
Abstract
Objective
Describe self-relating (self-criticism, self-compassion) and parenting competence (satisfaction, self-efficacy) in mothers of children born preterm, and their associations with child characteristics, maternal sociodemographics at childbirth, and maternal concurrent well-being.
Study design
The sample comprised 1926 biological mothers of 3- to18-year-old children born preterm with self-ratings on the standardized Forms of Self-Criticising/Attacking & Self-Reassuring Scale, Self-Compassion Scale, and Parenting Sense of Competence Scale.
Results
Mothers of children in early childhood reported significantly (p < 0.05) lower self-compassion than in middle childhood and adolescence. They also reported significantly lower parenting satisfaction than mothers of adolescents and higher self-efficacy than their middle childhood counterparts. Maternal psychosocial well-being was most strongly associated with self-compassion, parenting satisfaction, and self-efficacy after accounting for maternal psychopathology, child gestation, and child age.
Conclusion
Longer-term associations of preterm birth with maternal self-relating and parenting competence emphasize broadening the scope of neonatal follow-up services, extending beyond child neurodevelopmental surveillance and postpartum psychopathology screening.
Similar content being viewed by others


Postpartum depression is well-recognized as one of the most frequent maternal psychological diagnoses after childbirth. A recent meta-analysis found that mothers face between 1.2 and 18.4 times the risk for depression after preterm birth relative to term birth [1]. Similar risks have been reported for anxiety and posttraumatic stress [2, 3], and even in the absence of psychopathology, mothers report suboptimal well-being. A recent synthesis of 30 quantitative, qualitative, and mixed-methods studies of maternal experiences after preterm birth identified themes of shock and horror, consuming guilt, pervasive anxiety and hypervigilance, emotional numbing, and intrusive thoughts of the event [4]. These findings are concerning as psychopathology and/or suboptimal well-being have cascading implications for parental outcomes, particularly disrupted parent-infant bonding and maternal sensitivity.
Along with maternal psychopathology, parenting behaviors described as specific, observable, child caregiving behaviors have been extensively investigated in the preterm birth population. Nonetheless, there is limited investigation of maternal intrapersonal experiences beyond this scope spanning cognitive and affective dimensions. For example, one of the most recent meta-analyses on parenting among parents of children born preterm identified only four studies examining parenting attitudes (intrapersonal dimension), in contrast to 23 studies evaluating parenting behavior (interpersonal dimension) [5]. This illustrates the shortcomings of existing preterm birth follow-up research regarding intrapersonal parenting experiences, a key determinant of parenting behavior [6]. Therefore, a multidimensional conceptualization of maternal experiences is needed to comprehensively characterize mothers’ unique and complex experiences after preterm birth, recognizing their dynamic nature over time.
A core facet of parenting experiences that remains unclear after preterm birth is self-relating, the way individuals relate to themselves through self-directed, internalized processes in the face of adversities. Self-criticism involves high levels of self-evaluation where negative judgment, blame, and/or attack are present [7], whereas self-compassion involves self-reassurance, understanding, and kindness [8]. While these contrasting self-relating styles are often associated, they are distinct constructs [9].
Consequently, more critical self-relating increases the risk for the development and maintenance of psychopathology [7, 10], parenting stress, reduced acceptance of the parenting role and associated challenges [11], and notably, maladaptive parenting behavior [12]. Further, self-compassionate relating is independently associated with more favorable parenting outcomes. A recent meta-analysis of 13 studies synthesizing the benefits of interventions aimed at increasing parental self-compassion found significant reductions in parental psychopathology, including depression, anxiety, and stress, as well as increases in mindfulness [13, 14]. In addition, greater self-compassion is associated with reduced negative emotional responses to adversities including guilt and shame [15], and more adaptive parenting behaviors [16]. Positive effects of self-compassion in parents of children with autism spectrum disorder, a common neurodevelopmental outcome associated with preterm birth [17], have been identified. These include less disappointment, more functional relationships and greater emotional connection to the child, as well as decreased perceptions of difficult child behavior [18]. Nonetheless, research on maternal self-relating in the aftermath of preterm birth is limited, with self-criticism remaining a peripheral, secondary outcome, and insufficient conceptualization and inadequate description of how maternal self-relating changes over time.
Another related dimension that has been insufficiently investigated after preterm birth is parenting sense of competence, described as the caregiver’s beliefs and perceptions about their ability to effectively engage in parenting tasks [19]. Parenting competence has implications for parental expectations and maladaptive parenting behavior [6, 20]. This is important for parents of children born preterm, as perceived loss of parental role and autonomy is consistently identified as a significant stressor associated with neonatal intensive care unit admission. Pivotal to the development of parenting competence are the affective domain of satisfaction (i.e., frustration, anxiety, motivation), and the instrumental domain of self-efficacy (i.e., self-perceived beliefs about successfully completing parenting tasks) [19, 21]. Parenting competence in the general population typically increases over time as mastery is gained through experience; however, among parents of children born preterm, mixed findings have been reported, partially accounted for by varying study designs, conceptualizations of parenting outcomes, and assessment instruments. For example, a prospective study investigating maternal confidence after preterm birth, defined as confidence in the ability to provide adequate infant care, found decreasing confidence between 3–4 and 6–8 weeks after preterm birth [22]. Contrastingly, a cross-sectional study investigating parenting competence and self-efficacy in parents (98% mothers) of preterm- and term-born children at <24 months corrected age found greater parenting competence in mothers of older children, with no differences for the dimension of self-efficacy by age [23].
While the current focus of early neonatal follow-up including maternal psychopathology and parenting after preterm birth is valuable, the short- and long-term evaluation of intrapersonal maternal experiences has remained neglected. As a result, there is limited understanding of the extent of self-relating and parenting competence, particularly regarding the dynamic nature of these experiences after adverse birthing experiences, such as preterm birth. Long-term evaluation of maternal experiences after preterm birth is further justified due to expected changes in caregiving demands. Specifically, there are well-documented challenges experienced by mothers of children born preterm in coping with child behavioral and emotional difficulties that typically occur between school age and late adolescence [17, 24]. Hence, using a cross-sectional study design, this study aimed to describe self-relating (self-criticism and self-compassion) and parenting competence (satisfaction and self-efficacy) in mothers of children born preterm stratified by their child’s chronological age (early childhood, middle childhood, and adolescence). Another aim was to examine associations of self-relating and parenting competence with child characteristics, maternal sociodemographics at childbirth, and maternal concurrent well-being.
Methods
Participants
Between October 2019 and February 2020, primary caregivers of 3- to 18-year-old children born preterm (<37 weeks gestation) were recruited through parent organizations, with screening and outcome questionnaires administered via a secure web-based portal. If participants were the primary caregiver of more than one child born preterm, they were asked to consider their youngest child born preterm. For this study, eligible participants were biological mothers aged 22–63 years at assessment, for whom English was their primary (not necessarily native) language, and who resided in Australia, Canada, New Zealand, United Kingdom/Ireland, or United States of America. Further, mothers were eligible only if they served as a primary caregiver of a child born preterm who had not been diagnosed with a chromosomal anomaly, fetal alcohol spectrum disorder, and/or developmental disability (IQ < 70) if tested. In addition, mothers had to report being “confident”, “very confident”, or “extremely confident” on a 5-point Likert scale about their child’s gestational age at birth. Child gestational information was obtained twice, initially during eligibility screening and subsequently during post-consent data collection, using two distinct response formats. Of respondents (N = 2595/3300 eligible; 79%), gestational age reporting was congruent for 97%, with the remaining 3% (n = 80/2595) excluded from all analyses. A further reason for exclusion was incomplete responses (n = 589/2595 [23%], including 511 participants with no primary outcomes data). Therefore, of mothers who consented to participate, 74% were included in the current study (N = 1926/2595). The final sample comprised 1926 biological mothers stratified into three groups corresponding to their child’s chronological age: early childhood (3–5 years, n = 865), middle childhood (6–9 years, n = 611), and adolescence (10–18 years, n = 450). Analysis of participants excluded and included in the current study demonstrated mothers who were excluded were more likely to be younger (p = 0.001), with lower educational attainment (p < 0.001), living within a lower family sociodemographic household at childbirth (p < 0.001), with a preterm-born child of slightly older gestations (p = 0.01).
The American Association for Public Opinion Research Best Practices for Survey Research [25] informed the design and conduct of this study. The University of Queensland Human Research Ethics Committee approved the study protocol, and all participants provided informed consent.
Measures
Intrapersonal maternal outcomes were self-reported at a single time point on three standardized instruments. After a comprehensive literature review, these tools were selected primarily due to cultural appropriateness and age- and domain-specificity for the study population.
Self-criticism was assessed using the 22-item Forms of Self-Criticising/Attacking & Self-Reassuring Scale [26]. Mothers indicated their agreement with statements on a 5-point Likert scale from “Not at all like me” to “Extremely like me”, with higher scores representing greater critical self-relating dialogue. This scale has strong construct validity ranging from 0.91 to 0.95 in clinical populations [27, 28].
Self-compassion was assessed using the 26-item Self-Compassion Scale [8]. Mothers indicated how often they experienced self-compassionate relating on a 5-point Likert scale from “Almost never” to “Almost always”. The total score comprises six subdomains and is represented as a grand mean. Higher scores represent a greater capacity for self-compassionate relating. This scale has satisfactory psychometric properties including robust construct, discriminant, and convergent validity [8, 29].
Parenting satisfaction and self-efficacy were assessed using the 17-item Parenting Sense of Competence Scale [30]. Mothers rated their agreement with item statements on a 6-point Likert scale from “Strongly disagree” to “Strongly agree”, with higher scores representing greater satisfaction and self-efficacy independently. This scale has moderate to strong construct, convergent, and discriminant validity, and factor analysis supports the satisfaction and self-efficacy domains as assessing distinct aspects of parenting competence [19, 31].
Statistical analyses
Data analysis was completed in three stages using the IBM® SPSS® Statistics software version 24.0. First, baseline sample characteristics were examined using the one-way analysis of variance for continuous variables and the Chi-square test of independence for categorical variables. Second, analysis of covariance with planned contrasts were performed to examine linear associations between maternal intrapersonal outcomes and the three child chronological age groups, with early childhood as the referent group for the test of linear associations and Cohen’s d as the measure of effect size. Country of residence was not included as a covariate due to marginal to negligible associations with the outcomes. Total psychopathology screening score on the Depression Anxiety Stress Scales Short Form (DASS-21) was entered as a covariate due to established independent associations with maternal outcomes and to account for potential self-reporting bias at the time of the assessment. All reported associations were reanalyzed with child age as a continuous variable using partial correlations controlling for maternal psychopathology screening score.
Third, a series of hierarchical linear regression modeling was undertaken to identify key variables associated with maternal intrapersonal outcomes. Variables were entered into the model in four blocks: (1) covariates including child gestational age at birth, child chronological age at assessment, and maternal total psychopathology screening score; (2) child characteristics including sex (coded as 0 = female, 1 = male), multiple birth (0 = singleton, 1 = multiple), neonatal risk (0 = low, 1 = high [presence of one or more of the following conditions: confirmed neonatal infection, oxygen therapy at 36 weeks, severe brain injury or abnormality]), and developmental risk (0 = low [none or developmental diagnosis in one domain], 1 = high [presence of two or more developmental diagnoses across neurobehavioral, neurosensory, physical/chronic domains]); (3) maternal sociodemographic characteristics at childbirth including age, educational attainment (0 = high, 1 = low [high school graduate or below]), family socioeconomic status (0 = high, 1 = low [unemployed, unskilled, semi-skilled]), parenthood status (0 = single, 1 = partnered), and identification with ethnic/racial minority (0 = no, 1 = yes); and (4) maternal concurrent well-being assessed using the Mental Health Continuum Short Form. Variables were modeled using backward and forward approaches to identify the most parsimonious model, with variables entered as a continuous measure where possible to optimize statistical precision. A p < 0.10 criterion was used to select variables for inclusion in the initial model, and a p < 0.05 criterion to retain variables in the final fitted model.
Results
Sample characteristics, as shown in Table 1, demonstrate that mothers of adolescents had significantly (p < 0.05) greater proportions of young motherhood, low educational attainment, and single parenthood at childbirth. Mothers of children in early childhood reported significantly greater concurrent total psychopathology screening scores. Furthermore, children born preterm in the early childhood group had a significantly lower proportion of confirmed neonatal infection.
Maternal intrapersonal outcomes by child chronological age groups
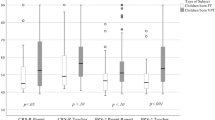
As described in Table 2, analyses of maternal self-relating and parenting competence outcomes across the three child chronological age groups showed that mothers of children in early childhood reported significantly lower self-compassion than mothers of children in middle childhood (Cohen’s d = 0.11, p = 0.04) and adolescence (Cohen’s d = 0.25, p = 0.003). They also reported significantly lower parenting satisfaction than mothers of adolescents (Cohen’s d = 0.20, p = 0.001), and higher self-efficacy than mothers of children in middle childhood (Cohen’s d = 0.12, p = 0.02). No statistically significant associations were evident for the remaining pairwise comparisons. Similar patterns of reported associations were observed after reanalysis of the data with child age as a continuous variable (see Online Supplement).
Correlates of maternal intrapersonal outcomes
As shown in Table 3, higher maternal self-criticism was associated with younger maternal age (β = −0.07, p < 0.001) and lower family socioeconomic status (β = −0.07, p = 0.001) at the time of childbirth. Lower maternal self-compassion was also associated with younger maternal age at childbirth (β = 0.05, p = 0.001), as well as two-parent family at childbirth (β = 0.04, p = 0.02) and lower concurrent well-being (β = 0.40, p < 0.001). The final fitted regression models explained 31% and 51% of the variance in self-criticism and self-compassion, respectively.
As shown in Table 4, lower maternal parenting satisfaction was associated with multiple birth status (β = −0.08, p < 0.001) and lower maternal concurrent well-being (β = 0.24, p < 0.001). Lower self-efficacy was also associated with multiple birth status (β = −0.08, p < 0.001), along with the absence of child developmental diagnosis or diagnosis restricted to a single domain (β = 0.04, p = 0.04), older maternal age at childbirth (β = −0.07, p = 0.001), and lower maternal concurrent well-being (β = 0.24, p < 0.001). The final fitted regression models explained 30% and 15% of the variance in parenting satisfaction and self-efficacy, respectively.
Discussion
This study, based on one of the largest samples to examine maternal outcomes after preterm birth to date, is novel in its multidimensional conceptualization and evaluation of long-term maternal intrapersonal experiences following preterm birth. Specifically, our research extends beyond the hospital stay and early childhood period, along with expanding the scope of investigation on postpartum psychopathology and parenting behavior outcomes, typical across follow-up studies of preterm birth. Study findings show mothers of children in early childhood reported lower self-compassion and parenting satisfaction compared with mothers of older children or adolescents, suggesting that these markers of suboptimal parental well-being following preterm birth are dynamic in nature, and may improve over time, at least at the group level. Nonetheless, we found similar reports of self-criticism among the three groups of mothers of children born preterm stratified by their child’s chronological age. Based on literature describing the acquisition of self-efficacy by Bandura (1982) [32] it was predicted that mothers of older children would report greater levels of self-efficacy in engaging with parenting tasks than mothers of younger children. Contrary to this prediction, mothers of children in early childhood (3–5 years of age) reported greater self-efficacy than mothers of children in middle childhood (6–9 years). It is plausible that this finding could be explained by the emergence of child behavioral and emotional difficulties during this period [17, 24], as well as an increase in the need and utilization of allied health support for a range of child-related challenges across domains of cognition, motor, language, and education [33].
While previous longitudinal research demonstrates long-standing and pervasive maternal psychopathology after preterm birth [34], findings of this study are consistent with parental quality of life converging closer to that of term birth over time [35]. In addition, current findings align with well-documented parenting research that describes the preschool-to-school entry transition period as one of the most stressful intervals for familial outcomes due to changes in routine, care responsibilities, child-related demands, and increased opportunity for parental comparisons. Among parents of children born preterm, these challenges are likely exacerbated due to the increased risk for poorer school readiness [36] and emerging child behavioral and emotional difficulties relative to their term-born peers [17]. Importantly, the findings of this study have identified a range of risk factors including child neonatal and sociodemographic characteristics. This information can be used for antenatal screening and targeted postpartum follow-up services.
Our findings provide support for the revised process model of parental functioning by Taraban & Shaw (2018) [37, 38], which highlights the importance of cognitive and affective parent characteristics in the development of optimal functioning. Further, findings highlight the importance of neonatal and early social factors in the development of these processes. This emphasizes the importance of early surveillance for mothers after preterm birth who may face a greater risk for disruptions in self-relating and parenting competence, particularly younger mothers, those who had a multiple birth pregnancy, and those who may not have a strong support system. Findings accentuate the unaddressed need for targeted support for intrapersonal outcomes beyond the treatment of early postpartum psychopathology and parenting behavior difficulties.
Our findings highlight the importance of a holistic and long-term characterization of maternal experiences after preterm birth [39,40,41]. This recommendation acknowledges the dynamic nature of parenting over time and will enable preventive approaches towards the inclusive optimization of outcomes for all parents rather than the reactive treatment of clinically significant cases. While several associations identified in this study are difficult to modify due to their complex nature, maternal psychosocial well-being and other related indicators (i.e., guilt, shame) may be more readily optimized through empirically supported psychosocial interventions. This includes but is not limited to compassion-focused therapy [42], compassionate mind training [43], acceptance and commitment therapy [44], mindfulness-based cognitive therapy [45], and the preterm birth-specific PREM-baby Triple P [46]. Despite the unique therapeutic differences of these approaches, collectively, they focus on intrapersonal outcomes and provide specific strategies and mechanistic pathways towards assisting parents who experience guilt and shame following a preterm birth.
Recently, due to technological advancements, psychosocial support has become more readily accessible through telehealth and social media avenues [47]. This is particularly pertinent for parents of children born preterm who may experience increased time demands because of ongoing child healthcare needs such as neurodevelopmental follow-up, relative to families with term-born children. Research has identified that mothers who use social media engage with a high level of information-seeking and sharing concerning their parenting role and consider internet-based connections as positive sources of social support [48]. The high proportion of families experiencing preterm birth who participate in neonatal and high-risk birth social media groups and pages, which were used to recruit for this study, supports the relevance of internet-based delivery systems for this population. While this aided in obtaining a large sample, these online recruitment efforts may have introduced selection bias to this study. Specifically, each organization had the primary aim of providing support and enhancing parental belonging. There are many benefits to receiving social support, particularly for mothers including reduced parenting stress [49], increased positive attitudes about being a mother [50], promoting adaptive and responsive parent-child interactions [51], and of note, buffering the negative association between parenting stress and satisfaction [52]. It is therefore plausible that our sample of mothers may have experienced a higher level of optimal well-being compared with mothers who do not belong to or relate with parenting organizations, potentially magnifying the importance of concurrent well-being as a key correlate for maternal outcomes.
There are additional limitations to our study that should be acknowledged while interpreting the findings. Despite extensive recruitment efforts, our sample predominantly comprised certain sociodemographic groups of mothers, including those of majority ethnicity/race (91%), high educational attainment (88%), and high family socioeconomic status (83%) at childbirth. While this study is novel in its multidimensional conceptualization of longer-term maternal intrapersonal experiences following preterm birth, caution should be exercised when considering these outcomes within the context of a more diverse and representative framework. Further, our sample was restricted to selected high-income countries with relatively homogenous parenting practices and access to advanced neonatal care with some form of maternal follow-up after preterm birth. There was also moderate potential for selection bias due to the requirement for English language fluency or access to a web-based device to complete the questionnaires. Other limitations include the cross-sectional study design, which did not allow the individual participant trajectories of the outcomes to be followed over time; and the psychometric quality of the available instruments for these outcomes in the context of the current population, which precluded comparison against standardized groups of parents. The potential impacts of these issues on the results are uncertain. Nevertheless, they identify pertinent areas for future research using prospectively recruited, longitudinally followed samples, representative of all infants born preterm and their families, particularly across factors including but not limited to diverse cultural and ethnic/racial backgrounds, socially determined parenting practices, and those residing in low- and middle-income countries. Furthermore, the findings from this study provide support for the continued investigation of multidimensional parenting outcomes after high-risk birth, with future research encouraged to include term-born comparison groups and an inclusive approach to parental recruitment.
In conclusion, study findings support adopting a multidimensional conceptualization of maternal experiences after preterm birth, extending beyond the current focus on postpartum psychopathology and parenting behavior. Further, findings highlight the need for a holistic, longer-term, psychosocial well-being framework of screening and intervention to optimize both maternal and child outcomes.
Data availability
The corresponding author will make data from this study available upon reasonable request.
References
de Paula Eduardo JAF, de Rezende MG, Menezes PR, Del-Ben CM. Preterm birth as a risk factor for postpartum depression: a systematic review and meta-analysis. J Affect Disord. 2019;259:392–403. https://doi.org/10.1016/j.jad.2019.08.069.
Winter L, Colditz PB, Sanders MR, Boyd RN, Pritchard M, Gray PH, et al. Depression, posttraumatic stress and relationship distress in parents of very preterm infants. Arch Women’s Ment Health. 2018;21:445–51. https://doi.org/10.1007/s00737-018-0821-6.
Yildiz PD, Ayers S, Phillips L. The prevalence of posttraumatic stress disorder in pregnancy and after birth: a systematic review and meta-analysis. J Affect Disord. 2017;208:634–45. https://doi.org/10.1016/j.jad.2016.10.009.
Beck CT, Harrison L. Posttraumatic stress in mothers related to giving birth prematurely: a mixed research synthesis. J Am Psychiatr Nurses Assoc. 2017;23:241–57. https://doi.org/10.1177/1078390317700979.
Toscano C, Soares I, Mesman J. Controlling parenting behaviors in parents of children born preterm: a meta-analysis. J Dev Behav Pediatr. 2020;41:230–41. https://doi.org/10.1097/DBP.0000000000000762.
de Haan AD, Prinzie P, Deković M. Mothers’ and fathers’ personality and parenting: the mediating role of sense of competence. Dev Psychol. 2009;45:1695–707. https://doi.org/10.1037/a0016121.
Ehret AM, Joormann J, Berking M. Examining risk and resilience factors for depression: the role of self-criticism and self-compassion. Cogn Emot. 2015;29:1496–504. https://doi.org/10.1080/02699931.2014.992394.
Neff KD. The development and validation of a scale to measure self-compassion. Self Identity. 2003;2:223–50. https://doi.org/10.1080/15298860309027.
Kim JJ, Parker SL, Doty JR, Cunnington R, Gilbert P, Kirby JN. Neurophysiological and behavioural markers of compassion. Sci Rep. 2020;10:6789 https://doi.org/10.1038/s41598-020-63846-3.
Zessin U, Dickhäuser O, Garbade S. The relationship between self-compassion and well-being: a meta-analysis. Appl Psychol Heal Well Being. 2015;7:340–64. https://doi.org/10.1111/aphw.12051.
Moreira H, Canavarro MC. The association between self-critical rumination and parenting stress: the mediating role of mindful parenting. J Child Fam Stud. 2018;27:2265–75. https://doi.org/10.1007/s10826-018-1072-x.
Gittins CB, Abbott MJ, Hunt C. What influences parenting behaviour? The role of parent self-concept. Behav Chang. 2020;37:195–205. https://doi.org/10.1017/bec.2020.13.
Jefferson FA, Shires A, McAloon J. Parenting self-compassion: a systematic review and meta-analysis. Mindfulness. 2020;11:2067–88. https://doi.org/10.1007/s12671-020-01401-x.
Sawyer Cohen JA, Semple RJ. Mindful parenting: a call for research. J Child Fam Stud. 2010;19:145–51. https://doi.org/10.1007/s10826-009-9285-7.
Sirois FM, Bögels S, Emerson L-M. Self-compassion improves parental well-being in response to challenging parenting events. J Psychol. 2019;153:327–41. https://doi.org/10.1080/00223980.2018.1523123.
Gouveia MJ, Carona C, Canavarro MC, Moreira H. Self-compassion and dispositional mindfulness are associated with parenting styles and parenting stress: the mediating role of mindful parenting. Mindfulness. 2016;7:700–12. https://doi.org/10.1007/s12671-016-0507-y.
Fitzallen GC, Taylor HG, Bora S. What do we know about the preterm behavioral phenotype? A narrative review. Front Psychiatry. 2020;11 https://doi.org/10.3389/fpsyt.2020.00154.
Neff KD, Faso DJ. Self-compassion and well-being in parents of children with autism. Mindfulness. 2015;6:938–47. https://doi.org/10.1007/s12671-014-0359-2.
Ohan JL, Leung DW, Johnston C. The Parenting Sense of Competence scale: evidence of a stable factor structure and validity. Can J Behav Sci. 2000;32:251–61. https://doi.org/10.1037/h0087122.
Mihelic M, Filus A, Morawaska A. Correlates of prenatal parenting expectations in new mothers: is better self-efficacy a potential target for preventing postnatal adjustment difficulties? Prev Sci. 2016;17:949–59. https://doi.org/10.1007/s11121-016-0682-z.
Vance AJ, Brandon DH. Delineating among parenting confidence, parenting self-efficacy, and competence. ANS Adv Nurs Sci. 2017;40:E18–E37. https://doi.org/10.1097/ANS.0000000000000179.
Premji SS, Pana G, Currie G, Dosani A, Reilly S, Young M, et al. Mother’s level of confidence in caring for her late preterm infant: a mixed methods study. J Clin Nurs. 2018;27:e1120–e1133. https://doi.org/10.1111/jocn.14190.
Pennell C, Whittingham K, Boyd R, Sanders M, Colditz P. Prematurity and parental self-efficacy: the Preterm Parenting & Self-Efficacy Checklist. Infant Behav Dev. 2012;35:678–88. https://doi.org/10.1016/j.infbeh.2012.07.009.
Johnson S, Marlow N. Preterm birth and childhood psychiatric disorders. Pediatr Res. 2011;69:11–18. https://doi.org/10.1203/PDR.0b013e318212faa0.
American Association for Public Opinion Research. Best Practices for Survey Research. Accessed May 17, 2019. https://aapor.org/standards-and-ethics/best-practices/.
Gilbert P, Clarke M, Hempel S, Miles JNV, Irons C. Criticizing and reassuring oneself: an exploration of forms, styles and reasons in female students. Br J Clin Psychol. 2004;43:31–50. https://doi.org/10.1348/014466504772812959.
Baião R, Gilbert P, McEwan K, Carvalho S. Forms of Self‐Criticising/Attacking & Self‐Reassuring Scale: psychometric properties and normative study. Psychol Psychother. 2015;88:438–52. https://doi.org/10.1111/papt.12049.
Halamová J, Kanovský M, Gilbert P, Troop NA, Zuroff DC, Hermanto N, et al. The factor structure of the Forms of Self-Criticising/Attacking & Self-Reassuring Scale in thirteen distinct populations. J Psychopathol Behav Assess. 2018;40:736–51. https://doi.org/10.1007/s10862-018-9686-2.
Costa J, Marôco J, Pinto-Gouveia J, Ferreira C, Castilho P. Validation of the psychometric properties of the Self-Compassion Scale. Testing the factorial validity and factorial invariance of the measure among borderline personality disorder, anxiety disorder, eating disorder and general populations. Clin Psychol Psychother. 2016;23:460–8. https://doi.org/10.1002/cpp.1974.
Gibaud-Wallston J, Wandersman LP Parenting Sense of Competence (PSOC). In: Touliatos J, Perlmutter BF, Holden GW, eds. Handbook of Family Measurement Techniques. Thousand Oaks, CA, USA: Sage Publications; 2001:166-7.
Karp SM, Lutenbacher M, Wallston KA. Evaluation of the Parenting Sense of Competence scale in mothers of infants. J Child Fam Stud. 2015;24:3474–81. https://doi.org/10.1007/s10826-015-0149-z.
Bandura A. Self-efficacy mechanism in human agency. Am Psychol. 1982;37:122–47. https://doi.org/10.1037/0003-066X.37.2.12.
Allotey J, Zamora J, Cheong-See F, Kalidindi M, Arroyo-Manzano, Asztalos E, et al. Cognitive, motor, behavioural and academic performances of children born preterm: a meta-analysis and systematic review involving 64 061 children. BJOG. 2018;125:16–25. https://doi.org/10.1111/1471-0528.14832.
Yaari M, Treyvaud K, Lee KJ, Doyle LW, Anderson PJ. Preterm birth and maternal mental health: longitudinal trajectories and predictors. J Pediatr Psychol. 2019;44:736–47. https://doi.org/10.1093/jpepsy/jsz019.
Wolke D, Baumann N, Busch B, Bartmann P. Very preterm birth and parents’ quality of life 27 years later. Pediatrics. 2017;140:e20171263 https://doi.org/10.1542/peds.2017-1263.
Reid LD, Strobino DM. A population-based study of school readiness determinants in a large urban public school district. Matern Child Health J. 2019;23:325–34. https://doi.org/10.1007/s10995-018-2666-z.
Taraban L, Shaw DS. Parenting in context: revisiting Belsky’s classic process of parenting model in early childhood. Dev Rev. 2018;48:55–81. https://doi.org/10.1016/j.dr.2018.03.006.
Belsky J. The determinants of parenting: a process model. Child Dev. 1984;55:83–96. https://doi.org/10.1111/j.1467-8624.1984.tb00275.x.
Krulik T, Turner-Henson A, Kanematsu Y, Al-Ma’aitah R, Swan J, Holaday B. Parenting stress and mothers of young children with chronic illness: a cross-cultural study. J Pediatr Nurs. 1999;14:130–40. https://doi.org/10.1016/S0882-5963(99)80051-7.
Maltby HJ, Kristjanson L, Coleman ME. The parenting competency framework: learning to be a parent of a child with asthma. Int J Nurs Pr. 2003;9:368–73. https://doi.org/10.1046/j.1440-172X.2003.00445.x.
Tanenbaum ML, Adams RN, Wong JJ, Hood KK. Diabetes-specific self-compassion: a new measure for parents of youth with type 1 diabetes. J Pediatr Psychol. 2020;45:488–97. https://doi.org/10.1093/jpepsy/jsaa011.
Gilbert P. The origins and nature of compassion-focused therapy. Br J Clin Psychol. 2014;53:6–41. https://doi.org/10.1111/bjc.12043.
Kelman AR, Evare BS, Barrera AZ, Muñoz RF, Gilbert P. A proof-of-concept pilot randomized comparative trial of brief Internet-based compassionate mind training and cognitive-behavioral therapy for perinatal and intending to become pregnant women. Clin Psychol Psychother. 2018;25:608–19. https://doi.org/10.1002/cpp.2185.
Hayes SC, Strosahl KD, Wilson KG Acceptance and Commitment Therapy: The Process and Practice of Mindful Change (2nd Edition). New York, NY, USA: The Guilford Press; 2012.
Segal ZV, Teasdale JD, Williams JMG, Hayes SC, Follette VM, Linehan MM. Mindfulness-based cognitive therapy: theoretical rationale and empirical status. Mindfulness and Acceptance: Expanding the Cognitive-Behavioral Tradition. New York, NY, USA: The Guilford Press; 2004. p. 45–65.
Ferrari AJ, Whittingham K, Boyd R, Sanders M, Colditz P. Prem Baby Triple P a new parenting intervention for parents of infants born very preterm: acceptability and barriers. Infant Behav Dev. 2011;34:602–9. https://doi.org/10.1016/j.infbeh.2011.06.004.
Wootton R, Bonnardot L. Telemedicine in low-resource settings. Front Public Heal. 2015;3:3 https://doi.org/10.3389/fpubh.2015.00003.
Baker B, Yang I. Social media as social support in pregnancy and the postpartum. Sex Reprod Health. 2018;17:31–34. https://doi.org/10.1016/j.srhc.2018.05.003.
Lutz KF, Burnson C, Hane A, Samuelson A, Maleck S, Poehlmann J. Parenting stress, social support, and mother-child interactions in families of multiple and singleton preterm toddlers. Fam Relat. 2012;61:642–56. https://doi.org/10.1111/j.1741-3729.2012.00726.x.
Crnic KA, Greenberg MT, Ragozin AS, Robinson NM, Basham RB. Effects of stress and social support on mothers and premature and full-term infants. Child Dev. 1983;54:209–17. https://doi.org/10.2307/1129878.
Amankwaa LC, Pickler RH, Boonmee J. Maternal responsiveness in mothers of preterm infants. Newborn Infant Nurs Rev. 2007;7:25–30. https://doi.org/10.1053/j.nainr.2006.12.001.
Crnic K, Ross E Parenting stress and parental efficacy. In: Deater-Deckard K, Panneton R, eds. Parental Stress and Early Child Development: Adaptive and Maladaptive Outcomes. Springer International Publishing; 2017:263-84 https://doi.org/10.1007/978-3-319-55376-4_11.
Acknowledgements
Mr. Paul Jackson at The University of Queensland, Australia developed the secure web-based data collection portal. The following parent organizations listed in alphabetical order contributed to the recruitment of study participants. Australian Dad’s Network; Australian Multiple Birth Association; Brisbane Dads; Brisbane Multiple Birth Association—Southside; Canadian Premature Babies Foundation; Colourful Beginnings; Hand to Hold; Hoju Martial Arts; International Council of Multiple Birth Organizations; Irish Neonatal Health Alliance; Jessica and Lily (@lilyslittlelungs); Jonathon II and Zoe (@theprincetwins); Keep em Cookin; Life’s Little Treasures Foundation Ltd; Miracle Babies Foundation and Ms. Melinda Cruz Turner; Monoamniotic Twins Ireland; Multiple Birth South Australia; Multiple Births Canada; Multiples Illuminated; Mums Parenting Teens Australia; NICU and High-Risk-Pregnancy Support AUS; NICU MOM’s and Family Support Group; North Brisbane Parents Group; Octopus for Preemie Baby Queensland; Our Little Preemie; Parents of Preemies/Premature Babies; Parents of Preemies Support UK; Preemiehood; PreemieWorld; Preterm Infants’ Parents’ Association; Project Sweet Peas; Seattle Parents of Preemies; Silvie Bells; Small Babies; The Champion Centre; The Little Miracles Trust; TinyLife; Twins and Multiples (@twinsandmultiples); Twins, Triplets, and More Association of Calgary—TTMAC; Twinfo; Twins Trust; The Zaky by Nurtured by Design. This work was supported by a Mater Foundation Principal Research Fellowship and the University Hospitals Cleveland Medical Center and Case Western Reserve University School of Medicine’s Joint Strategic Research Investment to Dr. Samudragupta Bora, and The University of Queensland Research Training Program and Frank Clair Scholarship to Dr. Grace C. Fitzallen. The funding sources had no role in the writing of the manuscript or the decision to submit it for publication.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Contributions
GCF conceptualized the study, designed the study protocol, performed data collection and analyses, interpreted the results, drafted and revised the initial manuscript, and approved the final manuscript as submitted. JNK, HGT, and HGL conceptualized the study, supervised data analyses, interpreted the results, critically reviewed and revised the initial manuscript, and approved the final manuscript as submitted. SB acquired funds and resources, conceptualized the study, designed the study protocol, supervised data collection and analyses, interpreted the results, critically reviewed and revised the initial manuscript, and approved the final manuscript as submitted.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fitzallen, G.C., Kirby, J.N., Taylor, H.G. et al. Evaluating multidimensional facets of the maternal experience after preterm birth. J Perinatol 44, 635–642 (2024). https://doi.org/10.1038/s41372-024-01865-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-024-01865-y
