
Abstract
Diagnostic criteria for hypoplastic myelodysplasic syndrome (h-MDS) have not been clearly established, making the differential diagnosis from other bone marrow failure syndromes (BMF) challenging. In this study, we aimed to delineate clinical, histopathological, and molecular features of h-MDS, based on a large and well-annotated cohort of patients with bone marrow (BM) hypocellularity. The study included 534 consecutive adult patients with hypocellular BM (278 h-MDS and 136 aplastic anemia), and 727 with normo- or hypercellular MDS (n-MDS). Comparison of clinical features of patients with h-MDS as defined by BM cellularity ≤25% (n = 204) or reduced age-adjusted cellularity (n = 74) did not reveal significant differences. We developed a diagnostic score to discriminate h-MDS from non-malignant BMF based on histological and cytological variables with the highest specificity for MDS (h-score). The information from chromosomal abnormalities and somatic mutation patterns was then integrated into a cyto-histological/genetic score (hg-score). This score was able to segregate two groups of h-MDS with a significantly different risk of blast progression (P < 0.001). The integration of cyto-histological and genetic features in adult patients with hypocellular BM facilitated segregation into two distinct groups, one with clinical and genetic features highly consistent with myeloid neoplasm, and one with features more consistent with non-malignant BMF.
Similar content being viewed by others


Introduction
Myelodysplastic syndromes (MDS) are clonal hematopoietic stem cell disorders characterized by ineffective erythropoiesis, dysplasia involving one or more cell lineages, peripheral cytopenia, and increased risk of transformation to acute myeloid leukemia (AML). [1] In most cases, MDS patients exhibit a normo- or hypercellular bone marrow (BM), whereas 10–20% of cases present a decreased bone marrow cellularity. [2,3,4,5] This group is referred to as hypoplastic MDS (h-MDS) in the World Health Organization (WHO) classification of myeloid neoplasm, without being recognized as a distinct MDS subtype. [6]
A higher response rate to immunosuppressive therapy has been reported in hypoplastic MDS (h-MDS) compared with normo-hypercellular MDS (n-MDS). [7,8,9] However, precise diagnostic criteria for h-MDS have not been clearly defined and conflicting data on clinico-pathological characteristics and prognosis of h-MDS have been reported. [2,3,4,5, 9,10,11,12] Foremost, this uncertainty encompasses the actual definition of BM hypocellularity. In fact, a cutoff value of 20–30% cellularity has been derived from aplastic anemia (AA) [13] and applied to the definition of h-MDS. [4, 7, 9, 11, 12] However, this threshold does not account for age-related changes, resulting in an uncertain classification of younger MDS patients. In addition, the definition of hypocellularity appears problematic in the elderly population of MDS patients in whom these values partly overlap with the wide range of age-related changes. [5, 14, 15]
Hypocellularity in MDS may lead to difficulties in the differential diagnosis with other bone marrow failure syndromes (BMF), especially AA and congenital BMF (c-BMF). [2, 16,17,18,19,20] In routine clinical practice, this distinction is even more challenging in the frequent cases of inadequate diagnostic specimens. [21]
Recurrent somatic mutations in multiple genes have been reported in MDS. [22, 23] However, recent studies have shown that mutations in some of these genes are commonly acquired in hematopoietic cells during aging without being associated with a hematologic phenotype. [24,25,26,27] In addition, mutations in genes recurrently mutated in MDS have been detected in patients with AA without evidence of myeloid neoplasm. [28,29,30,31] So far, few genetic studies have focused on h-MDS, without firm conclusion. [32,33,34,35]
In a recent study on patients with unexplained cytopenia, including MDS and AA, we found that mutation profiling has a high predictive value for identifying individuals with a myeloid neoplasm. [36] In particular, selected mutation patterns were proven highly specific for myeloid neoplasms with myelodysplasia, which may possibly identify bona fide MDS even in the absence of definitive morphological features, as previously acknowledged for selected cytogenetic abnormalities. [36]
In this work, based on a large and well-annotated cohort of consecutive patients with BM hypocellularity from two reference centers, we aimed to define the clinical and histopathological features of h-MDS, and to elucidate the role of genetic profiles in discriminating malignant and non-malignant BMF in elderly individuals.
Methods
Patients’ characteristics and clinical procedures
This study included 1261 consecutive adult patients investigated at the IRCCS Policlinico San Matteo & University of Pavia, Italy and King’s College Hospital, London, UK. The study was approved by the respective Local Research Ethics Committees. The procedures followed were in accordance with the Declaration of Helsinki of 1975, as revised in 2000, and samples were obtained after patients provided written informed consent.
Age-adjusted bone marrow cellularity was assessed on bone marrow trephine according to European consensus. [14] Diagnostic procedures aimed at distinguishing myeloid neoplasms from reactive causes of cytopenia or other hematologic disorders were in accord to recent recommendations. [21, 37, 38] The diagnosis of myeloid neoplasm and the differentiation between h-MDS and AA was in accord to the criteria of the WHO classification of myeloid neoplasms, as well as current standards and recommendations. [2, 13, 39] Paroxysmal nocturnal hemoglobinuria (PNH) clones were detected according to standard guidelines. [40] Idiopathic cytopenia of undetermined significance (ICUS) was defined as previously reported. [41] Peripheral blood and bone marrow specimens were analyzed by two independent hematopathologists who were blinded to clinical data. Discordant results were resolved by a joint review of the specimens. [42] Clinical features of patients included in the study are reported in Table 1: 534 patients had a hypocellular BM, including 204 MDS with BM cellularity ≤25% and 74 with reduced age-adjusted cellularity, 136 AA, 96 ICUS and 24 c-BMF (2 Fanconi Anemia, 1 Diamond-Blackfan Anemia, 1 germline RUNX1 mutation, 4 typical Dyskeratosis Congenita, 16 Telomeropathy unspecified), whereas 727 patients had a normo- or hypercellular MDS (n-MDS).
Mutation analysis
A core panel of 24 genes selected on the basis of prior implication in the pathogenesis of myeloid disorders was analyzed in the whole study cohort (Supplemental Table 1). Details of the sequencing analysis and functional annotation of variants are provided in the Supplemental Material. [36]
Statistical analysis
All the statistical analyses were performed using the Stata SE 12.1 (StataCorp LP, College Station, TX, http://www.stata.com) software. Full details of the statistical analysis are reported in the Methods section of the Supplemental Material.
Results
Clinical correlates of absolute and age-adjusted reduced BM cellularity in MDS
In order to define consistent criteria for BM hypocellularity, we identified two subsets of patients with potentially conflicting BM cellularity estimates based on either an absolute cutoff value and age-adjusted reference ranges: younger patients with BM cellularity reduced for their age but > 25%; and elderly individuals with a BM cellularity ≤25% but consistent with their age-adjusted reference ranges.
We first compared clinical features and outcomes of patients with a BM cellularity reduced for their age but > 25% (age 17–61 years, n = 74) with those of patients with h-MDS as defined by BM cellularity ≤25% (age 20–87 years, n = 204). Patients with reduced age-adjusted cellularity were, as expected, younger compared with those with BM cellularity ≤25% (P < 0.001), and had a higher female prevalence (58 vs 44%, P = 0.033). Conversely, no significant differences were found between these two groups in clinical and hematological variables (P values ranging from 0.91 to 0.11), except for a marginally higher reticulocyte count in patients with reduced age-adjusted cellularity compared with those with BM cellularity ≤25% (63 × 109/L vs 42 × 109/L, P = .025) (Supplemental Table 2). In addition, no significant difference in overall survival (OS) (P = 0.94) and cumulative incidence (CI) of AML evolution (P = 0.77) were observed between patients with reduced age-adjusted cellularity and those with BM cellularity ≤25% (Supplemental Fig. 1). These results were confirmed in multivariable analyses including demographic and disease-related prognostic factors (Supplemental Table 3). Comparable results were obtained when this analysis was restricted to patients younger than 65 years of age (BM cellularity ≤25%: n = 114 vs BM cellularity reduced for age but >25%: n = 74). These findings suggest that, in younger MDS patients, a reduced age-adjusted BM cellularity identifies a group with homogeneous features irrespective of the threshold of 25% cellularity.
Then, we identified 52 patients aged 65 year or older with a BM cellularity ≤25% but consistent with their age-adjusted cellularity reference ranges. [14] When comparing clinical and hematological features of this subset of patients with those of age-matched individuals with a BM cellularity ≤25% and reduced by age-adjusted criteria, no significant difference were observed (P values ranging from 0.06 to 0.83) (Supplemental Table 4), suggesting that a BM cellularity ≤25% in elderly patients identifies a group with homogeneous clinical features and outcomes, and may represent a consistent criterion to define BM hypocellularity.
Taken together, these data suggest that a combined criterion of BM cellularity reduced according age-adjusted reference ranges or ≤25% can be adopted to define h-MDS.
Clinical features and outcome of patients with hypoplastic MDS
Patients with h-MDS as defined by reduced age-adjusted BM cellularity and/or BM cellularity ≤25% (n = 278) were significantly younger, displayed lower percentage of BM blasts, ring sideroblasts (RS) and CD34 + cells as determined by immunohistochemistry (IHC) compared with n-MDS (P values from < 0.001 to 0.01) (Table 2 and Supplemental Fig. 2). A significantly higher prevalence of PNH clones was observed in h-MDS compared with n-MDS (24% vs 2%, P < 0.001). Compared with AA, h-MDS showed a significantly higher percentage of RS, BM blasts, dysmegakaryopoiesis, and dysgranulopoiesis, BM fibrosis, clusters of CD34 + cells, and chromosomal abnormalities (P values from < 0.001 to 0.004) (Table 2).
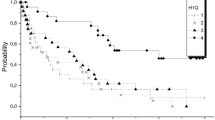
Patients with h-MDS showed a significantly different OS compared with n-MDS and AA (P = 0.001). Two-group comparisons showed that h-MDS had a significantly worse OS compared with AA (P = 0.007), and a marginally better OS compared with n-MDS (P = 0.05) (Fig. 1). Conversely, patients with h-MDS showed a significantly lower CI of leukemic evolution compared with n-MDS (P = 0.001), and a significantly higher CI compared with AA (P < 0.001) (Fig. 1).

Overall survival and cumulative incidence of progression into acute myeloid leukemia of patients with hypoplastic MDS, normo- or hypercellular MDS, and aplastic anemia. Plots A and B report, respectively, overall survival and cumulative incidence of AML evolution of patients with hypoplastic MDS (red curve), as defined by reduced age-adjusted cellularity and/or BM cellularity ≤25%, normo- or hypercellular MDS (blue curve), and aplastic anemia (green curve)
Cytological and histological variables of discriminant value in hypoplastic MDS and non-malignant BMF
Next, we aimed to identify cytological and histological parameters potentially useful to differentiate h-MDS from non-neoplastic BMF, including AA and c-BMF. To this purpose, we first calculated the specificity for MDS of the most relevant bone marrow variables in either the whole population (MDS and non-neoplastic BMF) or in the population of patients with hypocellular bone marrow (h-MDS and non-neoplastic BMF) (Supplemental Table 5 and Supplemental Fig. 3). The following categorical variables showed a specificity for MDS higher than 0.95: BM blasts or CD34 + cells 3–4% or ≥ 5%, RS 5–14% or ≥15%, BM fibrosis grade 2–3, dysmegakaryopoiesis and severe dysgranulopoiesis.
These variables were combined in a cytological/histological diagnostic score for h-MDS (h-score) aimed at discriminating h-MDS from non-neoplastic BMF (Table 3). The h-score encompassed established MDS-associated features (i.e., BM blasts or CD34 + ≥5% and RS ≥15%) in order to permit its applicability to all patients with hypocellular bone marrow without requiring any pre-selection. The score variables were classified as requisite criteria, which can be attained by either cytology on BM aspirate and/or histopathology on biopsy evaluation (BM blasts/CD34 + cells, BM fibrosis, dysmegakaryopoiesis), and as co-criteria if they are obtainable by BM aspirate only (RS and dysgranulopoiesis). A score of 2 was assigned to MDS-defining criteria (BM blasts or CD34 + cells ≥5% and RS ≥15%), and a score of 1 to the remaining variables (BM blasts or CD34 + cells 3–4%, RS 5–14%, BM fibrosis grade 2–3, dysmegakaryopoiesis, and severe dysgranulopoiesis). By applying ROC analysis, a cutoff value of 2 was associated with a specificity for MDS of 0.96 (Supplemental Table 6). When excluding c-BMF, specificity increased to 1.00.
Clinical features of h-MDS patients classified according to the h-score are reported in Supplemental Table 7. The h-score was able to segregate two distinct groups with a significantly different CI of blast progression, as defined by increase of BM blast percentage (to ≥5% for h-MDS without excess blasts, to a higher MDS-EB category or AML for MDS-EB) (P < 0.001) (Supplemental Fig. 4). Comparable results were obtained when limiting the analysis to patients without MDS-EB or MDS-RS, as well as when considering the whole population of patients with hypocellular bone marrow (h-MDS, AA, and c-BMF) (Supplemental Fig. 5).
Genetic profile of hypoplastic MDS
Eighty-five of 234 evaluable patients with h-MDS (36%) showed chromosomal abnormalities, without significant differences when compared with n-MDS (P = 0.86) (Fig. 2). In addition, no significant difference was found between h-MDS and n-MDS in the prevalence of chromosomal abnormalities providing presumptive evidence of MDS according to WHO criteria (P = 0.88). [6]

Patterns of the genetic lesions identified in the study cohort. a Distribution of somatic genetic lesions in AA, h-MDS, and n-MDS according to the final diagnosis, resulting from standard work-up. Blue bar indicates absence of genetic lesions, maroon bar denotes cytogenetic abnormalities, green bar somatic mutations, orange bar cytogenetic abnormality and somatic mutation. b Distribution of somatic genetic lesions proven specific for MDS in AA, h-MDS, and n-MDS according to the final diagnosis, resulting from standard work-up. Blue bar indicates absence of specific genetic lesions, maroon bar represents cytogenetic abnormalities providing presumptive evidence of MDS according to WHO criteria, green bar denotes somatic mutation patterns proven highly specific for MDS according to Malcovati et al. [36] c Distribution of somatic mutations in the analyzed genes according to the final diagnosis, resulting from standard work-up. Red color indicates a diagnosis of n-MDS, green of h-MDS, blue of AA. Each column represents an individual patient sample
Targeted sequencing of 24 commonly mutated myeloid genes was performed on a total of 471 patients, including 93 h-MDS, 51 non-neoplastic BMF and 239 n-MDS (Fig. 3). Thirty-five of 93 patients with h-MDS (38%) showed one or more somatic mutation (median 1; range 1–4). Compared with n-MDS, h-MDS revealed a significantly lower number of mutations per subject (P < 0.001). Conversely, significantly lower number of mutations per patient and variant allele frequency were observed in AA compared with h-MDS (P = 0.031 and P = 0.003, respectively) (Supplemental Fig. 6).

Cumulative incidence of blast progression, AML evolution, and overall survival of h-MDS according to hg-score. a Cumulative incidence of blast progression, as defined by increase of BM blast percentage (to ≥ 5% for MDS without excess blasts, to a higher MDS-EB category or AML for MDS-EB) of patients with hypoplastic MDS according to the hg-score. Red curve refers to patients with low score (i.e., hg-score < 2), blue curve to high score (i.e., hg-score ≥ 2). b Cumulative incidence of AML progression of patients with hypoplastic MDS according to the hg-score (high hg-score: blue curve; low hg-score: red curve), n-MDS (black curve), and AA (green curve). c Overall Survival of patients with hypoplastic MDS according to the hg-score (high hg-score: blue curve; low hg-score: red curve), n-MDS (black curve) and AA (green curve)
Focusing on mutation patterns, patients with h-MDS showed a significantly lower prevalence of mutations in splicing factors compared with n-MDS (SF3B1: 9% vs 29%, P < 0.001; SRSF2: 5% vs 14%, P = 0.031), as well as in ASXL1 (0% vs 16%, P < 0.001) and TET2 (9% vs 21%, P = 0.008). In addition, patients with h-MDS showed a significantly lower prevalence of somatic mutation patterns proven highly specific for MDS, including mutations in splicing factors and co-mutation patterns involving TET2, DNMT3A, or ASXL1, compared with n-MDS (21/93 vs 137/239, P < .001). [36] Conversely, the prevalence of these patterns in h-MDS was significantly higher than in non-neoplastic BMF (21/93 vs 2/51, P = 0.003) (Fig. 2). Notably, 71% of patients with a hypoplastic BM and low h-score (0–1) had no evidence of clonal disease by cytogenetic or mutation analyses or had a mutation pattern consistent with age-related clonal hematopoiesis.
Definition of an integrated cyto-histologic and genetic score for hypoplastic MDS
Then, we combined the information derived from genetic profile and the h-score into an integrated cyto-histologic and genetic score for h-MDS (hg-score) to discriminate h-MDS from non-neoplastic BMF, by assigning a score of 2 to chromosomal abnormalities presumptive of MDS according to WHO criteria, [6] and a score of 1 to somatic mutation patterns proven highly specific for MDS (Table 4). [36] ROC analysis confirmed that a cutoff value of 2 was associated with the highest percentage of correctly classified (AUC 0.89, P < 0.001) (Supplemental Table 8).
Compared with patients with h-MDS and positive hg-score (i.e., hg-score ≥2), those with a negative score (i.e., hg-score 0–1) were significantly younger (P = 0.03), and showed a significantly higher incidence of PNH clones (P = 0.003) (Supplemental Table 9). The hg-score was able to segregate two distinct groups of h-MDS with a significantly different CI of blast progression (P < 0.001) (Fig. 3, Supplemental Fig. 7). Comparable results were obtained when limiting the analysis to patients without MDS-EB or MDS-RS, as well as when considering the whole population of patients with hypocellular BM (Supplemental Fig. 8). Notably, clonal progression was entirely accounted in the group having a positive hg-score, whereas no progression events were noticed in the group with a negative hg-score. When comparing OS and CI of AML progression of h-MDS patients according to hg-score with those of patients with n-MDS and AA, h-MDS patients with a positive hg-score showed OS and CI of AML progression comparable to those of patients with n-MDS (P = 0.42 and P = 0.74, respectively). These results were confirmed within the categories of MDS-SLD or –MLD, MDS-RS, MDS del(5q), and MDS-EB. Within h-MDS with hg-score ≥ 2, IPSS-R retained a significant effect on both OS and CI of AML evolution (HR = 1.94 and HR = 3.61, respectively, P < 0.001). Conversely, h-MDS patients with a negative hg-score had OS and CI of AML progression not significantly different from those of patients with AA (P = 0.72 and P = 1, respectively) (Fig. 3). In addition, no significant difference was noticed between h-MDS patients with negative hg-score and AA in the CI of blast progression, as defined by an increase of BM blast percentage to ≥5% (P = 0.49).
Molecular features and clinical outcome of patients with idiopathic cytopenia of undetermined significance and hypocellular bone marrow
Within the population of adult patients with hypocellular bone marrow, we identified 96 patients with reduced age-adjusted BM cellularity and mild peripheral cytopenia who did not fulfill diagnostic criteria for MDS or AA. According to conventional diagnostic work-up, these patients received a provisional diagnosis of ICUS, [41] herein designated as hypoplastic ICUS (h-ICUS). Patients provisionally classified in this category were significantly younger and showed a higher female to male ratio and milder cytopenia compared with those receiving a diagnosis of h-MDS (Supplemental Table 10). Eight of these patients developed an overt myeloid neoplasm after a median follow-up 21 months (range (4–49 months) (Supplemental Fig. 9).
Somatic mutation analysis was available for 88 h-ICUS patients: 16 patients showed one or more somatic mutations (18%) and eight showed a mutation pattern proven highly predictive of MDS (9%), including mutations in splicing factors and co-mutation patterns involving TET2, DNMT3A, or ASXL1 (Supplemental Fig. 10). [36]
According to the hg-score, 7 h-ICUS patients showed a positive score. The hg-score was able to segregate two distinct groups with a significantly different CI of progression into myeloid neoplasm (P < 0.001) (Supplemental Fig. 11). Three patients having a hg-score < 2 eventually developed a myeloid neoplasm: one showed a pattern of co-mutation in DNMT3A and IDH1, previously proven as highly predictive of a myeloid neoplasm, and two had an isolated mutation in ASXL1.
Discussion
It is well established that a variable fraction of patients with MDS present with a decreased BM cellularity, referred to as hypoplastic MDS in the current WHO classification of myeloid neoplasm. [6] Although this subset has not been recognized as a separate MDS subtype, distinctive features have been associated with a hypocellular bone marrow, including a higher response rate to immunosuppressive therapy and a favorable prognosis. [2, 4, 7,8,9] However, accurate diagnostic criteria for h-MDS have not been clearly defined to date, making everyday differential diagnosis from other BMF and clinical-decision making challenging. [2] In this study, we took advantage of a large and well-annotated cohort of consecutive patients with BM hypocellularity from two reference centers, and identify robust histopathological criteria to recognize h-MDS. This information was then combined with cytogenetic and somatic mutation profiles to develop an integrated score that was able to clearly segregate two distinct groups of h-MDS, one with clinical and genetic features highly consistent with a myeloid neoplasm, and one with features more consistent with a non-malignant bone marrow failure.
A prerequisite for the recognition of h-MDS is the definition of BM hypocellularity. However, precise criteria have not been clearly defined. In fact, a cutoff value of 20–30% cellularity, as derived from AA, does not account for age-related changes, resulting in an uncertain classification of younger MDS patients. In addition, the definition of hypocellularity is problematic in elderly patients in whom these values may partly overlap with the expected age-adjusted cellularity. [14, 15] To address this issue, we first compared clinical features and outcome of patients with h-MDS as defined by a BM cellularity ≤25% and of patients with a reduced age-adjusted cellularity. Then, we identified patients aged 65 year or older with a BM cellularity ≤25% but consistent with their age-adjusted cellularity reference values, and compared their clinical and hematological features with those of age-matched individuals with a BM cellularity ≤25% and reduced by age-adjusted criteria. Overall, no significant differences were found between these groups in clinical and hematological variables, survival and risk of AML evolution, suggesting that a combined criterion of reduced age-adjusted BM cellularity or BM cellularity ≤25% can be adopted to define h-MDS. This definition allows a correct classification of young patients with age-adjusted reduced cellularity, as well as of elderly individuals, in whom the wide range of age-related changes may preclude robust estimates. Although several factors may concur to BM hypocellularity, including bone marrow microenvironment abnormalities, inflammation and T-cell mediated autoimmunity, and we cannot exclude that this definition may capture at least partly diverse pathophysiology processes, at present it may represent a robust criterion recognizing a clinically homogeneous group of patients within MDS.
Next, we aimed to identify cytological and histological parameters potentially useful to differentiate h-MDS from non-neoplastic BMF. We found that erythroid dysplasia, as well as mild to moderate myeloid dysplasia, in the context of hypocellular bone marrow were a frequent finding yet compatible with a diagnosis of AA, partly at odds with previous findings. [2] Conversely, dysmegakaryopoiesis and severe dysgranulopoiesis were proven highly specific for MDS. These findings may be useful to separate MDS from non-neoplastic BMF in the everyday clinical practice, and may provide the frame for the interpretation of hematopoietic clones in the context of BM hypocellularity.
We then explored genetic profile of h-MDS, and found that MDS patients with hypocellular bone marrow revealed mutation patterns in-between that of myeloid neoplasm and AA. [22, 23, 28, 29] In addition, h-MDS showed a significantly lower prevalence of somatic mutation patterns proven highly specific for MDS, including mutations in splicing factors and co-mutation patterns involving TET2, DNMT3A, or ASXL1, compared with n-MDS, suggesting the absence of MDS-specific drivers in a fraction of these patients. [36, 43,44,45] Conversely, the prevalence of these patterns in h-MDS was significantly higher than in non-malignant BMF. [28, 29, 46]
We combined cytological and histological parameters proven highly specific for MDS with the information derived from genetic profiles into an integrated score to discriminate h-MDS from non-neoplastic BMF. Although the inclusion in the hg-score of established MDS-associated morphological and genetic features (i.e., BM blasts or CD34 + , RS, and MDS presumptive cytogenetic abnormalities) may appear redundant, this allows in everyday clinical practice its application to all patients with hypocellular BM without any pre-selection. Conversely, selected morphological features, such as dysmegakaryopoiesis, and specific mutation patterns appear to be very helpful in distinguishing true h-MDS from non-malignant bone marrow failures.
Considering that suboptimal or inadequate aspirate specimens are frequent shortcomings in everyday clinical practice when investigating hypocellular BM, score variables were classified as requisite criteria, attained by biopsy evaluation (and/or BM aspirate when available), and co-criteria, obtainable by BM aspirate. Whereas morphological analysis remains the standard for BM blast count, CD34 immunostaining can be adopted for assessing blast percentage in case of inadequate aspirate specimen that may result in an underestimated blast count. [2, 6, 16, 42] This nested structure allows one to optimize the information obtained through diagnostic work-up: as expected, the applicability is maximal when considering requisite-criteria only, achievable in the great majority of patients, whereas the percentage of correctly identified is progressively increasing when filling in cytological and genetic information (Supplemental Fig. 12). The implementation of genetic profiling from peripheral blood cells will further increase the applicability of the score. [36, 47]
Notably, the hg-score was able to clearly segregate two distinct groups of h-MDS with a significantly different risk of blast progression. Remarkably, clonal progression was entirely accounted for by the group with a positive hg-score, whereas no events were noticed in the group with a negative hg-score, supporting the hypothesis that a classification as MDS might not be appropriate for these patients. When comparing survival and risk of AML progression of h-MDS patients classified according to the hg-score with those of the reference populations of patients with n-MDS and AA, h-MDS patients with a positive hg-score showed a clinical course comparable to that of patients with n-MDS, whereas h-MDS patients with a negative hg-score had outcomes not dissimilar from those of patients with AA. Taken together, these data suggest that the integration of cyto-histological and genetic features in adult patients with hypocellular BM permits the segregation within h-MDS of two distinct groups, one with clinical and genetic features highly consistent with myeloid neoplasm, and one with features more consistent with a non-malignant BMF. Compared with patients with h-MDS and positive hg-score, those with a negative score were significantly younger, and showed a higher proportion of females and a significantly higher incidence of PNH clone, consistent with this conclusion.
Although a validation of the hg-score in independent patient populations is warranted, the results of this study may have relevant implications in the clinical management of adult patients with a hypocellular bone marrow. In individuals with a negative hg-score calculated on the basis of both cytological and genetic information, abstaining from a diagnosis of myeloid neoplasm should be advisable. Although data on response to immunosuppressive therapy with ATG plus cyclosporine A in our study did not allow firm conclusion, a management strategy as in non-malignant BMF seems appropriate, although this requires validation in a prospective study. Notably, even in the absence of cytological and genetic information in case of inadequate diagnostic specimen, patients with a negative score have a limited risk of blast progression, and we propose that a diagnosis of myeloid neoplasm should be carefully pondered and reconsidered after adequate follow-up. Conversely, in patients with h-MDS and positive hg-score a MDS treatment strategy seems justified, though tolerance and efficacy of treatment modalities with hematologic toxicity, such as hypometylating agents, will deserve confirmation and appropriate monitoring. [48]
Finally, in a proportion of patients, conventional diagnostic work-up was not diagnostic for AA or h-MDS, and a provisional diagnosis of hypoplastic ICUS was adopted. Even in this area of uncertainty, the hg-score was able to segregate two distinct groups with a significantly different CI of progression into myeloid neoplasm, the higher risk group having a risk not dissimilar from that observed in clonal cytopenia of undetermined significance. [36]
In conclusion, this study provides evidence for robust criteria to define h-MDS. The integration of cyto-histological and genetic features in adult patients with a hypocellular BM enables the segregation into two distinct groups, one with clinical and genetic features highly consistent with myeloid neoplasm, in whom a diagnosis of h-MDS seems appropriate, and one with features more consistent with a non-malignant bone marrow failure.
References
Cazzola M, Malcovati L. Myelodysplastic syndromes--coping with ineffective hematopoiesis. N Engl J Med. 2005;352:536–8.
Bennett JM, Orazi A. Diagnostic criteria to distinguish hypocellular acute myeloid leukemia from hypocellular myelodysplastic syndromes and aplastic anemia: recommendations for a standardized approach. Haematologica. 2009;94:264–8.
Sloand EM. Hypocellular myelodysplasia. Hematol Oncol Clin North Am. 2009;23:347–60.
Huang TC, Ko BS, Tang JL, Hsu C, Chen CY, Tsay W, et al. Comparison of hypoplastic myelodysplastic syndrome (MDS) with normo-/hypercellular MDS by International Prognostic Scoring System, cytogenetic and genetic studies. Leukemia. 2008;22:544–50.
Tuzuner N, Cox C, Rowe JM, Watrous D, Bennett JM. Hypocellular myelodysplastic syndromes (MDS): new proposals. Br J Haematol. 1995;91:612–7.
Hasserjian RP, Orazi A, Brunning R, Germing U, Le Beau MM, Porwit A, et al. Myelodysplastic syndromes: Overview. In: Swerdlow SH CE, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Arber, DA, Hasserjian RP, Le Beau, MM, orazi, A, Siebert, R, editor. WHO Classification of Tumors Of Haematopoietic and Lymphoid Tissues. Lyon (France): IARC; 2017. p. 98-106.
Passweg JR, Giagounidis AA, Simcock M, Aul C, Dobbelstein C, Stadler M, et al. Immunosuppressive therapy for patients with myelodysplastic syndrome: a prospective randomized multicenter phase III trial comparing antithymocyte globulin plus cyclosporine with best supportive care--SAKK 33/99. J Clin Oncol. 2011;29:303–9.
Sloand EM, Wu CO, Greenberg P, Young N, Barrett J. Factors affecting response and survival in patients with myelodysplasia treated with immunosuppressive therapy. J Clin Oncol. 2008;26:2505–11.
Lim ZY, Killick S, Germing U, Cavenagh J, Culligan D, Bacigalupo A, et al. Low IPSS score and bone marrow hypocellularity in MDS patients predict hematological responses to antithymocyte globulin. Leukemia. 2007;21:1436–41.
Kobayashi T, Nannya Y, Ichikawa M, Oritani K, Kanakura Y, Tomita A, et al. A nationwide survey of hypoplastic myelodysplastic syndrome (a multicenter retrospective study). Am J Hematol. 2017;92:1324–32.
Koh Y, Lee HR, Song EY, Kim HK, Kim I, Park S, et al. Hypoplastic myelodysplastic syndrome (h-MDS) is a distinctive clinical entity with poorer prognosis and frequent karyotypic and FISH abnormalities compared to aplastic anemia (AA). Leuk Res. 2010;34:1344–50.
Maschek H, Kaloutsi V, Rodriguez-Kaiser M, Werner M, Choritz H, Mainzer K, et al. Hypoplastic myelodysplastic syndrome: incidence, morphology, cytogenetics, and prognosis. Ann Hematol. 1993;66:117–22.
Killick SB, Bown N, Cavenagh J, Dokal I, Foukaneli T, Hill A, et al. Guidelines for the diagnosis and management of adult aplastic anaemia. Br J Haematol. 2016;172:187–207.
Thiele J, Kvasnicka HM, Facchetti F, Franco V, van der Walt J, Orazi A. European consensus on grading bone marrow fibrosis and assessment of cellularity. Haematologica. 2005;90:1128–32.
Tuzuner N, Cox C, Rowe JM, Bennett JM. Bone marrow cellularity in myeloid stem cell disorders: impact of age correction. Leuk Res. 1994;18:559–64.
Orazi A, Albitar M, Heerema NA, Haskins S, Neiman RS. Hypoplastic myelodysplastic syndromes can be distinguished from acquired aplastic anemia by CD34 and PCNA immunostaining of bone marrow biopsy specimens. Am J Clin Pathol. 1997;107:268–74.
Barrett J, Saunthararajah Y, Molldrem J. Myelodysplastic syndrome and aplastic anemia: distinct entities or diseases linked by a common pathophysiology? Semin Hematol. 2000;37:15–29.
Calado RT, Young NS. Telomere diseases. N Engl J Med. 2009;361:2353–65.
Brown AL, Churpek JE, Malcovati L, Dohner H, Godley LA. Recognition of familial myeloid neoplasia in adults. Semin Hematol. 2017;54:60–8.
Malcovati L, Cazzola M. The shadowlands of MDS: idiopathic cytopenias of undetermined significance (ICUS) and clonal hematopoiesis of indeterminate potential (CHIP). Hematol Am Soc Hematol Educ Program. 2015;2015:299–307.
Malcovati L, Hellstrom-Lindberg E, Bowen D, Ades L, Cermak J, Del Canizo C, et al. Diagnosis and treatment of primary myelodysplastic syndromes in adults: recommendations from the European LeukemiaNet. Blood. 2013;122:2943–64.
Papaemmanuil E, Gerstung M, Malcovati L, Tauro S, Gundem G, Van Loo P, et al. Clinical and biological implications of driver mutations in myelodysplastic syndromes. Blood. 2013;122:3616–27.
Haferlach T, Nagata Y, Grossmann V, Okuno Y, Bacher U, Nagae G, et al. Landscape of genetic lesions in 944 patients with myelodysplastic syndromes. Leukemia. 2013;28:241–7.
Jaiswal S, Fontanillas P, Flannick J, Manning A, Grauman PV, Mar BG, et al. Age-related clonal hematopoiesis associated with adverse outcomes. N Engl J Med. 2014;371:2488–98.
Genovese G, Kahler AK, Handsaker RE, Lindberg J, Rose SA, Bakhoum SF, et al. Clonal hematopoiesis and blood-cancer risk inferred from blood DNA sequence. N Engl J Med. 2014;371:2477–87.
Xie M, Lu C, Wang J, McLellan MD, Johnson KJ, Wendl MC, et al. Age-related mutations associated with clonal hematopoietic expansion and malignancies. Nat Med. 2014;20:1472–8.
Shlush LI. Age-related clonal hematopoiesis. Blood. 2018;131:496–504.
Kulasekararaj AG, Jiang J, Smith AE, Mohamedali AM, Mian S, Gandhi S, et al. Somatic mutations identify a subgroup of aplastic anemia patients who progress to myelodysplastic syndrome. Blood. 2014;124:2698–704.
Yoshizato T, Dumitriu B, Hosokawa K, Makishima H, Yoshida K, Townsley D, et al. Somatic Mutations and Clonal Hematopoiesis in Aplastic Anemia. N Engl J Med. 2015;373:35–47.
Ogawa S. Clonal hematopoiesis in acquired aplastic anemia. Blood. 2016;128:337–47.
Mufti G, Marsh J. Somatic mutations in aplastic anemia. Hematol Oncol Clin North Am. 2018;32:595–607.
Nazha A, Seastone D, Radivoyevitch T, Przychodzen B, Carraway HE, Patel BJ, et al. Genomic patterns associated with hypoplastic compared to hyperplastic myelodysplastic syndromes. Haematologica. 2015;100:e434–7.
Negoro E, Nagata Y, Clemente MJ, Hosono N, Shen W, Nazha A, et al. Origins of myelodysplastic syndromes after aplastic anemia. Blood. 2017;130:1953–7.
Cooper JN, Young NS. Clonality in context: hematopoietic clones in their marrow environment. Blood. 2017;130:2363–72.
Keel SB, Scott A, Sanchez-Bonilla M, Ho PA, Gulsuner S, Pritchard CC, et al. Genetic features of myelodysplastic syndrome and aplastic anemia in pediatric and young adult patients. Haematologica. 2016;101:1343–50.
Malcovati L, Galli A, Travaglino E, Ambaglio I, Rizzo E, Molteni E, et al. Clinical significance of somatic mutation in unexplained blood cytopenia. Blood. 2017;129:3371–8.
Mufti GJ, Bennett JM, Goasguen J, Bain BJ, Baumann I, Brunning R, et al. Diagnosis and classification of myelodysplastic syndrome: International Working Group on Morphology of myelodysplastic syndrome (IWGM-MDS) consensus proposals for the definition and enumeration of myeloblasts and ring sideroblasts. Haematologica. 2008;93:1712–7.
Goasguen JE, Bennett JM, Bain BJ, Vallespi T, Brunning R, Mufti GJ. Morphological evaluation of monocytes and their precursors. Haematologica. 2009;94:994–7.
Arber DA, Orazi A, Hasserjian RP, Brunning R, Germing U, Le Beau MM, et al. Introduction and overview of the classification of myeloid neoplasms. In: Swerdlow SH CE, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Arber, DA, Hasserjian RP, Le Beau, MM, orazi, A, Siebert, R, editor. WHO Classification of Tumors Of Haematopoietic and Lymphoid Tissues. Lyon (France): IARC; 2017. p. 16–27.
Borowitz MJ, Craig FE, Digiuseppe JA, Illingworth AJ, Rosse W, Sutherland DR, et al. Guidelines for the diagnosis and monitoring of paroxysmal nocturnal hemoglobinuria and related disorders by flow cytometry. Cytometry B Clin Cytom. 2010;78:211–30.
Valent P, Orazi A, Steensma DP, Ebert B, Haase D, Malcovati L, et al. Proposed minimal diagnostic criteria for myelodysplastic syndromes (MDS) and potential pre-MDS conditions. Oncotarget. 2017;8:73483–500.
Della Porta MG, Travaglino E, Boveri E, Ponzoni M, Malcovati L, Papaemmanuil E, et al. Minimal morphological criteria for defining bone marrow dysplasia: a basis for clinical implementation of WHO classification of myelodysplastic syndromes. Leukemia. 2015;29:66–75.
Papaemmanuil E, Cazzola M, Boultwood J, Malcovati L, Vyas P, Bowen D, et al. Somatic SF3B1 mutation in myelodysplasia with ring sideroblasts. N Engl J Med. 2011;365:1384–95.
Yoshida K, Sanada M, Shiraishi Y, Nowak D, Nagata Y, Yamamoto R, et al. Frequent pathway mutations of splicing machinery in myelodysplasia. Nature. 2011;478:64–9.
Graubert TA, Shen D, Ding L, Okeyo-Owuor T, Lunn CL, Shao J, et al. Recurrent mutations in the U2AF1 splicing factor in myelodysplastic syndromes. Nat Genet. 2011;44:53–7.
Bluteau O, Sebert M, Leblanc T, Peffault de Latour R, Quentin S, Lainey E, et al. A landscape of germ line mutations in a cohort of inherited bone marrow failure patients. Blood. 2018;131:717–32.
He J, Abdel-Wahab O, Nahas MK, Wang K, Rampal RK, Intlekofer AM, et al. Integrated genomic DNA/RNA profiling of hematologic malignancies in the clinical setting. Blood. 2016;127:3004–14.
Seymour JF, Bennett JM, List AF, Mufti GJ, Gore SD, Fenaux P, et al. Bone marrow hypocellularity does not affect tolerance or efficacy of azacitidine in patients with higher-risk myelodysplastic syndromes. Br J Haematol. 2014;165:49–56.
Acknowledgements
This work was supported by Associazione Italiana per la Ricerca sul Cancro (AIRC, Milan, Italy) IG #20125 to LM, and AIRC 5 × 1000 project #21267 to MC and LM (MYNERVA project, http://www.progettoagimm.it), and by Fondazione Regionale Ricerca Biomedica, Milan, Italy (FRRB project no. 2015-0042 to MC).
Author contributions
EB, DM, LM, and GM designed the study, interpreted the data and wrote the manuscript; SG, AAK, AGK, KR, EC, RMI, AB, GT, collected clinical data; AG, JJ performed genetic analyses; VVF performed statistical analysis; ET, EB performed cytological and histological analyses; MC, JM contributed to study design and interpretation of the data.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bono, E., McLornan, D., Travaglino, E. et al. Clinical, histopathological and molecular characterization of hypoplastic myelodysplastic syndrome. Leukemia 33, 2495–2505 (2019). https://doi.org/10.1038/s41375-019-0457-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41375-019-0457-1
