
Abstract
Background
Currently, several therapies are available for metastatic castration-resistant prostate cancer (mCRPC) but no specific clinical factors to personalize treatment. We first sought the prognostic value of duration on androgen-deprivation therapy (ADT) for hormone-sensitive prostate cancer (HSPC) in patients receiving androgen-receptor-signaling inhibitors (ARSI) for mCRPC.
Methods
A multicenter cohort of mCRPC patients who started ARSI between July 2011 and October 2021 was identified. Based on their initial disease burden and duration on ADT for HSPC, primary progressive (PP) men were classified into four groups: low/intermediate-risk localized disease (LOC) and high-risk localized/locally advanced disease (LAD) and short-term (ST) < 24 vs. long-term (LT) ADT ≥ 24 months, whereas de novo (DN) mHSPC were subdivided into short-time vs. long-time to CRPC.
Results
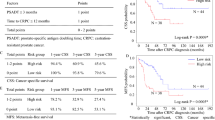
We included 919 mCRPC patients with a median age of 77 years [interquartile range (IQR) = 71–82)]. Median ADT duration in HSPC was 24 months (IQR = 14–40). Median follow-up was 91 months (IQR = 62–138), median OS and PFS from ARSI start were 20 (IQR 10–32) and 10 months (IQR = 5–19), respectively. In PP developing metastatic disease (n = 655, 71.3%), LOC and LAD with ST ADT had a greater than almost double-risk of death compared to LT ADT (LOC/ST: hazard ratio [HR] = 2.01; 95% CI 1.54–2.64; LAD/ST: HR = 1.73; 95% CI 1.34–2.24; p < 0.001). In the multivariate analysis including age, prognostic cohort, Gleason, ECOG, radical radiotherapy and prostatectomy, groups with ST ADT were associated with worse OS compared to LT ADT (LOC/ST: HR = 1.84; 95% CI 1.38–2.45; p < 0.001; LAD/ST: HR = 1.59; 95% CI 1.21–2.10; p < 0.001), along with ECOG > 2 (HR = 1.55; 95% CI 1.06–2.26; p = 0.03). There were also similar results of PFS. Moreover, long-time to CRPC in patients with history of DN mHSPC (n = 264, 28.7%) resulted in a better OS/PFS (HR = 0.76, 95% CI 0.56–1.02, p = 0.064 and HR = 0.74, 95% CI 0.55–0.99, p = 0.042, respectively).
Conclusions
Our study showed that duration on ADT for mHSPC was significantly associated with survival in mCRPC undergoing ARSI. These findings suggest a possible connection between initial management of prostate tumour and a better prognostication in mCRPC. Prospective trials are warranted.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 4 print issues and online access
$259.00 per year
only $64.75 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others


Data availability
The anonymized datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–49.
D’Amico AV, Whittington R, Malkowicz SB, Schultz D, Blank K, Broderick GA, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA. 1998;280:969–74.
Parker C, Castro E, Fizazi K, Heidenreich A, Ost P, Procopio G, et al. Prostate cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31:1119–34.
Davies A, Conteduca V, Zoubeidi A, Beltran H. Biological evolution of castration-resistant prostate cancer. Eur Urol Focus. 2019;5:147–54.
Ryan CJ, Smith MR, de Bono JS, Molina A, Logothetis CJ, de Souza P, et al. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med. 2013;368:138–48.
Beer TM, Armstrong AJ, Rathkopf DE, Loriot Y, Sternberg CN, Higano CS, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. 2014;371:424–33.
D’Amico AV, Chen M-H, Crook J, Armstrong JG, Malone S, Steigler A, et al. Duration of short-course androgen suppression therapy and the risk of death as a result of prostate cancer. J Clin Oncol. 2011;29:4682–7.
Gillessen S, Bossi A, Davis ID, de Bono J, Fizazi K, James ND, et al. Management of patients with advanced prostate cancer. Part I: intermediate-/high-risk and locally advanced disease, biochemical relapse, and side effects of hormonal treatment: report of the Advanced Prostate Cancer Consensus Conference 2022. Eur Urol. 2023;83:267–93.
Mottet N, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M, et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer—2020 update. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2021;79:243–62.
Sweeney CJ, Chen YH, Carducci M, Liu G, Jarrard DF, Eisenberger M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N Engl J Med. 2015;373:737–46.
Nuzzo PV, Ravera F, Saieva C, Zanardi E, Fotia G, Malgeri A, et al. Clinical outcomes of volume of disease on patients receiving enzalutamide versus abiraterone acetate plus prednisone as first-line therapy for metastatic castration-resistant prostate cancer. Ther Adv Med Oncol. 2023;15:17588359231156147.
Nuzzo PV, Pederzoli F, Saieva C, Zanardi E, Fotia G, Malgeri A, et al. Clinical impact of volume of disease and time of metastatic disease presentation on patients receiving enzalutamide or abiraterone acetate plus prednisone as first-line therapy for metastatic castration-resistant prostate cancer. J Transl Med. 2023;21:75.
Fizazi K, Gillessen S, ESMO Guidelines Committee. Updated treatment recommendations for prostate cancer from the ESMO Clinical Practice Guideline considering treatment intensification and use of novel systemic agents. Ann Oncol. 2023;34:557–63.
Watson PA, Arora VK, Sawyers CL. Emerging mechanisms of resistance to androgen receptor inhibitors in prostate cancer. Nat Rev Cancer. 2015;15:701–11.
Antonarakis ES, Lu C, Wang H, Luber B, Nakazawa M, Roeser JC, et al. AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. N Engl J Med. 2014;371:1028–38.
Conteduca V, Wetterskog D, Sharabiani MTA, Grande E, Fernandez-Perez MP, Jayaram A, et al. Androgen receptor gene status in plasma DNA associates with worse outcome on enzalutamide or abiraterone for castration-resistant prostate cancer: a multi-institution correlative biomarker study. Ann Oncol. 2017;28:1508–16.
Mu P, Zhang Z, Benelli M, Karthaus WR, Hoover E, Chen CC, et al. SOX2 promotes lineage plasticity and antiandrogen resistance in TP53- and RB1-deficient prostate cancer. Science. 2017;355:84–8.
Ku SY, Rosario S, Wang Y, Mu P, Seshadri M, Goodrich ZW, et al. Rb1 and Trp53 cooperate to suppress prostate cancer lineage plasticity, metastasis, and antiandrogen resistance. Science. 2017;355:78–83.
Conteduca V, Mosca A, Brighi N, de Giorgi U, Rescigno P. New prognostic biomarkers in metastatic castration-resistant prostate cancer. Cells. 2021;10:193.
Pradat Y, Viot J, Yurchenko AA, Gunbin K, Cerbone L, Deloger M, et al. Integrative pan-cancer genomic and transcriptomic analyses of refractory metastatic cancer. Cancer Discov. 2023;13:1116–43.
Conteduca V, Crabb SJ, Jones RJ, Caffo O, Elliott T, Scarpi E, et al. Persistent neutrophil to lymphocyte ratio >3 during treatment with enzalutamide and clinical outcome in patients with castration-resistant prostate cancer. PLoS ONE. 2016;11:e0158952.
Cursano MC, Conteduca V, Scarpi E, Gurioli G, Casadei C, Gargiulo S, et al. Grade group system and plasma androgen receptor status in the first line treatment for metastatic castration resistant prostate cancer. Sci Rep. 2022;12:7319.
Conteduca V, Casadei C, Scarpi E, Brighi N, Schepisi G, Lolli C, et al. Baseline plasma tumor DNA (ctDNA) correlates with PSA kinetics in metastatic castration-resistant prostate cancer (mCRPC) treated with abiraterone or enzalutamide. Cancers. 2022;14:2219.
van Soest RJ, de Morrée ES, Kweldam CF, de Ridder CMA, Wiemer EAC, Mathijssen RHJ, et al. Targeting the androgen receptor confers in vivo cross-resistance between enzalutamide and docetaxel, but not cabazitaxel, in castration-resistant prostate cancer. Eur Urol. 2015;67:981–5.
Scher HI, Morris MJ, Stadler WM, Higano C, Basch E, Fizazi K, et al. Trial design and objectives for castration-resistant prostate cancer: updated recommendations from the prostate cancer clinical trials working group 3. J Clin Oncol. 2016;34:1402–18.
Bolla M, de Reijke TM, Van Tienhoven G, Van den Bergh AC, Oddens J, Poortmans PM, et al. Duration of androgen suppression in the treatment of prostate cancer. N Engl J Med. 2009;360:2516–27.
Nabid A, Carrier N, Martin AG, Bahary JP, Lemaire C, Vass S, et al. Duration of androgen deprivation therapy in high-risk prostate cancer: a randomized phase III trial. Eur Urol. 2018;74:432–41.
Horwitz EM, Bae K, Hanks GE, Porter A, Grignon DJ, Brereton HD, et al. Ten-year follow-up of radiation therapy oncology group protocol 92-02: a phase III trial of the duration of elective androgen deprivation in locally advanced prostate cancer. J Clin Oncol. 2008;26:2497–504.
Schmidt-Hegemann NS, Zamboglou C, Mason M, Mottet N, Hinnen K, De Meerleer G, et al. ESTRO-ACROP recommendations for evidence-based use of androgen deprivation therapy in combination with external-beam radiotherapy in prostate cancer. Radiother Oncol. 2023;183:109544.
Attard G, Murphy L, Clarke NW, Cross W, Jones RJ, Parker CC, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: a meta-analysis of primary results from two randomised controlled phase 3 trials of the STAMPEDE platform protocol. Lancet. 2022;399:447–60.
Shore ND, de Almeida Luz M, De Giorgi U, Gleave M, Gotto GT, Haas GP, et al. LBA02-09 EMBARK: a phase 3 randomized study of enzalutamide or placebo plus leuprolide acetate and enzalutamide monotherapy in high-risk biochemically recurrent prostate cancer. J Urol. 2023;209:e1190.
Loriot Y, Eymard JC, Patrikidou A, Ileana E, Massard C, Albiges L, et al. Prior long response to androgen deprivation predicts response to next-generation androgen receptor axis targeted drugs in castration resistant prostate cancer. Eur J Cancer. 2015;51:1946–52.
Giacinti S, Carlini P, Roberto M, Bassanelli M, Strigari L, Pavese F, et al. Duration of response to first androgen deprivation therapy, time to castration resistance prostate cancer, and outcome of metastatic castration resistance prostate cancer patients treated with abiraterone acetate. Anticancer Drugs. 2017;28:110–5.
Halabi S, Yang Q, Roy A, Luo B, Araujo JC, Logothetis C, et al. External validation of a prognostic model of overall survival in men with chemotherapy-naïve metastatic castration-resistant prostate cancer. J Clin Oncol. 2023;41:2736–46.
Coquet J, Bievre N, Billaut V, Seneviratne M, Magnani CJ, Bozkurt S, et al. Assessment of a clinical trial-derived survival model in patients with metastatic castration-resistant prostate cancer. JAMA Netw Open. 2021;4:e2031730.
Lowentritt BH, Rossi C, Du S, Muser E, Kinkead F, Waters D, et al. Real-world time-to-castration resistance (CR) among patients (pts) with metastatic castration-sensitive prostate cancer (mCSPC) initiating apalutamide (APA), enzalutamide (ENZ), or abiraterone acetate (ABI) from an oncology database. J Clin Oncol. 2023;41:65–65.
Funding
This research was supported by ‘PRA-HE (Progetti di Ricerca di Ateneo propeudetici all’accesso ai finanziamenti del programma Horizon Europe) 2021’ to VC and ‘PNRR - M4C2-I1.3 Project PE_00000019 “HEAL ITALIA”, ‘5 per mille 2018-2019 LILT Investigator Grant’, ‘Ministry of University and Research (PRIN – PROGETTI DI RICERCA DI RILEVANTE INTERESSE NAZIONALE – Università degli Studi di Foggia – CUP D53D23014290006) and ‘Iniziativa regionale “RIPARTI: assegni di RIcerca per riPARTire con le Imprese” – CUP D74C22000040002’ to ML.
Author information
Authors and Affiliations
Contributions
VC conceptualized, designed and wrote the study. VC, PDT, RA, GB, CL, GS, GG, MG, VEC, LC, EZ, LG, FM, UF, PR, GF, FS, DS, GP, OC, and GC involved in acquisition of data. VC and AR analyzed and interpreted the data. ML and UDG revised the manuscript.
Corresponding author
Ethics declarations
Competing interests
VC has served as a consultant/advisory board member for Janssen, Astellas, Merck, AstraZeneca, Amgen, EISAI, Recordati, Novartis, Ipsen and Bayer and has received speaker honoraria or travel support from Astellas, Janssen, Ipsen, Bayer, Gilead and Bristol Myers Squibb. PR served as an advisory board for MSD and AstraZeneca Italy. FM has received research support and/or honoraria from Astellas, BMS, Janssen, Ipsen, MSD and Pfizer. GF served as an advisory board member for Astellas, Janssen, Pfizer, Bayer, MSD, Merck and received travel accommodation from Astellas, Janssen, Bayer. GP served as a consultant and/or a speaker for Bayer, BMS, Novartis, Amgen, Pfizer, Janssen, Ipsen, Boehringer. OC served as an advisory/board member of AAA, AstraZeneca, Astellas, Bayer, Janssen, Ipsen, MSD, Pfizer, and has received speaker honoraria from Ipsen, MSD, AstraZeneca, Astellas, Janssen. UDG served as an advisory/board member of Astellas, Bayer, BMS, IPSEN, Janssen, Merck, Pfizer, Sanofi, received research grant/funding to the institution from AstraZeneca, Roche, Sanofi and travel/accommodations/expenses from BMS, IPSEN, Janssen, Pfizer. No potential conflicts of interest were disclosed by the other authors.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Conteduca, V., Di Tullio, P., Allamprese, R. et al. Initial management approach for localized/locally advanced disease is critical to guide metastatic castration-resistant prostate cancer care. Prostate Cancer Prostatic Dis (2024). https://doi.org/10.1038/s41391-024-00800-8
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41391-024-00800-8
This article is cited by
-
Prostatectomy in oligometastatic prostate cancer: a call for high-quality evidence
Prostate Cancer and Prostatic Diseases (2024)
