
Abstract
Pharmacotherapy is an effective treatment modality across psychiatric disorders. Nevertheless, many patients discontinue their medication at some point. Evidence-based guidance for patients, clinicians, and policymakers on rational discontinuation strategies is vital to enable the best, personalized treatment for any given patient. Nonetheless, there is a scarcity of guidelines on discontinuation strategies. In this perspective, we therefore summarize and critically appraise the evidence on discontinuation of six major psychotropic medication classes: antidepressants, antipsychotics, benzodiazepines, mood stabilizers, opioids, and stimulants. For each medication class, a wide range of topics pertaining to each of the following questions are discussed: (1) Who can discontinue (e.g., what are risk factors for relapse?); (2) When to discontinue (e.g., after 1 year or several years of antidepressant use?); and (3) How to discontinue (e.g., what’s the efficacy of dose reduction compared to full cessation and interventions to mitigate relapse risk?). We thus highlight how comparing the evidence across medication classes can identify knowledge gaps, which may pave the way for more integrated research on discontinuation.
Similar content being viewed by others
Introduction
Clinical guidelines generally recommend prolonged pharmacological treatment following symptomatic remission, for example for antidepressants [1, 2] and antipsychotics [3], even though the minimal duration of continuation is often unspecified or variable [4, 5]. Although prolonged medication use can be effective, most patients discontinue their medication at some point, sometimes due to poor insight, but also because of symptomatic remission, lack of effectiveness, adverse events, or a perceived negative impact on functioning [6, 7]. However, patients and physicians are also concerned about episode recurrence and possible discontinuation symptoms (DS) [8, 9]. Given the frequency of discontinuation in clinical practice and the possible consequences, it is essential to have evidence-based clinical information on rational discontinuation strategies to guide patients, clinicians and policymakers.
In psychiatry, discontinuing medication is relevant for all major medication classes, i.e., antidepressants, antipsychotics, benzodiazepines, mood stabilizers, stimulants, and opioids. This may either involve complete discontinuation (stopping) or dose reduction strategies (staying on medication at a lower dose, sometimes below the minimally effective dose) [10]. Although answers to discontinuation topics may differ between medication classes, there may also be similarities. Therefore, comparing and integrating evidence can help to establish similarities and differences regarding discontinuation. Summarizing existing discontinuation knowledge can further help provide answers for patients and physicians and optimize discontinuation care.
Here, we provide an overview of the current evidence on discontinuation for all major medication classes used in psychiatry. For an overview of the pharmacological mechanisms hypothesized to subtend discontinuation symptoms, we refer to the Supplementary Text and Supplementary Fig. 1. Opioids are included due to their clinical relevance in discontinuation care (both illicit and prescription opioids) within psychiatry. We further discuss three major clinical questions for each medication class: (1) Who can discontinue with an acceptable risk of recurrence or discontinuation problems? (i.e., determinants of risk of DS, and relapse and recurrence risks following discontinuation); (2) When is the best time to discontinue following symptomatic remission?; and (3) How can medication best be discontinued to prevent recurrence or DS? (i.e., dose reduction strategies and effective discontinuation interventions). Finally, we compare similarities and differences across the medication classes.
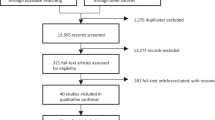
Methods
The first and last authors revisited the current evidence on discontinuation across the six major medication classes used in psychiatry: antidepressants, antipsychotics, benzodiazepines, mood stabilizers, stimulants, and opioids. Experts from each medication class were invited to contribute for their respective field. All experts have made significant contributions to the literature in their respective field and most experts have multiple year of experience clinically guiding patients in discontinuing their psychotropic medication. Four consensus meetings were held between January 2021 and October 2021. During the consensus meetings, we defined three essential questions on discontinuation that we considered to be the most clinically relevant:
-
(1)
Who can discontinue with an acceptable risk of recurrence or discontinuation problems? (i.e., determinants of risk of DS and relapse and recurrence risk following discontinuation);
-
(2)
When is the best time to discontinue following remission? (i.e., optimal timing of discontinuation); and
-
(3)
How can medication be most effectively discontinued to prevent recurrence or DS? (i.e., dose reduction strategies and discontinuation interventions).
For each psychotropic medication class, one or several expert(s) then conducted a targeted literature search and selected high-quality key research articles in the literature related to their area of expertise. Key search terms were: “antidepressants”, “antipsychotics”, “mood stabilizers”, “benzodiazepines”, “stimulants”, “opioids”, “discontinuation”, “tapering”, “discontinuation symptoms”, “discontinuation syndrome”, “withdrawal”, and “relapse”. After examining the literature on discontinuation, the expert panel identified commonalities between medication classes and reached consensus with regards to recommendations for clinical practice as well as future research avenues. Finally, the first and last authors critically revised and integrated these contributions into the current piece.
Discontinuation evidence across psychotropic medication classes
In the following section, we examine the three key clinical discontinuation questions (summarized in Table 1).
Antidepressants
Who can discontinue?
Relapse rates after discontinuation
Continuing antidepressants in patients with major depressive disorder (MDD) who responded to acute treatment halves the relapse risk compared to placebo (from 40 to 20%), in both specialized and primary care [1, 2, 11,12,13,14]. The most recent meta-analysis on this topic found that the number needed to treat (NNT) was 6, favouring continuation of antidepressants [15]. A landmark study pointed in the same direction in the context of primary care [16]. An important limitation of double-blind placebo-controlled discontinuation studies is their relatively short follow-up period (study duration averaging 40 weeks) and often rapid or abrupt antidepressant discontinuation, although the absolute relapse risk gradually decreases over time in discontinued patients [2, 15].
Discontinuation symptoms (DS)
DS of antidepressants include a range of somatic (e.g., nausea, dizziness) and psychological (e.g., irritability, low mood) symptoms [8], and are summarized using the FINISH acronym, which stands for Flu-like symptoms, Insomnia, Nausea, Imbalance, Sensory disturbances, and Hyperarousal (anxiety/agitation). DS in SSRIs were found to be higher in both surveys of selected populations and open-label studies [17, 18] (55%), than in double-blind studies (30%) [19], possibly due to smaller nocebo effects in double-blind studies and selection bias in surveys. DS especially occur during treatment with SSRIs and SNRIs that have relatively short elimination half-lives (<24 h), such as paroxetine and venlafaxine [17, 20], though other mechanisms unrelated to elimination contribute as well. For example, paroxetine has strong affinity for the M1 receptor and also inhibits its own metabolism (just like fluvoxamine and fluoxetine) [21]. Abrupt discontinuation leads to higher DS incidence rates (35–100%) compared to tapering over several weeks (42–56%) for paroxetine [17]. Conversely, fluoxetine has an elimination half-life of around 5 days (active metabolite 4–16 days), and is generally associated with fewer DS [22]. It is hypothesized that most DS coincide with the largest reductions in serotonin transporter (SERT) occupancy, which particularly occur at lower doses [8, 23, 24]. DS generally quickly resolve after dose increases or reinstatement of the antidepressant, which can aid in distinguishing DS from relapse [8].
Risk factors for relapse or DS following discontinuation
To our knowledge, based on a systematic review, no consistent empirical evidence links patient characteristics to predicting DS, including residual symptoms, number of prior episodes, and duration of antidepressant use [25]. Length of antidepressant use has been suggested to be a risk factor for some antidepressants, though the data are inconsistent [1]. Possible predictors of relapse following discontinuation are effort-reward decision time and cognitive reactivity, the latter being the most consistent predictor independent of residual symptoms [26,27,28]. However, these predictors have not been firmly established.
When to discontinue?
Most guidelines recommend to continue antidepressants for at least 4–6 months after successful acute-phase therapy in patients with first-episode MDD to prevent relapse, and longer periods after recurrent MDD [29,30,31]. Nevertheless, there is little evidence supporting a minimum duration of antidepressant treatment after stable remission. Patients with recurrent MDD should stay on treatment longer and sometimes indefinitely [16].
How to discontinue?
Discontinuation strategies
Consensus supports slow discontinuation of antidepressants, but few randomized studies have compared discontinuation strategies. Most studies employ a rather rapid 2-week tapering period with at most two steps [32,33,34]. Compared to abrupt discontinuation, 1–3-week tapering schedules lower DS frequency [32,33,34]. Although hyperbolic tapering, which involves decreasing relative dose reductions over time (Supplementary Text), is supported by expert opinion, it lacks evidence [8, 35]. Given the heterogeneity of DS between antidepressants and individual patient variation, general advice would be to slowly taper in those taking antidepressants for longer periods of time (e.g., years), and antidepressants with higher DS risk.
Dose reduction
A meta-analysis of five randomized trials found that dose reductions of phenelzine, maprotiline, imipramine, amineptine, and paroxetine increased the risk of MDD relapse by 62% relative to the group randomized to unchanged continuation [36].
Discontinuation interventions
A meta-analysis of four randomized controlled trials found no significant difference in time to depression relapse between patients receiving psychological interventions (e.g., cognitive behavioral therapy) during or after antidepressant tapering, compared to those who continued with antidepressant maintenance therapy only [37]. Another meta-analysis of 12 RCTs showed that MDD patients receiving psychotherapy during antidepressant treatment or tapering had a lower rate of relapse compared to those receiving active controls (antidepressant treatment) or treatment as usual [38]. In conclusion, a (preventive) psychotherapy is as effective as antidepressant maintenance.
Antipsychotics
Who can discontinue
Relapse rates after discontinuation
Within 18 months after treatment initiation, 74% of patients with schizophrenia discontinue because of adverse events or insufficient efficacy [39]. A comprehensive network meta-analysis of RCTs found that all continuation strategies outperformed discontinuation, with large risk reductions for continuing at standard dose (RR = 0.37; NNT = 3.2) and switching antipsychotics (RR = 0.47; NNT = 3.6) [40]. Dose reduction was moderately effective in relapse prevention (RR = 0.68; NNT 6.3) but was outperformed by continuation and switching strategies [40]. Doses below recommended levels were also associated with relapse in other studies (in first and multi-episode schizophrenia), possibly due to insufficient D2 receptor occupancy [41, 42]. Moreover, risk of poor clinical outcomes doubles in schizophrenia patients discontinuing antipsychotics at 10-year follow up relative to those continuing antipsychotics [43]. This is supported by European and Asian registry observational and cohort studies, which found lower rehospitalization rates in patients continuing antipsychotics compared to discontinuation [44]. It is also supported by observed reductions in relapse rates and mortality in patients on long-acting antipsychotics as compared to those taking oral antipsychotics [45, 46].
Discontinuation symptoms (DS)
Antipsychotic-associated DS can be somatic (e.g., nausea, sweating), motor (e.g., restlessness), and psychological (e.g., irritability) in nature [47]. Hyperkinesia may also occur upon withdrawal and can last for months [48]. A systematic review of five studies (of mediocre quality) found a pooled frequency of DS of 53%, while abrupt discontinuation resulted in DS in 37–70% of patients (Table 1), with nocebo effects potentially playing a role [47].
Risk factors for relapse following discontinuation
Established risk factors for relapse after discontinuation or dose reduction include a diagnosis of schizophrenia (as compared to other psychotic disorders), long illness duration, poor pre-morbid functioning, no receipt of psychosocial intervention programs during discontinuation, shorter follow-up and in-hospital care [49,50,51]. Increased prolactin concentration, recurring hospitalizations, higher score on the Clinical Global Impression (CGI) severity scale, smoking, oral antipsychotic treatment (compared to long-acting injectables) and smoking have also been identified as predictors for relapse after discontinuation [52].
When to discontinue
Even though guidelines differ in their recommendations, several of them advise antipsychotic continuation up to 1–2 years after a first episode of psychosis (FEP) and life-long maintenance treatment after multiple psychotic episodes [53]. For those with a FEP, quick recovery and few poor prognostic factors, discontinuation may be considered after 6 months of remission. Relapse risk increases with longer illness duration and time since discontinuation [43, 54, 55]. We therefore emphasize the need for careful shared decision-making on discontinuing antipsychotics for patients who have been using them for longer time periods.
How to discontinue
Discontinuation strategies
For antipsychotic discontinuation, no evidence exists that gradual tapering decreases the risk of DS, although some recommend gradual and slowly (in months, possibly hyperbolic) tapering over quicker or abrupt discontinuation (Supplementary Text) [51, 56]. Tapered discontinuation (compared to abrupt discontinuation) may reduce the risk of adverse somatic events after full discontinuation [57], although the minimum dose threshold appears to have more relevance [51].
Dose reduction
To our knowledge, no published trials have compared dose reduction with complete discontinuation. A meta-analysis found that dose reduction doubles relapse risk relative to dose maintenance, particularly below 200 mg/day chlorpromazine equivalent or 2.5 mg risperidone equivalent, highlighting the importance of the extent of dose reduction [58, 59]. The one trial at the time of writing that had compared antipsychotic dose reduction with maintenance strategies was conducted in people with recurrent psychotic disorders and FEP [10]. It compared maintenance treatment with gradual, monitored, reduction of antipsychotics over several months (median dose reduction at any point 67% in the reduction group and 0% in the maintenance group). The results indicate that social functioning after 2 years is equal between groups, but that the risk of severe relapse is higher in the dose reduction than the maintenance group [10]. In contrast, observational data hint at possible functional improvements in functioning after antipsychotic dose reduction in similar patient populations [60, 61], but the possibility of confounding by indication precludes definitive conclusions from such data. New trials are underway to compare dose reduction or drug discontinuation with continuation strategies [62, 63], including guided dose reduction to establish the minimum effective dose [64]. Besides dose reduction studies, intermittent dosing strategies have also been proposed, with either regular gaps in dosing (from alternate days to several weeks) [65], or only initiating antipsychotics when psychotic symptoms emerge, with no antipsychotic use between psychotic episodes. While the first strategy has shown some merits if drug-free days are few, the second strategy increased relapse risk and rehospitalization [66], limiting the current role of intermittent dosing strategies for antipsychotics.
Discontinuation interventions
No interventions to mitigate relapse risks in those discontinuing antipsychotics have been described. In clinical practice, patients tapering antipsychotics are closely monitored, family members may be involved, and psychosocial interventions may be considered [67].
Mood stabilizers
Who can discontinue?
Relapse rates after discontinuation
General: the question whether to continue or stop a mood stabilizer (lithium, valproate, lamotrigine, and carbamazepine) is relevant in long-term prophylactic (maintenance) treatment of bipolar disorder [68]. Patients with multiple recurrences are obvious candidates for long-term maintenance pharmacotherapy, but convincing evidence for this strategy is scarce [69]. Sustained (e.g., ≥10 years) maintenance therapy without relapses can hint that treatment may be no longer needed, but can also indicate treatment effectiveness, given the general assumption that bipolar disorder is a lifelong illness with a high risk of recurrence [68]. Given the highly heterogeneous course of bipolar disorder, decisions about whether or not to discontinue maintenance treatment require a thorough evaluation of illness course before and during treatment and assessment of risk factors for recurrence in each individual patient, as well as patients previous experiences with stopping mood stabilizers [68].
Lithium: few studies have reported follow-up after discontinuation vs. discontinuation of maintenance treatment. One observational study found that continuous lithium use reduced relapse risk by half compared to discontinuation during 6 year follow-up [70]. It is important to note that lithium discontinuation, particularly abrupt discontinuation, can lead to increased suicidality [71].
Valproate/carbamazepine/lamotrigine: a meta-analysis on lithium, lamotrigine, and second-generation antipsychotics (SGA’s) found a 61% relative risk reduction after 6 months in continuation compared to discontinuation groups [72].
Antipsychotics: although SGA’s are not mood stabilizers in the strict sense, several SGA’s have been recommended for maintenance treatment in bipolar disorder as monotherapy or combined with a mood stabilizer: quetiapine, asenapine, aripiprazole, olanzapine, risperidone, paliperidone, and lurasidone [72].
Discontinuation symptoms (DS)
Lithium: discontinuation of lithium may lead to irritability, anxiety, restlessness, vertigo, dizziness, and lightheadedness, particularly in the first week. Symptoms are generally mild and self-limiting [48, 73]. Abruptly or rapidly stopping lithium (within 2 weeks) can lead to “rebound” manic and depressive episodes [74]. There is no strong evidence that lithium is less effective when discontinued and restarted, compared to continuous treatment, a phenomenon that has been seen in anecdotal case reports and in about 15% of patients across seven published cohort studies [75].
Valproate/carbamazepine/lamotrigine: for carbamazepine, valproate, and lamotrigine, discontinuation phenomena include anxiety, agitation, irritability, lack of energy, depression, insomnia, depersonalization, and impaired concentration and memory [48].
Antipsychotics: SGA’s have been addressed in the section on antipsychotics above.
Risk factors for relapse following discontinuation
In bipolar disorder, young age of onset, psychotic features, numerous previous episodes, rapid cycling, comorbid anxiety, comorbid substance use, and persistent subthreshold symptoms are risk factors for recurrence, even during maintenance treatment [76]. These factors likely increase the risk of relapse following discontinuation, although direct evidence is lacking.
When to discontinue?
Most guidelines recommend that mood stabilizers for acute manic or depressive episodes be continued at least for several months after symptomatic remission (i.e., during the continuation treatment phase following the acute treatment and preceding maintenance treatment) [77], but evidence is scarce. However, in most patients with bipolar disorder it is recommended that a mood stabilizer should be continued for long-term maintenance treatment to prevent recurrences and improve inter-episodic functioning [68, 76].
How to discontinue?
Discontinuation strategies
Lithium: gradual discontinuation of lithium (at least over a month) reduces risk of DS and early recurrence relative to rapid discontinuation [74]. In clinical practice, lithium and other mood stabilizers are often tapered hyperbolically (Supplementary Text) [78]. If lithium needs to be discontinued because of inefficacy or severe side effects, it may be replaced with another mood stabilizer or SGA [79].
Valproate/carbamazepine/lamotrigine: it is unclear whether this also applies to other mood stabilizers [48].
Dose reduction
Lithium: for lithium, recommended effective doses for the prevention of manic and depressive episodes result in blood plasma levels of 0.6–0.8 mmol/l, or, in some cases, 0.4–0.6 mmol/l [80]. Dose reductions below these levels may diminish effectiveness.
Valproate/carbamazepine/lamotrigine: minimally effective blood levels are less robustly established than for lithium: 50 mg/l for valproate, 4 mg/l for carbamazepine, and 3 mg/l for lamotrigine.
Discontinuation interventions
There are no known interventions to reduce relapse risk or DS during or after mood stabilizer discontinuation. Closely monitoring mood symptoms during discontinuation of mood stabilizers is recommended, for at least 1 year [78].
Benzodiazepines
Who can discontinue?
Relapse rates after discontinuation
Relapse rates for benzodiazepines are generally intricate to ascertain given the diversity of symptoms for which benzodiazepines are prescribed. Nevertheless, the majority of patients succeed in discontinuing benzodiazepines, as shown by systematic reviews and meta-analyses that found an average 1-year discontinuation success rate of 55–64% [81,82,83].
Discontinuation symptoms (DS)
Most patients discontinuing benzodiazepines experience some degree of DS (59–78%) [84, 85]. Physical DS of benzodiazepine discontinuation include muscle tension, weakness, spasms, pain, and influenza-like symptoms (sweating and shivering). Psychological DS include anxiety and panic attacks, restlessness, agitation, depression, mood swings, concentration difficulties, and sleep disturbances [86, 87]. In rare instances, rapid discontinuation may induce more severe DS, including seizures and psychotic symptoms [88]. DS may emerge or worsen weeks after discontinuation, with highest risks in short elimination half-life benzodiazepines (temazepam and lorazepam) [89,90,91].
Risk factors for relapse following discontinuation
Patients often want to stop after long-term benzodiazepine use, but face barriers such as dependence and misuse, reliance on benzodiazepines for comfort, and anticipation of sleep problems [92]. Intrinsic motivation and sufficient time to consider the benefits of discontinuation can help [92].
When to discontinue?
For most patients, adverse events of long-term benzodiazepine use (e.g., increased fall risk, sleepiness and cognitive impairment) do not outweigh the benefits [93]. For the sedative and anticonvulsant actions of benzodiazepines, discontinuation should commence before tolerance develops (i.e., first weeks of use) [94]. There is no evidence suggesting that discontinuation is easier after short-term use than long-term use. Regarding the anxiolytic and amnesic effects of benzodiazepines, there is no evidence that tolerance develops. The risk/benefit ratio of continued use should be discussed at least annually and discontinuation advised where possible.
How to discontinue?
Discontinuation strategies
Benzodiazepines should be gradually discontinued to prevent seizures and severe DS after more than 3 months of use [78]. Even after chronic use, discontinuation over a period of less than 6 months is feasible and appropriate [95]. Gradual dose reduction reduces DS intensity and improves discontinuation success [95]. However, no RCTs have compared different dose reduction methods. UK guidelines pragmatically suggest a reduction of about 12.5% of the daily dose every 2 weeks [96]. In clinical practice, a weekly reduction of 25% for the first 75% of the dose, followed by hyperbolic tapering or steps of 12.5% for the final 25% of the dose is often used [97]. There is no evidence for week-on week-off (pulse) dosing [98]. Switching to a long-acting benzodiazepine before discontinuation may be preferable for some patients, particularly when discontinuation attempts have failed, or with high doses (over 30 mg diazepam equivalent) [90, 95, 99]
Dose reduction
No evidence comparing dose reduction to discontinuation exists. Long-term use of benzodiazepines is generally not recommended and complete discontinuation should be attempted.
Discontinuation interventions
Cognitive behavioral therapy add-on results in little added value over solely gradual dose reduction in the long run (>6 months post-intervention) [87, 100]. Multifaceted deprescribing interventions are effective in reducing benzodiazepine use [101]. While motivational interviewing may be used, there is insufficient evidence for its standard application [87]. Gradual dose reduction combined with a brief or “minimal” intervention (personalized letter, self-help information) in primary care is superior to routine care alone [102,103,104]. Generally, interventions focused on patient self-awareness and education up discontinuation successes [92]. Valproic acid, carbamazepine and tricyclic antidepressants may help with benzodiazepine discontinuation, albeit with low quality evidence [83, 93]. The use of flumazenil for benzodiazepine discontinuation remains experimental [105, 106].
Opioids
Who can discontinue?
Relapse rates after discontinuation
Opioids are commonly prescribed for two indications: analgesic indications and agonist treatment in patients with illicit opioid use. As an analgesic, opioids have a place in acute and cancer-related pain. However, continued long-term use for chronic non-cancer pain may induce adverse events, such as elevated pain, mood disorders and reduced quality of life, without clear benefits as an analgesic [107,108,109,110,111]. In these cases, opioid discontinuation should be initiated as early as possible as nearly 5% of patients develop an opioid use disorder [112]. Patients with chronic non-cancer pain and an opioid use disorder discontinuing their opioids have a relapse rate of 23% after 1 year [113, 114]. In patients on opioid agonist treatment (methadone or buprenorphine), the aim is to reduce opioid-related harm [115]. These patients generally had several previous failed attempts to stop illicit opioid use. Patients with illicit opioid use disorder who use agonist treatment have a relapse rate of 71% within 1 month after discontinuation of agonist treatment [113, 114]. Treatment goals for these patients should be more toward harm reduction with opioid agonist therapy (i.e., methadone or buprenorphine) instead of tapering. Only in a subset of individuals who have a wish to taper or discontinue their agonist treatment, and have improved psychological or social conditions, such as improvement on co-occurring mental disorders or housing situations, tapering or discontinuation can be considered [115].
Discontinuation symptoms (DS)
Opioid discontinuation in patients with chronic pain reduces pain severity and improves quality of life [116]. Increased pain and craving can occur in some patients in short term, particularly at higher doses [117]. In patients on agonist treatment, discontinuation of agonist treatment has been associated with increased craving levels, and reduced quality of life. Discontinuation of prescription opioids is usually accompanied by DS after more than 3 weeks of use [116, 118, 119]. Typical opioid DS include dysphoria, anxiety, agitation, nausea, muscle ache, rhinorrhea, sweating, diarrhea, yawning, fever, and insomnia [120]. Higher opioid doses and long-term use result in more severe DS, while long-acting opioids (methadone or buprenorphine) cause less severe DS [121]. Among patients with opioid use disorders, acute discontinuation or rapid tapering of opioids may lead to withdrawal that requires medical care [122]. In individuals discontinuing opioids after long-term use for chronic pain, suicidal ideation and self-directed violence may occur [123124]. Overdose-related morbidity is more likely in the first month after discontinuation, due to decreased tolerance to original doses following relapse [125]. Opioid discontinuation may result in illicit opioid use, including heroin and illegally manufactured fentanyl [126].
Risk factors for relapse following discontinuation
Individuals dissatisfied with their opioid use and those not experiencing the desired analgesic effect are more likely to discontinue opioids successfully [118, 127]. Young age, low doses, short duration of use, good socio-economic context, and a negative history of psychiatric illness are positively associated with successful opioid discontinuation [118, 127,128,129,130]. Conversely, adequate depression treatment may increase the incidence of opioid use cessation in patients with chronic pain [131].
When to discontinue?
Opioids prescribed as analgesics should be discontinued before tolerance develops as long-term use is not indicated for chronic (non-cancer related) pain [132]. The risk/benefit ratio of continued use should be discussed regularly and discontinuation advised when possible.
In patients on opioid agonis treatment, treatment effectiveness, and co-use of other drugs (including illicit opioids) should regularly assessed. In individuals who have a wish to taper or discontinue their agonist treatment, and have improved psychological or social conditions, such as improvement on co-occurring mental disorders or housing situations, tapering or discontinuation can be considered [115].
How to discontinue?
Discontinuation strategies
Patients on low-dose prescription opioids (<20 mg oral morphine equivalents) and/or for a short duration (<2–3 weeks) can generally discontinue without tapering [128]. In other patients, tapering is advised [128]. More rapid tapering generally results in more severe withdrawal and lower success rates [133, 134]. The advised rate of discontinuation in guidelines ranges between 10% per month and 50% per week of the initial dose, with slower tapers (i.e., 10% reduction per month) being more likely to be better tolerated [133, 134]. If rapid discontinuation of opioids is necessary for medical reasons, reduction strategies of up to 50% per week are possible [128]. Switching to long-acting opioids (usually 70% dose-equivalent) can be considered with high doses (>90 mg morphine equivalents) and/or prolonged opioid use (>3 months), but also in patients with prior failed discontinuation attempts. Long-acting opioids should be tapered to the lowest possible dose, and then discontinued [135, 136].
Dose reduction
Discontinuation should be the primary goal in patients using opioids for analgesic purposes. Nevertheless, in patients at high risk of relapse (high opioid doses, long-time use, either with or without opioid use disorder) [118, 128, 129], long-acting opioid agonist treatment (e.g., methadone or buprenorphine) can be considered [137]. In patients on agonist treatment, dose reduction strategies are recommended when adverse events develop, or in the event of pharmacokinetic changes, e.g., due to co-medication, successful treatment of hepatitis, or ageing.
Discontinuation interventions
Mindfulness and cognitive behavioral therapy in patients with opioid use disorder result in lower perceived pain and focus on analgesics [138]. Such strategies may facilitate discontinuation of opioids, although evidence is lacking. There is limited evidence for clonidine for agitation, shaking and muscle ache, anti-emetics for nausea, and loperamide for diarrhea. For insomnia, benzodiazepines should be given with caution in this patient group, due to their risk of developing sedative use disorder [137].
Stimulants
Who can discontinue?
Relapse rates after discontinuation
Patients with ADHD who continue stimulants have a better quality of life, less impulsive behavior and hyperactivity, compared to those who discontinue [139, 140]. The majority of patients who discontinue stimulants need to re-start treatment within 2 weeks due to worsening of ADHD symptoms REF. Nevertheless, ~30% of children with ADHD can discontinue their stimulants without worsening of ADHD symptoms at 3 months follow up [141, 142].
Discontinuation symptoms (DS)
DS are uncommon after discontinuation, although transient fatigue, insomnia (or hypersomnia), vivid dreaming, and irritability have been described [120, 143]. Transient motor symptoms may particularly occur with concomitant use of antipsychotics.
Risk factors for relapse following discontinuation
Re-emergence of ADHD symptoms is independent of age and sex, although adults may be at less risk compared to minors after stimulant discontinuation [139, 144]. There are no other reliable predictors for successful stimulant discontinuation.
When to discontinue?
Guidelines recommend to annually review patients taking prescription stimulants. During such evaluations, patients’ perspectives, risk-to-benefit ratios, and medication doses should be evaluated [145]. Prolonged treatment is recommended in adolescence, due to a high level of negative outcomes in ADHD patients during this age phase. The American Academy of Child and Adolescent Psychiatry suggests clinicians consider stimulant discontinuation in ADHD after a 1-year period without significant ADHD symptoms, dose adjustments, or symptom worsening during drug holidays [146].
How to discontinue?
Discontinuation strategies
Discontinuation of prescribed stimulants is considered safe, usually without tapering. In clinical practice, tapering stimulants is sometimes considered, while lacking evidence [139, 147].
Dose reduction
One RCT found that a 50% dose reduction results in significant worsening of ADHD symptoms [148]. At the risk of unwanted worsening drug adherence [149], drug-free “holidays” may have positive effects on ADHD symptoms and adverse events [139].
Discontinuation interventions
Guidelines on detoxification of non-prescribed stimulants support the use of supportive measures. Short-term (<2 weeks) use of benzodiazepines may reduce irritability and improve sleep [150].
Integration of evidence across medication classes
From the current evidence across medication classes in this perspective, we identified seven commonalities that are discussed below (see also Supplementary Text, Section 2 for more details). An important limitation that should be kept in mind is that the discontinuation studies at hand often have methodological shortcomings, including short follow up, as well as abrupt or very rapid discontinuation schedules [151]. There is thus a strong need for more robust evidence to guide evidence-based decision-making on psychotropic drug discontinuation in clinical practice.
Discontinuation symptoms are common but remain difficult to predict
First, discontinuation symptoms are common, particularly after abrupt or rapid cessation of medication, except in the case of stimulants. These symptoms generally dampen over time and seem less likely when discontinuation occurs gradually. In general, DS risk is higher for psychotropic drugs with shorter elimination half-lives, such as paroxetine, venlafaxine, clozapine, morphine, oxycodone, lorazepam, and temazepam (Table 1). Nevertheless, estimations of DS prevalence across medication groups are heterogeneous (see also Table 1). A challenge is that DS are often not measured at all, and, if measured, their operationalization varies (e.g., concerning questionnaires, cutoff values, and time points) [18]. Moreover, in many blinded studies, medication is abruptly stopped. Thus, current estimations of DS not only reflect the situation following abrupt or very quick cessation, but also include the influence of expectations and patients and clinicians’ experiences and may thus be subject to nocebo effects. Finally, it can be challenging to disentangle DS from relapse due to symptom overlap [8]. This may result in DS being misdiagnosed as relapse in discontinuation studies [22].
Do not discontinue medication too quickly
Second, it is clear that abrupt discontinuation is not only associated with DS, but also entails increased relapse risks. Nevertheless, the optimal period during which medication should be discontinued and the rate of dose reduction are unclear. Pragmatically, discontinuation over months is advisable, but evidence for these strategies is lacking. Gradual lowering of the dose is generally recommended for several reasons. First, relapse may be less severe if a patient is on a medium or low dose relative to discontinuation. Second, steady-state may be more readily re-achieved if relapse occurs while a patient is on a lower dose. Third, gradual tapering may be more comfortable for patients because of the decreased likelihood of DS. Gradual tapering is often possible using conventional dose regimens, and many patients can discontinue using these existing doses. Nevertheless, when discontinuation poses a greater challenge, a gradual decrease with low doses may be feasible. Another option that becomes apparent across medication classes is the possibility to switch to long-acting agents, e.g., diazepam, sustained-release buprenorphine and fluoxetine (although of the latter intervention only case reports are known). For some medications, e.g., opioids and antipsychotics, (demographic) variables have been associated with successful tapering, but given the lack of replicated findings these are not ready for translation into clinical practice.
Urgent need for more interventions to help patients successfully discontinue
Third, the literature on pharmacotherapeutic and psychological interventions to help patients start and finish tapering regiments is heterogeneous. For benzodiazepines, easy-to-use interventions, such as letters, are effective, but whether this extends to other medication classes is unknown. For preventive CBT, there is some evidence that it can help successfully discontinue antidepressants. More intervention studies are needed to assess whether time-intensive psychosocial interventions, CBT or simple interventions can help patients discontinue. For drugs that can lead to physical dependence (i.e., benzodiazepines and opioids), the need to discontinue is often relatively urgent and pressing.
Many patients can successfully discontinue
Fourth, while relapse risks increase after discontinuation (two-fold for antidepressants, stimulants and higher for antipsychotics), a (considerable) proportion of patients do not relapse. Conversely, a substantial proportion of patients still relapses while using medication. Therefore, the long-term perspective of discontinuation is that the risk-benefit ratio may shift for patients toward stopping their medication at some point, at least once. The weighing of risks vs. benefits related to discontinuation are personal and involve considerations about side effects, patient preferences, psychiatric history, and treatment efficacy. We believe that (dis)continuation should be periodically discussed with patients and family, and an emergency plan with relapse signs and subsequent advised actions can be helpful.
Chronic treatment with benzodiazepines and opioids should be discouraged
Fifth, discontinuing benzodiazepines and opioids is different from stopping antidepressants, mood stabilizers, or antipsychotics due to their potential for dependence after chronic use. The decision to discontinue should, in our opinion, be based on shared decision-making between patients and their families, physicians, and pharmacists. Shared decision-making can facilitate one to come up with the most viable strategy, which often includes considerations about relapse risk as well as other domains, such as quality of life and well-being.
Relapse is too narrow an outcome
Sixth, studies have predominantly focused on relapse risk, largely ignoring other outcomes relevant to patients, such as social functioning or subjective well-being. Moreover, there are varying definitions of relapse and remission both within and across different diagnostic entities, such as MDD, bipolar disorder, and schizophrenia. Therefore, even though phenotypes may be comparable, unique patterns and courses within a certain disorder necessitate uniform criteria for what constitutes relapse or remission. This heterogeneity of definitions hampers comparisons of relapse rates across disorders, and emphasize to include outcomes that are transdiagnostic and transcend relapse-based outcomes. Incorporating a transdiagnostic approach in future discontinuation studies, and including patient groups with conditions like schizoaffective disorder and bipolar depression, is crucial to broaden our understanding across various psychiatric disorders, highlighting the need for adaptive and individualized treatment protocols, regardless of specific diagnosis.
The need for shared decision making and integrated deprescribing
Shared decision-making is essential for the success of the discontinuation strategy, tailoring decisions to individual patient needs, abiding by informed consent procedures and empowering a patient’s autonomy, while at the same time carefully weighing in the harm/benefit ratio of discontinuation [152]. Moreover, the overall infrastructure of a county’s healthcare system is an important determinant of how discontinuing practices can be implemented. For instance, in a well-resourced healthcare system, there might be more opportunities for close monitoring, early intervention, and comprehensive support services, which can be pivotal in preventing relapse. This aspect is often under-discussed but is critical for understanding and improving treatment outcomes in mental health care. Indeed, rational deprescribing can benefit from interdisciplinary support and interdisciplinary collaboration, wherein physicians and pharmacists together discuss with patients to decide whether or not to discontinue [153].
Conclusion
Cross-pollination across medication classes has helped us to identify, catalog, and advance our knowledge on medication discontinuation in psychiatry. For clinicians it is important to have background knowledge about this topic to be able to advise on the safest strategies for treatment discontinuation for patients considering discontinuation [154]. There is already quite some evidence that can be applied to clinical practice where patients often have limited help in the discontinuation of their medication. At the same time, it is also clear that both the quantity and quality of discontinuation evidence is not only heterogeneous, but also quite limited [155]. Therefore, in Box 1, we have summarized several recommendations on how to further advance our knowledge about discontinuation in psychiatry. We believe research priorities should be drawn toward deprescribing in psychiatry, aiming to help patients and clinicians discontinue responsibly and jointly.
References
Baldessarini RJ, Lau WK, Sim J, Sum MY, Sim K. Duration of initial antidepressant treatment and subsequent relapse of major depression. J Clin Psychopharmacol. 2015;35:75–6.
Geddes JR, Carney SM, Daview C, Furukawa TA, Kupfer DJ, Frank E, et al. Relapse prevention with antidepressant drug treatment in depressive disorders: a systematic review. Lancet. 2003;361:9.
Leucht S, Tardy M, Komossa K, Heres S, Kissling W, Salanti G, et al. Antipsychotic drugs versus placebo for relapse prevention in schizophrenia: a systematic review and meta-analysis. Lancet. 2012;379:2063–71.
Cleare A, Pariante CM, Young AH, Anderson IM, Christmas D, Cowen PJ, et al. Evidence-based guidelines for treating depressive disorders with antidepressants: a revision of the 2008 British Association for Psychopharmacology guidelines. J Psychopharmacol. 2015;29:459–525.
Kennedy SH, Lam RW, McIntyre RS, Tourjman SV, Bhat V, Blier P, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 3. Pharmacological treatments. Can J Psychiatry. 2016;61:540–60.
Ambresin G, Palmer V, Densley K, Dowrick C, Gilchrist G, Gunn JM. What factors influence long-term antidepressant use in primary care? Findings from the Australian diamond cohort study. J Affect Disord. 2015;176:125–32.
Samalin L, Belzeaux R. Why does non-adherence to treatment remain a leading cause of relapse in patients with bipolar disorder? Eur Neuropsychopharmacol. 2023;73:16–8.
Horowitz MA, Taylor D. Tapering of SSRI treatment to mitigate withdrawal symptoms. Lancet Psychiatry. 2019;6:538–46.
Renoir T. Selective serotonin reuptake inhibitor antidepressant treatment discontinuation syndrome: a review of the clinical evidence and the possible mechanisms involved. Front Pharm. 2013;4:45.
Moncrieff J, Crellin N, Stansfeld J, Cooper R, Marston L, Freemantle N, et al. Antipsychotic dose reduction and discontinuation versus maintenance treatment in people with schizophrenia and other recurrent psychotic disorders in England (the RADAR trial): an open, parallel-group, randomised controlled trial. Lancet Psychiatry. 2023;10:848–59.
Borges S, Chen YF, Laughren TP, Temple R, Patel HD, David PA, et al. Review of maintenance trials for major depressive disorder: a 25-year perspective from the US Food and Drug Administration. J Clin Psychiatry. 2014;75:205–14.
Furukawa TA, Cipriani A, Barbui C, Geddes JR. Long-term treatment of depression with antidepressants: a systematic narrative review. Can J Psychiatry. 2007;52:545–52.
Gueorguieva R, Chekroud AM, Krystal JH. Trajectories of relapse in randomised, placebo-controlled trials of treatment discontinuation in major depressive disorder: an individual patient-level data meta-analysis. Lancet Psychiatry. 2017;4:230–7.
Viguera AC, Baldessarini RJ, Friedberg J. Discontinuing antidepressant treatment in major depression. Harv Rev Psychiatry. 1998;5:293–306.
Kato M, Hori H, Inoue T, Iga J, Iwata M, Inagaki T, et al. Discontinuation of antidepressants after remission with antidepressant medication in major depressive disorder: a systematic review and meta-analysis. Mol Psychiatry. 2021;26:118–33.
Lewis G, Marston L, Duffy L, Freemantle N, Gilbody S, Hunter R, et al. Maintenance or discontinuation of antidepressants in primary care. N Engl J Med. 2021;385:1257–67.
Davies J, Read J. A systematic review into the incidence, severity and duration of antidepressant withdrawal effects: are guidelines evidence-based? Addict Behav. 2019;97:111–21.
Jauhar S, Hayes J. The war on antidepressants: what we can, and can’t conclude, from the systematic review of antidepressant withdrawal effects by Davies and Read. Addict Behav. 2019;97:122–5.
Baldwin DS, Montgomery SA, Nil R, Lader M. Discontinuation symptoms in depression and anxiety disorders. Int J Neuropsychopharmacol. 2007;10:73–84.
Rosenbaum JF, Fava M, Hoog SL, Ascroft RC, Krebs WB. Selective serotonin reuptake inhibitor discontinuation syndrome: a randomized clinical trial. Biol Psychiatry. 1998;44:77–87.
Jauhar S, Hayes J, Goodwin GM, Baldwin DS, Cowen PJ, Nutt DJ. Antidepressants, withdrawal, and addiction; where are we now? J Psychopharmacol. 2019;33:655–9.
Horowitz MA, Taylor D. Distinguishing relapse from antidepressant withdrawal: clinical practice and antidepressant discontinuation studies. BJPsych Adv. 2022;28:297–311.
Meyer JH, Wilson AA, Sagrati S, Hussey D, Carella A, Potter WZ, et al. Serotonin transporter occupancy of five selective serotonin reuptake inhibitors at different doses: an [11C]DASB positron emission tomography study. Am J Psychiatry. 2004;161:826–35.
Fava GA, Gatti A, Belaise C, Guidi J, Offidani E. Withdrawal symptoms after selective serotonin reuptake inhibitor discontinuation: a systematic review. Psychother Psychosom. 2015;84:72–81.
Berwian IM, Walter H, Seifritz E, Huys QJ. Predicting relapse after antidepressant withdrawal—a systematic review. Psychol Med. 2017;47:426–37.
Figueroa CA, Ruhe HG, Koeter MW, Spinhoven P, Van der Does W, Bockting CL, et al. Cognitive reactivity versus dysfunctional cognitions and the prediction of relapse in recurrent major depressive disorder. J Clin Psychiatry. 2015;76:e1306–12.
de Klerk-Sluis JM, Huijbers MJ, Locke S, Spijker J, Spinhoven P, Speckens AEM, et al. Factors associated with relapse and recurrence of major depressive disorder in patients starting mindfulness-based cognitive therapy. Depress Anxiety. 2022;39:113–22.
Berwian IM, Wenzel JG, Collins AGE, Seifritz E, Stephan KE, Walter H, et al. Computational mechanisms of effort and reward decisions in patients with depression and their association with relapse after antidepressant discontinuation. JAMA Psychiatry. 2020;77:513–22.
Davidson JR. Major depressive disorder treatment guidelines in America and Europe. J Clin Psychiatry. 2010;71:e04.
Nutt DJ, Davidson JR, Gelenberg AJ, Higuchi T, Kanba S, Karamustafalioglu O, et al. International consensus statement on major depressive disorder. J Clin Psychiatry. 2010;71:e08.
Van Avendonk M, van Weel-Baumgarten E, van der Weele G, Wiersma T, Burgers JS. Summary of the Dutch College of General Practitioners’ practice guideline ‘Depression’. Ned Tijdschr Geneeskd. 2012;156:A5101.
Tint A, Haddad PM, Anderson IM. The effect of rate of antidepressant tapering on the incidence of discontinuation symptoms: a randomised study. J Psychopharmacol. 2008;22:330–2.
Khan A, Musgnung J, Ramey T, Messig M, Buckley G, Ninan PT. Abrupt discontinuation compared with a 1-week taper regimen in depressed outpatients treated for 24 weeks with desvenlafaxine 50 mg/d. J Clin Psychopharmacol. 2014;34:365–8.
Gallagher JC, Strzinek RA, Cheng RF, Ausmanas MK, Astl D, Seljan P. The effect of dose titration and dose tapering on the tolerability of desvenlafaxine in women with vasomotor symptoms associated with menopause. J Womens Health. 2012;21:188–98.
Ruhe HG, Horikx A, van Avendonk MJP, Groeneweg BF, Woutersen-Koch H. Discontinuation of antidepressants T. Tapering of SSRI treatment to mitigate withdrawal symptoms. Lancet Psychiatry. 2019;6:561–2.
Papakostas GI, Perlis RH, Seifert C, Fava M. Antidepressant dose reduction and the risk of relapse in major depressive disorder. Psychother Psychosom. 2007;76:266–70.
Breedvelt JJF, Warren FC, Segal Z, Kuyken W, Bockting CL. Continuation of antidepressants vs sequential psychological interventions to prevent relapse in depression: an individual participant data meta-analysis. JAMA Psychiatry. 2021;78:868–75.
Guidi J, Fava GA. Sequential combination of pharmacotherapy and psychotherapy in major depressive disorder. JAMA Psychiatry. 2021;78:261.
Lieberman JA, Stroup TS, McEvoy JP, Swartz MS, Rosenheck RA, Perkins DO, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353:1209–23.
Ostuzzi G, Vita G, Bertolini F, Tedeschi F, De Luca B, Gastaldon C, et al. Continuing, reducing, switching, or stopping antipsychotics in individuals with schizophrenia-spectrum disorders who are clinically stable: a systematic review and network meta-analysis. Lancet Psychiatry. 2022;9:614–24.
Taipale H, Tanskanen A, Correll CU, Tiihonen J. Real-world effectiveness of antipsychotic doses for relapse prevention in patients with first-episode schizophrenia in Finland: a nationwide, register-based cohort study. Lancet Psychiatry. 2022;9:271–9.
Hojlund M, Kemp AF, Haddad PM, Neill JC, Correll CU. Standard versus reduced dose of antipsychotics for relapse prevention in multi-episode schizophrenia: a systematic review and meta-analysis of randomised controlled trials. Lancet Psychiatry. 2021;8:471–86.
Hui CLM, Honer WG, Lee EHM, Chang WC, Chan SKW, Chen ESM, et al. Long-term effects of discontinuation from antipsychotic maintenance following first-episode schizophrenia and related disorders: a 10 year follow-up of a randomised, double-blind trial. Lancet Psychiatry. 2018;5:432–42.
Oh J, Nam H, Park S, Chae JH, Kim TS. Decreased cardiovascular death in schizophrenia patients treated with antipsychotics: a Korean national cohort study. Schizophr Res. 2021;228:417–24.
Correll C, Solmi M, Croatto G, Schneider L, Rohani-Montez S, Fairley L, et al. Mortality in people with schizophrenia: a systematic review and meta-analysis of relative risk and aggravating or attenuating factors. World Psychiatry. 2022;21:248–71.
Lähteenvuo M, Tanskanen A, Taipale H, Hoti F, Vattulainen P, Vieta E, et al. Real-world effectiveness of pharmacologic treatments for the prevention of rehospitalization in a Finnish nationwide cohort of patients with bipolar disorder. JAMA Psychiatry. 2018;75:347–55.
Brandt L, Bschor T, Henssler J, Muller M, Hasan A, Heinz A, et al. Antipsychotic withdrawal symptoms: a systematic review and meta-analysis. Front Psychiatry. 2020;11:569912.
Cosci F, Chouinard G. Acute and persistent withdrawal syndromes following discontinuation of psychotropic medications. Psychother Psychosom. 2020;89:283–306.
Alvarez-Jimenez M, Parker AG, Hetrick SE, McGorry PD, Gleeson JF. Preventing the second episode: a systematic review and meta-analysis of psychosocial and pharmacological trials in first-episode psychosis. Schizophr Bull. 2011;37:619–30.
Alvarez-Jimenez M, O’Donoghue B, Thompson A, Gleeson JF, Bendall S, Gonzalez-Blanch C, et al. Beyond clinical remission in first episode psychosis: thoughts on antipsychotic maintenance vs. guided discontinuation in the functional recovery era. CNS Drugs. 2016;30:357–68.
Bogers JPAM, Hambarian G, Walburgh Schmidt N, Vermeulen JM, de Haan L. Risk factors for psychotic relapse after dose reduction or discontinuation of antipsychotics in patients with chronic schizophrenia: a systematic review and meta-analysis. Schizophr Bull Open. 2022;1:11–23.
Brandt L, Ritter K, Schneider-Thoma J, Siafis S, Montag C, Ayrilmaz H, et al. Predicting psychotic relapse following randomised discontinuation of paliperidone in individuals with schizophrenia or schizoaffective disorder: an individual participant data analysis. Lancet Psychiatry. 2023;10:184–96.
Shimomura Y, Kikuchi Y, Suzuki T, Uchida H, Mimura M, Takeuchi H. Antipsychotic treatment in the maintenance phase of schizophrenia: an updated systematic review of the guidelines and algorithms. Schizophr Res. 2020;215:8–16.
Tiihonen J, Tanskanen A, Taipale H. 20-year nationwide follow-up study on discontinuation of antipsychotic treatment in first-episode schizophrenia. Am J Psychiatry. 2018;175:765–73.
Luykx JJ, Stam N, Tanskanen A, Tiihonen J, Taipale H. In the aftermath of clozapine discontinuation: comparative effectiveness and safety of antipsychotics in patients with schizophrenia who discontinue clozapine. Br J Psychiatry. 2020;217:498–505.
Horowitz MA, Jauhar S, Natesan S, Murray RM, Taylor D. A method for tapering antipsychotic treatment that may minimize the risk of relapse. Schizophr Bull. 2021;47:1116–29.
Brandt L, Schneider-Thoma J, Siafis S, Efthimiou O, Bermpohl F, Loncar L, et al. Adverse events after antipsychotic discontinuation: an individual participant data meta-analysis. Lancet Psychiatry. 2022;9:232–42.
Tani H, Takasu S, Uchida H, Suzuki T, Mimura M, Takeuchi H. Factors associated with successful antipsychotic dose reduction in schizophrenia: a systematic review of prospective clinical trials and meta-analysis of randomized controlled trials. Neuropsychopharmacology. 2020;45:887–901.
Leucht S, Bauer S, Siafis S, Hamza T, Wu H, Schneider-Thoma J, et al. Examination of dosing of antipsychotic drugs for relapse prevention in patients with stable schizophrenia: a meta-analysis. JAMA Psychiatry. 2021;78:1238–48.
Wunderink L, Nieboer RM, Wiersma D, Sytema S, Nienhuis FJ. Recovery in remitted first-episode psychosis at 7 years of follow-up of an early dose reduction/discontinuation or maintenance treatment strategy: long-term follow-up of a 2-year randomized clinical trial. JAMA Psychiatry. 2013;70:913–20.
Omachi Y, Sumiyoshi T. Dose reduction/discontinuation of antipsychotic drugs in psychosis; effect on cognition and functional outcomes. Front Psychiatry. 2018;9:447.
Weller A, Gleeson J, Alvarez-Jimenez M, McGorry P, Nelson B, Allott K, et al. Can antipsychotic dose reduction lead to better functional recovery in first-episode psychosis? A randomized controlled-trial of antipsychotic dose reduction. The reduce trial: study protocol. Early Inter Psychiatry. 2019;13:1345–56.
Begemann MJH, Thompson IA, Veling W, Gangadin SS, Geraets CNW, van‘t Hag E, et al. To continue or not to continue? Antipsychotic medication maintenance versus dose-reduction/discontinuation in first episode psychosis: HAMLETT, a pragmatic multicenter single-blind randomized controlled trial. Trials. 2020;21:147.
Liu CC, Hsieh MH, Chien YL, Liu CM, Lin YT, Hwang TJ, et al. Protocol of guided antipsychotic reduction to reach minimum effective dose (GARMED) in patients with remitted psychosis based on pragmatic design. Early Inter Psychiatry. 2021;16:178–85.
Remington G, Kapur S. Antipsychotic dosing: how much but also how often? Schizophr Bull. 2010;36:900–3.
Gaebel W. Intermittent medication—an alternative? Acta Psychiatr Scand Suppl. 1994;382:33–8.
Horowitz MA, Moncrieff J, de Haan L, Bogers J, Gangadin SS, Kikkert M, et al. Tapering antipsychotic medication: practical considerations. Psychol Med. 2022;52:32–35.
Qureshi MM, Young AH. Hamlet’s augury: how to manage discontinuation of mood stabilizers in bipolar disorder. Ther Adv Psychopharmacol. 2021;11:20451253211000612.
Murru A, Colom F, Nivoli A, Pacchiarotti I, Valenti M, Vieta E. When should mood stabilizers be withdrawn due to lack of efficacy? Some methodological considerations. Eur Psychiatry. 2011;26:183–6.
Biel MG, Peselow E, Mulcare L, Case BG, Fieve R. Continuation versus discontinuation of lithium in recurrent bipolar illness: a naturalistic study. Bipolar Disord. 2007;9:435–42.
Baldessarini RJ, Tondo L, Hennen J. Effects of lithium treatment and its discontinuation on suicidal behavior in bipolar manic-depressive disorders. J Clin Psychiatry. 1999;60:77–84.
Kishi T, Matsuda Y, Sakuma K, Okuya M, Mishima K, Iwata N. Recurrence rates in stable bipolar disorder patients after drug discontinuation v. drug maintenance: a systematic review and meta-analysis. Psychol Med. 2021;51:2721–9.
Gutwinski S, Fierley L, Schreiter S, Bermpohl F, Heinz A, Henssler J. Lithium withdrawal symptoms—a systematic review. Psychiatr Prax. 2021;48:341–50.
Faedda GL, Tondo L, Baldessarini RJ, Suppes T, Tohen M. Outcome after rapid vs gradual discontinuation of lithium treatment in bipolar disorders. Arch Gen Psychiatry. 1993;50:448–55.
de Vries C, van Bergen A, Regeer EJ, Benthem E, Kupka RW, Boks MP. The effectiveness of restarted lithium treatment after discontinuation: reviewing the evidence for discontinuation-induced refractoriness. Bipolar Disord. 2013;15:645–9.
Yatham LN, Kennedy SH, Parikh SV, Schaffer A, Bond DJ, Frey BN, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018;20:97–170.
Tohen M, Frank E, Bowden CL, Colom F, Ghaemi SN, Yatham LN, et al. The International Society for Bipolar Disorders (ISBD) Task Force report on the nomenclature of course and outcome in bipolar disorders. Bipolar Disord. 2009;11:453–73.
Taylor D, Barnes T, Young A. Maudsley prescribing guidelines in psychiatry. 14th ed. New York, NY: Wiley Blackwell; 2021.
Holm M, Tanskanen A, Lähteenvuo M, Tiihonen J, Taipale H. Comparative effectiveness of mood stabilizers and antipsychotics in the prevention of hospitalization after lithium discontinuation in bipolar disorder. Eur Neurpscyhopharmacol. 2022;61:36–42.
Nolen WA, Licht RW, Young AH, Malhi GS, Tohen M, Vieta E, et al. What is the optimal serum level for lithium in the maintenance treatment of bipolar disorder? A systematic review and recommendations from the ISBD/IGSLI Task Force on treatment with lithium. Bipolar Disord. 2019;21:394–409.
Ribeiro PRS, Schlindwein AD. Benzodiazepine deprescription strategies in chronic users: a systematic review. Fam Pr. 2021;38:684–93.
Reeve E, Ong M, Wu A, Jansen J, Petrovic M, Gnjidic D. A systematic review of interventions to deprescribe benzodiazepines and other hypnotics among older people. Eur J Clin Pharm. 2017;73:927–35.
Voshaar RC, Couvee JE, van Balkom AJ, Mulder PG, Zitman FG. Strategies for discontinuing long-term benzodiazepine use: meta-analysis. Br J Psychiatry. 2006;189:213–20.
Jobert A, Laforgue EJ, Grall-Bronnec M, Rousselet M, Pere M, Jolliet P, et al. Benzodiazepine withdrawal in older people: what is the prevalence, what are the signs, and which patients? Eur J Clin Pharm. 2021;77:171–7.
Inoue Y, Takaesu Y, Koebis M. Prevalence of and factors associated with acute withdrawal symptoms after 24 weeks of eszopiclone treatment in patients with chronic insomnia: a prospective, interventional study. BMC Psychiatry. 2021;21:193.
Lader M, Kyriacou A. Withdrawing benzodiazepines in patients with anxiety disorders. Curr Psychiatry Rep. 2016;18:8.
Darker CD, Sweeney BP, Barry JM, Farrell MF, Donnelly-Swift E. Psychosocial interventions for benzodiazepine harmful use, abuse or dependence. Cochrane Database Syst Rev. 2015(5):CD009652.
Petursson H. The benzodiazepine withdrawal syndrome. Addiction. 1994;89:1455–9.
Basinska-Szafranska A. Delayed crises following benzodiazepine withdrawal: deficient adaptive mechanisms or simple pharmacokinetics? Detoxification assisted by serum-benzodiazepine elimination tracking. Eur J Clin Pharm. 2022;78:101–10.
Rickels K, Schweizer E, Case WG, Greenblatt DJ. Long-term therapeutic use of benzodiazepines. I. Effects of abrupt discontinuation. Arch Gen Psychiatry. 1990;47:899–907.
Schweizer E, Rickels K. Benzodiazepine dependence and withdrawal: a review of the syndrome and its clinical management. Acta Psychiatr Scand Suppl. 1998;393:95–101.
Rasmussen AF, Poulsen SS, Oldenburg LIK, Vermehren C. The barriers and facilitators of different stakeholders when deprescribing benzodiazepine receptor agonists in older patients—a systematic review. Metabolites. 2021;11:254.
Baandrup L, Ebdrup BH, Rasmussen JO, Lindschou J, Gluud C, Glenthoj BY. Pharmacological interventions for benzodiazepine discontinuation in chronic benzodiazepine users. Cochrane Database Syst Rev. 2018;3:CD011481.
Vinkers CH, Olivier B. Mechanisms underlying tolerance after long-term benzodiazepine use: a future for subtype-selective GABA(A) receptor modulators? Adv Pharm Sci. 2012;2012:416864.
Lader M, Tylee A, Donoghue J. Withdrawing benzodiazepines in primary care. CNS Drugs. 2009;23:19–34.
Clinical Guidelines on Drug Misuse and Dependence Update 2017 Independent Expert Working Group. Drug misuse and dependence: UK guidelines on clinical management. London: Department of Health; 2017.
Brouillet E, Chavoix C, Bottlaender M, Khalili-Varasteh M, Hantraye P, Fournier D, et al. In vivo bidirectional modulatory effect of benzodiazepine receptor ligands on GABAergic transmission evaluated by positron emission tomography in non-human primates. Brain Res. 1991;557:167–76.
Lingford-Hughes AR, Welch S, Peters L, Nutt DJ. British Association for Psychopharmacology ERG. BAP updated guidelines: evidence-based guidelines for the pharmacological management of substance abuse, harmful use, addiction and comorbidity: recommendations from BAP. J Psychopharmacol. 2012;26:899–952.
Soyka M. Treatment of benzodiazepine dependence. N Engl J Med. 2017;376:1147–57.
Takaesu Y, Utsumi T, Okajima I, Shimura A, Kotorii N, Kuriyama K, et al. Psychosocial intervention for discontinuing benzodiazepine hypnotics in patients with chronic insomnia: a systematic review and meta-analysis. Sleep Med Rev. 2019;48:101214.
Gould RL, Coulson MC, Patel N, Highton-Williamson E, Howard RJ. Interventions for reducing benzodiazepine use in older people: meta-analysis of randomised controlled trials. Br J Psychiatry. 2014;204:98–107.
Lynch T, Ryan C, Hughes CM, Presseau J, van Allen ZM, Bradley CP, et al. Brief interventions targeting long-term benzodiazepine and Z-drug use in primary care: a systematic review and meta-analysis. Addiction. 2020;115:1618–39.
Mugunthan K, McGuire T, Glasziou P. Minimal interventions to decrease long-term use of benzodiazepines in primary care: a systematic review and meta-analysis. Br J Gen Pr. 2011;61:e573–8.
Parr JM, Kavanagh DJ, Cahill L, Mitchell G, Mc DYR. Effectiveness of current treatment approaches for benzodiazepine discontinuation: a meta-analysis. Addiction. 2009;104:13–24.
Gallo AT, Hulse G. Pharmacological uses of flumazenil in benzodiazepine use disorders: a systematic review of limited data. J Psychopharmacol. 2021;35:211–20.
MacDonald T, Gallo AT, Basso-Hulse G, Hulse GK. Outcomes of patients treated with low-dose flumazenil for benzodiazepine detoxification: a description of 26 participants. Drug Alcohol Depend. 2022;237:109517.
Manchikanti L, Vallejo R, Manchikanti KN, Benyamin RM, Datta S, Christo PJ. Effectiveness of long-term opioid therapy for chronic non-cancer pain. Pain Physician. 2011;14:E133–56.
Abdel Shaheed C, Maher CG, Williams KA, Day R, McLachlan AJ. Efficacy, tolerability, and dose-dependent effects of opioid analgesics for low back pain: a systematic review and meta-analysis. JAMA Intern Med. 2016;176:958–68.
Busse JW, Wang L, Kamaleldin M, Craigie S, Riva JJ, Montoya L, et al. Opioids for chronic noncancer pain: a systematic review and meta-analysis. JAMA. 2018;320:2448–60.
van Rijswijk SM, van Beek M, Schoof GM, Schene AH, Steegers M, Schellekens AF. Iatrogenic opioid use disorder, chronic pain and psychiatric comorbidity: a systematic review. Gen Hosp Psychiatry. 2019;59:37–50.
Griffin ML, Bennett HE, Fitzmaurice GM, Hill KP, Provost SE, Weiss RD. Health-related quality of life among prescription opioid-dependent patients: results from a multi-site study. Am J Addict. 2015;24:308–14.
Higgins C, Smith BH, Matthews K. Incidence of iatrogenic opioid dependence or abuse in patients with pain who were exposed to opioid analgesic therapy: a systematic review and meta-analysis. Br J Anaesth. 2018;120:1335–44.
Smyth BP, Barry J, Keenan E, Ducray K. Lapse and relapse following inpatient treatment of opiate dependence. Ir Med J. 2010;103:176–9.
Huffman KL, Sweis GW, Gase A, Scheman J, Covington EC. Opioid use 12 months following interdisciplinary pain rehabilitation with weaning. Pain Med. 2013;14:1908–17.
Bruneau J, Ahamad K, Goyer M, Poulin G, Selby P, Fischer B, et al. Management of opioid use disorders: a national clinical practice guideline. CMAJ. 2018;190:E247–57.
Frank JW, Lovejoy TI, Becker WC, Morasco BJ, Koenig CJ, Hoffecker L, et al. Patient outcomes in dose reduction or discontinuation of long-term opioid therapy: a systematic review. Ann Intern Med. 2017;167:181–91.
Tsui JI, Lira MC, Cheng DM, Winter MR, Alford DP, Liebschutz JM, et al. Chronic pain, craving, and illicit opioid use among patients receiving opioid agonist therapy. Drug Alcohol Depend. 2016;166:26–31.
Duceppe MA, Perreault MM, Frenette AJ, Burry LD, Rico P, Lavoie A, et al. Frequency, risk factors and symptomatology of iatrogenic withdrawal from opioids and benzodiazepines in critically Ill neonates, children and adults: a systematic review of clinical studies. J Clin Pharm Ther. 2019;44:148–56.
Bienek N, Maier C, Kaisler M, Michel-Lauter B, Schwarzer A, Meyer-Frießem CH. Intensity of withdrawal symptoms during opioid taper in patients with chronic pain-individualized or fixed starting dosage? Pain Med. 2019;20:2438–49.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, DC: American Psychiatric Publishing; 2013.
Kosten TR, Baxter LE. Review article: effective management of opioid withdrawal symptoms: a gateway to opioid dependence treatment. Am J Addict. 2019;28:55–62.
Mark TL, Parish W. Opioid medication discontinuation and risk of adverse opioid-related health care events. J Subst Abus Treat. 2019;103:58–63.
Mackey K, Anderson J, Bourne D, Chen E, Peterson K. Benefits and harms of long-term opioid dose reduction or discontinuation in patients with chronic pain: a rapid review. J Gen Intern Med. 2020;35:935–44.
Demidenko MI, Dobscha SK, Morasco BJ, Meath THA, Ilgen MA, Lovejoy TI. Suicidal ideation and suicidal self-directed violence following clinician-initiated prescription opioid discontinuation among long-term opioid users. Gen Hosp Psychiatry. 2017;47:29–35.
Quinn PD, Chang Z, Bair MJ, Rickert ME, Gibbons RD, Kroenke K, et al. Associations of opioid prescription dose and discontinuation with risk of substance-related morbidity in long-term opioid therapy. Pain. 2021;163:e588–95.
Binswanger IA, Glanz JM, Faul M, Shoup JA, Quintana LM, Lyden J, et al. The association between opioid discontinuation and heroin use: a nested case-control study. Drug Alcohol Depend. 2020;217:108248.
Pergolizzi JV Jr, Rosenblatt M, Mariano DJ, Bisney J. Tapering opioid therapy: clinical strategies. Pain Manag. 2018;8:409–13.
Davis MP, Digwood G, Mehta Z, McPherson ML. Tapering opioids: a comprehensive qualitative review. Ann Palliat Med. 2020;9:586–610.
Minegishi T, Garrido MM, Stein M, Oliva EM, Frakt AB. Opioid discontinuation among patients receiving high-dose long-term opioid therapy in the veterans health administration. J Gen Intern Med. 2020;35:903–9.
Campbell G, Bruno R, Darke S, Degenhardt L. Associations of borderline personality with pain, problems with medications and suicidality in a community sample of chronic non-cancer pain patients prescribed opioids for pain. Gen Hosp Psychiatry. 2015;37:434–40.
Scherrer JF, Salas J, Sullivan MD, Ahmedani BK, Copeland LA, Bucholz KK, et al. Impact of adherence to antidepressants on long-term prescription opioid use cessation. Br J Psychiatry. 2018;212:103–11.
Mercadante S, Arcuri E, Santoni A. Opioid-induced tolerance and hyperalgesia. CNS Drugs. 2019;33:943–55.
US Department of Health and Human Services. HHS guide for clinicians on the appropriate dosage reduction or discontinuation of long-term opioid analgesics. 2019. https://www.drugabuse.gov/nidamed-medical-health-professionals/opioid-crisis-pain-management/hhs-guide-clinicians-appropriate-dosage-reduction-or-discontinuation-long-term-opioid.
US Department of Veterans Affairs. Pain management opioid taper decision tool; a VA clinician’s Guide. 2016. http://www.pbm.va.gov/PBM/academicdetailingservicehome.asp.
Kaye AD, Jones MR, Kaye AM, Ripoll JG, Galan V, Beakley BD, et al. Prescription opioid abuse in chronic pain: an updated review of opioid abuse predictors and strategies to curb opioid abuse: part 1. Pain Physician. 2017;20:S93–109.
Noble M, Treadwell JR, Tregear SJ, Coates VH, Wiffen PJ, Akafomo C, et al. Long-term opioid management for chronic noncancer pain. Cochrane Database Syst Rev. 2010;2010:Cd006605.
Dijkstra B, Van Oort M, Schellekens A, De Haan H, De Jong C. Dutch guidelines on detoxification of psychoactive substances. Amsterfoort: Resultaten Scoren; 2017.
Tripp CC, Rak E, Burker E. A review of effective treatments for patients with co-occurring chronic pain and opioid addiction. VISTAS Online. 2017.
Lohr WD, Wanta JW, Baker M, Grudnikoff E, Morgan W, Chhabra D, et al. Intentional discontinuation of psychostimulants used to treat ADHD in youth: a review and analysis. Front Psychiatry. 2021;12:642798.
Zeiner P. Do the beneficial effects of extended methylphenidate treatment in boys with attention-deficit hyperactivity disorder dissipate rapidly during placebo treatment? Nord J Psychiatry. 1999;53:55–60.
Arnold LE, Lindsay RL, Conners CK, Wigal SB, Levine AJ, Johnson DE, et al. A double-blind, placebo-controlled withdrawal trial of dexmethylphenidate hydrochloride in children with attention deficit hyperactivity disorder. J Child Adolesc Psychopharmacol. 2004;14:542–54.
Coghill DR, Banaschewski T, Lecendreux M, Johnson M, Zuddas A, Anderson CS, et al. Maintenance of efficacy of lisdexamfetamine dimesylate in children and adolescents with attention-deficit/hyperactivity disorder: randomized-withdrawal study design. J Am Acad Child Adolesc Psychiatry. 2014;53:647–e51.
Howland RH. Potential adverse effects of discontinuing psychotropic drugs. J Psychosoc Nurs Ment health Serv. 2010;48:11–4.
Tsujii N, Okada T, Usami M, Kuwabara H, Fujita J, Negoro H, et al. Effect of continuing and discontinuing medications on quality of life after symptomatic remission in attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. J Clin Psychiatry. 2020;81:19r13015.
National Guideline Center. Attention deficit hyperactivity disorder: diagnosis and management. London: National Institute for Health and Care Excellence (NICE); 2019.
Pliszka S. Issues AWGoQ. Practice parameter for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2007;46:894–921.
Faraone SV, Banaschewski T, Coghill D, Zheng Y, Biederman J, Bellgrove MA, et al. The World Federation of ADHD International Consensus Statement: 208 evidence-based conclusions about the disorder. Neurosci Biobehav Rev. 2021;128:789–818.
Sandler AD, Glesne CE, Bodfish JW. Conditioned placebo dose reduction: a new treatment in attention-deficit hyperactivity disorder? J Dev Behav Pediatr. 2010;31:369–75.
National Guideline Centre (UK). Withdrawal from pharmacological treatment and drug holidays: attention deficit hyperactivity disorder: diagnosis and management: evidence review I. London: National Institute for Health and Care Excellence (NICE); 2018.
World Health Organization. Clinical guidelines for withdrawal management and treatment of drug dependence in closed settings. Geneva: World Health Organization; 2009.
Vinkers CH, Ruhe HG, Penninx BW. Antidepressant discontinuation: in need of scientific evidence. J Clin Psychopharmacol. 2021;41:512–5.
Wentink C, Huijbers MJ, Lucassen PL, van der Gouw A, Kramers C, Spijker J, et al. Enhancing shared decision making about discontinuation of antidepressant medication: a concept-mapping study in primary and secondary mental health care. Br J Gen Pr. 2019;69:e777–85.
Desai M, Park T. Deprescribing practices in Canada: a scoping review. Can Pharm J. 2022;155:249–57.
Grootens K, Verwijmeren D. A shared decision journey to bridge the gap between treatment recommendation and low adherence? Eur Neuropsychopharmacol. 2023;69:77–8.
Horowitz M, Taylor D. How to reduce and stop psychiatric medication. Eur Neuropsychopharmacol. 2022;55:4–7.
Quilichini JB, Revet A, Garcia P, Bouquie R, Hamard J, Yrondi A, et al. Comparative effects of 15 antidepressants on the risk of withdrawal syndrome: a real-world study using the WHO pharmacovigilance database. J Affect Disord. 2022;297:189–93.
Kuyken W, Hayes R, Barrett B, Byng R, Dalgleish T, Kessler D, et al. Effectiveness and cost-effectiveness of mindfulness-based cognitive therapy compared with maintenance antidepressant treatment in the prevention of depressive relapse or recurrence (PREVENT): a randomised controlled trial. Lancet. 2015;386:63–73.
Uhlenhuth EH, Balter MB, Ban TA, Yang K. International study of expert judgment on therapeutic use of benzodiazepines and other psychotherapeutic medications: IV. Therapeutic dose dependence and abuse liability of benzodiazepines in the long-term treatment of anxiety disorders. J Clin Psychopharmacol. 1999;19:23S–9S.
Gowing L, Farrell M, Ali R, White JM. Alpha(2)-adrenergic agonists for the management of opioid withdrawal. Cochrane Database Syst Rev. 2016;2016:CD002024.
Author information
Authors and Affiliations
Contributions
The authors confirm contribution to the paper as follows: study conceptualization and design: CV and JL; data collection: CV, RK, BP, HR, JG, PH, AS, SJ, JR, EV, JT, SV, WV, RV, LW, and JL; analysis and interpretation of results: CV, RK, HR, JG, PH, AS, SJ, JR, EV, JT, SV, WV, RV, LW, and JL; draft manuscript preparation: CV, RK, HR, JG, PH, AS, JT, SV, WV, RV, LW, and JL; draft review and editing: BP, SJ, JR, and EV. All authors reviewed the results and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
CV received research funding from ZonMW, Hersenstichting. HR received research funding from ZonMW, Hersenstichting, an unrestricted educational grant from Janssen and speaking fees from Janssen, Prelum, Benecke and Lundbeck. CV and HR are PIs of the TEMPO RCT examining different discontinuation strategies. SJ has received honoraria for educational talks given for Lundbeck, Boehringer-Ingelheim, Janssen and Sunovion. He has consulted for LLA Pharmaceuticals on an antipsychotic and has sat as panel member for a Wellcome Trust funding panel and expert member for a NICE panel on tardive dyskinesia. He is a Council Member for the British Association for Psychopharmacology (unpaid). JT has participated in research projects funded by grants from Janssen-Cilag and Eli Lilly to his employing institution. He has been a consultant to HLS Therapeutics, Janssen, Orion and WebMed Global and received lecture fees from Janssen and Otsuka. JR was on the speakers’ bureau and/or acted as consultant for Biogen, Janssen-Cilag, Novartis, Shire, Takeda, Bial, Shionogi, Sincrolab, Novartis, BMS, Medice, Rubió, Uriach, Technofarma and Raffo in the last 3 years. He also received travel awards (air tickets + hotel) for taking part in psychiatric meetings from Janssen-Cilag, Rubió, Shire, Takeda, Shionogi, Bial and Medice. The Department of Psychiatry chaired by him received unrestricted educational and research support from the following companies in the last 3 years: Janssen-Cilag, Shire, Oryzon, Roche, Psious, and Rubió. EV has received grants and served as consultant, advisor or CME speaker for the following entities (unrelated to the present work): AB-Biotics, Abbott, Abbvie, Aimentia, Angelini, Biogen, Biohaven, Boehringer-Ingelheim, Casen-Recordati, Celon, Compass, Dainippon Sumitomo Pharma, Ethypharm, Ferrer, Gedeon Richter, GH Research, Glaxo Smith-Kline, Idorsia, Janssen, Lundbeck, Novartis, Organon, Otsuka, Rovi, Sage, Sanofi-Aventis, Sunovion, Takeda, and Viatris. RV, LW, WV, AS, SV, JL, BP, JG, RK, and PH have no conflict of interests to declare.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Vinkers, C.H., Kupka, R.W., Penninx, B.W. et al. Discontinuation of psychotropic medication: a synthesis of evidence across medication classes. Mol Psychiatry 29, 2575–2586 (2024). https://doi.org/10.1038/s41380-024-02445-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41380-024-02445-4

{kind=link}