
Abstract
Several phenotypic differences observed in Parkinson’s disease (PD) patients have been linked to age at onset (AAO). We endeavoured to find out whether these differences are due to the ageing process itself by using a combined dataset of idiopathic PD (n = 430) and healthy controls (HC; n = 556) excluding carriers of known PD-linked genetic mutations in both groups. We found several significant effects of AAO on motor and non-motor symptoms in PD, but when comparing the effects of age on these symptoms with HC (using age at assessment, AAA), only positive associations of AAA with burden of motor symptoms and cognitive impairment were significantly different between PD vs HC. Furthermore, we explored a potential effect of polygenic risk score (PRS) on clinical phenotype and identified a significant inverse correlation of AAO and PRS in PD. No significant association between PRS and severity of clinical symptoms was found. We conclude that the observed non-motor phenotypic differences in PD based on AAO are largely driven by the ageing process itself and not by a specific profile of neurodegeneration linked to AAO in the idiopathic PD patients.
Similar content being viewed by others

Introduction
Although considered as one disease entity, Parkinson’s disease (PD) displays substantial clinical heterogeneity with various phenotypes that translate into different combinations of both motor and non-motor symptoms. To address this heterogeneity, the age at onset (AAO) has been suggested as a key indicator associated with the clinical profile and progression of PD1,2,3. Previous studies with cross-sectional design have identified later AAO to be related with a stronger motor as well as non-motor impairment suggesting that late AAO is associated with higher progression rate of motor symptoms and cognitive decline. Conversely, early onset PD has been reported to show a specific disease profile with higher rate of motor complications such as early dyskinesia and dystonia4,5,6. Furthermore, both prospective7 and retrospective studies with autopsy-proven PD8 have shown similar findings, but given the heterogeneity of the study designs and various cut-offs used for categorising AAO, the reproducibility of the findings is limited. Despite reporting multiple AAO-related phenotypic differences, no study so far has endeavoured to integrate the effect of the physiological ageing process. Therefore, the associations between AAO and severity of PD phenotypes require further analysis.
Apart from AAO, the concept of polygenic risk scores (PRS) in sporadic forms of PD has recently been established to assess the complex genetic architecture of PD beyond known rare familial forms of PD with Mendelian inheritance of mutations in disease-causing genes9. Even though PRS were reported to be significantly negatively correlated with AAO10, potential effects of PRS on the disease severity and the phenotypic profile have not yet been explored in detail.
Previous studies focusing on the role of AAO in PD were limited by (i) not addressing the concomitant effect of the physiological ageing process on the clinical phenotype by modelling age-related effects in a healthy control group, (ii) including relatively small numbers of PD patients from highly specific subgroups (e.g. drug naïve), (iii) using different AAO cut-offs across the studies and (iv) lacking a detailed genetic profiling of the study sample to exclude individuals with monogenic forms and variants presenting a genetic risk factor for developing PD. Therefore, our study addresses these issues by combining a mono-centric idiopathic PD dataset and healthy control group (HC) with detailed genetic data with the aim (i) to investigate the effect of AAO on clinical phenotype in idiopathic PD, (ii) to separate the PD-related ageing effect from the natural ageing effect and finally (iii) to explore the effect of the genetic background reflected by PRS on the disease severity in idiopathic PD.
Results
Effect of AAO on clinical outcomes in PD
Several traits in PD phenotypic profiles were found in association with AAO. An overview of clinical outcomes, sociodemographic characteristics and comorbidities among participants of the Luxembourg Parkinson’s Study is shown in Tables 1 and 2. As expected, the PD group comprised more males than females (67% vs. 33%) with mean AAO of 61.8 ± 12.0 years and mean disease duration since diagnosis of 5.5 ± 5.5 years. The mean age at assessment (AAA) was 67.3 ± 11.0 years. To investigate the effects of AAO on the clinical outcomes, a multiple regression analysis adjusting for disease duration was performed with results shown in Fig. 1. The overall motor disease severity as reflected by modified H&Y, MDS-UPDRS III, frequency of falls and gait disorder were all significantly positively associated with AAO. With regard to the motor complications of PD, no significant association of AAO was found with total hours of dyskinesia/day, dystonia/day, nor OFF time/day, however, a significant negative association of AAO with the MDS-UPDRS IV total score was identified. Additionally, SCOPA-AUT total score and Starkstein Apathy scale had significant positive associations with AAO indicating that patients with higher AAO experience more non-motor symptoms including urinary incontinence. Cognition as reflected by the MoCA score was significantly negatively associated with AAO showing higher impairment in patients with an older AAO. Similarly, AAO was significantly negatively associated with olfactory dysfunction. All other putative associations were not significantly associated with AAO as shown in Fig. 1.

The colour blue indicates significant negative effects of AAO on the clinical outcome, and the colour red indicates significant positive effects at the Bonferroni-adjusted 5% level. The binary variables are annotated by asterisk. Clinical symptoms and scales are described in Supplementary Material.
Analysing the difference in ageing effect in PD vs HC
When investigating the effects of AAA and AAO on the clinical phenotypes of PD, all associations were found to be comparable in both models (cf. Table 3). The reason is the strong correlation between AAA and AAO (statistically significant Kendall’s tau ρ = 0.73, see Supplementary Fig. 1). To investigate an effect of physiological ageing on the PD phenotypes, we also included the HC group into the regression models. When investigating the ageing-associated effects in PD, we determined a significant positive association in PD between AAA and H&Y, MDS-UPDRS III, frequency of falls and urine incontinence, SCOPA-AUT, Starkstein Apathy Scale as well as significant negative association between AAA and MoCA and Sniffin’ Stick test (cf. Table 3). Similarly in the HC group, we found a significant positive association between AAA and MDS-UPDRS III, SCOPA-AUT, Starkstein Apathy Scale, frequency of urine incontinence and gait disorder as well as significant negative association between AAA and MoCA and Sniffin’ Stick test as demonstrated in Table 4. Surprisingly, after comparing the ageing effect between PD vs HC (i.e. comparing effect of AAA on the clinical variables; see Table 5, column AAA:status), the only significant differences between PD and HC were found for H&Y, MDS-UPDRS III, MDS-UPDRS IV and MoCA indicating that the concomitant ageing process might be the main determinant of the non-motor PD phenotypic differences when studying the isolated effect of age in PD.
Correlation between AAO and PRS and its effect on severity of the PD phenotype
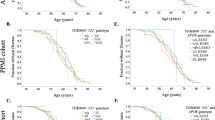
Using a polygenic risk score defined by the imputed genotypic data from the Luxembourg Parkinson’s Study and the summary statistics of 90 single nucleotide polymorphisms (SNP) that were previously identified to be genome-wide significantly associated with PD risk, we identified a significant negative correlation between PRS and AAO as shown in Fig. 2. However, neither Kendall’s tau correlation test for continuous variables nor Mann–Whitney U test for binary variables estimating the effect of PRS on clinical outcomes nor multiple regression models including PRS adjusted for AAA and disease duration showed effects of PRS on the severity of the clinical phenotype as demonstrated in Tables 6 and 7 respectively.

Significant inverse association was determined between AAO and PRS and AAA and PRS indicating the younger the AAO of PD, the higher cummulative burden of small effect size variants (represented by PRS).
Discussion
The presented cross-sectional analysis of PD patients and HC at the baseline clinical visit uses data from one of the largest ongoing observational studies, focusing on PD with demographic and clinical parameters corresponding closely to other recently published large PD datasets11,12,13. In our study, we have identified several significant associations of different PD-associated motor and non-motor symptoms with AAO using a comprehensive set of clinical assessments. This is in line with previous cross-sectional, retrospective and prospective studies suggesting that later onset PD is associated with a more rapid progression rate of motor symptoms4,11,14,15. Conversely, comparing to the Cardiff community-based PD longitudinal cohort16 and the longitudinal study at the Movement Disorders Clinic Saskatchewan4, both demonstrating higher frequency of dyskinesia, motor fluctuations and dystonia in the younger onset groups vs. older onset groups, we could not identify such associations with AAO. Only an overall burden of motor complications reflected by MDS-UPDRS IV score was significantly negatively associated with AAO in our study. The significant positive association of olfactory dysfunction and significant negative association of cognitive performance with AAO observed in our study correlate with previous findings17,18 and in terms of cognitive impairment it might point to a decreased ability of senescent brain to cope with the pathological neurodegenerative process known as cognitive resilience19. Additionally, another large multi-centric study using the Quebec Parkinson Network (QPN) dataset of over 1000 PD individuals showed comparable results with a positive association between late-onset PD and higher motor burden reflected by H&Y, higher cognitive decline and higher frequency of falls, but differed on significantly higher frequency of constipation and hallucinations late-onset PD (defined as AAO > 50 years) compared to early onset PD11. However, most scales applied in QPN differ from our study and different categorical approaches were used in QPN both for AAO and disease duration, influencing the comparability of results. To summarise our results, the earlier AAO, patients experience a lower level of motor impairment, lower cognitive impairment and less global autonomic dysfunction, apathy and olfactory deficit, but present with more motor complications even after adjusting for disease duration as a main determinant of disease severity.
These phenotypic differences observed in PD based on different AAO were previously not clearly separated from the physiological ageing process and challenged the concept that phenotypic differences are related specifically to the age at which the disease first manifests. This intriguing aspect evolves from the inherent close correlation between the main co-variates (AAA, AAO and disease duration) and thus raises a major methodological concern in most of the cross-sectional studies when aiming at determining the effect of all three co-variates on the clinical outcomes in a single model as discussed by Johnson et al. 200220. Therefore, we tried to disentangle the effect of ageing on the clinical phenotype in the cross-sectional setting by determining the ageing effect in individuals with and without PD. Surprisingly, the effect of ageing (AAA) on clinical outcomes in PD vs HC differed significantly only in motor disease severity (H&Y, MDS-UPDRS III), motor complications (MDS-UPDRS IV) and cognitive performance. These results suggest that the majority of the observed significant non-motor phenotypic differences in PD should be attributed rather to the physiological ageing process itself than age-specific dynamics of PD.
When considering the effect and role of AAO and age in classification of the respective PD phenotypes, potential underlying genetic determinants need to be considered. It is well known that rare disease-causing mutations in monogenic PD (e.g. in PARKIN, PINK1, SNCA or GBA21,22,23) have an effect on both AAO and PD phenotype. However, until now only few studies have explored the cumulative effects of common genetic variants with small effect sizes (as defined by PRS) on the clinical phenotype24. Here our results are in line with several recent studies observing no significant association between PRS and cognitive decline, severity of motor symptoms25 or ICD26 in contrast to other longitudinal prospective study27. It is worth noting that our statistical models included individuals without any known PD causing monogenic mutation or genetic risk variant (i.e. PD-associated variants in the GBA gene). Nevertheless, the significance of the PRS effect on clinical outcomes did not change in the models including PD-associated mutation or genetic variant carriers. Together with the significant negative correlation between AAO and PRS (cf. Fig. 2), our findings suggest that PRS may increase the risk to develop PD but might not have an effect on the severity of the disease phenotype. This observation is in favour of the hypothesis that initiation of the disease on one hand and the disease progression rate on the other might be driven by distinct factors.
Besides the mentioned strengths of our study design, several limitations need to be considered. First, the cross-sectional design does not allow for the identification of causal relations between AAO and clinical phenotypes. Second, we cannot consider the Luxembourg Parkinson’s Study as community-based by design, although some clinical indicators (such as mean AAO and male-to-female ratio) correspond closely to several community-based studies28,29,30,31. Third, we observe a relatively high frequency of positive family history of parkinsonism in the HC group (26% vs. 25% in PD) as well as high frequency of a family history of dementia in HC (32% vs 24%). We assume that there are two principal reasons why we observe increased frequencies of neurodegenerative diseases in HC group: (i) HC with personal experience with parkinsonism and/or dementia in their family are more aware to support research and (ii) family members of study participants are more inclined to participate in the study. To address these points and eliminate a potential bias, we excluded 1st, 2nd and 3rd degree relatives from our statistical models.
In summary, our study sought to overcome limitations identified in previous studies on the role of AAO in PD by (i) including substantially higher number of PD patients and HCs in the model accounting for the independent effect of ageing, (ii) our study being based on monocentric data collection and including PD patients of all disease stages regardless of the cognitive status, (iii) investigating an idiopathic dataset of PD and PD-related mutation free HC, (iv) refuting the categorisation bias by a priori arbitrary AAO grouping, and finally (v) exploring the effect of PRS on severity of the PD phenotype in a large genotyped sample.
Methods
Study population
All subjects were recruited from March 2015 until 10th December 2020 in the frame of the nation-wide monocentric observational longitudinal Luxembourg Parkinson’s Study. The diagnosis of PD was based on UKPDSBB diagnostic criteria32. The initial visit dataset of 430 PD patients and 556 HC genetically screened by both NeuroChip and PacBio were analysed after exclusion of 6 PD and 39 HC individuals for 1st, 2nd and 3rd degree relationships and after exclusion of 53 PD carriers and 27 HC carriers of pathogenic PD-associated variants. The overall study design, inclusion and exclusion workflow are illustrated in Fig. 3.

PD individuals with Parkinson’s disease, HC healthy control.
All participants taking part in Luxembourg Parkinson’s Study agreed and signed a written informed consent. The study has been approved by the National Ethics Board (CNER Ref: 201407/13). The patients with PD were included regardless of the disease duration, cognitive status, age or disease stage. The HC were partially recruited from the pool of independent observational studies in Luxembourg (ORISCAV-LUX study; EHES-LUX) or were recruited from Luxembourg or the surrounding area of Greater Region based on individual interest not meeting any of the exclusion criteria (presence of a neurodegenerative disorder, active cancer; age under 18 and pregnant women)33.
Clinical assessment and data
A description of the design of the Luxembourg Parkinson’s Study was previously published33. Sociodemographic characteristics and clinical outcomes validated for PD were chosen from the basic clinical assessment battery and listed in Tables 1 and 2. Validated self-administered questionnaires and scales for PD were used. All patients have been evaluated in medication ON state and where applicable, in deep brain stimulation ON state. AAO is defined as age at diagnosis of PD. The clinical symptoms as scales are defined in detail in the Supplementary material.
Missing data statement
The absolute number of missing data per variable are shown in Tables 1 and 2. Given the low proportions of missing values in the outcome variables and 0% of missing values in the co-variates (AAA, AAO and disease duration), we used a pairwise deletion for all statistical models.
Genotyping and quality-control analyses
DNA samples were genotyped using the NeuroChip array (v.1.0 and v1.1; Illumina, San Diego, CA) that was specifically designed to integrate rare and common neurodegenerative disease-related variants34. Quality-control (QC) analysis was performed as follows: samples with call rates < 95% and whose genetically determined sex deviated from reported sex in clinical data were excluded from the analysis, and the filtered variants were checked for cryptic relatedness and excess of heterozygosity. Samples exhibiting excess heterozygosity (F statistic > 0.2) and first-degree relatedness were excluded. Once sample QC was completed, SNPs with Hardy−Weinberg equilibrium P value < 1E−6, and missingness rates >5% were excluded. All samples except for twelve from all individuals entering the analysis after exclusion of the 1st, 2nd and 3rd degree relatives and presence of PD-linked mutation and genetic risk factors passed the QC (424 PD and 550 HC). The data were then imputed using the Haplotype Reference Consortium r1.1 2016 and the Michigan Imputation Server and filtered for imputation quality (RSQ > 0.8)35. Genetic analysis and QC was done using PLINK v1.9. Additionally, all samples underwent targeted sequencing of the GBA locus using single-molecule sequencing on a Sequel II sequencer from Pacific BioScience36. Variants were called with DeepVariant 1.037. PD causing rare variants were defined by the ClinVar classification ‘pathogenic/likely-pathogenic’. All PD causing variants (listed in Supplementary material) identified by any method were Sanger validated and all samples with a validated PD causing variant were excluded from further analysis.
Polygenic risk score (PRS)
We generated PRSs with PRSice-2 under default settings. PRSs for each individual were calculated using the imputed genotype data from Luxembourg Parkinson’s Study as a target sample. The base GWAS data used to determine PRS for PD was the summary statistics of the 90 SNPs that were previously found to be genome-wide significantly associated with PD risk38. The criteria for linkage disequilibrium (LD) clumping of SNPs were pairwise LD r2 < 0.1 within the 250 kb window. Briefly, PRSs were calculated by summing the weighted effects of GWAS PD risk genetic variants present in the target samples, with a possible proxy of R2 > 0.9, meeting p value thresholds ranging from 5e−08 to 0.5. The values of PRS were Z-normalised.
Statistical analysis
Firstly, we performed an intergroup comparison (PD vs HC) of sociodemographic and clinical characteristics as well as polygenic risk score and comorbidities with the Mann−Whitney U test for numerical variables and Fisher’s exact test for binary variables (Tables 1 and 2). Secondly, we used multiple regression models (linear and logistic) to identify effects of AAO (as a numerical variable) on numerical or binary clinical outcomes accounting for disease duration (Fig. 1). Subsequently, we performed a multiple regression model for both HC and PD (Table 5) to examine whether the effect of ageing (AAA) on clinical outcomes differs between HC and PD adjusted for disease duration. For this, we included the main effects of the continuous variable AAA and the binary variable status (HC: status = 0, PD: status = 1), their interaction effect (HC: status*AAA = 0, PD: status*AAA > 0), and the main effect of the continuous variable disease duration (HC: duration = 0, PD: duration > 0). To investigate the role of PRS in PD, a pairwise association analysis with Kendall’s tau correlation test between PRS and AAO and AAA was performed (Fig. 2). Furthermore, we performed a Kendall correlation test between PRS and clinical outcome for PD and HC respectively (Table 6). As a last step, we employed a multiple regression model including PRS adjusting for AAA and disease duration, to investigate the effect of PRS on the clinical phenotype in PD (Table 7). At all instances, the significance at the 5% level and the Bonferroni-adjusted 5% level was set.
Data availability
The dataset for this manuscript is not publicly available as it is linked to the Luxembourg Parkinson’s Study and its internal regulations. Any requests for accessing the dataset can be directed to request.ncer-pd@uni.lu.
Code availability
The code for the statistical models is available at: https://doi.org/10.17881/hr67-ba06.
Change history
02 September 2022
A Correction to this paper has been published: https://doi.org/10.1038/s41531-022-00378-9
References
Elizabeth, Qian & Yue, Huang Subtyping of Parkinson’s disease - where are we up to? Aging Dis. 10, 1130–1139 (2019).
Rodríguez-Violante, M., Cervantes-Arriaga, A., Fahn, S. & Tolosa, E. Two-hundred years later: Is Parkinson’s disease a single defined entity? Rev. Invest Clin. 69, 308–313 (2017).
Krüger, R. et al. Classification of advanced stages of Parkinson’s disease: translation into stratified treatments. J. Neural Transm. 124, 1015–1027 (2017).
Pagano, G., Ferrara, N., Brooks, D. J. & Pavese, N. Age at onset and Parkinson disease phenotype. Neurology 86, 1400–1407 (2016).
Jellinger, K. A. Parkinson disease with old-age onset. Arch. Neurol. 60, 1814–1815 (2003).
Zhou, M. Z. et al. The association between non-motor symptoms in Parkinson’s disease and age at onset. Clin. Neurol. Neurosurg. 115, 2103–2107 (2013).
Ferguson, L. W., Rajput, A. H. & Rajput, A. Early-onset vs. Late-onset Parkinson’s disease: a clinical-pathological study. Can. J. Neurol. Sci. 43, 113–119 (2016).
Jellinger, K. A. Very old onset parkinsonism: a clinical-pathological study. Parkinsonism Relat. Disord. 57, 39–43 (2018).
Ohnmacht, J., May, P., Sinkkonen, L. & Krüger, R. Missing heritability in Parkinson’s disease: the emerging role of non-coding genetic variation. J. Neural Transm. 127, 729–748 (2020).
Escott-Price, V., International Parkinson’s Disease Genomics Consortium & Nalls, M. A. et al. Polygenic risk of Parkinson disease is correlated with disease age at onset. Ann. Neurol. 77, 582–591 (2015).
Gan-Or, Z. et al. The Quebec Parkinson network: a researcher-patient matching platform and multimodal biorepository. J. Parkinsons Dis. 10, 301–313 (2020).
Santos García, D. et al. COPPADIS-2015 (COhort of Patients with PArkinson’s DIsease in Spain, 2015): an ongoing global Parkinson’s disease project about disease progression with more than 1000 subjects included. Results from the baseline evaluation. Eur. J. Neurol. 26, 1399–1407 (2019).
Marek, K. et al. The Parkinson’s progression markers initiative (PPMI) - establishing a PD biomarker cohort. Ann. Clin. Transl. Neurol. 5, 1460–1477 (2018).
Diederich, N. J., Moore, C. G., Leurgans, S. E., Chmura, T. A. & Goetz, C. G. Parkinson disease with old-age onset: a comparative study with subjects with middle-age onset. Arch. Neurol. 60, 529–533 (2003).
Wickremaratchi, M. M. et al. The motor phenotype of Parkinson’s disease in relation to age at onset. Mov. Disord. 26, 457–463 (2011).
Mehanna, R., Moore, S., Hou, J. G., Sarwar, A. I. & Lai, E. C. Comparing clinical features of young onset, middle onset and late onset Parkinson’s disease. Parkinsonism Relat. Disord. 20, 530–534 (2014).
Chase, B. A. & Markopoulou, K. Olfactory dysfunction in familial and sporadic Parkinson’s Disease. Front Neurol. 11, 447 (2020).
Kim, R., Shin, J. H., Park, S., Kim, H. J. & Jeon, B. Longitudinal evolution of non-motor symptoms according to age at onset in early Parkinson’s disease. J. Neurol. Sci. 418, 117157 (2020).
Pettigrew, C. & Soldan, A. Defining cognitive reserve and implications for cognitive aging. Curr. Neurol. Neurosci. Rep. 19, 1 (2019).
Johnson, S. B. & Meltzer, L. J. Disentangling the effects of current age, onset age, and disease duration: parent and child attitudes toward diabetes as an exemplar. J. Pediatr. Psychol. 27, 77–86 (2002).
Blauwendraat, C. et al. Genetic modifiers of risk and age at onset in GBA associated Parkinson’s disease and Lewy body dementia [published correction appears in Brain]. Brain 143, 234–248 (2020).
Yahalom, G. et al. Age at onset of Parkinson’s disease among Ashkenazi Jewish patients: contribution of environmental factors, LRRK2 p.G2019S and GBA p.N370S mutations. J. Parkinsons Dis. 10, 1123–1132 (2020).
Hernandez, D. G., Reed, X. & Singleton, A. B. Genetics in Parkinson disease: Mendelian versus non-Mendelian inheritance. J. Neurochem. 139, 59–74 (2016).
Manolio, T. A. et al. Finding the missing heritability of complex diseases. Nature 461, 747–753 (2009).
Liu, G. et al. Genome-wide survival study identifies a novel synaptic locus and polygenic score for cognitive progression in Parkinson’s disease. Nat. Genet 53, 787–793 (2021).
Ihle, J. et al. DIGPD study group; Parkinson’s disease polygenic risk score is not associated with impulse control disorders: a longitudinal study. Parkinsonism Relat. Disord. 75, 30–33 (2020).
Paul, K. C., Schulz, J., Bronstein, J. M., Lill, C. M. & Ritz, B. R. Association of polygenic risk score with cognitive decline and motor progression in Parkinson disease. JAMA Neurol. 75, 360–366 (2018).
Alves, G. et al. Incidence of Parkinson’s disease in Norway: the Norwegian ParkWest study. J. Neurol. Neurosurg. Psychiatry 80, 851–857 (2009).
Granieri, E. et al. Parkinson’s disease in Ferrara, Italy, 1967 through 1987. Arch. Neurol. 48, 854–857 (1991).
Winter, Y. et al. Incidence of Parkinson’s disease and atypical parkinsonism: Russian population-based study. Mov. Disord. 25, 349–356 (2010).
Savica, R., Grossardt, B. R., Rocca, W. A. & Bower, J. H. Parkinson disease with and without Dementia: a prevalence study and future projections. Mov. Disord. 33, 537–543 (2018).
Litvan, I. et al. SIC Task Force appraisal of clinical diagnostic criteria for parkinsonian disorders. Mov. Disord. 18, 467–486 (2003).
Hipp, G. et al. The Luxembourg Parkinson’s study: a comprehensive approach for stratification and early diagnosis. Front Aging Neurosci. 10, 326 (2018).
Blauwendraat, C. et al. NeuroChip, an updated version of the NeuroX genotyping platform to rapidly screen for variants associated with neurological diseases. Neurobiol. Aging 57, 247.e9–247.e13 (2017).
Das, S. et al. Next-generation genotype imputation service and methods. Nat. Genet 48, 1284–1287 (2016).
Korlach, Jonas et al. Real-time DNA sequencing from single polymerase molecules. Methods Enzymol. 472, 431–455 (2010).
Poplin, R. et al. A universal SNP and small-indel variant caller using deep neural networks. Nat. Biotechnol. 36, 983–987 (2018).
Nalls, M. A. et al. Identification of novel risk loci, causal insights, and heritable risk for Parkinson’s disease: a meta-analysis of genome-wide association studies. Lancet Neurol. 18, 1091–1102 (2019).
Acknowledgements
We would like to give special thanks to all participants in the Luxembourg Parkinson’s Study. Furthermore, we acknowledge the joint effort of the NCER-PD consortium members generally contributing to the Luxembourg Parkinson’s Study as listed below. The work presented here was supported within the framework of the National Centre of Excellence in Research on Parkinson’s Disease (NCER-PD) funded by the Luxembourg National Research Fund (FNR/NCER13/BM/11264123), the PEARL program (FNR/P13/6682797 to R.K.), MotaSYN (12719684 to R.K.), MAMaSyn (to R.K.), MiRisk‐PD (C17/BM/11676395 to R.K., E.G., P.M.), the FNR/DFG Core INTER (ProtectMove, FNR11250962 to P.M.), and the PARK-QC DTU (PRIDE17/12244779/PARK-QC to R.K. and S.P.), FNR PD-Strat (INTER/11651464 to EG), DIGIPD (ERAPERMED 2020-314 to EG).
Author information
Authors and Affiliations
Consortia
Contributions
L.P.: Conceived, organised, and executed the research project; co-executed the statistical analysis and interpretation of results; wrote the manuscript; substantially participated in data collection, data exportation and data curation. R.K.: Conceived, organised, and co-executed the research project; participated in interpretation of results; critically revised the manuscript. A.R.: Executed the statistical analysis and interpretation, critically revised the manuscript, substantially participated in data curation. E.G.: Co-executed the research project; participated in interpretation of results; critically revised the manuscript. P.M.: Executed the genetic analysis; participated in interpretation of results; critically revised the manuscript. S.P.: Contributed genetic data; co-executed the research project; critically revised the manuscript. Z.L.: Executed the genetic analysis; participated in interpretation of results; critically revised the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pavelka, L., Rauschenberger, A., Landoulsi, Z. et al. Age at onset as stratifier in idiopathic Parkinson’s disease – effect of ageing and polygenic risk score on clinical phenotypes. npj Parkinsons Dis. 8, 102 (2022). https://doi.org/10.1038/s41531-022-00342-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41531-022-00342-7
This article is cited by
-
The combined effect of lifestyle factors and polygenic scores on age at onset in Parkinson’s disease
Scientific Reports (2024)
-
Clinical utility of polygenic risk scores: a critical 2023 appraisal
Journal of Community Genetics (2023)
-
Accurate long-read sequencing identified GBA1 as major risk factor in the Luxembourgish Parkinson’s study
npj Parkinson's Disease (2023)
