
Abstract
Introduction
Studies linked obesity with a large number of medical conditions including decreased cognitive functioning. The relation between BMI and cognition was proven in adults, but in adolescents the results are conflicting. Further, limited data are available on the impact of weight loss on cognition. This study analyzed the impact of a 30-week lasting weight loss program on cognition and determined the impact of changes in body composition and self-perceived fatigue on changes in cognition.
Methods
Sixty-two obese adolescents were evaluated at baseline and after 30 weeks. Stroop test (ST; selective attention), Continuous Performance Test (CPT; sustained attention) and Ray Auditory verbal learning test (RAVLT; short-term memory) were assessed. Additionally, body composition parameters and fatigue (MFI-20) were evaluated.
Results
Improved reaction times were found for ST and CPT after the intervention, but were independent for reductions in BMI, fat mass, fat%, and fatigue. Short memory also improved with decreased fatigue as an influencing parameter. Accuracy of ST and CPT showed no significant changes.
Conclusion
A 30-week lasting inpatient weight loss program improved selective attention, sustained attention, and short-term memory. Changes in body composition did not explain the improvements in cognitive functioning. Decreased fatigue resulted in improved aspects of cognition.
Similar content being viewed by others

Introduction
Obesity, defined as an excess accumulation of fat mass, is a well known world-wide problem due to increased sedentary behavior and unhealthy eating habits. An imbalance in caloric intake and expenditure is very often the reason for fat accumulation. The World Health Organization uses BMI cutoffs of 25 and 30 kg/m2 to define respectively overweight and obesity, in children and adolescents the use of age- and sex-specific cutoffs are mandatory.1 In Flanders, 5% of the children and adolescents, both boys and girls, between 2 and 17 years are obese.2
The consequences of being obese can be dramatic, it is not only linked with physiological problems such as increased heart problems, arterial hypertension, diabetics, CVA, and cancer,3 but also with the increased psychological disorders such as depression, decreased quality of life, and increased self-perceived fatigue (SpF).4,5 Additionally, adult obesity is also related to the decreased cognitive function6 and structural brain differences.7 These correlations were also found in adolescents, even when correcting for socio-economic factors, blood pressure, and serum lipid profile.8 Adolescents with increased BMI-z scores scored poor on the Stroop task9 and had increased reaction times on the Continuous Performance Test (CPT)10 compared to normal weight peers. Further, obese subjects with increased uncontrolled eating behavior scored worse on inhibitory control and working memory.10 A literature review provided evidence that diet and exercise interact with cognition, neuroplasticity, and mood in adults, but in children and adolescents the evidence remains ambiguous.11,12,13
This study incorporated the Stroop task test (response inhibition), the CPT (sustained attention), and the Rey Auditory Verbal learning test (RAVLT) (short-term memory) to assess the different aspects of cognition. With the chosen tests, the effectivity of the provided weight loss program on cognitive functioning in obese adolescents was investigated. Additionally, the impact of body composition and SpF on cognitive functions was evaluated.
Methods
Recruitment and participants
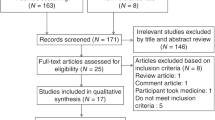
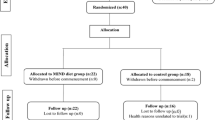
All obese adolescents (BMI 40.0 ± 8.4) between 12 and 18 years of age (mean age 15.8 ± 1.8), who started a weight loss program at the Zeepreventorium (De Haan, Belgium), a specialized residential center for obese children in Belgium, were invited to participate. At baseline, 62 subjects (18 boys, 44 girls) were included. After the 30-week lasting multi-dimensional weight loss program, 48 subjects (12 boys, 36 girls) were willing to be reassessed (23% dropout rate). A control group of 30 normal weight1 (mean age 16.0 ± 1.1) sportive adolescents (16 boys, 14 girls) at Koninklijk Atheneum Etterbeek (Brussels, Belgium) were assessed in the same period of obese baseline measures. The parents of all participating minors provided written informed consent. The study was approved by the Academic Ethical committee of the Brussels Alliance for Research and Higher Education (IRB B200-2016-072).
Multi-disciplinary obesity treatment program
Physical activity
Obese adolescents received an individualized and monitored exercise program consisting of fitness exercises (strength and endurance), physiotherapy (psychomotor training), and swimming. Every 2 months the exercise program was adapted according to the participants’ progression. During the first 2 months, two exercise moments per week were implemented, consisting of physiotherapy (combination of psychomotor and aerobic training) and swimming. The next 4 months, three training sessions per week were provided consisting of fitness exercises (initiation level), physiotherapy, and swimming.
Diet
Depending on the age and sex, individual energy intake was determined, ranging between 1450 and 2690 kcal per day consisting of 23% protein, 51% carbohydrate, and 26% fat. The participants were encouraged to consume six meals a day: breakfast, healthy morning snack, lunch, healthy afternoon snack, dinner, and healthy evening snack. The healthy snacks were fruit or low-fat dairy products.
Measures
Anthropometric and body composition measures
Standing height was measured with a stadiometer (Seca 217, SECA, Hamburg, Germany) to the nearest 0.1 cm. Body weight as well as body composition (fat mass, fat percentage, fat-free mass, and muscle mass) were determined with a class III Bioelectrical Impedance Analysis device, Tanita MC780MAS, to the nearest 0.1 kg (Tanita, Tokyo, Japan) following a standardized protocol.14 Between the knees, an isolating panel was placed to avoid shortcuts through touching knees. BMI was calculated as weight/height2 (kg/m2)
Self-perceived fatigue
SpF was assessed using the Dutch15 version of the Multidimensional Fatigue Inventory (MFI-20). The MFI-20 covers five domains of fatigue: general fatigue, physical fatigue, mental fatigue, reduced motivation, and reduced activities. Each subscale includes four items with five-point categories, resulting in a subscale score range of 4–20, with higher scores indicating greater fatigue. Also, a total MFI score (score range from 20 to 100) was calculated by summing up the scores of the five subscales. Internal consistency of the total MFI-20 score for this population was measured by Cronbach’s α, α=0.87 which indicates a good internal consistency.16
Cognitive tasks
Rey Auditory Verbal learning test
The Dutch (native language spoken by the participants) version of the RAVLT was used to assess short-term memory.17 Fifteen words were five times read aloud by a trained staff member. Participants were each time asked to recall as many words as possible. After 20 min, at the end of the test battery, participants were asked to recall as many words as possible and to recognize the words within a list of 30 words. The sum of recalled words of the five first trials, the amount of recalled words of the recall session, and the amount of correctly and incorrectly recognized words during the recognition trial were used as outcome measures.
Stroop task test
E-prime 2.0 software was used to program and execute the Stroop task test (Psychology Software Tools, Inc., Pittsburg, PA).18 This test was used to assess selective attention and response inhibition.19 Three parts were incorporated in this test:20 (I) A simple reaction time test. (II) The words yellow, red, blue, and green were shown in matching colors (congruent condition) and non-matching colors (incongruent condition). Subjects responded by pushing the button corresponding to the color in which the words were displayed. (III) The words yellow, red, blue, and green were again shown in congruent and incongruent conditions. This time the subjects responded by pushing the button matching to the word displayed on the screen. The three parts were separated by a 30-s rest period. Outcome measures were accuracy (%) and reaction time (ms).
Rosvold CPT
E-prime 2.0 software was used to program and execute the Rosvold CPT.18 During a 7-min period, sustained attention was measured. Brief description of the test, letters were presented every 1000 ms, when an ‘X’ appeared on the screen the subjects were asked to push the space bar.
Data analysis
Data were analyzed using SPSS 24.0 for mac (SPSS, Chicago,IL). Descriptives for age, weight, length, BMI, body fat, self-perceived fatigue, Stroop test (accuracy and reaction time), RAVLT (total score, recall and recognition) and CPT (accuracy and reaction time) are displayed as mean ± SD. To determine normality of the data, one-sample Kolmogorov–Smirnov test was used. Differences between baseline measures and the control group were assessed by independent samples t-test or Mann–Whitney U for respectively parametric and non-parametric data. Data obtained after the intervention were compared with baseline measures using paired sample t-test for all parametrical data and the Wilcoxon test for non-parametrical data. Effect size for each group:1 baseline obese group vs normal weight peers (O vs NW) and2 baseline obese subjects vs post-intervention obese subjects (intervention) was calculated using the absolute values of Cohen’s d (Cohen’s d = (mean2 − mean1)⁄SDpooled; SDpooled = √(((N1 − 1) × SD12 + (N2 − 1) × SD22) ⁄ (N1 + N2) − 2)).
The impact of cognitive functions on decreased fat outcomes was assessed using multiple linear regression stepwise method. Reductions in fat mass and fat percentage were used as dependent variables, cognitive outcomes along with age and sex (male is the neutral sex) as independent variables. Model performance fit was assessed using multiple correlation (R2). Longitudinal data analyses were performed using repeated measures mixed models to evaluate changes in cognitive functions from baseline and post intervention adjusting for changes in body composition parameters and SpF.
Results
At baseline, the obese group (15.8 ± 1.8 years) had similar age as the control group (16.0 ± 1.1 years) and comparable length (Table 1). Anthropometric measures were significantly higher (all p < 0.001) in obese subjects at baseline even as total SpF (p < 0.01) compared to the control group. Post-intervention values in obese subjects improved all significantly for anthropometric measures and SpF (Table. 1). Cohen’s d of obese vs normal weight peers (O vs NW) were all higher compared to intervention (Table 1).
Cognition
Normal weight adolescents had enhanced reaction times (RT) and accuracy scores on CPT compared to obese subjects (both p < 0.001; Table 2). After the weight loss intervention, obese subjects improved RT (p < 0.001) and a trend to improved accuracy (p = 0.056) was found (Table 2). Cohen’s d for accuracy and RT in O vs NW were respectively 0.71 and 1.00, whereas Cohen’s d for accuracy and RT of the intervention were respectively 0.18 and 0.28 (Table 2).
Total and recall scores of the RAVLT improved significantly (respectively p < 0.01 and p < 0.001), and a trend to significance for recognition (p = 0.06) was noticed after the intervention. Cohen’s d was calculated for intervention total score, recall, and recognition (respectively 0.43, 0.5, and 0.22) (Table 2). No significant differences were found between baseline obesity measures and the control group.
Stroop task test reaction times of normal weight adolescents and post intervention were all significantly higher compared to baseline obese values (Table 3). Cohen’s ds of O vs NW were all higher compared to intervention Cohen’s d (Table 3).
Accuracy of the Stroop task decreased significantly for the simple stimulus (p < 0.05) after completing the intervention and was increased for word incongruent stimuli in normal weight adolescents compared to the obese group (Table 4) other stimuli were not significantly different with baseline measures of the obese subjects.
Reaction time of the continuous performance test along with sex and age were selected to estimate the decrease in fat percentage (F3,47 = 9.410, p < 0.0001, R2 = 0.35).
Decrease in fat% = −39.11 (constant) − 4.25 × sex + 1.12 × age + 0.03 × reaction time CPT
Interaction effects
Repeated measures ANOVA (mixed model) with calculated differences in fat mass, fat percentage, BMI, and self-perceived fatigue as covariates revealed limited evidence of interaction with sustained attention and response inhibition. Increased accuracy in Stroop task, modality “color congruent”, was associated with decreased SpF (F1,42 = 4.424; p < 0.05). A trend to significance (F1,42 = 3.078; p = 0.08) was found for the influence of reduced fat mass on improvements reaction time for the Stroop task modality “word congruent”. Changed accuracy or reaction time in CPT could not be explained by changes in fat mass, fat percentage, BMI nor by SpF. Improved short-term memory, measured by means of RAVLT, was significantly influenced by decreased SpF (F1,41 = 5.534; p = 0.02), RAVLT was not influenced by changes in anthropometric measures.
Discussion
The general idea of weight loss programs is losing body weight and body fat in particular. Fat was already linked with increased health problems in adults and adolescents as described in the introduction. Current study examined the impact of a weight loss program on cognition and explored the importance of reduced anthropometric measures and SpF on changes in cognitive functions in obese adolescents.
The effectivity of the program was proved by the strong significant reductions in body weight, BMI, fat mass, and fat percentage after the weight loss program. Moreover, enhanced responds inhibition, sustained attention, and short-term memory were found after this 30-week lasting multi-disciplinary weight loss program. Improved reaction times were obtained for all modalities of the Stroop task test (response inhibition) and CPT (sustained attention). Similar improved reaction times were found by Delgado-Rico and colleagues in obese adolescents for cognitive inhibition after a 12-week multi-component intervention.21 Accuracy, a second parameter beside reaction time, did not change. The high accuracy scores between 88 and 98% are possibly an explanation for this status quo. Similar unchanged accuracy results were found in adolescents following a physical activity program.18 Beside reduced reaction times for Stroop task and CPT, improved results on the RAVLT (short-term memory) were acquired. Even though significant improvements on all the cognitive tasks were found after the intervention, comparison with the healthy, physically active control group revealed that further improvements are still possible, for this a continuous effort is necessary.
This study has found that beside a positive impact of the intervention program on cognitive parameters, enhanced cognitive functions at baseline resulted in higher fat loss, along with younger age and male sex. Pauli and colleagues linked impulsivity and inattention to higher BMI in obese children and pointed out to the importance of impulsivity regulation to improve weight reductions at younger age,22 but the effect was not verified after an intervention. Additionally, increased impulsivity in young girls resulted in a less beneficial weight outcome.23 In previous studies,22,23 BMI was used to evaluate the intervention outcome instead of fat measures. Because BMI is a (weight/length2) ratio, it does not evaluate fatness and can give wrong indications.
Finally, this study aimed to determine whether improvements in cognition were attributed to changes in body composition parameters or SpF. No proof was found that changes in fat, weight, or BMI were responsible for increased cognitive functions. Presented data suggest that decreased SpF was responsible for improved aspects of cognition such as short-term memory and response inhibition. In contrast, Delgado-Rico and colleagues attributed greater loss in BMI to improved response inhibition21 and proved that reduced inhibitory control resulted in greater BMI loss.24 Different baseline BMI measures between the studies and a steeper BMI decrease in current study are plausible determining factors for contradicting outcomes. Studies have demonstrated that exercise, an adapted diet, or the benevolent effect of the combination of both, enhanced cognition.13,18,25 Because no objective data of food intake and physical activity were available at the Zeepreventorium before and during the intervention, we hypothesized that changes in lifestyle due to a multidimensional weight loss program were of importance for improved cognition. Previous research linked increased physical activity and decreased body fat already with reduced SpF,16 but the effect on cognition needs to be clarified in future research.
Current study revealed novel insights concerning the impact of a multi-dimensional weight loss program on cognition and the interaction between SpF and aspects of cognition.
The strength of this study was the use of absolute fat measures to evaluate progress instead of BMI. Second strength is the link between decreased SpF and improved cognitive outcomes. A possible limitation of this study is the use of the Multi-dimensional Fatigue Inventory developed by Smets and colleagues.15 This questionnaire is not yet validated in adolescents although promising properties were already found, such as a high internal consistency and the possibility to discriminations levels of SpF based on body composition.16 To fully understand the influence of the multi-dimensional weight loss program on cognitive functions, objective physical activity and nutritional data are warrant to reveal new insights in the interaction with cognition.
Conclusion
This study also found, beside positive changes in body composition, cognitive improvement and decreased self-perceived fatigue in obese adolescents who participated in a 30-week inpatient weight loss program. Greater fat mass loss in obese adolescents was associated with improved cognitive functions, lower age and male sex. Further, this is the first study that attributes decreased SpF to improved aspects of cognition after a weight loss program in obese adolescents.
References
Cole, T. J., Bellizzi, M. C., Flegal, K. M. & Dietz, W. H. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 320, 1240–1243 (2000).
Drieskens, S. Gezondheidsenquete 2013. Wetenschappelijk Instituut Volksgezondheid, Surveillance ODVe; 2014. Report No.: PHS Report 2014-47 Contract No.: D/2014/2505/69.
Neilson, A. & Schneider, H. Obesity and its comorbidities: present and future importance on health status in Switzerland. Soz. Prav. 50, 78–86 (2005).
Morrison, K. M., Shin, S., Tarnopolsky, M. & Taylor, V. H. Association of depression & health related quality of life with body composition in children and youth with obesity. J. Affect Disord. 172C, 18–23 (2014).
Varni, J. W., Limbers, C. A., Bryant, W. P. & Wilson, D. P. The PedsQL multidimensional fatigue scale in pediatric obesity: feasibility, reliability and validity. Int J. Pediatr. Obes. 5, 34–42 (2010).
Smith, E., Hay, P., Campbell, L. & Trollor, J. N. A review of the association between obesity and cognitive function across the lifespan: implications for novel approaches to prevention and treatment. Obes. Rev. 12, 740–755 (2011).
Pannacciulli, N. et al. Brain abnormalities in human obesity: a voxel-based morphometric study. Neuroimage 31, 1419–1425 (2006).
Li, Y. F., Dai, Q., Jackson, J. C. & Zhang, J. Overweight is associated with decreased cognitive functioning among school-age children and adolescents. Obesity 16, 1809–1815 (2008).
Cao, H. et al. [Study on the Stroop task test in adolescents with different degrees of obesity before and after mental workload]. Wei Sheng Yan Jiu. 41, 566–570 (2012).
Calvo, D., Galioto, R., Gunstad, J. & Spitznagel, M. B. Uncontrolled eating is associated with reduced executive functioning. Clin. Obes. 4, 172–179 (2014).
Leigh Gibson, E. & Green, M. W. Nutritional influences on cognitive function: mechanisms of susceptibility. Nutr. Res Rev. 15, 169–206 (2002).
Green, M. W., Elliman, N. A. & Rogers, P. J. Lack of effect of short-term fasting on cognitive function. J. Psychiatr. Res. 29, 245–253 (1995).
Gomez-Pinilla, F. & Tyagi, E. Diet and cognition: interplay between cell metabolism and neuronal plasticity. Curr. Opin. Clin. Nutr. Metab. Care. 16, 726–733 (2013).
Wan, C. S. et al. Bioelectrical impedance analysis to estimate body composition, and change in adiposity, in overweight and obese adolescents: comparison with dual-energy X-ray absorptiometry. BMC Pediatr. 14, 249 (2014).
Smets, E. M. A., Garssen, B., Bonke, B. & Dehaes, J. C. J. M. The Multidimensional Fatigue Inventory (Mfi) psychometric qualities of an instrument to assess fatigue. J. Psychosom. Res. 39, 315–325 (1995).
Vantieghem, S., Bautmans, I., Tresignie, J. & Provyn, S. Self-perceived fatigue in adolescents in relation to body composition and physical outcomes. Pediatr Res. 83, 2017.
Larson, M. J. et al. Cognitive and typing outcomes measured simultaneously with slow treadmill walking or sitting: implications for treadmill desks. PLoS ONE 10, e0121309 (2015).
Torbeyns, T. et al. Cycling on a bike desk positively influences cognitive performance. PLoS ONE 11, e0165510 (2016).
Gualtieri, C. T. & Johnson, L. G. Reliability and validity of a computerized neurocognitive test battery, CNS Vital Signs. Arch. Clin. Neuropsychol. 21, 623–643 (2006).
Alderman, B. L., Olson, R. L. & Mattina, D. M. Cognitive function during low-intensity walking: a test of the treadmill workstation. J. Phys. Act. Health 11, 752–758 (2014).
Delgado-Rico, E. et al. Effects of a multicomponent behavioral intervention on impulsivity and cognitive deficits in adolescents with excess weight. Behav. Pharmacol. 23, 609–615 (2012).
Pauli-Pott, U., Albayrak, O., Hebebrand, J. & Pott, W. Association between inhibitory control capacity and body weight in overweight and obese children and adolescents: dependence on age and inhibitory control component. Child Neuropsychol. 16, 592–603 (2010).
Nederkoorn, C., Jansen, E., Mulkens, S. & Jansen, A. Impulsivity predicts treatment outcome in obese children. Behav. Res Ther. 45, 1071–1075 (2007).
Kulendran, M. et al. Neuropsychological assessment as a predictor of weight loss in obese adolescents. Int. J. Obes. 38, 507–512 (2014).
Chang, Y. K., Labban, J. D., Gapin, J. I. & Etnier, J. L. The effects of acute exercise on cognitive performance: a meta-analysis. Brain Res. 1453, 87–101 (2012).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Vantieghem, S., Bautmans, I., Guchtenaere, A.D. et al. Improved cognitive functioning in obese adolescents after a 30-week inpatient weight loss program. Pediatr Res 84, 267–271 (2018). https://doi.org/10.1038/s41390-018-0047-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-018-0047-3
This article is cited by
-
Pediatric quality of life multidimensional fatigue scale (PedsQL-MFS) detects the effects of a 3-week Inpatient body weight reduction program for children and adolescents with obesity
Health and Quality of Life Outcomes (2022)
-
Obesity and Poststroke Fatigue: A 2-Year Longitudinal Study
Neurology and Therapy (2021)
