Serving Gansu Economic and Social Development (contract number 2019-FWZX-11) and Research on Total Health Expenditure in Gansu Province (contract number 2022620005002671).
Author information
Authors and Affiliations
Contributions
J.L. contributed to the data cleaning and the statistical analysis, and wrote the original draft of the manuscript. H.D. and F.D. contributed to the data cleaning and verified all the raw data. C.Y. contributed to the data cleaning and the interpretation of the results. Y.Z. and Z.M. contributed to the data cleaning. X.H. designed the study protocol and contributed to the final manuscript approval. All authors contributed to the fieldwork and the data collection.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
No personal patient information was accessed during data acquisition. There was no interaction with the patient, and the patient ID was unavailable. Therefore, ethical approval and informed consent are not required.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, J., Du, H., Dou, F. et al. A study on the changing trend and influencing factors of hospitalization costs of schizophrenia in economically underdeveloped areas of China. Schizophr 9, 4 (2023). https://doi.org/10.1038/s41537-023-00331-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41537-023-00331-6
