
Background
Pancreatic ductal adenocarcinoma (PDAC) harbouring germline BRCA1-2 pathogenic variants (gBRCA1-2pv) is a distinct nosological entity. Information on second-line therapy (2LT) outcome in this setting is lacking.
Methods
Data of gBRCA1-2pv metastatic PDAC patients treated with chemotherapy were collected. A primary analysis of 2LT RECIST response, median progression-free survival (mPFS2) and overall survival (mOS2), was performed. A secondary analysis addressed the impact of timing of platinum introduction on the outcome of patients receiving at least a first-line combination chemotherapy (1LT).
Results
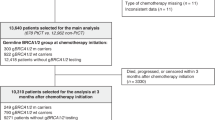
Eighty-four gBRCA1-2pv metastatic PDAC patients were enrolled. The primary analysis, including 43 patients, highlighted a significant improvement of mPFS2 and a doubled response rate, in the platinum-based 2LT subgroup as compared to the platinum-free (8.8 versus 3.7 months, p = 0.013). Seventy-seven patients were included in the secondary analysis. Median PFS1 of 3- and 4-drug platinum-based 1LT significantly outperformed both platinum-free combinations and platinum-based doublets (11.4 versus 6.4 versus 7.9 months, p = 0.01). Albeit still immature, data on mOS paralleled those on mPFS.
Conclusions
This study highlighted the beneficial role of platinum agents in gBRCA1-2pv PDAC patients also in second-line treatment setting. However, our data suggest that early use of 3- and 4-drug platinum-based chemotherapy combinations provides a survival outcome advantage.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 24 print issues and online access
$259.00 per year
only $10.79 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

Data availability
Data are available upon reasonable request.
References
Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin. 2021;71:7–33.
Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74:2913–21.
Park W, Chawla A, O’Reilly EM. Pancreatic cancer: a review. JAMA. 2021;326:851–62.
Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369:1691–703.
Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364:1817–25.
Reni M, Zanon S, Peretti U, Chiaravalli M, Barone D, Pircher C, et al. Nab-paclitaxel plus gemcitabine with or without capecitabine and cisplatin in metastatic pancreatic adenocarcinoma (PACT-19): a randomised phase 2 trial. Lancet Gastroenterol Hepatol. 2018;3:691–7.
Blomstrand H, Batra A, Cheung WY, Elander NO. Real-world evidence on first- and second-line palliative chemotherapy in advanced pancreatic cancer. World J Clin Oncol. 2021;12:787–99.
Cherri S, Noventa S, Zaniboni A. Pancreatic adenocarcinoma: beyond first line, where are we? World J Gastroenterol. 2021;27:1847–63.
Gill S, Ko YJ, Cripps C, Beaudoin A, Dhesy-Thind S, Zulfiqar M, et al. PANCREOX: a randomized phase III study of fluorouracil/leucovorin with or without oxaliplatin for second-line advanced pancreatic cancer in patients who have received gemcitabine-based chemotherapy. J Clin Oncol. 2016;34:3914–20.
Oettle H, Riess H, Stieler JM, Heil G, Schwaner I, Seraphin J, et al. Second-line oxaliplatin, folinic acid, and fluorouracil versus folinic acid and fluorouracil alone for gemcitabine-refractory pancreatic cancer: outcomes from the CONKO-003 trial. J Clin Oncol. 2014;32:2423–9.
Wang-Gillam A, Li CP, Bodoky G, Dean A, Shan YS, Jameson G, et al. Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1): a global, randomised, open-label, phase 3 trial. Lancet. 2016;387:545–57.
Taieb J, Prager GW, Melisi D, Westphalen CB, D’Esquermes N, Ferreras A, et al. First-line and second-line treatment of patients with metastatic pancreatic adenocarcinoma in routine clinical practice across Europe: a retrospective, observational chart review study. ESMO Open. 2020;5:e000587.
Golan T, Kanji ZS, Epelbaum R, Devaud N, Dagan E, Holter S, et al. Overall survival and clinical characteristics of pancreatic cancer in BRCA mutation carriers. Br J Cancer. 2014;111:1132–8.
Peretti U, Cavaliere A, Niger M, Tortora G, Di Marco MC, Rodriquenz MG, et al. Germinal BRCA1-2 pathogenic variants (gBRCA1-2pv) and pancreatic cancer: epidemiology of an Italian patient cohort. ESMO Open. 2021;6:100032.
Golan T, Hammel P, Reni M, Van Cutsem E, Macarulla T, Hall MJ, et al. Maintenance Olaparib for germline BRCA-mutated metastatic pancreatic cancer. N Engl J Med. 2019;381:317–27.
Macchini M, Centonze F, Peretti U, Orsi G, Militello AM, Valente MM, et al. Treatment opportunities and future perspectives for pancreatic cancer patients with germline BRCA1-2 pathogenic variants. Cancer Treat Rev. 2021;100:102262.
Rebelatto TF, Falavigna M, Pozzari M, Spada F, Cella CA, Laffi A, et al. Should platinum-based chemotherapy be preferred for germline BReast CAncer genes (BRCA) 1 and 2-mutated pancreatic ductal adenocarcinoma (PDAC) patients? A systematic review and meta-analysis. Cancer Treat Rev. 2019;80:101895.
Wattenberg MM, Asch D, Yu S, O’Dwyer PJ, Domchek SM, Nathanson KL, et al. Platinum response characteristics of patients with pancreatic ductal adenocarcinoma and a germline BRCA1, BRCA2 or PALB2 mutation. Br J Cancer. 2020;122:333–9.
Orsi G, Di Marco M, Cavaliere A, Niger M, Bozzarelli S, Giordano G, et al. Chemotherapy toxicity and activity in patients with pancreatic ductal adenocarcinoma and germline BRCA1-2 pathogenic variants (gBRCA1-2pv): a multicenter survey. ESMO Open. 2021;6:100238.
Chiorean EG, Guthrie KA, Philip PA, Swisher EM, Jalikis F, Pishvaian MJ, et al. Randomized phase II study of PARP inhibitor ABT-888 (Veliparib) with modified FOLFIRI versus FOLFIRI as second-line treatment of metastatic pancreatic cancer: SWOG S1513. Clin Cancer Res. 2021;27:6314–22.
Conroy T, Hammel P, Hebbar M, Ben Abdelghani M, Wei AC, Raoul JL, et al. FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. N Engl J Med. 2018;379:2395–406.
Vivaldi C, Caparello C, Musettini G, Pasquini G, Catanese S, Fornaro L, et al. First-line treatment with FOLFOXIRI for advanced pancreatic cancer in clinical practice: patients’ outcome and analysis of prognostic factors. Int J Cancer. 2016;139:938–45.
Reni M, Balzano G, Zanon S, Zerbi A, Rimassa L, Castoldi R, et al. Safety and efficacy of preoperative or postoperative chemotherapy for resectable pancreatic adenocarcinoma (PACT-15): a randomised, open-label, phase 2-3 trial. Lancet Gastroenterol Hepatol. 2018;3:413–23.
Louvet C, Labianca R, Hammel P, Lledo G, Zampino MG, André T, et al. Gemcitabine in combination with oxaliplatin compared with gemcitabine alone in locally advanced or metastatic pancreatic cancer: results of a GERCOR and GISCAD phase III trial. J Clin Oncol. 2005;23:3509–16.
Sonbol MB, Ahn DH, Goldstein D, Okusaka T, Tabernero J, Macarulla T, et al. CanStem111P trial: a Phase III study of napabucasin plus nab-paclitaxel with gemcitabine. Future Oncol. 2019;15:1295–302.
Tempero M, Oh DY, Tabernero J, Reni M, Van Cutsem E, Hendifar A, et al. Ibrutinib in combination with nab-paclitaxel and gemcitabine for first-line treatment of patients with metastatic pancreatic adenocarcinoma: phase III RESOLVE study. Ann Oncol. 2021;S0923-7534:00098-3.
Giommoni E, Maiello E, Vaccaro V, Rondini E, Vivaldi C, Tortora G, et al. Activity and safety of NAB-FOLFIRI and NAB-FOLFOX as first-line treatment for metastatic pancreatic cancer (NabucCO Study). Curr Oncol. 2021;28:1761–72.
Funding
This study was partially supported by MyEverest ONLUS (no grant number).
Author information
Authors and Affiliations
Contributions
GO, MM and MR: conception of the study; data acquisition, analysis and interpretation. AC, GT, SL, MM, MDM, GG, EV, MS, SB, SN, MGR, AMM, IGR, IG, SDL, BM, AB, LS, LP, CP, AS, UP, MN, EG, IB, ET, KB, LF, MMV: data acquisition. SC: data interpretation. All authors: manuscript drafting, revision and final approval.
Corresponding author
Ethics declarations
Competing interests
GT reports advisory board for BMS, AZ, MSD, Merck, Servier. SL reports consulting or advisory role for Amgen, Merck, Serono, Lilly, Astra Zeneca, Incyte, Daiichi-Sankyo, Bristol-Myers Squibb, Servier, MSD; Speakers’ Bureau for Roche, Lilly, Bristol-Myers Squibb, Servier, Merck, Serono, Pierre-Fabre, GSK, Amgen; research funding for Amgen, Merck, Serono, Bayer, Roche, Lilly, Astra Zeneca, Bristol-Myers Squibb. LS reports speakers’ and consultant’s fee from MSD, Astra-Zeneca, Servier, Bayer, Merck, Amgen, Pierre-Fabre. AS reports advisory board or invited speaker for Pierre Fabre, Lilly, Merck, Viatris. MN reports travel expenses from Celgene, speaker honorarium from Accademia della Medicina; honoraria from Medpoint SRL for editorial collaboration; consultant honoraria from EMD Serono, Basilea Pharmaceutica, Incyte and MSD Italia. SC reports travel expenses and personal honoraria for the following companies: Speaker for Amgen, Bayer, Eli Lilly, Servier; Advisory Boards for Amgen, Eli Lilly, Bayer, Baxter, Merck Sharp & Dohme (MSD), Servier; Consultant for Amgen, Baxter, Eli Lilly, Celgene, Novartis, MSD; Research grant for Celgene, Eisai. MM reports personal honoraria as speaker or consultant for Astrazeneca, MSD, Boehringer Ingelheim, Pfizer, EUSA Pharma, Merck-Serono, Novartis, Roche, Ipsen, Mylan. MR reports advisory boards for Astra-Zeneca, PANAVANCE, Viatris, SOTIO, Servier, MSD, Lilly, Celgene, Shire, Baxter, Sanofi and a research grant from Astra-Zeneca. All remaining authors have declared no competing interests.
Ethics approval and consent to participate
Before testing, all patients signed an informed consensus statement that was revised and approved by a local ethics committee and allowed for genetic testing and data collection, analysis and elaboration. Data were irreversibly anonymised before entering into the database.
Consent for publication
Not applicable.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Orsi, G., Cavaliere, A., Tortora, G. et al. Second-line therapy in pancreatic ductal adenocarcinoma (PDAC) patients with germline BRCA1-2 pathogenic variants (gBRCA1-2pv). Br J Cancer 128, 877–885 (2023). https://doi.org/10.1038/s41416-022-02086-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41416-022-02086-w
