
Learning objectives
Upon completion of this activity, participants will be able to:
-
1.
Distinguish the annual incidence of essential infantile esotropia (EIE) in the current study.
-
2.
Assess the mean ages at diagnosis and intervention for EIE in the current study.
-
3.
Compare characteristics of children who received observational management for EIE vs active interventions.
-
4.
Evaluate outcomes of surgical treatment for EIE vs botulinum toxin in the current study.
Accreditation statements
In support of improving patient care, this activity has been planned and implemented by Medscape, LLC and Springer Nature. Medscape, LLC is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
Medscape, LLC designates this Journal-based CME activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Credit hours
1.0

Release date: February 2, 2024
Expiration date: February 2, 2025
Post-test link: https://www.medscape.org/eye/posttest999130
EDITOR
Sobha Sivaprasad, MD, Editor, Eye
Journal CME author disclosure information
Charles P. Vega has the following relevant financial relationships: Consultant or advisor for Boehringer Ingelheim Pharmaceuticals, Inc.; GlaxoSmithKline; Johnson & Johnson Services, Inc.
Abstract
Background/objectives
A national study was undertaken through the British ophthalmology surveillance unit (BOSU) to determine the incidence, presenting features and management of essential infantile esotropia (EIE) in the UK.
Methods
Data from a prospective national observational study of newly diagnosed EIE presenting to clinicians in the United Kingdom over a 12-month period were collected. Cases with a confirmed diagnosis by a clinician of a constant, non-accommodative esotropia ≥20 prism dioptres (PD), presenting at ≤12 months, with no neurological or ocular abnormalities were identified through BOSU. Follow-up data were collected at 12 months.
Results
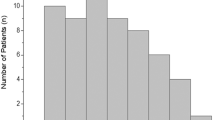
A total of 57 cases were reported giving an incidence of EIE of 1 in 12,828 live births. The mean age of diagnosis and intervention were 7.05 ± 2.6 months (range 2–12) and 14.7 ± 4.9 months (range 6.5–28.1), respectively. Management was surgical in 59.6%, botulinum toxin alone in 22.8%, and 17.5% were observed. The preoperative angle of esotropia was smaller in the observation group (P = 0.04). The postoperative angle of esotropia was not statistically significant between botulinum toxin or surgery (P = 0.3), although the age of intervention was earlier in the botulinum group (P = 0.007). Early intervention (before 12 months of age) did not influence the post-intervention motor outcomes between 0 and 10 prism dioptres of esotropia (P = 0.78).
Conclusions
The incidence of EIE in the UK is considerably lower than reported in other population-based studies. The preferred method of treatment was surgical with earlier intervention in those treated with botulinum toxin. An early age of intervention (<12 months) did not influence motor outcomes.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 18 print issues and online access
$259.00 per year
only $14.39 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others


Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request. This data will not be available past 2030.
References
Louwagie CR, Diehl NN, Greenberg AE, Mohney BG. Is the incidence of infantile esotropia declining?: a population-based study from Olmsted County, Minnesota, 1965 to 1994. Arch Ophthalmol. 2009;127:200–3.
Arora A, Williams B, Arora AK, McNamara R, Yates J, Fielder A. Decreasing strabismus surgery. Br J Ophthalmol. 2005;89:409–12.
Carney CV, Lysons DA, Taplet JV. Is the incidence of constant esotropia in childhood reducing? Eye. 1995;9:40–1.
Ferguson JA, Goldacre MJ, Henderson J, Bron AJ. Ophthalmology in the Oxford region: analysis of time trends from linked statistics. Eye (Lond). 1991;5:379–84.
MacEwen CJ, Chakrabarti HS. Why is squint surgery in children in decline? Br J Ophthalmol. 2004;88:509–11.
Finlay R. Unexpected beneficial effects of measles immunisation. Number of squint operations has decreased. BMJ. 2000;320:939.
Heng SJ, MacEwen CJ. Decrease in the rate of esotropia surgery in the United Kingdom from 2000 to 2010. Br J Ophthalmol. 2013;97:598–600.
Lyons C. Surgery for infantile esotropia: how early is early? / Le traitement chirurgicale de l’esotropie infantile: «precoce», qu’est-ce a dire? Can J Ophthalmol. 2008;43:629.
Wong AM. Timing of surgery for infantile esotropia: sensory and motor outcomes. Can J Ophthalmol. 2008;43:643–51.
McNeer KW, Tucker MG, Spencer RF. Botulinum toxin management of essential infantile esotropia in children. Arch Ophthalmol. 1997;115:1411–8.
Wright KW, Edelman PM, McVey JH, Terry AP, Lin M. High-grade stereo acuity after early surgery for congenital esotropia. Arch Ophthalmol. 1994;112:913–9.
Campos EC, Schiavi C, Bellusci C. Critical age of botulinum toxin treatment in essential infantile esotropia. J Pediatr Ophthalmol Strabismus. 2000;37:328–32. quiz 54–5.
Simonsz HJ, Kolling GH, Unnebrink K. Final report of the early vs. late infantile strabismus surgery study (ELISSS), a controlled, prospective, multicenter study. Strabismus. 2005;13:169–99.
Mayet I, Ally N, Alli HD, Tikly M, Williams S. Botulinum neurotoxin injections in essential infantile esotropia-a comparative study with surgery in large-angle deviations. Eye (Lond). 2021;35:3071–6.
de Alba Campomanes AG, Binenbaum G, Campomanes Eguiarte G. Comparison of botulinum toxin with surgery as primary treatment for infantile esotropia. J AAPOS. 2010;14:111–6.
Birch E, Stager D, Wright K, Beck R. The natural history of infantile esotropia during the first six months of life. Pediatric Eye Disease Investigator Group. J AAPOS. 1998;2:325–8.
Pediatric Eye Disease Investigator Group, Christiansen SP, Chandler DL, Holmes JM, Arnold RW, Birch E, et al. Instability of ocular alignment in childhood esotropia. Ophthalmology. 2008;115:2266–74.
Simonsz HJ, Kolling GH. Best age for surgery for infantile esotropia. Eur J Paediatr Neurol. 2011;15:205–8.
Birch EE, Stager DR Sr. Long-term motor and sensory outcomes after early surgery for infantile esotropia. J AAPOS. 2006;10:409–13.
Graham PA. Epidemiology of strabismus. Br J Ophthalmol. 1974;58:224–31.
Darlow BA, Clemett RS, Horwood LJ, Mogridge N. Prospective study of New Zealand infants with birth weight less than 1500 g and screened for retinopathy of prematurity: visual outcome at age 7-8 years. Br J Ophthalmol. 1997;81:935–40.
VanderVeen DK, Allred EN, Wallace DK, Leviton A, Investigators ES. Strabismus at age 2 years in children born before 28 weeks’ gestation: antecedents and correlates. J Child Neurol. 2016;31:451–60.
Louwagie CR, Diehl NN, Greenberg AE, Mohney BG. Long-term follow-up of congenital esotropia in a population-based cohort. J AAPOS. 2009;13:8–12.
Fu VL, Stager DR, Birch EE. Progression of intermittent, small-angle, and variable esotropia in infancy. Invest Ophthalmol Vis Sci. 2007;48:661–4.
Pediatric Eye Disease Investigator Group. Spontaneous resolution of early-onset esotropia: experience of the Congenital Esotropia Observational Study. Am J Ophthalmol. 2002;133:109–18.
Bhate M, Flaherty M, Martin FJ. Timing of surgery in essential infantile esotropia—what more do we know since the turn of the century? Indian J Ophthalmol. 2022;70:386–95.
Birch EE, Fawcett S, Stager DR. Why does early surgical alignment improve stereoacuity outcomes in infantile esotropia? J AAPOS. 2000;4:10–4.
O’Connor AR, Fawcett SI, Stager D. Factors influencing sensory outcome following surgical correction of infantile esotropia. Am Orthopt J. 2002;52:69–74.
Gerth C, Mirabella G, Li X, Wright T, Westall C, Colpa L, et al. Timing of surgery for infantile esotropia in humans: effects on cortical motion visual evoked responses. Invest Ophthalmol Vis Sci. 2008;49:3432–7.
Acknowledgements
Special thanks to Anwen Coughlan and Tina McDonald for their help with the data collection. Special thanks to the following for their participation in the BOSU study: Adam Bates, Anna Maino, Annegret Dahlmann-Noor, Anthony Quinn, Clare Roberts, Conrad Schmoll, Geeta Thurairajan, Gill Adams, I.Chris Lloyd, Jan Hoole, Jane Ashworth, Jeremy Butcher, Joanne Hancox, John Ferris, Kate Taylor, Lawrence Gnanaraj, Louise Allen, Lucy Barker, Luke Clifford, M.Ashwin Reddy, Manor Parulekar, Maria Theodorou, Maria Tsimpida, Peter Tiffin, Richard Bowman, Richard Smith, Robert Taylor, Rod Savides, Rosemary Lambley, Rosie Brennan, Stephanie West, Tamsin Sleep, Tina Duke, Vasileios Kostakis, Vernon Geh, Alan Mulvihill, Annie Joseph, Anthony Vivian, Aravind Reddy, Bina Parmar, Dinesh Dave, David Jones, G. A. Shun-Shin, James Acheson, Kate Bush, Michael Clarke, Shona Sutherland, Stephen Burgess, Susmito Biswas, Tina Duke, and Victoria Barrett.
Funding
The Paediatric Eye Fund at Cardiff and Vale University Health Board kindly funded a total of £5000.
Author information
Authors and Affiliations
Contributions
DCMY: research design, data collection, data analysis, manuscript preparation. RD: data collection. WJW: data analysis. PW: research concept, research design, data analysis, manuscript preparation.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Yeo, D.C.M., Davies, R., Watkins, W.J. et al. The incidence, clinical features, and management of essential infantile esotropia in the United Kingdom. A British Ophthalmology Surveillance Unit (BOSU) study. Eye 38, 680–686 (2024). https://doi.org/10.1038/s41433-023-02901-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-023-02901-5
