
Abstract
Objective
Infants born to mothers with preeclampsia are at risk for many short and long-term complications. The objective of this study was to examine the association between preeclampsia and ICD diagnosis of neonatal sepsis in a large United States data set.
Study design
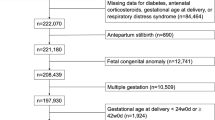
A retrospective cohort study from the Consortium on Safe Labor. A total of 180,277 women with a singleton gestation greater than 23 weeks were included. The primary outcome, neonatal sepsis, was compared between women stratified by diagnosis of preeclampsia using univariable and multivariable analyses.
Results
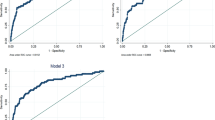
Of the 180,277 women eligible for analysis, 8331 (4.6%) were diagnosed with preeclampsia. Neonatal sepsis rates were higher among women diagnosed with preeclampsia (6.4 vs. 2.0%, p < 0.001). In multivariable logistic regression, adjusted for confounders, the association between preeclampsia and neonatal sepsis remained significant (adjusted OR = 1.30, 95% CI: 1.06–1.60).
Conclusion
In this large cohort, the rate of neonatal sepsis ICD diagnosis was higher among women diagnosed with preeclampsia.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
American College of Obstetricians and Gynecologists. ACOG Practice bulletin no. 202: gestational hypertension and preeclampsia. Obstet Gynecol. 2019;133:e1–25.
Langenveld J, Broekhuijsen K, van Baaren GJ, van Pampus MG, van Kaam AH, Groen H, et al. Induction of labour versus expectant monitoring for gestational hypertension or mild pre-eclampsia between 34 and 37 weeks’ gestation (HYPITAT-II): a multicentre, open-label randomised controlled trial. BMC Pregnancy Childbirth. 2011;11:50.
Cruz MO, Gao W, Hibbard JU. Obstetrical and perinatal outcomes among women with gestational hypertension, mild preeclampsia, and mild chronic hypertension. AM J Obstet Gynecol. 2011;205:260.
Lu CQ, Lin J, Yuan L, Zhou JG, Liang K, Zhong QH, et al. Pregnancy induced hypertension and outcomes in early and moderate preterm infants. Pregnancy Hypertens. 2018;14:68–71.
Jelin AC, Cheng YW, Shaffer BL, Kaimal AJ, Little SE, Caughey AB. Early-onset preeclampsia and neonatal outcomes. J Matern Fetal Neonatal Med. 2010;23:389–92.
Backes CH, Markham K, Moorehead P, Cordero L, Nankervis CA, Giannone PJ. Maternal preeclampsia and neonatal outcomes. J Pregnancy. 2011;2011:1–8.
Perger L, Mukhopadhyay D, Komidar L, Wiggins-Dohlvik K, Uddin MN, Beeram M. Maternal pre-eclampsia as a risk factor for necrotizing enterocolitis. J Matern Fetal Neonatal Med. 2016;29:2098–103.
Hall DR, Odendaal HJ, Kirsten GF, Smith J, Grove D. Expectant management of early onset, severe pre‐eclampsia: perinatal outcome. BJOG. 2000;107:1258–64.
Stevens W, Shih T, Incerti D, Ton TG, Lee HC, Peneva D, et al. Short-term costs of preeclampsia to the United States health care system. AM J Obstet Gynecol. 2017;217:237–48.
Habli M, Levine RJ, Qian C, Sibai B. Neonatal outcomes in pregnancies with preeclampsia or gestational hypertension and in normotensive pregnancies that delivered at 35, 36, or 37 weeks of gestation. AM J Obstet Gynecol. 2007;197:406.
Davies EL, Bell JS, Bhattacharya S. Preeclampsia and preterm delivery: a population-based case–control study. Hypertens Pregnancy. 2016;35:510–9.
Cetinkaya M, Ozkan H, Koksal N. Maternal preeclampsia is associated with increased risk of necrotizing enterocolitis in preterm infants. Early Hum Dev. 2012;88:893–8.
Beiner ME, Simchen MJ, Sivan E, Chetrit A, Kuint J, Schiff E. Risk factors for neonatal thrombocytopenia in preterm infants. Am J Perinatol. 2003;20:049–54.
de Souza Rugolo LM, Bentlin MR, Trindade CE. Preeclampsia: early and late neonatal outcomes. Neoreviews. 2012;13:e532–41.
Lewin S, Bussel JB. Review of fetal and neonatal immune cytopenias. Clin Adv Hematol Oncol. 2015;13:35–43.
Koenig JM, Christensen RD. Incidence, neutrophil kinetics, and natural history of neonatal neutropenia associated with maternal hypertension. N Eng J Med. 1989;321:557–62.
Sacks GP, Studena K, Sargent IL, Redman CW. Normal pregnancy and preeclampsia both produce inflammatory changes in peripheral blood leukocytes akin to those of sepsis. AM J Obstet Gynecol. 1998;179:80–6.
Leavey K, Grynspan D, Cox BJ. Both “canonical” and “immunological” preeclampsia subtypes demonstrate changes in placental immune cell composition. Placenta. 2019;83:53–6.
El-Chennawi F, Rageh IM, Mansour AI, Darwish MI, Elghzaly AA, Sakr BE, et al. Comparison of the percentages of CD4+ CD25 high FOXP3+, CD4+ CD25 low FOXP3+, and CD4+ FOXP3+ Tregs, in the umbilical cord blood of babies born to mothers with and without preeclampsia. Am J Reprod Immunol. 2017;78:e12761.
Ferguson KK, Meeker JD, McElrath TF, Mukherjee B, Cantonwine DE. Repeated measures of inflammation and oxidative stress biomarkers in preeclamptic and normotensive pregnancies. AM J Obstet Gynecol. 2017;216:527.
Vigil-De Gracia P, Tejada OR, Miñaca AC, Tellez G, Chon VY, Herrarte E, et al. Expectant management of severe preeclampsia remote from term: the MEXPRE Latin Study, a randomized, multicenter clinical trial. AM J Obstet Gynecol. 2013;209:425.
Friedman SA, Schiff E, Kao L, Sibai BM. Neonatal outcome after preterm delivery for preeclampsia. AM J Obstet Gynecol. 1995;172:1785–92.
Koopmans CM, Bijlenga D, Groen H, Vijgen SM, Aarnoudse JG, Bekedam DJ, et al. Induction of labour versus expectant monitoring for gestational hypertension or mild pre-eclampsia after 36 weeks’ gestation (HYPITAT): a multicentre, open-label randomised controlled trial. Lancet. 2009;374:979–88.
Broekhuijsen K, van Baaren GJ, Van Pampus MG, Ganzevoort W, Sikkema JM, Woiski MD, et al. Immediate delivery versus expectant monitoring for hypertensive disorders of pregnancy between 34 and 37 weeks of gestation (HYPITAT-II): an open-label, randomised controlled trial. Lancet. 2015;385:2492–501.
Shane AL, Sánchez PJ, Stoll BJ. Neonatal sepsis. Lancet. 2017;390:1770–80.
Heron M. National Vital Statistics Reports. CDC.GOV. Deaths: leading causes for 2015. 2017. vol. 66. https://www.cdc.gov/nchs/data/nvsr/nvsr66/nvsr66_05.pdf.
Khan AM, Morris SK, Bhutta ZA. Neonatal and perinatal infections. Pediatr Clin. 2017;64:785–98.
Zhang J, Troendle J, Reddy UM, Laughon SK, Branch DW, Burkman R, et al. Contemporary cesarean delivery practice in the United States. AM J Obstet Gynecol. 2010;203:326.
Boyle A, Reddy UM, Landy HJ, Huang CC, Driggers RW, Laughon SK. Primary cesarean delivery in the United States. Obstet Gynecol. 2013;122:33.
Puopolo KM, Draper D, Wi S, Newman TB, Zupancic J, Lieberman E, et al. Estimating the probability of neonatal early-onset infection on the basis of maternal risk factors. Pediatrics. 2011;128:e1155–63.
Schrag SJ, Hadler JL, Arnold KE, Martell-Cleary P, Reingold A, Schuchat A. Risk factors for invasive, early-onset Escherichia coli infections in the era of widespread intrapartum antibiotic use. Pediatrics. 2006;118:570–6.
Palatnik A, Liu LY, Lee A, Yee LM. Predictors of early-onset neonatal sepsis or death among newborns born at < 32 weeks of gestation. J Perinatol. 2019;39:949.
Bailit JL, Gregory KD, Reddy UM, Gonzalez-Quintero VH, Hibbard JU, Ramirez MM, et al. Maternal and neonatal outcomes by labor onset type and gestational age. AM J Obstet Gynecol. 2010;202:245.
Weston EJ, Pondo T, Lewis MM, Martell-Cleary P, Morin C, Jewell B, et al. The burden of invasive early-onset neonatal sepsis in the United States, 2005–2008. Pediatr Infect Dis J. 2011;30:937.
Windham GC, Hopkins B, Fenster L, Swan SH. Prenatal active or passive tobacco smoke exposure and the risk of preterm delivery or low birth weight. Epidemiology. 2000;11:427–33.
Hedderson MM, Ferrara A, Sacks DA. Gestational diabetes mellitus and lesser degrees of pregnancy hyperglycemia: association with increased risk of spontaneous preterm birth. Obstet Gynecol. 2003;102:850–6.
Higgins RD, Saade G, Polin RA, Grobman WA, Buhimschi IA, Watterberg K, et al. Evaluation and management of women and newborns with a maternal diagnosis of chorioamnionitis: summary of a workshop. Obstet Gynecol. 2016;127:426.
Martin JA, Osterman MJ, Centers for Disease Control and Prevention (CDC). Preterm births—United States, 2006 and 2010. MMWR Suppl. 2013;62(Suppl 3):136–8.
Easter SR, Molina RL, Venkatesh KK, Kaimal A, Tuomala R, Riley LE. Clinical risk factors associated with peripartum maternal bacteremia. Obstet Gynecol. 2017;130:710–7.
Boggess KA, Tita A, Jauk V, Saade G, Longo S, Clark EA, et al. Risk factors for postcesarean maternal infection in a trial of extended spectrum antibiotic prophylaxis. Obstet Gynecol. 2017;129:481.
Acknowledgements
We would like to acknowledge the NICHD for use of their database.
Author information
Authors and Affiliations
Contributions
RKH contributed to the design, analysis, and interpretation of the data as well as drafting the work. AP contributed to the design, analysis, and interpretation of the data as well as revising the work. All authors approved the final version to be published and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Harrison, R.K., Palatnik, A. The association between preeclampsia and ICD diagnosis of neonatal sepsis. J Perinatol 41, 460–467 (2021). https://doi.org/10.1038/s41372-020-00774-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-020-00774-0
