
Abstract
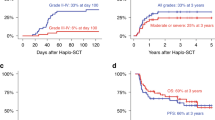
Hyper-IgM syndrome due to CD40 deficiency (HIGM3) is a rare disease with only a few reported cases of haematopoietic stem cell transplantation (HSCT). In retrospective study, we reviewed all patients with HIGM3 who underwent HSCT at King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia, between 2008 and 2013. Six patients were identified. Three male and three female patients from three families. The median age of diagnosis was 13 months (range, 1–28 months). All lacked CD40 expression on B cells by flow cytometry. The median time from diagnosis to transplantation was 8.5 months (range, 1–17 months). For all patients, the donors were HLA-identical siblings, with the exception of one patient for whom the donor was a sibling with one antigen mismatch. The conditioning regimen was busulfan and cyclophosphamide in five patients and busulfan, cyclophosphamide and antithymocyte globulin in one patient. For GVHD prophylaxis, cyclosporine and methotrexate was used. All patients engrafted. The survival rate was 100%, with a median follow-up of 54 months (range, 30–116 months). One patient developed acute GVHD. All patients showed complete immune recovery with positive CD40 expression on B cells and discontinued IVIG replacement. Our study shows that HSCT is potentially effective at curing the disease.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others


References
Ferrari S, Giliani S, Insalaco A, Al-Ghonaium A, Soresina A, Loubser M, et al. Mutations of CD40 gene cause an autosomal recessive form of immunodeficiency with hyper-IgM. Proc Natl Acad Sci USA. 2001;98:12614–19.
Lougaris V, Badolato R, Ferrari S, Plebani A. Hyper immunoglobulin M syndrome due to CD 40 deficiency: clinical, molecular, and immunological features. Immunol Rev. 2005;203:48–66.
Al-Saud BK, Al-Sum Z, Alassiri H, Al-Ghonaium A, Al-Muhsen S, Al-Dhekri H, Arnaout R, et al. Clinical, immunological, and molecular characterization of hyper-IgM syndrome due to CD40 deficiency in eleven patients. J Clin Immunol. 2013;33:1325–35.
Kutukculer N, Aksoylar S, Kansoy S, Cetingul N, Notarangelo LD. Outcome of hematopoietic stem cell transplantation in hyper-IgM syndrome caused by CD40 deficiency. J Pediatr. 2003;143:141–42.
Mazzolari E, Lanzi G, Forino C, Lanfranchi A, Aksu G, Ozturk C, et al. First successful stem cell transplantation in a child with CD40 deficiency. Bone Marrow Transplant. 2007;40:279–81.
Al-Dhekri H, Al-Zum Z, Al-Saud B, Ayas M, Al-Muhsen S, Arnaout R, et al. Successful outcome in two patients with CD40 deficiency treated with allogeneic HCST. Clin Immunol. 2012;143:96–8.
Leven EA, Maffucci P, Ochs HD, Scholl PR, Buckley RH, Fuleihan RL, et al. Hyper IgM syndrome: a report from the USIDNET registry. J Clin Immunol. 2016;36:490–501.
Gathmann B, Grimbacher B, Beauté J, Dudoit Y, Mahlaoui N, Fischer A, et al. The European internet-based patient and research database for primary immunodeficiencies: results 2006–8. Clin Exp Immunol. 2009;157(Suppl 1):3–11.
Fontana S, Moratto D, Mangal S, De Francesco M, Vermi W, Ferrari S, et al. Functional defects of dendritic cells in patients with CD40 deficiency. Blood. 2003;102:4099–106.
Kutukculer N, Moratto D, Aydinok Y, Lougaris V, Aksoylar S, Plebani A, et al. Disseminated cryptosporidium infection in an infant with hyper-IgM syndrome caused by CD40 deficiency. J Pediatr. 2003;142:194–6.
Karaca N, Forveille M, Aksu G, Durandy G, Kutukculer N. Hyper-immunoglobulin M syndrome type 3 with normal CD40 cell surface expression. Scand J Immunol. 2012;76:21–5.
Mishra A, Italia K, Gupta M, Desai M, Madkaikar M. Hyperimmunoglobulin syndrome due to CD40 deficiency: possibly the first case from India. J Postgrad Med. 2015;61:46–8.
O’Gorman MR, Zaas D, Paniagua M, Corrochano V, Scholl PR, Pachman LM. Development of a rapid whole blood flow cytometry procedure for the diagnosis of X-linked hyper-IgM syndrome. Clin Immunol Immunopathol. 1997;85:172–81.
Qamar N, Fuleihan RL. The hyper IgM syndromes. Clin Rev Allergy Immunol. 2014;46:120–30.
Levy J, Espanol-Boren T, Thomas C, Fischer A, Tovo P, Bordigoni P, et al. Clinical spectrum of X-linked Hyper-IgM syndrome. J Pediatr. 1997;131:47–54.
de la Morena MT, Leonard D, Torgerson TR, Cabral-Marques O, Slatter M, Aghamohammadi A, et al. Long-term outcomes of 176 patients with X-linked hyper-IgM syndrome treated with or without hematopoietic cell transplantation. J Allergy Clin Immunol. 2017;139:1282–92.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Al-Saud, B., Al-Jomaie, M., Al-Ghonaium, A. et al. Haematopoietic stem cell transplant for hyper-IgM syndrome due to CD40 defects: a single-centre experience. Bone Marrow Transplant 54, 63–67 (2019). https://doi.org/10.1038/s41409-018-0219-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41409-018-0219-0
This article is cited by
-
Compound Heterozygosity in Hyper‑IgM Syndrome Type 3: Case Report and Literature Review
Journal of Clinical Immunology (2024)
-
Clinical and Immunological Features, Genetic Variants, and Outcomes of Patients with CD40 Deficiency
Journal of Clinical Immunology (2024)
-
Cyclophosphamide
Reactions Weekly (2019)
