
Abstract
Background
Over the past 150 years, humans have become taller, and puberty has begun earlier. It is unclear if these changes are continuing in Sweden, and how longitudinal growth patterns are involved. We aimed to evaluate the underlying changes in growth patterns from birth to adulthood by QEPS estimates in two Swedish cohorts born in 1974 and 1990.
Methods
Growth characteristics of the longitudinal 1974 and 1990-birth cohorts (n = 4181) were compared using the QEPS model together with adult heights.
Results
There was more rapid fetal/infancy growth in girls/boys born in 1990 compared to 1974, as shown by a faster Etimescale and they were heavier at birth. The laterborn were taller also in childhood as shown by a higher Q-function. Girls born in 1990 had earlier and more pronounced growth during puberty than girls born in 1974. Individuals in the 1990 cohort attained greater adult heights than those in the 1974 cohort; 6 mm taller for females and 10 mm for males.
Conclusion
A positive change in adult height was attributed to more growth during childhood in both sexes and during puberty for girls. The QEPS model proved to be effective detecting small changes of growth patterns, between two longitudinal growth cohorts born only 16 years apart.
Similar content being viewed by others


Introduction
Growth pattern of human height is represented by different trajectories that run from birth until attained adult height. The pattern of growth is characterized by different periods of acceleration and deceleration, linked to certain periods of development, an evolutionary response to optimize the outcome for the growing human.1 The total growth in height can be divided into different phases; the rapid fetal growth before birth, the rapid, but also rapidly declining infancy growth period, the long linear period of childhood growth, and the pubertal growth spurt with initial acceleration and following deceleration until adult height is reached. Growth patterns differ between individuals, sexes and populations, and may also change with time,2,3 possibly related to plasticity in the transition of the different growth periods.4 Deviant growth patterns can be a signal of diseases or psychosocial problems.2,5 Different growth patterns are also associated with future health and disease in later life.4,6,7,8
Over the last 150 years, humans in affluent countries have become progressively taller and puberty has started earlier.9,10,11,12 Such secular changes in growth are likely to be consequences of improved nutrition, increasing weight and body mass index (BMI) in childhood, and the decline of serious infections during infancy/childhood.13,14 Positive secular trends in height have been found to be associated with improved health, as well as improved living standards and socioeconomic status.2,10 In recent decades, however, there is evidence that the progressive increase in height over time may be diminishing in Northern Europe.10 In the Netherlands, with the tallest known population, the increase in height is no longer apparent.15,16
When discussing secular trends in height at the population level, the observed trends may reflect both changes in a genetically stable population and changes in population demographics (owing to migration), or a combination of the two.9,17 An earlier cross-sectional comparison of two similarly obtained Swedish growth cohorts born in 1974 and 1990 (Grow Up 1974 and Grow Up 1990) showed an increase in attained height at 18 years in the later-born cohort.17 Previous research about secular changes has often been based on cross-sectional data without analyzing growth patterns.
Given the variety of ways to define and measure puberty, methodological differences are evident in studies of pubertal timing. There is a vast body of literature regarding age at menarche and the emergence of secondary sexual characteristics as markers of puberty.9 In contrast, studies regarding patterns of growth as markers of puberty are less common, and generally focus on peak height velocity (PHV) which only provides a measure of the midpoint of puberty.
For investigating the total growth patterns from birth to attained adult height together with the different growth phases, it is beneficial to have a growth model that can describe individual growth in height mathematically in a standardized way as a research tool.18,19 The ICP model was the first growth model that used three different mathematical functions, infancy– childhood– puberty, related to different growth phases.18 The recently developed QEPS model uses four growth functions: quadratic, exponential, puberty, and stop, where the combination of these functions, (T) total explains growth from fetal life to adult height (Fig. 1).19 Thanks to the specific pubertal growth function (P), it is possible to mathematically estimate the onset, middle, and end of pubertal growth, thus enabling a more detailed evaluation of growth during puberty than that which has been previously possible.20

The QEPS model. a The four mathematical functions of the QEPS model that are combined to describe total gain in height (T) from fetal life to adulthood: quadratic (Q), exponential (E), pubertal (P), and stop (S). B birth, marked with a vertical line. t0 about 6 weeks after conception. The QEPS model is fitted with six parameters. The three vertical arrows indicate the fitted individual height-scale parameters, from left to right Eheightscale, Qheightscale, and Pheightscale. The two horizontal arrows indicate the time-scale parameters, from left to right Etimescale and Ptimescale, and the sixth parameter is the location of mid-puberty, AgeP50, indicated with a dot. b Height (upper bold line) and height velocity (lower bold line) is shown for an individual male created by using the QEPS model, with pubertal growth estimates. AgeP5, representing the onset of pubertal growth, AgeP50 and AgeTPHV, representing mid-pubertal growth, and AgeP95, representing the end of pubertal growth are marked by vertical lines. Pmax, representing specific pubertal growth is shown both at the upper right on the height graph, and as the area under the curve (shaded) in the height velocity graph. TgainP5–95, total height gain during puberty due to combined Q- and P-function growth, is shown on the height graph. The duration of pubertal growth is shown with a horizontal bold line from AgeP5 to AgeP95
The aim of this study was to evaluate secular changes in growth patterns during growth phases from birth to adulthood, and the resulting adult heights in two Swedish cohorts born in 1974 and 1990, with use of growth functions from the QEPS model.
Methods
Study subjects
The study populations used, were selected subgroups from the Grow Up 1974 cohort21 and Grow Up 1990 cohort,22 including healthy individuals born at full term (gestational age, GA: 37−42 weeks) in Sweden, for whom information on longitudinal growth until adult height was available. Height and weight was measured at child healthcare centers and at school. A specially trained team measured the students in their 11th school year for Grow Up 1974 and in their 12th school year for Grow Up 1990. Height was measured to the nearest 0.1 cm using a calibrated Harpenden stadiometer. Adult height was ascertained following a height increase of <0.5 cm during the previous 12 months. Individuals who were still growing were followed with additional measurements by the study team until adult height was attained. A mathematical selection tool was used in both study cohorts to restrict the sample to those individuals with serial measurements at all age periods, together with visual growth curve analysis to select individuals with growth data of high quality.20,23
The 1974 study cohort included data from 2280 healthy individuals (1139 girls) born in Sweden (Supplemental Table S1). The 1990 study cohort included data from 1901 healthy individuals (929 girls) born in Sweden (Supplemental Table S1). Records of all babies delivered in Sweden in 1974 show that 6% were born to mothers from other Nordic countries, 3% were born to mothers from other European countries, and 1% were born to mothers from outside Europe.24 Corresponding records of all babies delivered in Sweden in 1990 show that 4.5% were born to mothers from other Nordic countries, 3.5% were born to mothers from other European countries, and 6% were born to mothers from outside Europe.24 In order to make the two study groups more homogeneous, only individuals of Nordic origin born in Sweden were included in the 1990 cohort (Supplemental Table S1). The figures showing the different QEPS functions were based on 2345 individuals in the 1974 cohort and 1908 in the 1990 cohort (Supplemental Table S1).
Ethical approval was obtained from the Regional Ethics Review Board in Gothenburg (Ad 91-92/131-93 and 444-08 T062-09). Informed consent was given from participants for both the school examination and the use of growth data from previous sources. Informed consent from legal guardians was given for individuals <18 years of age. Ethical approval was also obtained to compare available growth data from nonparticipating and participating individuals.
The QEPS growth model
The QEPS model was used to describe individual patterns of growth in terms of length/height from birth to adult height. Growth in height is modeled by a quadratic (Q) function, a negative exponential (E) function, a specific pubertal (P) function, and a stop (S) function (Fig. 1a).19 The different growth functions can be modified for E and P by both time-scale and height-scale parameters, and for Q and S by height-scale parameters, thus describing individualized growth. Separate curve fitting for each individual gives six estimates with CI and the possibility to compute individual QEPS-function values at all ages. The growth model can describe the total gain (called TgainP5–95) in height during puberty, as well as separate the specific gain in adult height related to puberty (Pmax) from the ongoing growth owing to the Q-function, as shown in Fig. 1a, b. The onset, middle, and end of pubertal growth was defined as the age at which 5%, 50%, and 95% of P-function growth was attained (AgeP5/AgeP50/AgeP95). The more traditional measure of the middle of puberty, age at PHV, was calculated from the total growth curve (AgeTPHV).20 The duration of growth during puberty was calculated as the time from AgeP5 to AgeP95.
Data handling and statistical analysis
To construct longitudinal growth curves for each individual, height data were exported to MATLAB®, and QEPS-model parameters were automatically computed by fitting the height data from each individual separately (The MathWorks, Inc., Natick, MA, v. 7.13.0 R2012b). Student’s two-tailed t-test was used to compare birth characteristics, growth estimates from the QEPS model, heights during childhood, and adult heights for the 1974 and 1990 growth cohorts. Statistical analyses were performed using SAS software® (SAS Institute Inc., Cary, NC, version 9.3). A p-value < 0.05 was considered statistically significant.
Results
Characteristics of growth during the fetal/infancy period including size at birth
This period includes the E-function and the first part of the Q-function of the QEPS model. The tempo of growth, mainly during infancy (Etimescale) and the gain in adult height due to E-function growth (Emax) were compared. In the 1990 compared with the 1974 cohort, growth during the fetal/infancy period was more rapid, as shown by a significantly shorter Etimescale for both girls and boys, while the total E-growth (Emax) was unchanged (Tables 1 and 2, Fig. 2). More E-growth was reached at birth in the 1990 cohort compared with the 1974 cohort and the decline in height velocity of E-function growth was more pronounced in the later-born cohort (Fig. 2), where the total E-function height is also significantly higher until 0.9 years for girls and 1.1 years for boys (Fig. 2). As a result, birth characteristics differed significantly between the 1974 and 1990 cohorts. Girls and boys born in 1990 were significantly heavier at birth (both p < 0.001), than those born in 1974 (Tables 1 and 2). Boys born in 1990 were also significantly longer than those born in 1974 (p < 0.001). In the context of increasing lengths at birth, it is interesting to note that GA was significantly lower for both girls and boys born in 1990 compared with those born in 1974.

E-height. a Difference in attained E-height between 1990 and 1974 cohorts together with the corresponding total mean E-height for girls/boys. The dotted lines show the 95% CI of the difference. The thin solid lines show the mean E-height of the 1990 cohort, and the thin dotted lines show the mean E-height of the 1974 cohort. b Difference in E-height velocity between 1990 and 1974 study cohorts together with the corresponding mean E-height velocity for girls/boys . The dotted lines show the 95% CI of the difference, meaning that there is a significant difference between the cohorts when this CI is not overlapping the zero (similar in Figs. 3 and 5). The thin solid lines show the E-height velocity of the 1990 cohort, and the thin dotted lines show the E-height velocity of the 1974 cohort
As shown in Fig. 3, the Q-function also starts before birth. Because of the higher Q-function of the 1990 cohort, boys in the 1990 cohort were significantly taller at 2 years of age than boys in the 1974 cohort (Table 2 and Fig. 3).

Q-height. a Difference in attained Q-height between 1990 and 1974 study cohorts together with the corresponding mean Q-function for girls/boys . The dotted lines show the 95% CI of the difference. The thin solid lines show the mean Q-height of the 1990 cohort, and the thin dotted lines show the mean Q-height of the 1974 cohort. b Difference in Q-height velocity between 1990 and 1974 study cohorts together with the corresponding mean Q-height velocity for girls/boys . The dotted lines show the 95% CI of the difference. The thin solid lines show the mean Q-height velocity of the 1990 cohort, and the thin dotted lines show the mean Q-height velocity of the 1974 cohort. The Q-function is a quadratic function with the height velocity declining linearly, and with significant differences between the two cohorts
Characteristics of growth during the childhood period
To study the differences in childhood growth, we evaluated one measure of growth from the QEPS model, the gain in adult height due to Q-function growth, Qmax, together with total height at 4, 6, and 8 years of age. During childhood, the Q-function describes an increase in height and the function extends into the pubertal period until adult height. Height gain related to Q-function growth was greater for girls and boys in the 1990 cohort than for girls and boys in the 1974 cohort, with a more pronounced increase for boys (Tables 1 and 2, Fig. 3). Boys in the 1990 cohort were therefore consistently taller than boys in the 1974 cohort between the ages of 2 and 8 years (Table 2, Fig. 3). For girls, the difference in Q-function was less increased, resulting in significantly increased height at 6 and 8 years in the 1990 cohort (Table 1, Fig. 3).
Characteristics of pubertal growth
To study the differences in the timing of pubertal growth for the two cohorts, four age-related measures from the QEPS model were evaluated; the ages at the start (AgeP5), middle (AgeP50), and end (AgeP95) of pubertal growth, as well as the traditional measurement of age at PHV (AgeTPHV). For girls, puberty was on average about 1 month earlier (range, 29–36 days) in the 1990 cohort based on mid (AgeP50) and end (AgeP95) estimates of pubertal growth. For boys, there were no changes in the timing of pubertal growth (Table 2).
The gain in adult height related to the specific P-function (Pmax) did not differ statistically between the two cohorts for girls or boys (Table 1, Fig. 4). Since growth in height during puberty is a combination of Q and P-functions, the total height gained during puberty (TgainP5–95) was statistically greater in girls from the 1990 compared with the 1974 cohort (p = 0.011) (Table 2). In contrast, for boys, there was no difference between the two cohorts in the total height gained during puberty (Table 2). The differences in attained height are also seen in Fig. 5, showing the total QEPS function for both height and height velocity. Both sexes have significantly higher attained heights during the pubertal years in the later-born cohort; however, the difference in the total QEPS function height velocity during puberty is not significantly changed between the two cohorts. The duration of pubertal growth was significantly shorter for girls in the 1990 compared with the 1974 cohort (–7.3 days), as seen in Table 1.

P-height. a Difference in attained P-height between 1990 and 1974 study cohorts together with the corresponding mean P-function for girls/boys . The dotted lines show the 95% CI of the difference. The thin solid lines show the mean P-function of the 1990 cohort, and the thin dotted lines show the mean P-function of the 1974 cohort. b Difference in P-height velocity between 1990 and 1974 study cohorts together with the corresponding mean P-height velocity for girls/boys. The dotted lines show the 95% CI of the difference. The thin solid lines show the mean P-height velocity of the 1990 cohort, and the thin dotted lines show the mean P-height velocity of the 1974 cohort. The age scale is adjusted for individualized onset of the P-function, AgeP5, meaning that the differences in the timing of puberty cannot be seen in this figure

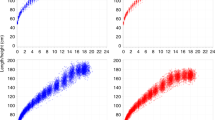
Total height. a Difference in attained QEPS height between 1990 and 1974 study cohorts together with the corresponding mean total QEPS height for girls/boys . The dotted lines show the 95% CI of the difference. The thin solid lines show the mean QEPS height of the 1990 cohort, and the thin dotted lines show the mean QEPS height of the 1974 cohort. b Difference in QEPS-height velocity between 1990 and 1974 study cohorts together with corresponding mean total QEPS-height velocity for girls/boys . The thin lines show the 95% CI of the difference. The thin solid lines show the mean QEPS-height velocity of the 1990 cohort, and the thin dotted lines show the mean QEPS-height velocity of the 1974 cohort
Adult height for both cohorts
Mean adult height was greater for the 1990 cohort than for the 1974 cohort (Table 1, Table 2). Boys in the 1990 cohort were 10 mm taller than boys in the 1974 cohort (Table 2); girls in the 1990 cohort were 6 mm taller than the girls in the 1974 cohort (Table 1). For boys, this increase in adult height was related to Q-function growth; they were taller during childhood than boys in the 1974 cohort (Table 2). For girls, the increase was due to growth during both childhood and puberty (Table 1). The difference in height and height velocity, from the total QEPS function, between the two cohorts is illustrated in Fig. 5. Increased height for both sexes is observed in the later-born cohort at all ages, except for girls in early childhood, where the CI of the difference in height between 2 and 5 years of age is just overlapping the zero, as indicated by the lower dotted line.
Discussion
Using the estimates of the QEPS model, we were able to identify the differences in growth patterns between two longitudinal growth cohorts in Sweden born only 16 years apart. These changes provided more insight why average individuals born in 1990 were taller as adults than those born in 1974. The QEPS model revealed that the increased growth in height observed in boys in the 1990 compared with the 1974 cohort was mainly a result of greater Q-function growth before puberty. For girls, the picture was more complicated. Not only did girls in the 1990 cohort show greater growth before puberty than their 1974 counterparts, but they also had an earlier and more pronounced pubertal growth. To our knowledge, the present study is the first detailed analysis of the changes of longitudinal growth patterns between two large community-based cohorts from birth to attained adult height.
The first evidence of the differences in early growth between the cohorts born in 1974 and 1990 was reflected in the “tempo”, i.e., the E-function, the Etimescale, which was found to be significantly faster in the 1990 compared with the 1974 cohort. Improved nutrition, both intrauterine and during infancy,25 and decreased maternal smoking during pregnancy,26 are potential reasons for these differences. Newborns from the 1990 cohort were heavier at birth than those in the 1974 cohort. This is in agreement with the increase in adult height between the cohorts, where higher birth weights have been associated with taller adult heights27 and is also in line with previous Nordic studies reporting a continuous rise in birth weight over time.26,28,29 We also found that boys born around 1990 were significantly longer at birth than boys born around 1974. Few studies have investigated secular changes in length at birth; however, a Danish study found an increase in length at birth between 1983 and 2003 for both sexes.29 Measuring length in newborn babies may be associated with specific methodological difficulties, and the change in length at birth that we observed should therefore be interpreted with caution. We also noted differences between the cohorts in terms of GA, however, the accuracy of this comparison requires special consideration because in 1974, GA was always based on the last menstrual period, whereas in 1990, GA could also be based on ultrasonography.26
Height at 2 years of age was also found to be greater for boys in the 1990 cohort than in the 1974 cohort, consistent with previous reports from other European countries based on repeated use of cross-sectional data.15,30,31 In addition, our results are consistent with the longitudinal studies of total growth for growth patterns by Xu et al.32 showing increased growth in height and weight, together with increased birth weight of Shanghai infants over a relatively short period of time, 10 years.
A faster tempo of early growth (in the present study expressed as a faster Etimescale) leads to an earlier transition between infancy and childhood (ICT) growth estimated by the ICP model.4,11,18,33 Earlier timing of ICT has been related to increased adult height.4,34 A recent, large study of growth patterns over 50 years in Japan and Korea has also shown that much of the secular trend in adult height was seen already at 1.5 years of age.3
In the current study, children in the 1990 cohort, particularly boys, grew more during childhood than children in the 1974 cohort, as shown by greater growth related to the Q-function of the QEPS model. This increased growth was also reflected in the observation that boys in the 1990 cohort were consistently taller than their 1974 counterparts during the childhood period. The finding that children born more recently were taller at 6 and 8 years of age than their earlier-born counterparts has also been reported in previous Swedish11,12 and Nordic growth studies.30,31,35 In our previously mentioned cross-sectional analyses of data from the two study cohorts, it was found that BMI had increased more over time in boys than in girls.17 An increase in BMI may be related to the difference in Q-function growth between boys and girls in the 1990 cohort. This is supported by recent data that showed a positive correlation between childhood BMI and Q-function growth.23
The QEPS model offers a unique possibility to dissect the components of the pubertal growth into the underlying Q-function growth and the superimposed specific pubertal growth (P-function). For girls, but not boys, the estimated middle and end of pubertal growth occurred at a significantly earlier age (by ~1 month) in the 1990 compared with the 1974 cohort. The earlier cessation of pubertal growth in girls may in part explain why adult height increased less in girls than in boys in the 1990 cohort. Weight at birth and weight patterns during childhood may be associated with the timing of pubertal growth. A recent paper by Di Giovanni et al. has shown that babies being large for GA (high birth weight) have earlier onset of pubertal growth, and a previous study by our research group found a linear negative correlation between BMI in childhood and onset of pubertal growth.23,36 Higher weight at birth and higher BMI in the 1990 cohort might be related to earlier pubertal growth seen for girls in the later-born cohort, analogous to these two studies. Compared with the former Swedish growth reference of individuals born in 1956, the 1974 cohort showed earlier mid-pubertal growth.11 For girls, our findings indicate a continuing secular trend in this respect, but at a lower level than during the prior decades; and for boys, this secular trend of earlier pubertal growth in Sweden seems to have leveled off. Previous studies from the last few decades regarding the progressively earlier timing of puberty in Europe are conflicting. Some investigations report a cessation of the trend, mainly based on the age at menarche or secondary sexual characteristics,9,37,38 whereas others have found a continuing earlier onset of pubertal growth or earlier ages at PHV.9,39,40 Also, in other affluent non-European country such as Japan, there is evidence indicating that the trend for earlier pubertal growth is leveling off, although not observed in South Korea.3
Recent studies based on the cross-sectional data used to develop new growth references in other Nordic populations have found attained height during the pubertal years to be significantly greater than that in earlier cohorts used to generate growth references.30,31,35 This finding probably indicates that there is a continuing trend for earlier pubertal growth in other Nordic countries. Estimates of the duration of pubertal growth made using the QEPS model showed that the duration of puberty was significantly shorter for girls in the 1990-born compared with the 1974 cohort, although such a short difference of ~7 days over a 4.8-year growth period may be of limited biological (and clinical) relevance.
The present study showed a positive secular trend in which height increased by 6 mm in females and 10 mm in males over a 16-year period. Given the short period, we estimate that this is a considerable change in height. Our results are in line with the previously presented cross-sectional study comparing the 1974 and 1990 cohorts at 18 years of age (including individuals from all ethnic backgrounds), which showed a significant increase in height between the two cohorts.17 The exact values are somewhat different to those of the current study (taller adult heights in the current study), explained by differences in the selection of individuals. In the present study, we included individuals, in particular males, who were still growing after the age of 18. The selection criteria were more demanding in the present study, to ensure longitudinal growth data throughout all growth phases. This is shown by both the higher mean number of measurements per individual and the reduced number of individuals studied. These findings highlight the need for standardization of the process for studying patterns of growth in a more detailed way. It should be noted that the increase in Q-function growth in the 1990 cohort is not fully transformed into adult height. More evident losses of height gain from mid-puberty until adult height were seen in the Japanese and South Korean secular study.3 Earlier and shorter duration of pubertal growth was the explanation for that loss. For girls born in 1990 in the present study, these two changes were observed. In both investigated cohorts, the proportions of parents from other Nordic countries was around 5%. All three Swedish neighboring countries Denmark, Finland, and Norway have developed new growth references within the last 7 years, also showing positive secular trends in adult heights for both sexes.30,31,35
The major strength of the current study was the use of the QEPS model, describing different specific growth that can be related to different growth phases and attained height. This has been possible due to the availability of comprehensive longitudinal data in individuals of both cohorts, an advantage over most other population growth studies that are based on cross-sectional data. Furthermore, specialized trained nurses, giving highly reliable adult height data for both the cohorts, performed standardized measurements of adult height. The selection procedure for the study population was also carefully standardized, to characterize cohorts of healthy individuals born at term in Sweden. Due to high levels of immigration in recent years, only those of Nordic origin were included in the 1990 cohort in order to improve comparability with the 1974 cohort. As this study was based on longitudinal growth data obtained in a community-based setting, including individuals of different socioeconomic status, it is likely that the results are generalizable to healthy individuals of Nordic origin in other parts of Sweden. The mean differences between the two cohorts can be regarded as quite small. Nevertheless, relatively small changes were detected by the QEPS model, which implies that the model is robust and can be used with confidence to study changes of greater magnitude in other study settings.
A limitation of this study is the lower participation rate in the 1990 cohort. Earlier, we have obtained ethical approval to analyze available growth data for nonparticipating as well as participating individuals.17,22 Comparisons of participants and nonparticipants revealed no systematic differences, with the exception of higher BMI for nonparticipating females in the 1990 cohort.22 Regarding secular changes in puberty, our study was based on only one aspect of puberty, height.
In conclusion, we confirm that over a 16-year period, there was a trend over time for length/height to increase from birth to adulthood in Swedish boys and girls. As revealed by the QEPS model, the progressively earlier timing of mid-puberty observed over the last century seems to have slowed in girls and leveled off in boys. These sex differences imply that two main components of the secular trend; being taller and entering puberty earlier, are not necessarily linked to each other. Moreover, the underlying mechanisms for these changes remain to be revealed. The QEPS model with its growth component analysis offers an alternative way to study how these mechanisms interplay with possible relations to hormones/biomarkers, results from other anthropometric measures, and imaging techniques. Another implication of the results from the present study is a need for updated national growth references reflecting current knowledge and contemporary longitudinal data.
References
Bogin, B. Evolutionary perspective on human growth. Annu. Rev. Anthropol. 28, 109–153 (1999).
Tanner, J. M. Growth as a mirror of the condition of society: secular trends and class distinctions. Acta Paediatr. 29, 96–103 (1987).
Cole T. J., Mori H. Fifty years of child height and weight in Japan and South Korea: contrasting secular trend patterns analyzed by SITAR. Am. J. Hum. Biol. 30 (2018).
Hochberg, Z. & Albertsson-Wikland, K. Evo-Devo of infantile and childhood growth. Pediatr. Res. 64, 2–7 (2008).
Gelander, L. Children’s growth: a health indicator and a diagnostic tool. Acta Paediatr. 95, 517–518 (2006).
Monteiro, P. O. & Victora, C. G. Rapid growth in infancy and childhood and obesity in later life–a systematic review. Obes. Rev. 6, 143–154 (2005).
Eriksson, J. G., Forsen, T. J., Kajantie, E., Osmond, C. & Barker, D. J. Childhood growth and hypertension in later life. Hypertension 49, 1415–1421 (2007).
Kindblom, J. M. et al. Pubertal timing is an independent predictor of central adiposity in young adult males: the Gothenburg osteoporosis and obesity determinants study. Diabetes 55, 3047–3052 (2006).
Parent, A. S. et al. The timing of normal puberty and the age limits of sexual precocity: variations around the world, secular trends, and changes after migration. Endocr. Rev. 24, 668–693 (2003).
Hatton, T. J. & Bray, B. E. Long run trends in the heights of European men, 19th–20th centuries. Econ. Human. Biol. 8, 405–413 (2010).
Liu, Y. X., Albertsson-Wikland, K. & Karlberg, J. New reference for the age at childhood onset of growth and secular trend in the timing of puberty in Swedish. Acta Paediatr. 89, 637–643 (2000).
Cernerud, L. & Lindgren, G. W. Secular changes in height and weight of Stockholm schoolchildren born in 1933, 1943, 1953 and 1963. Ann. Human. Biol. 18, 497–505 (1991).
Tanner, J. M. Growth as a monitor of nutritional status. Proc. Nutr. Soc. 35, 315–322 (1976).
Karlberg, J. Secular trends in pubertal development. Horm. Res. 57(Suppl 2), 19–30 (2002).
Fredriks, A. M. et al. Continuing positive secular growth change in The Netherlands 1955–1997. Pediatr. Res. 47, 316–323 (2000).
Schonbeck, Y. et al. The world’s tallest nation has stopped growing taller: the height of Dutch children from 1955 to 2009. Pediatr. Res. 73, 371–377 (2013).
Lissner, L. et al. Secular trends in weight, height and BMI in young Swedes: The ‘Grow up Gothenburg’ Studies. Acta Paediatr. 102, 314–317 (2013).
Karlberg, J. A biologically-oriented mathematical model (ICP) for human growth. Acta Paediatr. Scand. 350, 70–94 (1989).
Nierop, A. F. et al. Modelling individual longitudinal human growth from fetal to adult life - QEPS I. J. Theor. Biol. 406, 143–165 (2016).
Holmgren, A. et al. Insight into human pubertal growth by applying the QEPS growth model. BMC Pediatr. 17, 107 (2017).
Albertsson-Wikland, K., Luo, Z. C., Niklasson, A. & Karlberg, J. Swedish population-based longitudinal reference values from birth to 18 years of age for height, weight and head circumference. Acta Paediatr. 91, 739–754 (2002).
Sjöberg, A. et al. Body size and lifestyle in an urban population entering adulthood: the ‘Grow up Gothenburg’ Study. Acta Paediatr. 101, 964–972 (2012).
Holmgren A., et al. Pubertal height gain is inversely related to peak BMI in childhood. Pediatr. Res. (2017).
Welfare NBoHa (2015).
Silventoinen, K. Determinants of variation in adult body height. J. Biosoc. Sci. 35, 263–285 (2003).
Odlind, V., Haglund, B., Pakkanen, M. & Otterblad Olausson, P. Deliveries, mothers and newborn infants in Sweden, 1973–2000. Trends in obstetrics as reported to the Swedish Medical Birth Register. Acta Obstet. Et. Gynecol. Scand. 82, 516–528 (2003).
Karlberg, J. & Luo, Z. C. Foetal size to final height. Acta Paediatr. 89, 632–636 (2000).
Skjaerven, R., Gjessing, H. K. & Bakketeig, L. S. Birthweight by gestational age in Norway. Acta Obstet. Et. Gynecol. Scand. 79, 440–449 (2000).
Schack-Nielsen, L., Molgaard, C., Sorensen, T. I., Greisen, G. & Michaelsen, K. F. Secular change in size at birth from 1973 to 2003: national data from Denmark. Obesity 14, 1257–1263 (2006).
Saari, A. et al. New Finnish growth references for children and adolescents aged 0 to 20 years: Length/height-for-age, weight-for-length/height, and body mass index-for-age. Ann. Med. 43, 235–248 (2011).
Tinggaard, J. et al. The 2014 Danish references from birth to 20 years for height, weight and body mass index. Acta Paediatr. 103, 214–224 (2014).
Xu, X., Wang, W. P., Guo, Z. P., Cheung, Y. B. & Karlberg, J. P. Secular change in growth over one decade (1980–1990) in Shanghai infants. J. Pediatr. Endocrinol. Metab. 13, 1603–1614 (2000).
Liu, Y. X., Jalil, F. & Karlberg, J. Growth stunting in early life in relation to the onset of the childhood component of growth. J. Pediatr. Endocrinol. Metab. 11, 247–260 (1998).
Liu, Y., Albertsson-Wikland, K. & Karlberg, J. Long-term consequences of early linear growth retardation (stunting) in Swedish children. Pediatr. Res. 47(4 Pt 1), 475–480 (2000).
Juliusson, P. B. et al. Growth references for 0–19 year-old Norwegian children for length/height, weight, body mass index and head circumference. Ann. Human. Biol. 40, 220–227 (2013).
Di Giovanni, I. et al. Being born large for gestational age is associated with earlier pubertal take-off and longer growth duration: a longitudinal study. Acta Paediatr. 106, 61–66 (2017).
Juul, A. et al. Pubertal development in Danish children: comparison of recent European and US data. Int. J. Androl. 29, 247–255 (2006).
Papadimitriou, A. et al. Pubertal maturation of contemporary Greek boys: no evidence of a secular trend. J. Adolesc. Health.: Off. Publ. Soc. Adolesc. Med. 49, 434–436 (2011).
Aksglaede, L., Olsen, L. W., Sorensen, T. I. & Juul, A. Forty years trends in timing of pubertal growth spurt in 157,000 Danish school children. PLoS ONE 3, e2728 (2008).
Roelants, M., Hauspie, R. & Hoppenbrouwers, K. References for growth and pubertal development from birth to 21 years in Flanders, Belgium. Ann. Human. Biol. 36, 680–694 (2009).
Acknowledgements
We thank all the staff and students of the participating schools and the study team for the collection, and computerizing of the original data. Thanks for valuable editing and language revision to Harriet Crofts. The authors acknowledge financial support from the Swedish Research Council (7509 and VR 2006-7777); the Swedish Council Formas (259-2012-32); the Swedish Research Council for Working Life and Social Research (2006-1624); Pfizer AB; the Governmental Grants for University Hospital Research (ALF) from Region Västra Götaland; PhD grants from the Southern Swedish healthcare region; the R&D department, County of Halland; and the Foundation Växthuset for children.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
A.F.M.N. works for Muvara, Multivariate Analysis of Research Data, Statistical Consultation, the Netherlands. the remaining authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Holmgren, A., Niklasson, A., Nierop, A.F.M. et al. Estimating secular changes in longitudinal growth patterns underlying adult height with the QEPS model: the Grow Up Gothenburg cohorts. Pediatr Res 84, 41–49 (2018). https://doi.org/10.1038/s41390-018-0014-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-018-0014-z
This article is cited by
-
Growth pattern evaluation of the Edinburgh and Gothenburg cohorts by QEPS height model
Pediatric Research (2022)
-
Novel type of references for weight aligned for onset of puberty – using the QEPS growth model
BMC Pediatrics (2021)
